Clostridioides difficile infection in liver cirrhosis patients: A population-based study in United States
2021-09-03SyedaSahraMohammadAbureeshShivanthaAmarnathMotasemAlkhayyatRawanBadranAbdullahJahangirVivekGumaste
Syeda Sahra, Mohammad Abureesh, Shivantha Amarnath, Motasem Alkhayyat, Rawan Badran, Abdullah Jahangir, Vivek Gumaste
Syeda Sahra, Mohammad Abureesh, Shivantha Amarnath, Rawan Badran, Abdullah Jahangir, Department of Internal Medicine, Staten Island University Hospital, Staten Island, NY 10305, United States
Motasem Alkhayyat, Department of Internal Medicine, Cleveland Clinic Foundation, Cleveland, OH 44195, United States
Vivek Gumaste, Department of Gastroenterology, Staten Island University Hospital, Staten Island, NY 10305, United States
Abstract BACKGROUND Clostridioides (formerly Clostridium) difficile infection (CDI) is an increasingly frequent cause of morbidity and mortality in hospitalized patients.Multiple risk factors are documented in the literature that includes, but are not limited to, antibiotics use, advanced age, and gastric acid suppression.Several epidemiological studies have reported an increased incidence of CDI in advanced liver disease patients.Some have also demonstrated a higher prevalence of nosocomial infections in cirrhotic patients.AIM To use a large nationwide database, we sought to determine CDI’s risk among liver cirrhosis patients in the United States.METHODS We queried a commercial database (Explorys IncTM, Cleveland, OH, United States), and obtained an aggregate of electronic health record data from 26 major integrated United States healthcare systems comprising 360 hospitals in the United States from 2018 to 2021.Diagnoses were organized into the Systematized Nomenclature of Medicine Clinical Terms (SNOMED-CT) hierarchy.Statistical analysis for the multivariable model was performed using Statistical Package for Social Sciences (SPSS version 25, IBM CorpTM).For all analyses, a two-sided P value of < 0.05 was considered statistically significant.RESULTS There were a total of 19387760 patients in the database who were above 20 years of age between the years 2018-2021.Of those, 133400 were diagnosed with liver cirrhosis.The prevalence of CDI amongst the liver cirrhosis population was 134.93 per 100.000 vs 19.06 per 100.000 in non-cirrhotic patients (P < 0.0001).The multivariate analysis model uncovered that cirrhotic patients were more likely to develop CDI (OR: 1.857; 95%CI: 1.665-2.113, P < 0.0001) compared to those without any prior history of liver cirrhosis.CONCLUSION In this large database study, we uncovered that cirrhotic patients have a significantly higher CDI prevalence than those without cirrhosis.Liver cirrhosis may be an independent risk factor for CDI.Further prospective studies are needed to clarify this possible risk association that may lead to the implementation of screening methods in this high-risk population.
Key Words: Clostridioides difficile; Chronic liver disease; Liver cirrhosis; Liver transplant
INTRODUCTION
Clostridiodes difficileis a gram-positive anaerobic bacillus.It is widespread in the surrounding environment and a significant contributor to inpatient mortality in vulnerable subgroups[1].Risk factors for being predisposed to CDI include advanced age, enteral feeding, smoking, alcohol abuse, and use of antibiotics and acidsuppressive therapy.It is particularly predominant in elderly patients who reside in nursing homes and long-term acute care facilities and have a history of recurrent hospitalizations.CDI carries a significant economic burden on the USA health care system.A recent study by Desaiet al[2] uncovered that CDI's economic cost was roughly $5.4 billion, with $4.7 billion in the healthcare settings and $725 million in the community.
CDI has a spectrum of clinical symptoms, including nausea, vomiting, abdominal pain, watery diarrhea with the formation of pseudomembranous, progression to fulminant colitis, and even toxic mega colon[3-8].CDI can culminate in the possible rupture of the large colon, septic shock, and death.Reactive arthritis is also seen as one of the complications of CDI[9].
Broad-spectrum antibiotic use (penicillin, cephalosporins, clindamycin, fluoroquinolones) predispose individuals to selective elimination of healthy gut microbiota and overgrowth ofClostridium difficile(C.difficile)in the gastrointestinal flora[10,11] with the highest risk of CDI within the first three months of antibiotic exposure[12].As the environment and normal human gastrointestinal tract are heavily colonized with C.difficile[5,13-15], it is just a matter of loss of balance where C.difficileinvades the protective gastrointestinal barriers through the production of toxins (enterotoxin A, cytotoxin B, binary toxin/CDT) and enzymes (collagenase, chondroitin sulfatase, hyaluronidase) which promote inflammation[16-18].The virulence and pathogenicity are compounded by new hypervirulent strains and the potential ability of C.difficileto create biofilmsin vivo(after anin vitrodemonstration)[19,20].For instance,C.difficile, especially the new hypervirulent strain, NAP1/BI/027 that was uncovered in the year 2000, was responsible for a significant CDI-related mortality increase 5.7 deaths per million in 1999 to 23.7 deaths per million in 2004[21].CDI is currently considered the most common cause of nosocomial diarrhea in the western world.
CDI's have been classified based on the severity of infection, utilizing the markers of inflammation and organ function, including white blood cell count (WBC), creatinine and albumin levels.Prognostic markers in patients withC.difficilecolitis included low serum albumin (< 2.5 mg/dL) or a 1.1 mg/dL reduction in serum albumin from baseline, use of multiple antibiotics, and a positive CD cytotoxin in stool after completion of treatment (after seven or more days of treatment)[22].
The poor outcomes with CDI are not uncommon.They are particularly pronounced in patients with underlying chronic comorbidities (congestive heart failure, chronic obstructive pulmonary disease, and chronic kidney disease), history of solid organ transplants and immunosuppressive therapy, and chronic inflammatory diseases, including Crohn's disease and Ulcerative colitis[23-29].The morbidity and mortality from liver cirrhosis is on the rise[30].A prospective study by Bouzaet al[31] that focused on the recent outbreak ofC.difficilePCR ribotype 027 in Spain uncovered that this strain was most evident in patients with age > 75 years, the male gender, and comorbidities such hypertension, chronic cardiovascular disease, type 2 diabetes, and liver cirrhosis.Interestingly, liver cirrhosis was associated with an increased CDI recurrence risk of 44.4%vs14.8%[31].The increased prevalence of CDI in patients with advanced liver disease is being investigated as they are already immunocompromised[32,33].
Poor outcomes in cirrhotic patients who acquired CDI are reported in a recent study by Abdallaet al[34].Liver cirrhosis itself can predispose the individuals to nosocomial infections, the deadliest of them being CDI.For instance, several studies have reported that CLD patients with CDI have a higher mortality rate, prolonged length of stay, and higher hospital cost[35-37].We performed this large database study to re-evaluate the risk and severity of CDI in patients with cirrhosis.Prevalence ofC.difficileassociated disease (CDAD) was determined in the subgroups with established risk factors and comorbidities and prior history of liver disease and liver transplant.
MATERIALS AND METHODS
Database
Our study is a retrospective cohort analysis of a large, multicenter database (Explorys, Cleveland, OH, United States).Explorys aggregates healthcare data of more than 50 million unique patient records.Diagnoses, findings, and procedures are arranged into the Systematized Nomenclature of Medicine-Clinical Terms (SNOMED-CT) hierarchy, whereas prescription drug orders are mapped into RxNorm.Explorys provides an interactive search engine to generate multiple cohorts based on medical diagnoses.Medical data are de-identified, and therefore, it is a Health Insurance Portability and Accountability Act-compliant platform.
Patient selection
Using the Explorys platform, we identified cohorts of patients diagnosed with Liver cirrhosis between the period of March 2018 and March 2021.The study cohorts (liver cirrhosis) were identified by searching the database for a SNOMED-CT diagnosis of "Cirrhosis of Liver" after excluding patients younger than 20 years old.The control group was then identified for those who have no liver cirrhosis.Subsequently, a cohort of patients with "clostridioides difficle infection" diagnosis was identified between the period of March 2018 to March 2021 to calculate the prevalence of CDI in both study groups.Risk factors and predisposing medical conditions associated with CDI, in addition to demographic information, were collected.Possible risk factors included comorbid medical conditions, antibiotics, acid-suppressive therapy, liver transplant, and inpatient/skilled nursing facility settings were investigated using SNOMED-CT diagnostic codes.
Statistical analysis
The prevalence was calculated by dividing the total number of individuals with CDI in each cohort (liver cirrhosis and non-cirrhotics) by the total number of individuals in each cohort as identified by Explorys [2018-2021], thus making sure that all patients in the denominator had an equal opportunity of being diagnosed with CDI.We calculated the prevalence in subgroups based on sex, race, and age by dividing the number of individuals with CDI in each subgroup by a total number of patients in the same subgroup.A multivariate regression model was constructed using binary logistic regression, with CDI being the outcome to adjust for possible confounding from the covariates listed previously.We used SPSS version 25 (IBM Corp) to perform the multivariate regression analysis.A 2-sidedPvalue of < 0.05 was considered statistically significant.
RESULTS
Descriptive epidemiology
There were a total of 19387760 patients in the database who were above 20 years of age.Of those, 133400 were diagnosed with liver cirrhosis.The baseline characteristics of the study population are presented in Table 1.The prevalence of CDI amongst the liver cirrhosis population was 134.93 per 100.000vs19.06 per 100.000 in non-cirrhotic patients (P <0.0001).Figure 1 represents the prevalence of CDI in different age groups among cirrhotics.Females and Caucasian patients had a higher CDI prevalence than males and non-caucasian among both study groups (Table 2).Patients with nonalcoholic liver disease (NAFLD) as well as an alcoholic liver disease were found to have a higher prevalence of CDI when compared to cirrhotic patients with viral hepatitis (184.9/100.000 in NAFLDvs174.0/100.000 in alcoholic liver diseasevs117.9/100.000 in hepatitis Cvs81.7/100.000 in hepatitis B) (Figure 2).
Multivariate analysis
The multivariate analysis model uncovered that cirrhotic patients were more likely to develop CDI (OR 1.857; 95%CI: 1.665-2.113,P <0.0001) compared to those without any prior history of liver cirrhosis.The characteristics of the liver cirrhosis patients who developed CDI revealed that they were more likely to be of advanced age (age > 65) as opposed to being young (age < 65) with an OR 2.307, 95%CI: 2.179-2.442 (P <0.0001); had prior use of antibiotics (OR 19.749, 95%CI: 17.3-22.545,P <0.0001 ); had used acidsuppressive therapy (OR 2.243, 95%CI: 2.122-2.371,P <0.0001); and were mostly inpatients/skilled nursing facility occupantsvsthe community (OR 2.02, 95%CI: 1.911-2.134,P <0.0001 ).Among cirrhotic patients, those with a history of liver transplant (OR 2.737, 95%CI: 2.087-3.589) were highly likely to develop CDI.The multivariate analysis model with CDI being the outcome is presented in Table 3.
DISCUSSION
The multivariate analysis of this database study holds true for the high prevalence of CDI in cirrhotic patients with all the established risk factors (advanced age, use of antibiotics and acid suppression therapy, enteral feeding, residence at long term care facilities, and frequent hospitalizations) and comorbidities (obesity, hypertension, Diabetes Mellitus, chronic obstructive pulmonary disease, congestive heart failure)[38-45].The highest prevalence of CDI was reported in patients with a history of antibiotic use.CDI’s were also encountered in traditionally low-risk population groups in hospitalized patients with recent antibiotic exposure[46].
The colonization ofC.difficilehas been higher in cirrhotic patients with simultaneous hepatic encephalopathy and advanced stage (Child-Pugh C)[47].Risk factors of CDI in cirrhotic patients have been determined by Yanet al[48] in their latest study (advanced age, antibiotics, and proton pump inhibitors, prolonged and recurrent hospitalizations, hyponatremia,C.difficilecolonization, hepatic encephalopathy).
The bacterial infections, which generally would have been countered with immunoregulatory mechanisms (chemotaxis, phagocytosis, oxidation, interferon cascade, complement system, inflammatory response) in an immunocompetent individual, go rampant[49-52].High ammonia levels alter these neutrophilic responses[53].The inflammation response is also dampened from poor nutrition status and alcoholism, which come with cirrhosis.The mechanisms responsible include reticuloendothelial system dysfunction, portosystemic shunting, hyperdynamic circulation, increased permeability of gut, and bacterial translocation.The systemic inflammatory response syndrome (SIRS) is amplified by the increased nitric oxide (NO) and thecytokine storm.

Table 1 Baseline characteristics of study population, n (%)
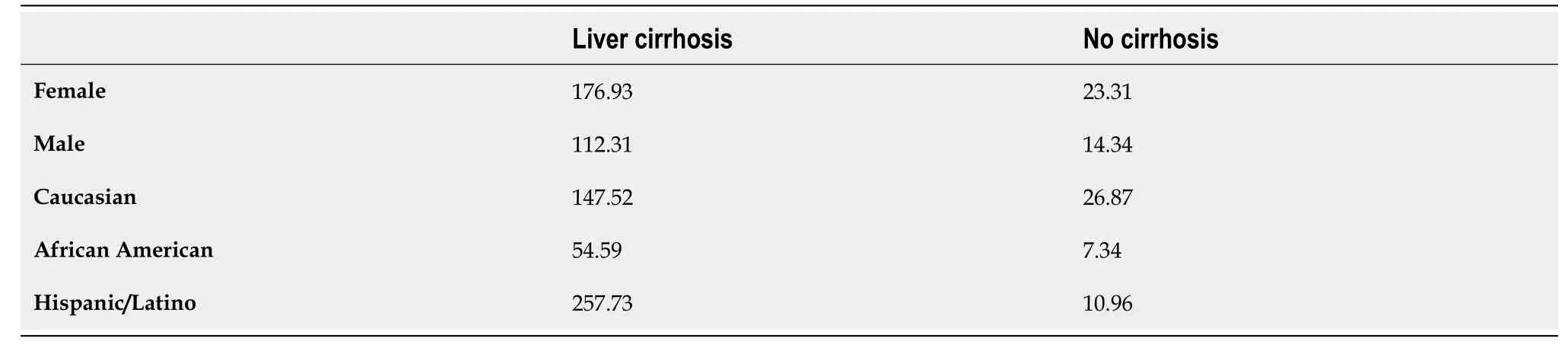
Table 2 Prevalence of Clostridioides difficile infection in different age and race groups in patients with liver cirrhosis vs no cirrhosis (per 100000)
The rate of CDI was significantly high in patients who underwent hepatic transplantation.CDI risk is increased in immunocompromising health conditions involving any solid organ transplant[54,55], including liver transplant recipients[56].The timeline of CDI in post-transplant patients has been established based on the underlying severity of cirrhosis dictated by model for end-stage liver disease (MELD) scoring, concurrent intra-abdominal hemorrhage, repeat grafting and transplant, vascular complications, infections, and the need for endoscopy with sicker patients developing CDI earlier with higher mortality[57,58].Musaet al[59] researched CDI and chronic liver disease with an additional focus on liver transplant patients.Male sex and high pre-op creatinine levels (> 1 g/L) are considered predisposing risk factors for CDI in the subgroup who received a living donor hepatic transplant[60].Advanced cirrhosis (High MELD score), impaired renal function in the donor, and postoperative complications (infection, bleeding, wound) leading to prolonged hospital stay wereconcluded predisposing factors for CDI after a deceased liver transplant[57].Recurrence of pseudomembranous colitis up to five times after living donor liver transplantation has been reported in the literature[61].
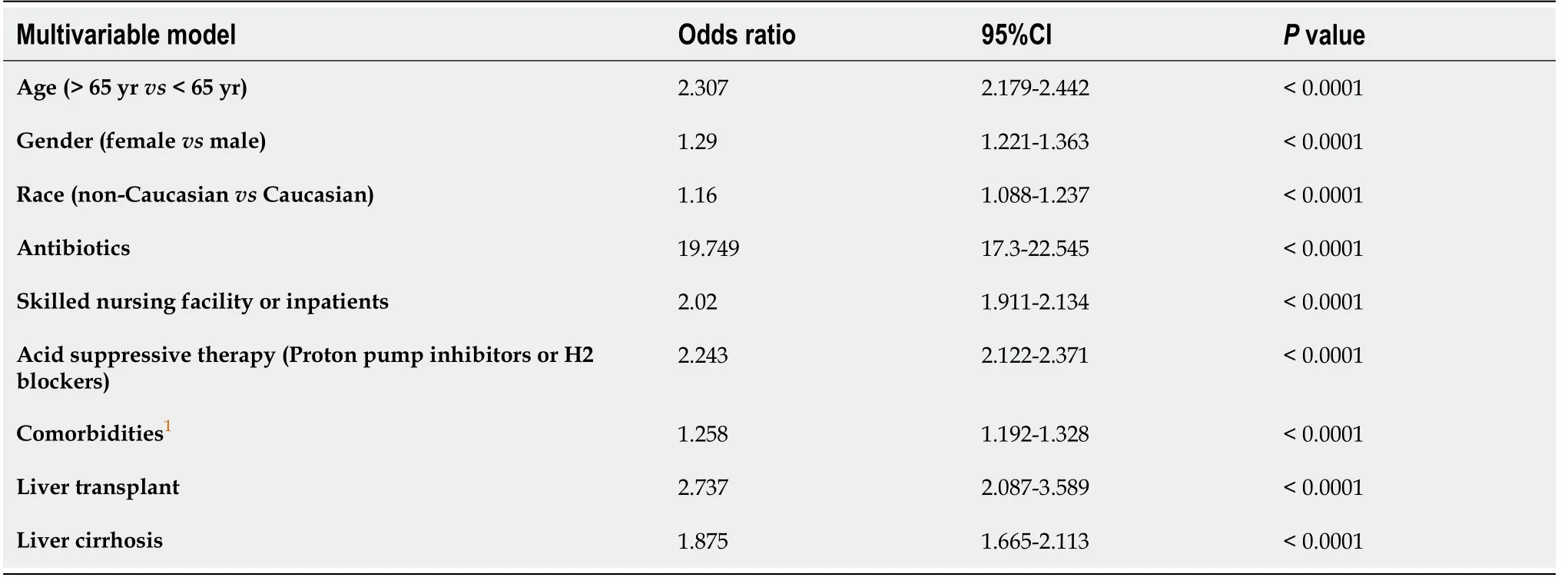
Table 3 Multivariable model with Clostridioides difficile infection being the outcome

Figure 1 Prevalence of Clostridioides difficile infection in patients with liver cirrhosis vs no cirrhosis.
The CDI rate was higher in patients with autoimmune hepatitis, prolonged hospital stay, and antibiotic exposure in a study performed by Vanjaket al[62].Hepatitis C is increasingly identified as an underlying viral infection responsible for cirrhosis in patients who developed CDI later in life[63].Comparing CDI incidence in cirrhosis due to hepatitis B and hepatitis C has not been explored yet.Our study explores this comparison and demonstrates that the prevalence of CDI is higher in inpatient subgroups with hepatitis C than hepatitis B.Sundaramet al[36] reported higher inpatient mortality secondary to CDI in patient subgroups with alcohol abuse-related hepatic cirrhosis.Additionally, NAFLD has been identified as a risk factor for CDI by Papićet al[64]; after adjusting for other comorbidities, hospitalization rates, and antibiotic exposure (Sundaramet al[36]).
Acid suppressive therapy has been implicated with CDI in the general population.A study reported increased 30-d mortality in cirrhotic patients with proton pump inhibitor (PPI) use[35].The association is being attributed to their excessive unindicated use.The majority of people presenting with variceal bleed get discharged with PPIs renewed on each visit[33,65].Chronic use of PPIs causes altered gut flora and motility and decreased neutrophilic function[66].Long-term PPIs use has been attributed to CDI’s by suppressing gastric acid, although the evidence[67-71].PPIs are said to have worse outcomes in cirrhotic patients than H2 blockers in one study[8].Hence, the proper need for PPIs should be assessed at each visit and discharge.
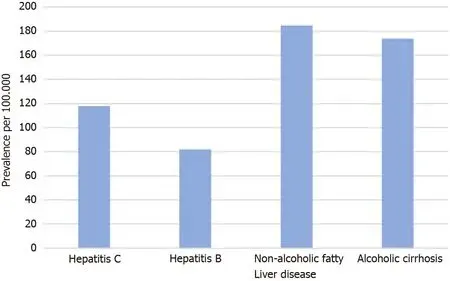
Figure 2 Prevalence of Clostridioides difficile infection in cirrhotic patients based on the etiology of cirrhosis.
Generally, women are more likely to get CDI regardless of their liver function, which was also reflected in our study[72].The incidence rate of CDI is higher in Caucasians with cirrhosis.A higher incidence and mortality rate from CDI in the caucasian population has been reported in the literature[73-75].An even higher prevalence of CDI was seen in the African American and Hispanic/Latin subgroups, which could be due to regional data differences[76].The hospitalization patterns have been fluctuating, and long-term mortality from CDI has been counterintuitively low, as concluded by recent studies[59,76,77].
Vancomycin and metronidazole have been used historically in the treatment of initial and recurrent CDI.Several meta-analyses have been performed, emphasizing the non-inferiority of metronidazole, and thereby, guidelines have been revised.Vancomycin and fidaxomicin are considered the mainstay of antibiotic treatment now, along with fecal microbiota transplantation (FMT).Surgery is pursued when there is a suspicion of toxic megacolon or colon perforation[5,17,78-82].Lactulose was also evaluated in liver cirrhosis patients carryingC.difficilein a study done by Itoet al[83] with promising results.Lactulose may increase fecal acidity by decreasing short-chain fatty acids and increasing lactate and acetate, leading to possible suppression ofC.difficilegrowth.FMT has been used in patient subgroups with cirrhosis to help with recurrent CDI colonization[78,84].Additionally, lactulose as a prebiotic may play a prominent role in restoring the hosts' indigenous microbiota and conferring resistance against CDI[85].Recently, the benefit of preventing CDI by using maintenance rifaximin[86].
The benefit of screening hospitalized cirrhotic patients forC.difficilemight be purely theoretical, as screening in the absence of symptoms would lead to over-reporting[87,88].Meltzeret al[89] did a 10-wk surveillance study after screening asymptomatic patients on admission.They demonstrated a higher incidence of CDI during hospitalization in patients who tested positive forC.difficileon admission rectal swabs.Whether clinicians should treat a prior CDI carrier state still remains unclear, as most of the positive patients in that particular study had the classical risk factors for CDI (prolonged hospital and rehabilitation stays, exposure to infections, and antibiotics).Third-generation cephalosporins are the treatment of choice for subacute bacterial peritonitis (SBP), which are counterintuitively associated with increased risk of CDI.Both SBP and CDI translate into poor outcomes for the patient[21].Bactrim and fluoroquinolones (ciprofloxacin, norfloxacin) are recommended as SBP prophylaxis in high-risk patients, but their long-term benefit is questionable for now[90].
C.difficiletoxins in stool sample or visualization of pseudomembrane formation on endoscopic or histological examination are diagnostic for CDI.Due to its ability to spread by spore formation[91,92], poor hygiene contributes to its rapid spreadviathe fecal-oral route and can result in outbreaks in health care facilities.Hand hygiene, therefore, has been the cornerstone in the control of CDI spread along with isolation of symptomatic patients and implementation of environmental sanitation protocols[93-97].
The results obtained from this database are significant due to the large sample size, appropriate gender and racial representation, and inclusion of patients above the age of twenty years.Recent studies have confirmed poor outcomes with concurrent CDI and CLD[37].All data prior to 2018 has been excluded to determine the persistence of historically established risk factors for CDI based on point prevalence.Relevant comorbidities have been included along with a subgroup of patients with liver transplants.The underlying cause of cirrhosis has also been delineated (Table 2).
The study is at a disadvantage as it is retrospective.The sample size is subjected to selection bias which was attempted to be minimized by relevant inclusion and exclusion criterion.The prevalence of liver cirrhosis in the population database is lower than the general population (0.69 %)[98].While this may reduce the effective sample size, it has no bearing on the conclusions drawn regarding the risk factors associated with CDI in cirrhotic patients.The inclusion of patient classification based on their MELD score would have indicated the severity of CDI at different cirrhosis stages.The multivariate analysis by Honget al[99] had suggested that the patients with higher MELD scoring are at increased risk of mortality from CDI (1.06 ± 0.02,Pvalue < 0.022 with an increase of 21.5% mortality rate with every five-unit increase of MELD score), and MELD scoring should be used to triage them and monitor their outcomes.However, the application of MELD score in SNOMED-CT would be scrupulous as the routine discharge diagnoses are not updated based on the patient's current MELD scores.Results from future perspective studies with patient cohorts stratified into liver, solid organ transplants and MELD classes can vindicate the yield ofC.difficilescreening in asymptomatic patients.
CONCLUSION
The prevalence of CDI is seven times higher in cirrhotic patients than those without liver cirrhosis.In the multivariate analysis, cirrhotic patients with advanced age, frequent hospitalizations, residence in a nursing home and long-term facilities, along with the use of antibiotics, acid-suppressive therapy, chronic comorbidities, and history of hepatic transplantation, were more likely to develop CDI.Further studies are needed to explore this risk, and precautionary measures are needed to be implemented to prevent CDI in this group of patients.
ARTICLE HIGHLIGHTS
Research background
Clostridium difficile (C.difficile) is one of the major causes of nosocomial diarrhea and associated morbidity and mortality.The risk factors of C.difficile are historically established.Cirrhosis is a major disease burden in the United States health care system.The risk of morbidity and mortality is higher in cirrhotic patients who acquire C.difficile infection.
Research motivation
This research was motivated by the lack of recent large population study describing the risk factors of C.difficile in liver cirrhotic patients.We also wanted to study the association in patient cohorts who underwent liver transplant as it was not done previously with such higher sample size.
Research objectives
To determine the prevalence of C.difficile infection in patients with liver cirrhosis and to establish the risk factors of C.difficile infection in patients with liver cirrhosis with special emphasis on liver transplantation cohort.
Research methods
The authors used the Explorys database to obtain data that was classified using SNOMED diagnostic codes.Prevalence and association were calculated using multivariate regression and SPS Software.Details are in the main manuscript.
Research results
The prevalence ofC.difficileinfection (CDI) amongst the liver cirrhosis population was 134.93 per 100.000vs19.06 per 100.000 in non-cirrhotic patients.The multivariate analysis model showed that cirrhotic patients were more likely to develop CDI.
Research conclusions
This research study concluded that cirrhotic patients have a significantly higher CDI prevalence, and liver cirrhosis may be an independent risk factor for CDI.
Research perspectives
There is a possibility of reducing the CDI mortality in cirrhotic patients by screening them for CDI.Future prospective studies are needed in this regard.
杂志排行
World Journal of Hepatology的其它文章
- Evolution of liver transplant organ allocation policy: Current limitations and future directions
- Antibiotic prophylaxis in patients with cirrhosis: Current evidence for clinical practice
- Kidney transplant from donors with hepatitis B: A challenging treatment option
- Unpacking the challenge of gastric varices: A review on indication,timing and modality of therapy
- Pathogenesis of autoimmune hepatitis
- Current state of endohepatology: Diagnosis and treatment of portal hypertension and its complications with endoscopic ultrasound