Arantius’ ligament approach for the laparoscopic left hemihepatectomy
2021-07-24XueHuiChuYaKuanZhaoXiaoDongShanYuanYuanSunYuZeShiXiTaiSun
Xue-Hui Chu ,Ya-Kuan Zhao ,Xiao-Dong Shan,Yuan-Yuan Sun,Yu-Ze Shi,Xi-Tai Sun
Department of General Surgery, Affiliated Drum Tower Hospital, Medical School, Nanjing University, Nanjing 210 0 08, China
In recent years,the technique of laparoscopic hepatectomy has been developed rapidly,and its indications are approximately equal to open surgery [ 1,2 ].Laparoscopic left hemihepatectomy (LLH)has become a mature and standardized operation [ 3,4 ],and there are many reports on the relevant surgical paths and norms [5-7].Herein,the Arantius’ ligament approach for the LLH is proposed,which provides a reference for the standardized path of LLH.
Between March 2015 and June 2018,18 consecutive patients(11 females and 7 males) undergoing LLH were selected as the study subjects.The median patient age at the time of resection was 51.5 years (range,40–69 years).Inclusive criteria: 1) patients aged from 18 to 70 years; 2) liver function was classified as Child-Pugh A; 3) the lesions were located in the left lobe of liver and were surgically resectable; and 4) all patients underwent Arantius’ ligament approach for the LLH.Exclusive criteria: 1) patients with other liver diseases such as severe cirrhosis; 2) patients with infectious diseases,cardiovascular diseases or systemic immune diseases; and 3) laparoscopic operation was converted to open operation.
Trocars were placed by the conventional five-hole method( Fig.1 ).Both the main operational holes and the observational hole were 12 mm,and the auxiliary operational holes were 5 mm.The abdominal cavity was probed after entering the abdomen and portal pre-occlusion band was placed.Firstly both sides of the left Glissonian pedicle were dissected ( Fig.2 ).Then,a curved laparoscopic instrument (Goldfinger dissector or the Endo Retract Maxi)was used to pass through the dissected space above the Arantius’ ligament,and the left hepatic pedicle was transected with endoscopic stapling system.Secondly,the second hepatic hilum was dissected to expose the left hepatic vein (LHV) ( Fig.3 ).The root of LHV was found by dissecting the cephalic side of Arantius’ ligament,of which the posterior and left side were dissected and exposed.The LHV was encircled with right-angle forceps and then pulled by a vascular sling.Subsequently,liver parenchyma was transected along the plane between the Arantius’ ligament and middle hepatic vein (MHV),and the trunk of MHV was then gradually exposed ( Fig.4 ).Finally,the liver parenchyma was separated along the plane of the hepatic ischemia line and the MHV,after the LHV was transected with endoscopic stapling system,and the specimen was resected completely.Left liver lobe was taken out and hepatic stump was examined.After confirming that there was no bleeding or bile leakage,a drainage tube was placed.
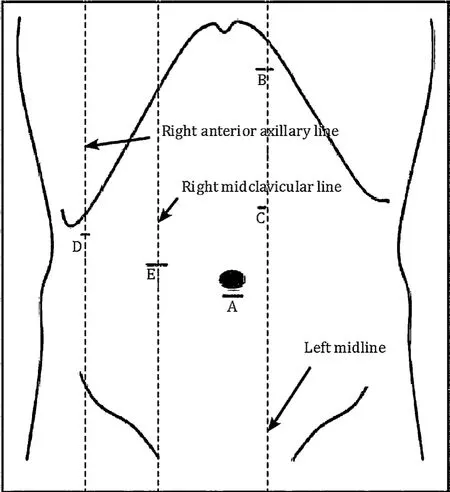
Fig.1.Trocars were placed by the conventional five-hole method.A: Observational hole; B: Main operational hole; C: Auxiliary operational hole (the midpoint of A and B); D: Assistant’s auxiliary operational hole; E: Assistant’s main operational hole.

Fig.2.Treatment of the left hepatic pedicle through Arantius’ ligament approach.A: Dissection of the right side of the left hepatic pedicle; B: dissection of the left side of the left hepatic pedicle above the Arantius’ ligament; C: the left Glissonean pedicle encircled extrahepatically through the dissected space with a Goldfinger dissector; D:transection of the hepatic pedicle with Endo-GIA.

Fig.4.Exposure of the MHV through Arantius’ ligament approach.A: Exposure of the root of LHV; B: the root of MHV; C: the liver parenchyma from the cephalic side to the caudal side was separated along the Arantius’ ligament; D: exposure of the trunk of MHV.LHV: left hepatic vein; MHV: middle hepatic vein.
The general data of patients were observed and recorded,including sex,age,diagnosis,as well as the perioperative indicators of patients.The incidence of complications including biliary fistula,incision infection,pleural effusion,refractory ascites and lung infection was analyzed.
General characteristics were shown in Table 1.There were 12 cases of hepatolithiasis,3 cases of hepatic hemangioma,2 cases of hepatocellular carcinoma,and 1 case of intrahepatic cholangiocarcinoma.All patients underwent the Arantius’ ligament approach for the LLH,with median operative time of 195 min,median intraoperative blood loss of 200 mL,intraoperative blood transfusion performed in 3 cases (200,300,and 600 mL,respectively).Median postoperative hospital stay was 7 days.No postoperative complications occurred and no patient died.Median alanine aminotransferase on the first day after surgery was 140.8 U/L,aspartate transaminase was 68.5 U/L,white blood cell was 9.6 × 109/L,and C-reactive protein was 48.4 mg/L,which indicated that the patients only had mild liver damage and low surgical stress response.
With the development of endoscopic techniques,laparoscopic hepatectomy has made great progress in recent years.However,there are two main problems at present: the control of intraoperative bleeding,and the identification of surgical plane.
Bleeding control is important in LLH.Glissonean pedicle transection is a good method to control the blood inflow and the left hepatic pedicle could be dissected easily according to the Arantius’ligament,whose caudal end is attached to the angle part of the left portal vein [8].However,it is not suitable for patients with the right posterior hepatic duct branched from the left hepatic duct.Dissection and exposure of the LHV is important to identify the root of MHV and control the outflow.It is a feasible method to search for the root of LHV by dissecting along the Arantius’ ligament,whose cephalic end is often attached to LHV [9].And then the liver parenchymal dissection starts from the root side of the MHV and moves towards the peripheral side,which can avoid major split vein injury.However,for some patients with short extrahepatic segment of LHV or long common trunk of LHV and MHV,the dissection and exposure of the LHV was dangerous and unnecessary.In our study,most patients’ blood loss was less than 200 mL,and only 3 patients (16.7%) received intraoperative blood transfusion due to severe inflammation and low pre-operational hemoglobin.
Identification of surgical plane is another problem in LLH.To identify the surgical planes,the MHV must be firstly found.The root of the MHV can be easily exposed when the LHV was dissected,then the trunk of MHV could be exposed gradually from the cephalic side to the caudal side by separating the liver parenchyma between the left lobe and caudate lobe along the Arantius’ ligament.In this way,the trunk of MHV could be easily exposed and the other plane between the MHV and Arantius’ligament could be easily identified.
In conclusion,the Arantius’ ligament is a very important anatomical marker in LLH because of its unique anatomical characteristics.Through the dissection of the cephalic and caudal edge of the Arantius’ ligament,the blood flow in and out of the liver can be well controlled and pretreated.Through the dissection of the anatomical plane on which the ligament lies,the left lobe and caudate lobe can be well separated and the MHV can be exposed.Arantius’ ligament approach for the LLH can control intraoperative bleeding well and identify the surgical plane easily,which can be used as a new path for the standardization and routinization of LLH.
Acknowledgments
None.
CRediTauthorshipcontributionstatement
Xue-HuiChu:Conceptualization,Formal analysis,Data curation,Methodology,Writing - original draft.Ya-KuanZhao:Formal analysis,Visualization,Writing - original draft.Xiao-DongShan:Investigation,Software.Yuan-YuanSun:Data curation,Software.Yu-ZeShi:Data curation,Software.Xi-TaiSun:Project administration,Resources,Supervision,Validation,Writing - review & editing.
Funding
None.
Ethicalapproval
This protocol was approved by the Research Ethics Committee of Drum Tower Hospital.Informed consent was obtained from each patient,and the study protocol was conformed to the ethical guidelines of the 1975DeclarationofHelsinki.
Competinginterest
No benefits in any form have been received or will be received from a commercial party related directly or indirectly to the subject of this article.
杂志排行

Hepatobiliary & Pancreatic Diseases International的其它文章
- Cross-talk between hepatic stellate cells and T lymphocytes in liver fibrosis
- Diabetes mellitus is a risk factor of acute kidney injury in liver transplantation patients✩
- Hepatobiliary&Pancreatic Diseases International
- Application of machine learning models for predicting acute kidney injury following donation after cardiac death liver transplantation
- Postoperative adjuvant transcatheter arterial chemoembolization improves the prognosis of patients with huge hepatocellular carcinoma
- The effects of stereotactic body radiotherapy on peripheral natural killer and CD3 + CD56 + NKT-like cells in patients with hepatocellular carcinoma