Current state of endohepatology: Diagnosis and treatment of portal hypertension and its complications with endoscopic ultrasound
2021-09-03SeanRudnickJasonConwayMarkRusso
Sean R Rudnick, Jason D Conway, Mark W Russo
Sean R Rudnick, Jason D Conway, Section on Gastroenterology & Hepatology, Wake Forest School of Medicine, Winston-Salem, NC 27157, United States
Mark W Russo, Department of Hepatology, Atrium Health, Carolinas Medical Center, Charlotte, NC 28204, United States
Abstract The diagnosis and management of cirrhosis and portal hypertension (PH) with its complications including variceal hemorrhage, ascites, and hepatic encephalopathy continues to evolve.Although there are established “standards of care” in liver biopsy and measurement of PH, gastric varices remain an area without a universally accepted therapeutic approach.The concept of “Endo Hepatology” has been used to describe of the applications of endoscopic ultrasound (EUS) to these challenges.EUS-liver biopsy (EUS-LB) offers an alternative to percutaneous and transjuglar liver biopsy without compromising safety or efficacy, and with added advantages including the potential to reduce sampling error by allowing biopsies in both hepatic lobes.Furthermore, EUS-LB can be performed during the same procedure as EUS-guided portal pressure gradient (PPG) measurements, allowing for the collection of valuable diagnostic and prognostic data.EUS-guided PPG measurements provide an appealing alternative to the transjugular approach, with proposed advantages including the ability to directly measure portal vein pressure.In addition, EUS-guided treatment of gastric varices (GV) offers several possible advantages to current therapies.EUS-guided treatment of GV allows detailed assessment of the vascular anatomy, similar efficacy and safety to current therapies, and allows the evaluation of treatment effect through doppler ultrasound visualization.The appropriate selection of patients for these procedures is paramount to ensuring generation of useful clinical data and patient safety.
Key Words: Portal hypertension; Endoscopic ultrasound; Liver biopsy; Gastric varices
INTRODUCTION
Chronic liver disease (CLD) continues to represent a substantial healthcare burden, with an estimated 1.5 billion persons affected worldwide.Since 2000 there has been a 13% increase in incidence of CLD and cirrhosis, in addition to increasing prevalence and mortality of cirrhosis in the United States.Moreover, the epidemiology of CLD is shifting from viral hepatitis to an increasing prevalence of liver disease caused by metabolic syndrome and alcohol misuse[1].
Accompanying the increase in cirrhosis is the development of portal hypertension (PH); resulting in the majority of its complications including ascites, variceal hemorrhage, and encephalopathy.Clinically, cirrhosis is often dichotomized into compensated (absence of portal hypertensive complications) and decompensated (presence of portal hypertensive complications), with decompensated cirrhosis portending a poor prognosis[2].
A diagnosis of PH typically requires invasive testing to measure the gradient between the hepatic sinusoids and the hepatic vein (which is the outflow tract of the liver), termed the hepatic venous pressure gradient (HVPG) (Figure 1).PH is present if HVPG > 5 mmHg, with clinically significant PH (CSPH) defined as > 10 mmHg associated with the development of clinical complications (hence its designation) including variceal hemorrhage and ascites.HVPG is an independent prognostic variable, with a 3% increase in mortality risk for each 1 mmHg gradient increase[3].
Accompanying the increasing burden of CLD has been the need for safe, accurate, and cost-effective diagnostic modalities to appropriately classify patients requiring additional therapeutic interventions.Classically liver biopsy; percutaneous liver biopsy (PC-LB) and transjugular liver biopsy (TJ-LB) was utilized to assess the etiology and severity (fibrosis stage) of liver disease by histology.Additionally, invasive measurement of the HVPGviathe transjugular venous route in interventional radiology (IR) could be utilized to obtain additional prognostic data in appropriate circumstances.Noninvasive modalities, such as elastography or serologic markers, have been developed as alternatives to liver biopsy[4].
The concept of “Endo-hepatology” was introduced in 2012 as an area of integration or overlap of endoscopic procedures within the practice of Hepatology[5].In this review we focus on two diagnostic modalities including endoscopic ultrasound (EUS) guided liver biopsy (EUS-LB) and EUS-guided measurement of PH, and one therapeutic application; EUS-guided management of gastric varices (GV).
Hepatologists should have a fundamental understanding of the similarities and differences in techniques between current clinical standards of practice and EUSguided modalities, while also recognizing opportunities to appropriately implement EUS-guided diagnostics and therapeutics into their practice.An in depth review of EUS anatomy, devices, and techniques is outside the purview of this review.
LIVER BIOPSY
Once considered the cornerstone in the evaluation and management of liver disease, the role and modalities of liver biopsy has evolved substantially over the past decade.The evolution of noninvasive testing coupled with concerns regarding the cost and risk of liver biopsy has brought into question the exact role of liver biopsy in the early 21stcentury[4].At present, liver biopsy is still considered appropriate for establishing diagnosis, evaluating stage of liver disease (fibrosis), and directing management decisions[6].
Traditionally, liver biopsy has been performed through percutaneous, transjugular, or surgical approaches.At present, image-guided liver biopsy (“real time” or marking) has become the de facto standard of care in most centers, replacing the palpation/ percussion guided technique[7].Because the diagnosis, grading, and staging of liver disease is dependent upon adequate sample size, it is recommended that the length of the sample is at least 2-3 cm and 16-gauge in caliber (or wider), ideally with ≥ 11 portal tracts for evaluation[6].Complications related to liver biopsy include pain (30%-50% patients)[8], serious bleeding (0.6%)[9], injury to other organs (0.08%)[10], and rarely death (0.1%)[6] (Figure 2).
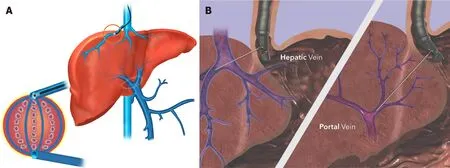
Figure 1 Comparison of modalities for measuring portal hypertension.
Since its first description in 2007, publications describing experience with EUS-LB have continued proliferate[11].Proposed advantages to EUS-LB include more precise localization and characterization of the target tissue, ability to biopsy both lobes of the liver, decreased invasiveness, improved patient tolerance, decreased recovery time, and decreased complications[12].Acknowledged disadvantages include increased technical difficulty and higher cost compared to other available methods.
A single center retrospective study compared the safety and efficacy of “standard of care” [PC-LB (n= 287) & TJ-LB (n= 91)] to EUS-LB (n= 135).There were no statistically significant differences between modalities in regards to rates of adverse events, technical success rate, and diagnostic adequacy.Notably, the number of complete portal tracts for analysis and mean specimen length (two metrics for assessing specimen adequacy) were higher in the EUS-LB group compared to PC-LB and TJ-LB[13].These results support comparable safety profile and diagnostic adequacy (i.e.,noninferiority) of EUS-LB to current standard of care liver biopsy modalities.
In 2019 a systematic review and meta-analysis that included eight studies with a total of 437 patients reported the efficacy and safety of EUS-LB biopsy[14].The primary analysis focused on diagnostic yield; specifically addressing successful histologic diagnosis and frequency of insufficient histologic sample size.A second analysis described pooled rates of all adverse events.A subgroup analysis was performed regarding needle type used for biopsy [core needlevsfine-needle aspiration (FNA) needle].A 19-gauge needle was used in all included studies.Indications for liver biopsy included abnormal liver tests, non-alcoholic steatohepatitis, cholestasis, primary sclerosing cholangitis, cirrhosis, and congestive heart failure.
The pooled rate of successful histologic diagnosis was 93.9% and the pooled insufficient specimen rate was 10.1%.The pooled rates of adverse events and bleeding were 2.3%, and 1.2%, respectively.In the subgroup analysis, the only statistically significant difference between core needle and FNA needle was obtaining insufficient specimen, which occurred in 20% of patients biopsied with core needle compared to 4% of patients biopsied with FNA needle (P= 0.03).The authors concluded that FNA needles provide better specimens and have improved diagnostic outcomes compared to other core needle biopsies, though they acknowledged significant heterogeneity in the overall analysis.

Figure 2 Proposed algorithm for choosing suitable modality for liver biopsy.
Despites its limitations, the study by Mohanet al[14] provides robust data describing the performance characteristics and technical considerations (needle device choice) of EUS-LB.The safety profile of “standard of care”; (PC-LB or TJ-LB) was compared head-to-head in a propensity score matched analysis of 978 patients who underwent PC-LB compared to 489 undergoing TJ-LB.Hematomas developed in 1.2% of patients undergoing PC-LB compared to 0.2% with TJ-LB (P= 0.049).Cardiac complications occurred more frequently in TJ-LB compared to PC-LB (0.4%vs0%;P= 0.045).There were no significant differences in other adverse events or complications[15].
Ultimately, multiple factors influence the choice of liver biopsy modality, and the decision should be made on a case-by-case basis.A seemingly pertinent use of EUSLB, is in patients with discordant noninvasive testing in whom the goal is to exclude cirrhosis and/or PH, as direct measurements of portal pressures can also be performed simultaneously and biopsies from both lobes can be obtained.With discordant noninvasive testing, accurate fibrosis staging by liver biopsy is paramount.Indeed, it has been demonstrated in patients with NAFLD, biopsies performed on the same day characterized 35% of patients with advanced fibrosis on one sample, while the other sample from the same day did not suggests significant fibrosis[16].This discordance is of profound significance and directly influences clinical decision-making.As PC-LB and TJ-LB typically sample one hepatic lobe, obtaining “bilobar” biopsies by EUS-LB provides a potential advantage to minimize the risk of misclassifying fibrosis stage.
MEASUREMENT OF PH
Although invasive and considered the gold standard in assessment of PH, HVPG is in fact an indirect method of measurement[17].Calculation of the HVPG includes measuring the free hepatic venous pressure (FHVP) and wedged hepatic venous pressure (WHVP; typically wedged pressure in the right hepatic vein).The transduced wedged hepatic venous pressure estimates sinusoidal pressure.The difference between the WHVP and FHVP is the estimated portosystemic gradient[18].Conceptually, this is analogous to Swan-Ganz catheterization in the pulmonary artery.
In the absence of fibrosis/nodules (i.e.cirrhosis), the pressure equalizes throughout the interconnected sinusoidal network, and results in minimal gradient (i.e.,normal; up to 4 mmHg).Thus, it does not provide useful information regarding prehepatic or presinusoidal PH (i.e., non-cirrhotic causes of PH).In the presence of cirrhosis, the WHVP is an accurate surrogate for portal vein pressure, allowing calculation of the gradient by the equation: WHVP-FHVP = HVPG.As previously outlined, HVPG has significant prognostic value in predicting poor outcomes in patients with PH[3].
In comparison, EUS-guided portal pressure gradient (PPG) measurements employ a direct sampling technique.Thus, the direct measurement of the portal vein pressure could be considered the gold standard because it is not an estimate of sinusoidal pressure as is WHVP.The difference in the mean measurement of these pressures is termed the PPG which is analogous to the HVPG, with the caveat that direct portal vein measurement also allows for the assessment of prehepatic/presinusoidal PH; a limitation of the transjugular approach.
In 2016, Huanget al[19] published their experience in a porcine animal model with a novel EUS-guided system which included a manometer attached to a 25-gauge FNA needle for directly measuring pressures in the hepatic and portal veins.The purpose of this animal study was to assess clinical feasibility and assess correlation with the standard of care; HVPG measurement through transjugular approach[19].
In a pilot study, 28 patients between the age of 18-75 years with a history of liver disease or suspected cirrhosis underwent EUS-PPG measurements utilizing the technique and equipment in the animal study.The portal vein and hepatic vein were targetedviaa transgastric-transduodenal approach (IVC was substituted for hepatic vein when not technically feasible).Feasibility was defined as the technical success of obtaining pertinent measurements.Safety was assessed by postprocedural interview and telephone call 48 h following procedure.As correlation to the standard of care (transjugular HVPG) was obtained in animal studies, clinical parameters of PH were evaluated in each patient.Exclusion criteria included pregnancy, international normalized ratio (INR) > 1.5, platelet count < 50000, active GI bleeding, and post sinusoidal PH[20].
Technical success rate of EUS-PPG measurement was 100% without any adverse events.PPG measurements had excellent correlation with clinical parameters of PH.Mean PPG in patients with varices was 14.37 mmHg, compared to 4.26 mmHg in patients without varices (P= 0.0002); which is consistent with criteria that gradients ≥ 10 mmHg (i.e., CSPH) are associated with the development of varices.The authors concluded that EUS-PPG measurement was a safe and feasible alternative to currently available diagnostics[20].
There are obvious limitations of this pilot study which may limit widespread generalizability of this technique.The exclusion of patients with INR > 1.5 and inclusion of only 4 patients with INR > 1.2 (especially with the knowledge that INR is a poor predictor of procedural bleeding risk in patients with cirrhosis) is a major limitation of this small pilot study[21].
Results of this pilot study ultimately led to the Food and Drug Administration approval of the EchoTip Insight portosystemic pressure gradient measurement system (Cook Medical, Winston-Salem, NC, United States) in 2019 (Figure 1).Following approval, multiple centers have begun utilizing this method.Registry data are eagerly anticipated to assess the feasibility, utility, and safety profile of this method outside the realm of small pilot study/clinical trials.
One of the challenges facing any new technology, including EUS-PPG measurement is identifying the appropriate clinical application.Despite the useful prognostic information it provides, in current clinical practice, obtaining the polysomnography is not considered standard of care in many areas due to its invasiveness, cost, and limited availability[2].With the exception of Transjugular intrahepatic portosystemic shunt (TIPS) and TJ-LB in the authors’ experience, HVPG measurements are not routinely obtained.
A potential role of EUS-PPG measurements in current practice would be to supplant the transjugular approach for HVPG/biopsy, and reserve the latter approach for patients undergoing TIPS and in those with more severe coagulopathy.Furthermore, the additional evidence gleaned during the endoscopic evaluation (i.e., presence/absence of varices or portal hypertensive gastropathy) would have treatment implications.Whether the combination of EUS-PPG measurements (with or without simultaneous liver biopsy) can be routinely incorporated during evaluation of patients with cirrhosis remains to be seen.
TREATMENT OF GV
There is significant heterogeneity in the location, vascular anatomy, bleeding risk, and response to treatment of GV.The Sarin classification has been the most commonly used for risk stratification and management, however it is limited to describing endoscopic anatomy, and does not necessarily reflect the underlying vascular anatomy of GV; which has significant treatment implications[22,23].
A proposed algorithm for the treatment of acute GV bleeding suggests utilizing variceal band ligation for treatment of gastroesophageal varices (GOV) 1 (i.e.,treat as esophageal varices), while utilizing injection therapies (i.e.,tissue adhesives such as cyanoacrylate) in the management of GOV2 and isolated gastric varices 1 (IGV1) (together known as “cardiofundal varics”)[24].At present, therapeutic options for treatment of GV hemorrhage include endoscopic injection of tissue adhesives (viaEGD or EUS), TIPS, and BRTO.It has been suggested that EUS-guided therapy of GV is superior to endoscopic injection as it decreases the rate of rebleeding[25].
In 2000, Leeet al[26] published their results of a prospective study utilizing cyanoacrylate and lipiodol injection in the management of bleeding GV[26].In this study 38% of patients had GOV2 and 27% patients had IGV1.After initial bleeding was controlled, 47 patients received “on demand” therapy if bleeding recurred, while 54 patients underwent biweekly EUS with injection until obliteration of varices was confirmed.Although early rebleeding rates (defined ≤ 48 h) were similar between both groups, the recurrence of late bleeding (> 48 h) was significantly reduced in the repeat injection group (18.5%vs44.7%,P= 0.0053).
A randomized trial evaluated prevention of first GV bleed (primary prophylaxis)[27].In a study of 89 patients with large (≥ 10 mm) GOV2 and IGV1, patients were randomized to endoscopic cyanoacrylate glue injection, nonselective beta blocker (NSBB), and observation.Overall, cyanoacrylate injection was associated with lower bleeding rates (10%) than NSBB (38%), and observation (53%).Survival was similar in the cyanoacrylate (93%), and NSBB group (83%), but higher compared to the observation group (74%).Of note, only 15% of patients in the study had IGV1.This study formed the basis for recommendation of NSBB for primary prophylaxis of GV hemorrhage in GOV2 and IGV1.
The management of active hemorrhage from GV remains a significant clinical challenge.A meta-analysis comparing cyanoacrylate glue injection to endoscopic band ligation demonstrated similar results for initial hemostasis, but favored cyanoacrylate injection for prevention of rebleeding[28].Limitations of this meta-analysis included variable quality of evidence, and heterogeneity in type of varices treated.
The addition of endovascular coils to cyanoacrylate glue injection has been proposed to reduce the risk of systemic embolization, a rare but potentially fatal complication[29,30].A single center retrospective study of 152 patients specifically addressed the use of coil injection and cyanoacrylate glue in patients with cardiofundal varices; 94% of whom had IGV1.Over a 6-year period, 5% of patients treated had active hemorrhage, while 69% had evidence of recent bleeding (i.e.,treatment constituted secondary prophylaxis).Technical success rate was 99%.Follow-up EUS examinations were available for 100/152 patients.Complete obliteration of varices based on Doppler was confirmed in 93%, and bleeding from obliterated varices occurred in 3% of patients.The authors concluded that combination of therapy with cyanoacrylate and coil embolization is highly effective for hemostasis and active bleeding, and for primary and secondary prophylaxis with minimal adverse effects.
A systematic review and meta-analysis compared combination therapy (cyanoacrylate + coils) to monotherapy with (cyanoacrylate alonevscoil alone or non-cyanoacrylate treatment)[31].Eleven studies were included (n= 536) which included 2 randomized control trials, one prospective study, and 8 retrospective studies.Measured outcomes included technical success, clinical success, adverse events, and rate of rebleeding/or intervention.Subgroup analysis compared 3 treatment cohorts; EUS- guided cyanoacrylate injection/EUS-guided coil embolization + cyanoacrylate injection/EUS-guided coil injection alone) (Table 1).
Overall technical success of EUS-guided therapies was 100%, clinical success was 97%, and adverse events were 14%.In the subgroup analysis (Table 2), combination therapy resulted in better technical success (100%) and clinical success (98%) compared to monotherapy with cyanoacrylate alone (97% and 96%, respectively) or coil embolization alone (99% and 90%, respectively).Combination therapy also resulted in lower adverse event rates (10%) compared to monotherapy with cyanoacrylate alone (21%), and coil embolization alone (3%).The authors concluded that EUS-guided treatment is safe and effective, and that combination therapies should be the preferred strategy for management of GV.
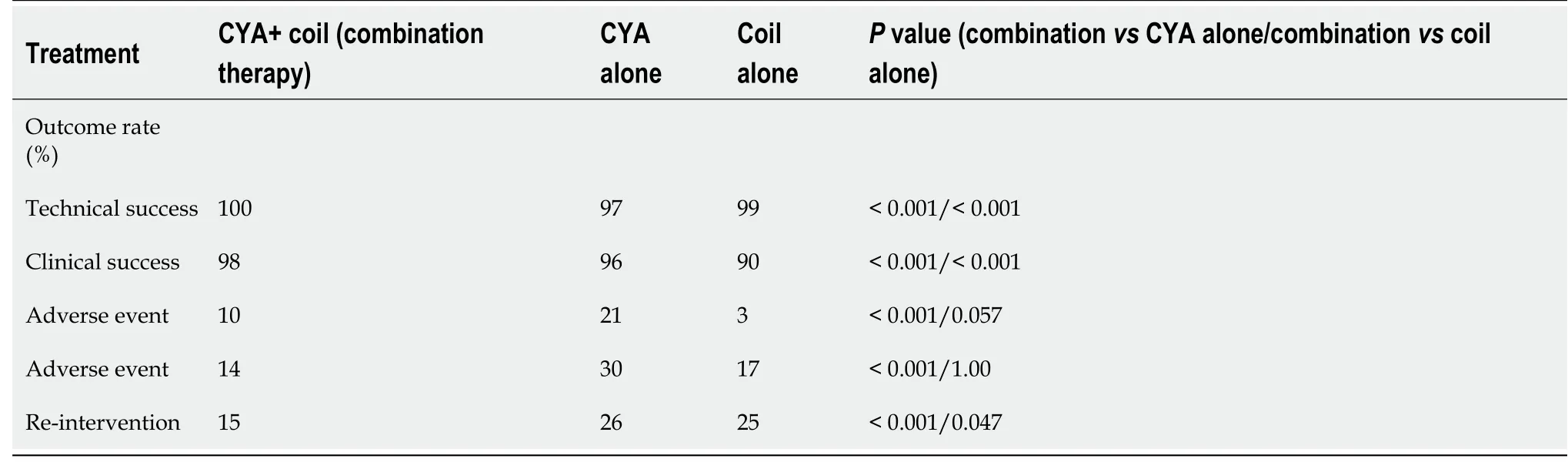
Table 1 Comparison of endoscopic ultrasound-guided treatment modalities for gastric varices; combination therapy vs monotherapy[31]

Table 2 Relative advantages and disadvantages of liver biopsy modalities
Based upon current treatment algorithms, and understanding the limitations of currently available data, EUS-guided treatment for GV should be reserved for cardiofundal varices.The main advantages of this approach include acute hemostasis and prevention of rebleeding.Furthermore, the use of EUS allows delineation of the vascular anatomy of the variceal complex, which can enable precise delivery of therapy into the varix lumen or afferent vessel (potentially decreasing the risk ofembolization) and allow confirmation of vessel obliterationviaDoppler examination[32-34].Cyanoacrylate is off-label for the treatment of GV hemorrhage in the United States, so its use should be limited to centers with appropriately trained endoscopists and experience[2,35].
CONCLUSION
EUS-guided interventions for the diagnosis and management of PH and its complications have evolved from a novel innovation into a useful clinical tool with a growing evidence-base supporting its role.
Available data suggests that EUS-LB results in comparable diagnostic adequacy (i.e.,tissue specimen) to currently available options with similar low rates of adverse events[14].Measurements of PPG correlate with HVPG measurements and have a similar safety profile[19,20].An additional benefit is the direct measurement of the portal vein pressure, allowing diagnosis of prehepatic/presinusoidal PH that is not obtained during HVPG measurements as well as the ability to perform liver biopsy.EUS- treatment for GV bleeding may be more effective than current endoscopic therapies, and offers several potential advantages[25,31].
EUS-guided interventions have demonstrated similar efficacy and safety to current standards of care, and should be viewed as a complement (not a replacement) to current diagnostic and therapeutic modalities.A multidisciplinary approach between Hepatologists and EUS-trained endoscopists is vital to ensure appropriate patient selection, ensure accurate and useful data are generated from diagnostic procedures, and that maximal therapeutic benefit is derived from EUS-guided treatments.
ACKNOWLEDGEMENTS
The authors wish to thank Cook Medical Endoscopy (Winston-Salem, NC) for their generous sharing of medical illustrations used in the preparation of this manuscript.
杂志排行
World Journal of Hepatology的其它文章
- Evolution of liver transplant organ allocation policy: Current limitations and future directions
- Antibiotic prophylaxis in patients with cirrhosis: Current evidence for clinical practice
- Kidney transplant from donors with hepatitis B: A challenging treatment option
- Unpacking the challenge of gastric varices: A review on indication,timing and modality of therapy
- Pathogenesis of autoimmune hepatitis
- Therapeutic plasma exchange in liver failure