Changes in the nutritional status of nine vitamins in patients with esophageal cancer during chemotherapy
2021-05-25LanQingLiangLingLingMengBoNingCaiZePingCuiNaMaLeHuiDuWeiYuBaoLinQuShengQiangFengFangLiu
Lan-Qing Liang, Ling-Ling Meng, Bo-Ning Cai, Ze-Ping Cui, Na Ma, Le-Hui Du, Wei Yu, Bao-Lin Qu, Sheng-Qiang Feng, Fang Liu
Abstract
Key Words: Esophageal cancer; Chemotherapy; Vitamins; Nutritional status; Body mass index
INTRODUCTION
Esophageal cancer (EC) is the ninth most commonly diagnosed cancer and the sixth leading cause of cancer death worldwide[1]. The incidence and mortality rates of EC are highly heterogeneous in terms of gender, histological type, geographic distribution and race[2]. The morbidity and mortality of EC in China are higher than the global averages[3]. Chemoradiotherapy remains the mainstay of treatment for patients with advanced EC. The most common complications during chemoradiotherapy in EC patients include weight loss, malnutrition, bone marrow suppression, electrolyte disturbances, hypoproteinemia and decreased quality of life[4 -7 ]. Multiple vitamins are involved in the pathogenesis, progression and prognosis of tumors and are closely related to the tumor microenvironment. Vitamin testing is valuable in tumor patients as it can identify whether there is a specific vitamin deficiency and/or justify vitamin therapy. Most clinical studies have shown that vitamin nutritional status varies greatly in tumors of different systems[8]. Although many studies have investigated the relationships between vitamins B, A, D and C with EC, most of these studies focused on the roles of vitamins in the prevention and treatment of EC. Few studies have examined the changes in vitamin nutritional status and their influencing factors before and after chemotherapy for EC.
Many vitamins have antitumor effects and are closely related to the occurrence,progression, prognosis and recovery of tumors. Vitamin supplementation can lower the risk of tumorigenesis and prevent abnormal DNA methylation changes in tumor cells[9]. With the advances in nutritional therapy in China, nutritional screenings,assessments and interventions have increasingly been applied in tumor patients. The standardized nutritional therapies involve three major macronutrients including carbohydrates, proteins and fats and have specific requirements on micronutrients.Nutritional therapy for tumor patients provides nutrients and energy and focuses on the metabolism-regulating roles of nutrients[10 ]. Vitamin supplementation is a common nutritional therapy for tumor patients in clinical practice. Serum vitamin levels vary among patients with different tumors. Zhanget al[11 ] analyzed the vitamin nutritional status of approximately 1000 hospitalized tumor patients and found that vitamin B1 concentrations were low in patients with digestive system tumors such as EC and gastric cancer. A study on postoperative nutritional deficiencies in patients with EC or gastric cancer revealed that the incidence of ferritin, folic acid, vitamin B12 and vitamin D deficiencies was 42 .86 %, 9 .52 %, 6 .35 % and 36 .67 %, respectively, and the vitamin levels were significantly improved after nutritional interventions[12 ]. In another study[13 ], most patients with advanced tumors had vitamin (particularly vitamins D, B6and C) deficiency symptoms during palliative care, and further analysis revealed a correlation between the degree of vitamin deficiency and clinical discomfort in these patients. Most vitamins were found to be negatively associated with the risk of colorectal and gastric cancer in addition to EC in an observational study, yet interventional treatment failed to demonstrate a clear preventive effect in these malignancies[14 ].
In the current study, we analyzed the effects of chemotherapeutic drugs on EC patients’ vitamin levels and hematological indicators by detecting the changes in nine vitamins and hematological indicators (e.g., hemoglobin, total protein, serum albumin and electrolytes) before and after chemotherapy, with an attempt to provide evidence for clinical vitamin supplementation and nutritional therapies. Our findings may be valuable for the implementation of tailored nutritional interventions, which will help to reduce chemotherapy-related complications, alleviate treatment resistance and improve chemotherapy efficacy.
MATERIALS AND METHODS
Subjects
In total, 203 EC patients (181 men and 22 women) aged 37 -78 yrs (mean: 60 .03 ± 7 .95 years) who were receiving chemotherapy in our center between July 2017 and September 2020 were enrolled in this study. The vast majority of subjects had esophageal squamous cell carcinoma (n= 192 , 94 .58 %), and 166 patients (81 .77 %) were in stage III-IV (Table 1 ). The inclusion criteria were as follows: (1 ) pathologically confirmed esophageal malignancies, with indications for chemotherapy, regardless of gender; (2 ) aged 18 -80 years; (3 ) an expected survival of > 6 mo; and (4 ) a Karnofsky performance status score of ≥ 70 points. The exclusion criteria included: (1 ) contraindications to chemotherapy; (2 ) coexisting tumors in other systems; (3 ) coexisting primary blood diseases or endocrine diseases; (4 ) coexisting cardiopulmonary dysfunction; and (5) coexisting psychiatric disorders.
Methods
Determination of vitamin concentrations and hematological indicators:Vitamin levels were measured using electrochemiluminescence with an LK3000 VI vitamin detector (Tianjin Lanbiao Electronic Technology Development Co., Ltd., Tianjin,China) pre- and postchemotherapy in EC patients. The normal thresholds were as follows: hemoglobin: 137 -179 g/L in males and 116 -155 g/L in females; total protein:55 -88 g/L; serum albumin: 35 -50 g/L; blood calcium: 2 .09 -2 .54 mmol/L; blood phosphorus: 0 .89 -1 .60 mmol/L; vitamin A: 0 .52 -2 .20 mmol/L; vitamin D: 25 -200 nmol/L; vitamin E: 10 -15 mg/mL; vitamin B9 : 6 .8 -36 .3 nmol/L; vitamin B12 : 200 -900 pg/mL; vitamin B1: 50 -150 nmol/L; vitamin C: 34 -114 mmol/L; vitamin B2 : 4 .26 -18 .42 mg/L; and vitamin B6: 14 .6 -72 .9 nmol/L.
Chemotherapy regimens:Of these 203 EC patients, 168 were treated with induction chemotherapy, 15 with postoperative adjuvant chemotherapy and 20 with postrelapse chemotherapy. The specific regimens were as follows: (1 ) squamous cell carcinoma:paclitaxel + platinum; (2 ) adenocarcinoma: oxaliplatin + fluorouracil; and (3 ) small cellcarcinoma: etoposide + platinum. All of these regimens were repeated every 3 wk.

Table 1 Baseline data of esophageal cancer patients (n = 203 )
Statistical methods
SPSS 24 .0 statistical software was used for analyzing the data. Normally distributed data were expressed as mean ± SD, and intergroup comparisons were based on the paired-samplet-test. Non-normally distributed data were expressed as quartiles and medians, and the rank sum test was applied for comparisons between two groups. The Spearman method was used to test for correlations between the changes in multiple vitamin serum concentrations (the independent variables) and body mass index (BMI)(the dependent variable) during chemotherapy using.Pvalue < 0 .05 was regarded as statistically significant.
RESULTS
Variation in BMI and hematological parameters in EC patients during chemotherapy
BMI declined after chemotherapy in 133 cases (65 .52 %). The number of patients with anemia increased from 119 before chemotherapy to 182 after chemotherapy. The differences in these proportions were statistically significant (P< 0 .05 ) (Table 2 ).
Vitamin levels in EC patients pre- and postchemotherapy
Vitamin A, C, B2and B6 concentrations significantly differed before and after chemotherapy (allP< 0 .05 ) (Table 3 ).

Table 2 Changes in body mass index and hematological indicators in esophageal cancer patients before and after chemotherapy [n(%)]
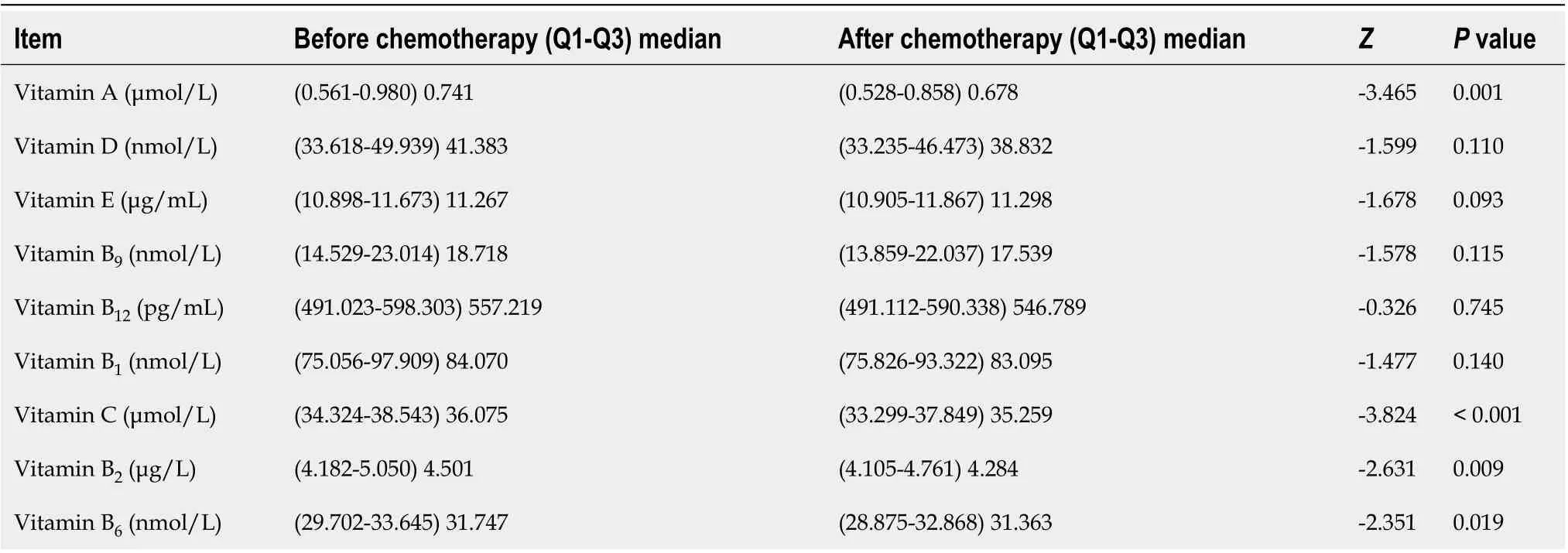
Table 3 Vitamin concentrations in esophageal cancer patients before and after chemotherapy
Vitamin deficiencies in EC patients undergoing chemotherapy
Deficiencies of vitamin A, D, C and B2were detected pre- and postchemotherapy, and the proportion of each of these four vitamin deficiencies increased after chemotherapy.In particular the proportions of vitamin C and B2deficiencies (24 .46 % vs 38 .85 %)increased significantly (bothP< 0 .05 ) (Table 4 ). Three EC patients had excessively high vitamin A concentrations before chemotherapy, which decreased to normal levels in 2 cases and to vitamin A deficiency in 1 case after chemotherapy. None of the other five vitamin (E, B9, B12 , B1 , B6 ) deficiencies were detected during chemotherapy.
Changes in hematological indicators in EC patients pre- and postchemotherapy
Hemoglobin, total protein, serum albumin and blood calcium concentrations significantly decreased, and blood phosphorus concentrations significantly increased after chemotherapy (allP< 0 .05 ) (Table 5 ).

Table 4 Vitamin deficiencies in esophageal cancer patients before and after chemotherapy, n (%)

Table 5 Changes in hematological indicators in esophageal cancer patients before and after chemotherapy
Factors affecting vitamins and hematological indicators in EC patients
After adjustment for covariates of each indicator before chemotherapy, vitamin A levels after chemotherapy showed a significant difference between males and females.Vitamin D levels after chemotherapy showed a significant difference among different tumor grades (bothP< 0 .05 ). No statistically significant differences were shown for the other baseline data (allP> 0 .05 ) (Table 6 ).
Correlation between vitamin concentrations and BMI during chemotherapy in EC patients
There were correlations between the changes in serum vitamin A and C concentrations and the change in BMI before and after chemotherapy (P< 0 .05 ) (Table 7 ).
Regression analysis of vitamins and BMI in EC patients
Using the difference in vitamin concentrations as the independent variables and the difference in BMI as the dependent variable, logistic regression analysis revealed statistically significant differences for three vitamins (F = 5 .082 , P = 0 .002 ) (Table 8 ).
DISCUSSION
It was found that EC patients had different degrees of vitamin deficiency during chemotherapy, and the hemoglobin, total protein, serum albumin concentration and blood calcium concentration significantly decreased after chemotherapy. In addition,the proportions of patients with weight loss, anemia and hypoproteinemia also significantly increased. Our subjects were most deficient in vitamin B2and vitamin C followed by vitamins A and D.
In the current study, EC patients undergoing chemotherapy were most deficient in vitamin B2(31 .53 % and 46 .80 % before and after chemotherapy, respectively), and vitamin B2concentration significantly decreased after chemotherapy (P < 0 .05 ).Vitamin B1, B9 , B12 and B6 deficiency or excess was not found in any of our EC patients.A comparison of vitamin levels before and after chemotherapy suggested that vitamin B6concentrations decreased significantly after chemotherapy but were still within the normal range. It has been reported that B vitamin intake is correlated with the risk of EC. Appropriate supplementation with vitamins B6and B9 (also known as folate) can reduce the risk, while higher intake of vitamin B12 may increase the risk[15 ,16 ]. A study of residents in Yanting County, Sichuan Province, a high-incidence area of EC inChina, found that riboflavin intake was markedly deficient, and riboflavin supplements in high-risk groups reduced the incidence of EC[17 ]. In a multicenter study in China, whole blood riboflavin was tested in 764 EC patients (and in controls), and the analysis revealed that whole blood riboflavin levels were not significantly correlated with the prevalence of EC. However, high whole blood riboflavin level was more
favorable for the survival of elderly EC patients aged 50 -70 yrs[18 ]. Therefore, B vitamin supplementation in EC patients undergoing chemotherapy is beneficial to improve vitamin nutritional status and reduce complications.

Table 6 Factors affecting various indicators in esophageal cancer patients during chemotherapy
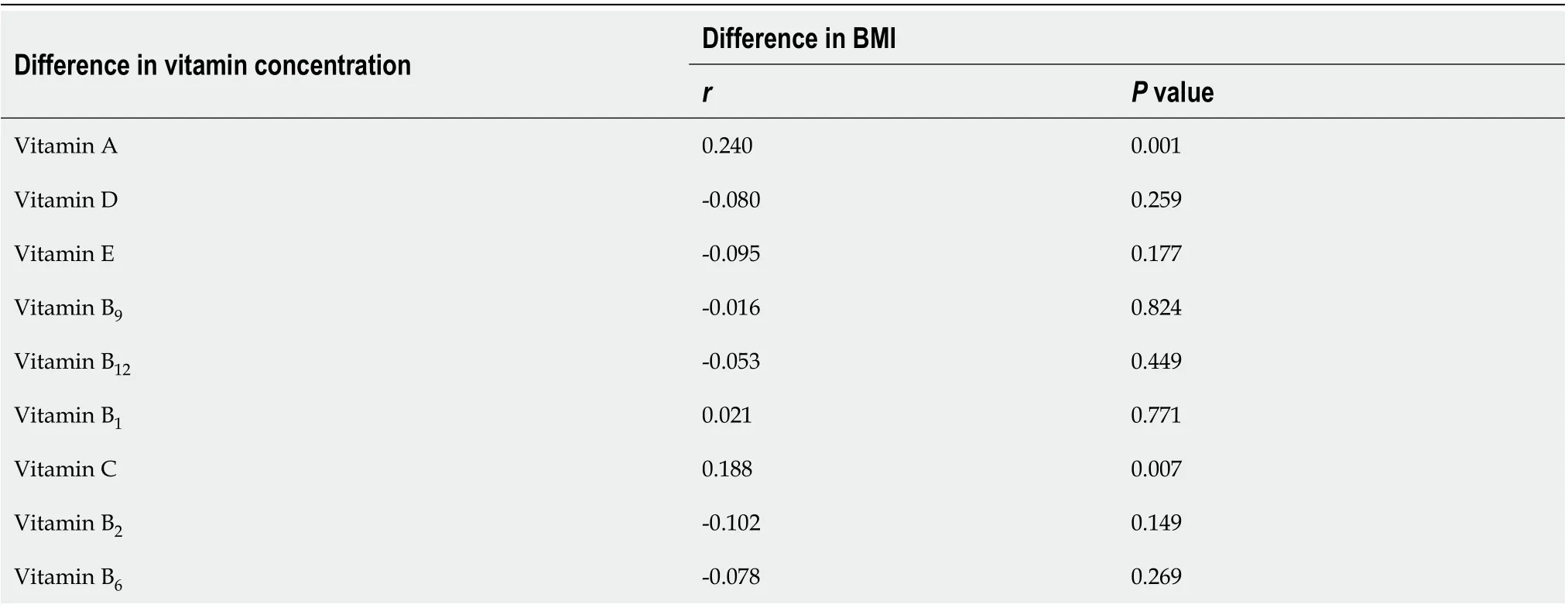
Table 7 Relationships between the differences in vitamins before and after chemotherapy and the difference in body mass index before and after chemotherapy in esophageal cancer patients

Table 8 Regression analysis of the relationships between the concentrations of various vitamins and body mass index in 203 esophageal cancer patients
In our research, the proportion of vitamin C deficiency cases was 23 .65 % and 34 .48 %, before and after chemotherapy, respectively. The difference was statistically significant, and vitamin C was the most deficient vitamin after chemotherapy. Thus,chemotherapy may have a considerable effect on vitamin C levels in EC patients. A meta-analysis showed a negative correlation between dietary vitamin C intake and EC risk and concluded that a high level of vitamin C may prevent EC[19 ]. Vitamin C supplementation was found to downregulate nuclear factor kappa B activity and significantly decrease proinflammatory cytokine levels in EC patients treated with neoadjuvant radiotherapy[20 ].
In the current study, vitamin A and D deficiencies were found in EC patients both before and after chemotherapy, and their proportions increased following chemotherapy. However, the changes in the proportions were not statistically significant after chemotherapy. Further stratified analysis of the baseline data showed that the change in vitamin A concentration during chemotherapy might be associated with gender, while vitamin D might differ among different tumor stages. Vitamins A and D are mainly derived from food sources. EC itself can affect the intake and absorption of food, and chemotherapy drugs further damage the nutritional status of patients, resulting in more significant vitamin deficiencies in patients after treatment.In the current study, we further analyzed the difference between vitamin concentrations and BMI in EC patients before and after chemotherapy and found that vitamins A and C were significantly correlated with the change in BMI. Regression analysis of multiple vitamins and BMI revealed a statistically significant overall model for three vitamins (A, D and C). Therefore, body weight, vitamin levels and hematological indicators interact with each other during chemotherapy in EC patients, and the supplementation of macronutrients and micronutrients are equally important.Developing holistic care is the key to nutritional therapy for tumor patients.
There were different degrees of vitamin A and D deficiencies in EC patients treated with chemotherapy, and a higher proportion of vitamin A deficiency than vitamin D deficiency and no vitamin E deficiency was detected during our observation. A metaanalysis suggested that vitamin A levels were negatively correlated with EC risk[21 ],and further studies are needed to confirm whether it affects the prognosis of EC patients. Vitamin D has been found to inhibit tumor cell proliferation, induce cell differentiation, promote apoptosis and suppress angiogenesis[22 ]. A meta-analysis did not observe an association between vitamin D levels and the development of esophageal lesions[23 ]. Another study reported that appropriate vitamin D supplementation in postoperative EC patients improved quality of life and disease-free survival, and further multivariate analysis found that vitamin D supplementation was an independent prognostic factor for disease-free survival but was not associated with overall survival[24 ].
This study had some limitations: (1) the sample size was not large due to the single center retrospective design of the study; (2) a control group was not included, and it is unclear whether vitamin supplementation is beneficial in EC patients undergoing chemotherapy; (3 ) the results might be biased due to different disease states and chemotherapy regimens; and (4) some patients might have received targeted therapy or immunotherapy during chemotherapy, which may have had an impact on the study results. In addition, no data on response rate or overall survival were included in our analysis, and the relationship between vitamin nutritional status and prognosis in EC patients requires further investigation in multicenter prospective studies.
CONCLUSION
Vitamin deficiencies (mainly vitamins A, D, C and B2deficiencies) are common in EC patients during chemotherapy and may be associated with the change in BMI. In addition, chemotherapy drugs decrease hematological indicators such as hemoglobin and albumin. Appropriate nutritional interventions and vitamin supplementation can reduce the adverse effects of chemotherapy, improve overall nutritional status of patients and improve drug tolerability and quality of life.
ARTICLE HIGHLIGHTS
杂志排行

World Journal of Gastroenterology的其它文章
- Celiac Disease in Asia beyond the Middle East and Indian subcontinent: Epidemiological burden and diagnostic barriers
- Biomarkers in autoimmune pancreatitis and immunoglobulin G4-related disease
- Risk of hepatitis B virus reactivation in patients with autoimmune diseases undergoing non-tumor necrosis factor-targeted biologics
- Risk factors and prognostic value of acute severe lower gastrointestinal bleeding in Crohn’s disease
- Effects of sepsis and its treatment measures on intestinal flora structure in critical care patients
- Gut microbiota dysbiosis in Chinese children with type 1 diabetes mellitus: An observational study