Meeting 24-h movement guidelines:Prevalence,correlates,and the relationships with overweight and obesity among Chinese children and adolescents
2021-05-22SiTongChenYngLiuMrkTremblyJinToHongYnTngZhenBoCoJieZhungZhengZhuXuepingWuLijunWngYujunCiPeijieChen
Si-Tong Chen,Yng Liu,b,*,Mrk S.Trembly,Jin-To Hong,Yn Tng,b,Zhen-Bo Co,Jie Zhung,Zheng Zhu,Xueping Wu,b,Lijun Wng,b,Yujun Ci,b,Peijie Chen
a School of Physical Education and Sport Training,Shanghai University of Sport,Shanghai 200438,China
b Shanghai Research Centre for Physical Fitness and Health of Children and Adolescents,Shanghai University of Sport,Shanghai 200438,China
c Healthy Active Living and Obesity Research Group,Children’s Hospital of Eastern Ontario Research Institute,Ottawa,ON K1H 8L1,Canada
d School of Kinesiology,Shanghai University of Sport,Shanghai 200438,China
Abstract Background:Meeting 24-h movement guidelines by children and adolescents has been associated with improved indicators of health,although it has been under-studied in China.Hence,this study aimed to investigate the prevalence of meeting the 24-h movement guidelines,its correlates,and its relationships with body mass index in children and adolescents in China. Methods:Cross-sectional data from the 2017 Youth Study in China of 114,072 children and adolescents(mean age=13.75 years,49.18%boys)were used.Meeting 24-h movement guidelines(≥60 min of daily moderate-to-vigorous physical activity,≤2 h of daily leisure screen time,9-11 h and 8-10 h nightly sleep duration for 6-13-year-olds and 14-17-year-olds,respectively)and height and weight of all participants were assessed.The prevalence of meeting the 24-h movement guidelines and World Health Organization weight status categories were determined.Generalized linear models were used to determine the correlates of meeting the 24-h movement guidelines and the relationships of meeting the 24-h movement guidelines with overweight(OW)and obesity(OB). Results:Only 5.12%of Chinese children and adolescents met the 24-h movement guidelines,and 22.44%were classified as OW/OB.Older children and adolescents were less likely to meet the 24-h movement guidelines.Parental education level and family income were positively related to meeting the 24-h movement guidelines.Children and adolescents meeting the 24-h movement guidelines showed lower odds ratios for OW/OB.Compared with participants meeting the 24-h movement guidelines,boys in 4th-6th grades met none of the recommendations(OR=1.22,95%CI:1.06-1.40),met the screen time recommendation only(OR=1.13,95%CI:1.01-1.28),met the nightly sleep duration recommendation only(OR=1.14,95%CI:1.03-1.28),and had significantly higher odds ratios for OW/OB.Similar trends were observed for girls in 4th-6th grades:meeting none of the guidelines(OR=1.35,95%CI:1.14-1.59),meeting sleep duration guidelines only(OR=1.23,95%CI:1.08-1.39),and meeting moderate-to-vigorous physical activity+nightly sleep duration guidelines(OR=1.24,95%CI:1.01-1.54).For girls in 7th-9th grades,the following trend was observed:meeting none of the guidelines(OR=1.30,95%CI:1.01-1.67). Conclusion:Very few Chinese children and adolescents met the 24-h movement guidelines.Age(negatively correlated),parental education level,and family income(both positively correlated)were correlates of meeting the 24-h movement guidelines.Children and adolescents meeting the 24-h movement guidelines were more likely to have lower risks for OW/OB,especially in the youngest age group(Grades 4-6);and girls in the middle age group(Grades 7-9)were also more likely to have lower risks for OW/OB.Further research studies should explore additional correlates and determinants for meeting the 24-h movement guidelines.Also,future studies should use longitudinal or interventional designs to determine the relationships between meeting the 24-h movement guidelines and OW/OB and other health indicators,while taking sex and age differences into account.
Keywords:Body weight;China Youth Study;Moderate-to-vigorous physical activity;School-aged children;Screen time;Sleep duration
1.Background
Child and adolescent overweight(OW)and obesity(OB)have been a growing global health problem.1Despite increasing concern and awareness,the prevalence of OW/OB in children and adolescents remains high.2The Global Burden of Disease 2015 Obesity Collaborators found that 107.7 million children around the world were obese.3In China,specifically,data from 2010 show that 8.1%of children aged 7-18 years were obese.4From 1991 to 2011,the prevalence of Chinese children aged 6-18 years who were OW doubled.5One study using nationally representative samples showed that the prevalence of OW/OB among Chinese school-aged children was approximately 30%.6This public health concern has garnered the attention of Chinese policymakers.7
Studies have shown that sufficient moderate-to-vigorous physical activity(MVPA),8limited screen time(ST),9and appropriate sleep duration(SLP),10collectively referred to as movement behaviors,are important and modifiable determinants of OW/OB in young people.For example,studies from the International Study of Childhood Obesity,Lifestyle and the Environment(ISCOLE)11found that more MVPA,less ST,and adequate SLP were associated with reduced OB.12-14Other studies have provided similar findings.15-17One study found that the international prevalence of sufficient MVPA among youth was 44.1%.12Based on a questionnaire survey,the prevalence of Chinese children and adolescents meeting MVPA guidelines was 34.1%.18Adherence to ST guidelines among youth is also low,with only 8.1%19of Canadian youth and 23.1% of UK youth meeting the recommendation.20In Hong Kong,China,38.6%of adolescents achieved the recommended SLP duration,21which is similar to results from surveys in the USA12and the mainland of China.12Collectively,there is compelling evidence of poor adherence to individual movement-behavior guidelines.
Based on convincing evidence of the combined health benefits of meeting MVPA,ST,and SLP recommendations,22the Canadian 24-Hour Movement Guidelines propose specific integrated recommendations for MVPA,ST,and SLP in children and adolescents,23and these recommendations have been applied as the research paradigm.24Time-use epidemiology provides a solid theoretical foundation for integrative health-behavior research.25The theoretical foundation highlights the importance of combining MVPA,ST,and SLP because these 3 time-use compositions cover the 24-h period,and a balance among them is required for optimal health.26Within the time-use framework,prevalence,correlates/determinants,and health outcomes are 3 essential components.25Many researchers have applied the Canadian 24-Hour Movement Guidelines to conduct time-use epidemiological research among young people.27-31
To capture the prevalence of meeting the 24-h movement guidelines,2 kinds of measures(i.e.,accelerometers and selfreported questionnaires)have been used.Using accelerometers(ActiGraph GT3X+;ActiGraph LLC,Penscola,FL,USA)in free-living conditions,1 international study reported that about 7%of children aged 9-11 years had sufficient MVPA,limited ST,and adequate SLP concurrently.12A recent study of Chinese adolescents(Hong Kong,China)using activPAL(Glasgow,Scotland)accelerometers indicated that only 1%of adolescents met the 24-h movement guidelines.21Investigations using self-reported questionnaires have also shown low levels of meeting guidelines for healthy 24-h movement behaviors.Two studies indicated that the prevalence of meeting the 24-h movement guidelines in Canadian children and adolescents ranged from 2.6%19(using the Health Behavior School-aged Children Questionnaire)to 17.5%28(using the Canadian Health Measures Survey).Lee et al.29reported that only 3%of South Korean adolescents met the 24-h movement guidelines.This large variation in the prevalence of meeting the guidelines may be due to the use of different measures.Despite the higher accuracy of accelerometers in estimating 24-h movement behaviors,self-reported measures are an ideal measurement method for large-scale monitoring and surveillance owing to their lower testing burden and costs.To our knowledge,however,little is known about the prevalence of meeting the 24-h movement guidelines among young people in China.32
With regard to the correlates of meeting the 24-h movement guidelines,a limited number of studies have been conducted.30,31Two studies suggested that parental support,residence,and outdoor time were the key correlates.30,31However,such evidence pertaining to Asia is not available and is insufficient for fully understanding the pattern of movement behaviors in Chinese children and adolescents.32Further studies are required in this field,especially studies that seek to identify sociodemographic correlates.20
Recent evidence has demonstrated that different combinations of MVPA,ST,and SLP(e.g.,MVPA+ST,MVPA+SLP,or all of them)rather than 1 single behavior can lower the risks of OW/OB in children and adolescents.12,21,27,28For example,Carson et al.27found that the greater number of guidelines that children and adolescents meet,the lower the odds of their having a high body mass index(BMI)z-score,after controlling for age,sex,and level of parents’education.Similar findings were also reported by Roman-Vi~nas et al.12(who adjusted for sex,age,household education,and diet)and Laurson et al.33,34(who adjusted for age,grade,and ethnicity).In sum,these studies,which all used objective measures to determine the BMI of participants,consistently showed that having sufficient MVPA,limited ST,and adequate SLP may be effective in preventing OW/OB.However,a study in Asia(Hong Kong,China)generated mixed results and showed that the combination of MVPA,ST,and SLP may not be associated with lower odds of OW/OB(adjusted for sex,age,and clustering school effects).21These inconsistent findings point to the need for more evidence to clarify the relationships between movement behaviors and OW/OB,especially in Asia.The Behavioral Epidemiology Framework suggests that an essential element in determining whether behaviors should be targeted for intervention is determining the associations between the behaviors and health outcomes.35However,the relationships reported in previous research have not been investigated in Chinese children and adolescents.32Thus,studying the relationships as they pertain to Chinese children and adolescents can provide public health insights for OW/OB prevention in China.
Using the time-use epidemiology framework25as a foundation,and to fill the gaps in the previous literature,the aims of this study were(1)to establish for the first time the prevalence of a national sample of Chinese children and adolescents meeting the 24-h movement guidelines(in insolation or in combination);(2)to determine,in relation to Chinese children and adolescents,the correlates of meeting the 24-h movement guidelines;and(3)to examine the relationships between meeting the 24-h movement guidelines and OW/OB in Chinese children and adolescents.
2.Methods
2.1.Study design and participants
This study used a sample from a nationwide survey drawn from the 2017 Physical Activity and Fitness in China—The Youth Study(PAFCTYS).36The overall study design for PAFCTYS can be found elsewhere.37In brief,PAFCTYS is a nationally representative surveillance survey that assessed the physical fitness and health level of children and adolescents in China,with administrative support of the Ministry of Education.Using a multistage sampling design,a balanced representation of geography,economic development,and rural-urban diversity was achieved.Public schools in 31 administrative regions in the mainland of China were recruited.The sampling procedure involved sampling administrative cities and districts,towns,and local community districts that represented a mix of rural and urban areas.The smallest sampling units were primary schools(Grades 4-6),junior middle schools(Grades 7-9),and junior high schools(Grades 10-12).The student sampling took place in classes selected randomly from each grade in the selected schools.The Ministry of Education selected 4 regions in each province or administrative region,of which 1 urban and 1 rural area in each region were identified.In each area(urban or rural),4 schools(2 primary,1 junior middle,and 1 junior high schools)were selected.At the school level,2 classes from each grade in the primary schools,and 1 class from each grade in the junior middle and junior high schools were randomly selected.Using the above procedure,a sex-balanced sample size of more than 30 students for each grade in the primary schools was achieved,and a sample size of more than 60 students was achieved for the junior middle and junior high schools.
Grades 1-3 were not included in this study because of the students’limited cognitive ability to take part in the study survey.In total,131,992 targeted students were recruited into the 2017 PAFCTYS.A total of 131,859 students(response rate=99.90%)completed the questionnaire survey and physical assessments.They were recruited from 490 primary schools,251 junior middle schools,and 245 junior high schools,from a total of 31 provinces,4 direct-controlled municipalities,and 6 regions.
The study protocol was approved by the Institutional Review Board of Shanghai University of Sport in 2017,and permission to conduct the study was obtained from the teachers and principals at the participating schools.All the children and adolescents participating in the study and their parents or guardians were informed that participation was voluntary.Verbal informed consent was obtained from all parents or guardians,and positive assent was obtained verbally from all the children before data collection.Data were collected and analyzed anonymously.
2.2.Procedures
All selected students were informed about the research project prior to participation.A research assistant registered each verbal consent/assent,which was put into a subject file with a numeric identification code and subsequently entered into a computer database accessed exclusively by authorized project staff.Data collection took place at school between October and December of 2017.This period was selected so that physical fitness and health examinations could be conducted with administrative support from the Ministry of Education in China.Participants received detailed directions on how to answer the survey.Following a standardized survey-administration protocol,37trained research assistants conducted a survey of physical activity and assessment of body weight and height during regular school time.Students first had body weight and height assessments.Then they independently completed the survey questionnaire either online(68%)or on a paper version(32%)in a classroom setting.
2.3.Measures
2.3.1.Demographics and socioeconomic status
Demographic information about the children and adolescents was collected via a student self-reported questionnaire,including gender(boy or girl),grade(4,5,...12),ethnicity(Han or others),and residence location(urban or rural).
Socioeconomic status(SES)information,including parental educational level(both parents:less than college or university,college or university or higher;in our study,the former was defined as low education level,while the latter was defined as high education level)and family income per person annually(Chinese currency(RMB):<9000,9000-30,000,30,001-100,000,>100,000),was collected via a parent-reported questionnaire based on the method developed by Cirino et al.38(reliability coefficient=0.78,validity coefficient=0.30).
2.3.2.Movement behaviors
PA was measured by the reliable and valid item derived from the Health Behavior in School-aged Children survey questionnaire(reliability coefficient=0.82).39The following item was used:How many days did you engage in MVPA at least 60 min on weekdays over the past week?(0=none,1=1 day,2=2 days,3=3 days,4=4 days,5=5 days,6=6 days,and 7=7 days).So that students would have a better understanding of MVPA,it was explained as“any kind of physical activity increasing your heart rate and breathing frequencies during a period(including physical education,physical exercising,sports training,and various regular daily activities,such as brisk walking,hiking,and excursion)”.According to the Canadian 24-Hour Movement Guidelines,23meeting the MVPA guideline requires that participants report 7 days with a minimum of 60 min of MVPA daily.
ST was also measured using reliable and valid items derived from the Health Behavior in School-aged Children.39The following items were used:(1)How many hours did you spend watching TV or movies in your leisure time on weekdays and weekend days over the past week,respectively?(reliability coefficients:0.74 and 0.72,respectively);(2)How many hours did you spend playing video games in your leisure time on weekdays and weekend days over the past week,respectively?(reliability coefficients:0.54 and 0.69,respectively);and(3)How many hours did you spend in activities using electronic screen-based devices in leisure time on weekdays and weekend days over the past week,respectively?(reliability coefficients:0.33 and 0.50,respectively);The responses to these questions could be:none,about 0.5 h,1 h,2 h,or 3 h or more.According to the Canadian 24-Hour Movement Guidelines,23meeting the ST guideline requires daily ST≤2 h per day.
SLP was measured by 1 item from the China Health and Nutrition Survey,which has accepted validation(reliability coefficient=0.83).40The item asked participants to report their usual nightly sleep duration(in hours)on a normal day.According to the Canadian 24-Hour Movement Guidelines,239-11 h are recommended for 6-13-year-olds and 8-10 h are recommended for 14-17-year-olds.Participants who reported the recommended nightly sleep duration were regarded as meeting the SLP guidelines.Based on the above definitions,the combined prevalence(s)were defined as meeting two or all three of the guidelines(e.g.,the prevalence of meeting the MVPA,ST,and SLP guidelines).
2.3.3.Weight status
Weight status was determined by BMI,calculated as the participants’weight-height ratio.These measurements were conducted by well-trained research staff who followed a standardized protocol.37Weight was measured to the nearest 0.1 kg with a balance-beam scale while the participants were wearing lightweight clothing.Height was measured to the nearest 0.1 cm with a portable stadiometer while the participants were barefoot.Both measures were assessed using a portable instrument(GMCS-IV;Jianmin,Beijing,China).BMI values were calculated(BMI=Weight(kg)/Height(cm)2;kg/m2).According to sex-and age-specific cut-offs for OW and OB established by the World Health Organization,41participants were dichotomized into non-OW/OB or OW/OB.
2.4.Statistical analysis
After cleaning invalid and abnormal values of all independent and dependent variables(Fig.1),the final analytical sample size was 114,072.Descriptive analyses were performed to report the characteristics of the sample,the prevalence of meeting the recommendations(in isolation or in combination),and the prevalence of non-OW/OB and OW/OB.To produce nationally representative results,prevalence estimates(reported as percentages with 95% confidence interval(95%CI))of the 2017 PAFCTYS sample were weighted according to the Chinese school-aged population of children in the current school education system(i.e.,primary,junior middle,and junior high schools).Because of the non-normal distribution of age and BMI in our sample,Mann-Whitney tests were performed to examine sex differences by age and BMI.Generalized linear models were used to examine the associations between the prevalence of meeting the recommendations(in isolation or in combination)and weight status.Models set the study sites as fixed effects and the school as random effects.There was a sex×age group interaction between the prevalence of meeting the various combinations of the 24-h movement guidelines and weight status.Thus,the models were presented by total samples,and then by sex and age group.The level of statistical significance was set atp<0.05.Cohendwas calculated as a measure of effect size.All statistical analyses were executed using SPSS(Version 24.0;IBM Corp.,Corp.Armonk,NY,USA).
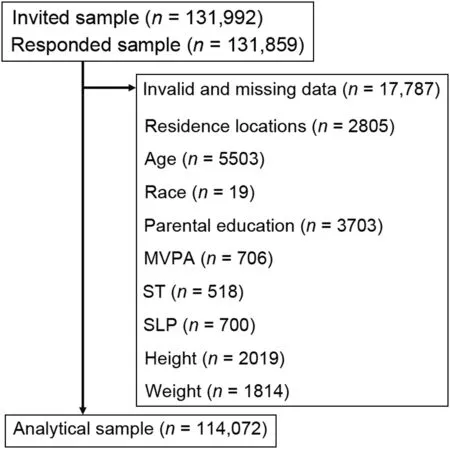
Fig.1.The procedure used for cleaning invalid and missing data in this study.MVPA=moderate-to-vigorous physical activity;SLP=sleep duration;ST=sedentary time.
3.Results
The descriptive characteristics of the samples in this study are shown in Table 1.The percentages for boys and girls were 49.18%and 50.82%,respectively.The mean age of the participants was 13.75±2.61 years old(weighted:13.16,95%CI:13.14-13.17),with statistical difference between sex groups(p<0.001).The mean BMI was 19.93±3.65 and was significantly different between sexes(p<0.001,Cohend=0.06).The proportions of the sample across the 3 age groups were 34.83%(4th-6th graders;weighted:42.85%,95%CI:42.55%-43.16%);33.21%(7th-9th graders;weighted:37.28%,95%CI:36.98%-37.57%);and 31.96%(10th-12th graders;weighted:19.87%,95%CI:19.67%-20.07%),respectively.Most participants identified as Han ethnicity(86.37%;weighted:86.19%,95%CI:85.98%-86.39%).There were no sex differences in age or ethnicity groups(bothp>0.05,both Cohend=0.01).The participants living in urban areas accounted for about 60%(weighted:61.87%,95%CI:61.58%-62.16%)of the sample,and there was a sex difference in residence locations(p<0.001,Cohend=0.02).The majority of participants’parents had low education levels(81.38%,weighted:80.92%,95%CI:80.68%-81.16%;no sex difference,p=0.927,Cohend=0.01).More than 57% of
families(weighted:57.80%,95%CI:57.50%-58.09%)had 2 or more children(pfor sex difference<0.001,Cohend=0.18).Only about 7%(weighted=7.27%,95%CI:7.12%-7.43%)of families had an income>100,000 RMB per person(pfor sex difference<0.001,Cohend=0.06).More than 22%(weighted:23.79%,95%CI:23.53%-24.05%)of participants were classified as OW/OB(pfor sex difference<0.001,Cohend=0.27).
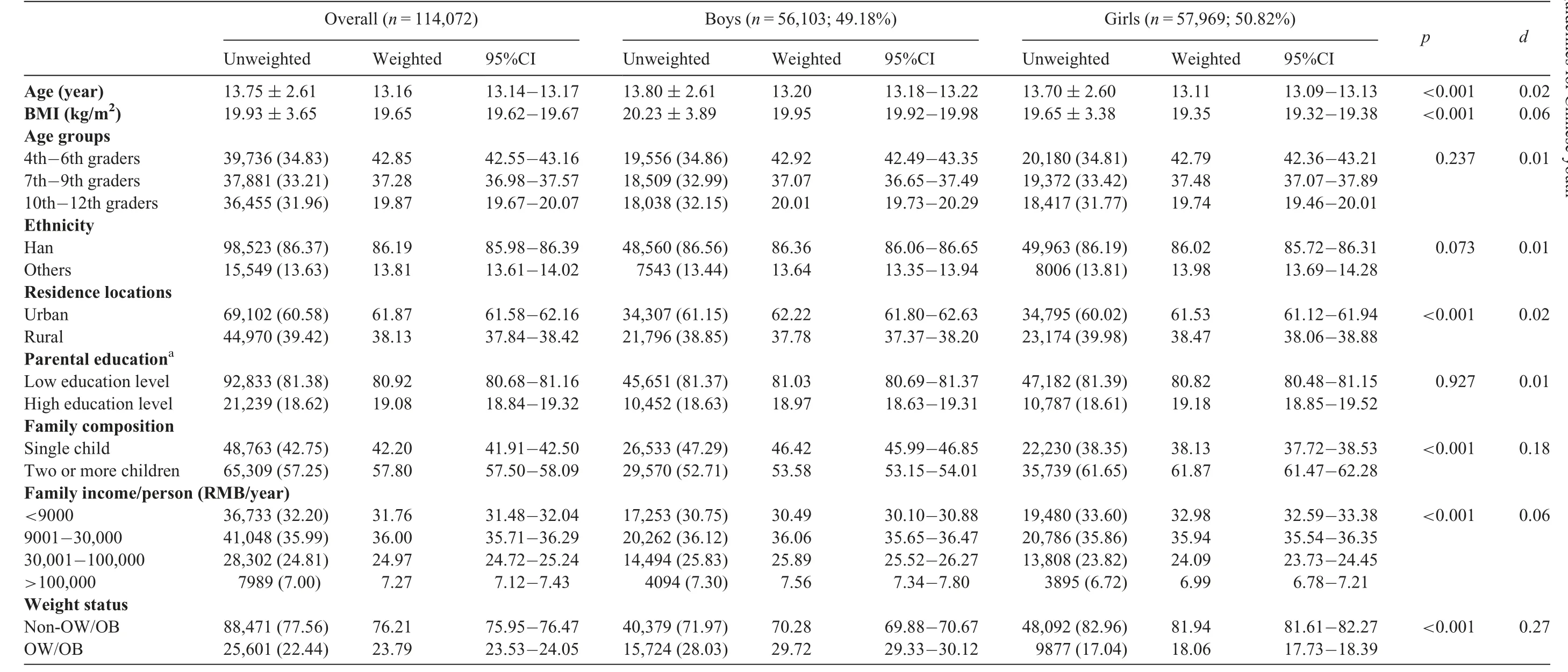
Table 1Descriptive characteristics of the study sample(mean±SD or n(%)).
Table 2 presents the prevalence of participants meeting various combinations of the 24-h movement guidelines.The percentage meeting the 24-h movement guidelines was 5.12%(weighted:6.04%,95%CI:5.89%-6.19%)(no sex difference,Cohend=0.01).The prevalence of meeting the MVPA,ST,and SLP guidelines was 11.80%(weighted:12.89%,95%CI:12.68%-13.10%),65.26%(weighted:64.75%,95%CI:64.46%-65.03%)and 44.40%(weighted:50.74%,95%CI:50.44%-51.04%),respectively.More boys reported meeting the MVPA and SLP guidelines than did girls(p<0.001,Cohend=0.09 and 0.06,respectively).The prevalence of meeting some combination of the 24-h movement guidelines(e.g.,MVPA+ST,MVPA+SLP,and ST+SLP)varied greatly,from 7.10%(weighted:8.35%,95%CI:8.18%-8.53%)to 28.49%(weighted:32.71%,95%CI:32.42%-33.00%).Boys had significantly higher prevalence of the combination of the MVPA+ST guidelines and MVPA+SLP guidelines than did girls(p<0.001,Cohend=0.03 and 0.05,respectively).

Table 2Prevalence of meeting different combinations of 24-h movement behavior guidelines by gender n(%).
The associations between demographics and the prevalence of meeting the 24-h movement guidelines are presented in Table 3.The odds ratios for meeting the 24-h movement guidelines among 4th-6th graders(odds ratio(OR)=15.70,95%CI:13.89-17.74)and 7th-9th graders(OR=4.10,95%CI:3.59-4.67)were significantly higher when compared to 10th-12th graders.Boys living in urban locations were more likely(OR=1.11,95%CI:1.02-1.21)to meet the 24-h movement guidelines compared with either boys or girls living in rural locations.Participants whose parents had high education levels were 1.23 times more likely to meet the 24-h movement guidelines compared to participants whose parents had low education levels.These statistically significant trends were observed for both sexes(OR for boys=1.25,95%CI:1.13-1.37;OR for girls=1.23,95%CI:1.11-1.35).Participants in the higher family-income groups were more likely to meet the 24-h movement guidelines than participants in the lowest family-income group.A consistent gradient related to family income was observed among girls;however,only boys from families with the second highest(30,001-100,000)and the highest(>100,000)family income categories were significantly more likely to meet the 24-h movement guidelines(OR for the second highest=1.12,95%CI:1.00-1.25;OR for the highest=1.46,95%CI:1.26-1.68).Ethnicity and family composition were not significantly correlated with the prevalence of meeting the 24-h movement guidelines.
Table 4 shows the associations between meeting different 24-h movement guidelines with OW/OB among the participants.After controlling for all the covariates(e.g.,sex,grade,and parental education level),meeting none or fewer of the guidelines showed higher ORs for OW/OB when compared with the group meeting the MVPA+ST+SLP guidelines.However,only meeting none(OR=1.25,95%CI:1.16-1.34),ST(OR=1.20,95%CI:1.12-1.28),SLP(OR=1.15,95%CI:1.07-1.23),and MVPA+SLP(OR=1.12,95%CI:1.01-1.25)guidelines exhibited higher statistically significant odds for OW/OB compared with those meeting the MVPA+ST+SLP guidelines(allp<0.05).
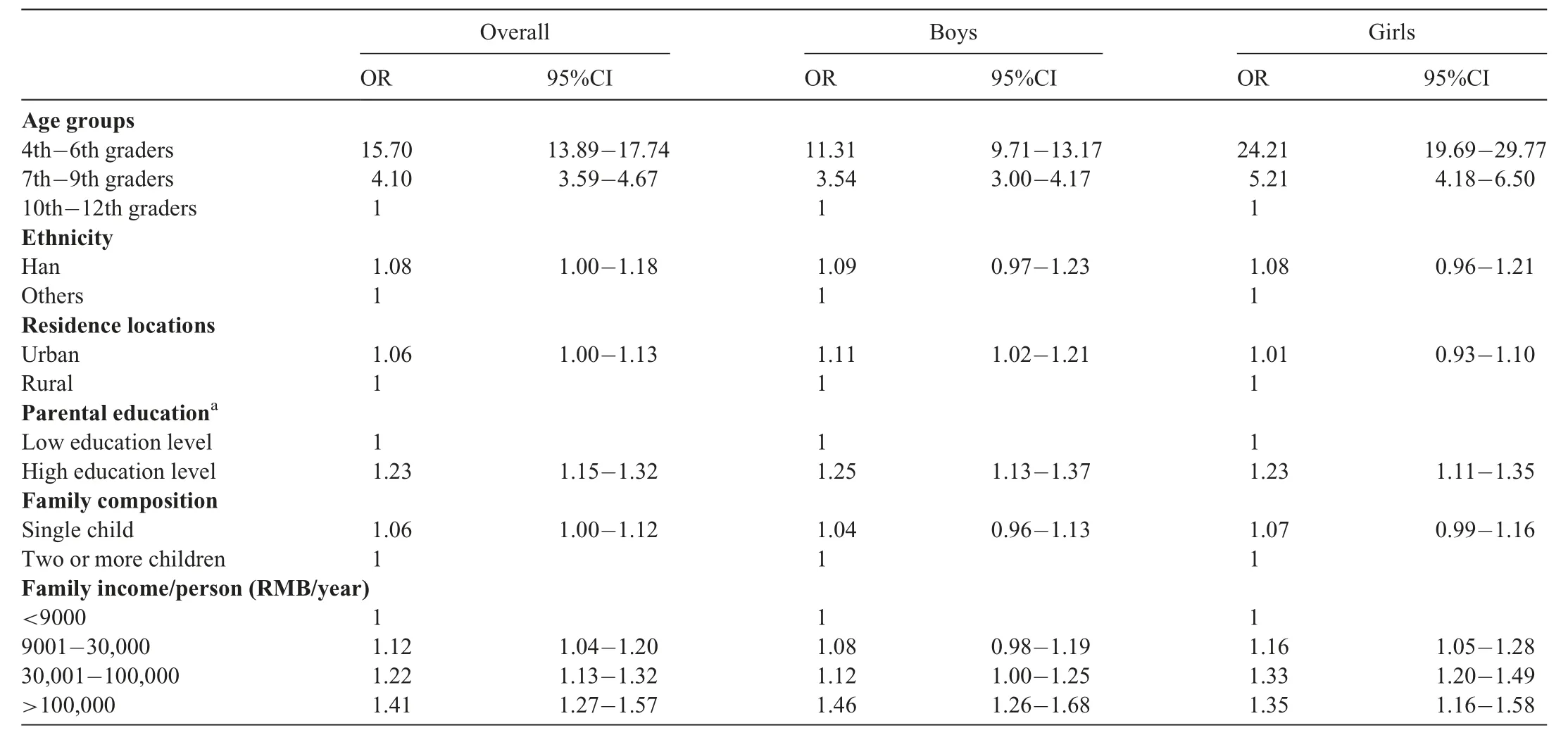
Table 3The associations between meeting the 24-h movement guidelines and sociodemographic correlates.
The summarized results for the OR for OW/OB participants meeting the different 24-h movement guidelines by sex and grade levels are shown in Table 5.A general pattern emerged,with lower odds of OW/OB participants’meeting more 24-h movement guidelines,though most were not significant.The relationships appeared to be stronger in younger children and girls than in adolescents and boys.
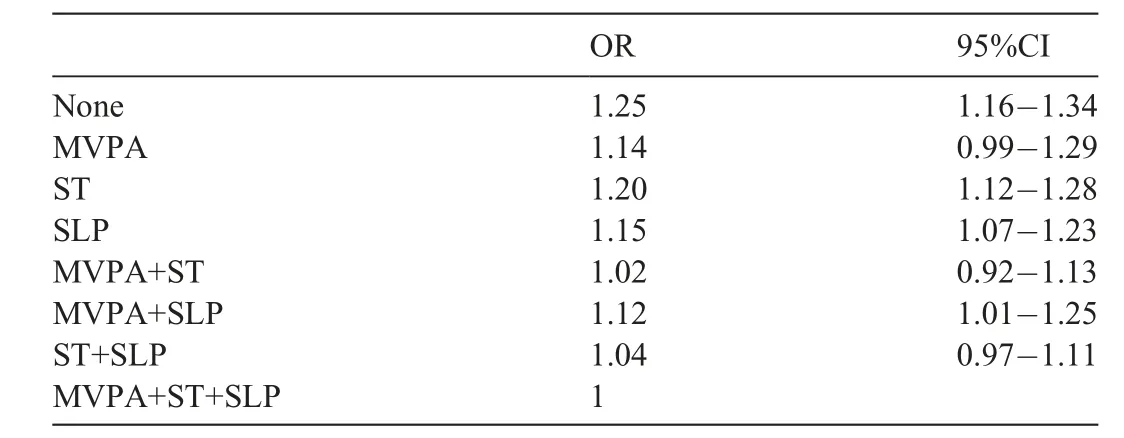
Table 4ORs for overweight and obesity associated with meeting different 24-h movement guidelines.
4.Discussion
Using nationally representative data,this study aimed to investigate the prevalence among Chinese children and adolescents of meeting the 24-h movement guidelines,determine the sociodemographic correlates of the prevalence,and explore the relationships between meeting the integrated guidelines and OW/OB.We found that the prevalence of meeting the integrated guidelines was low,which was associated with age,parental education level,and family income.Meeting the 24-h movement guidelines was related to a lower OR of being OW/OB for boys in the 4th through 6th grades and girls in the 7th through 9th grades but not for the other age or sex groups(though a similar pattern was observed).
Gaining a thorough understanding of prevalence of meeting the 24-h movement guidelines is beneficial in promoting movement behavior in young people.32The current study demonstrated that 5.12%(weighted:6.04%)of Chinese children and adolescents met the 24-h movement guidelines.This is the first study to investigate the prevalence of meeting the 24-h movement guidelines in a nationally representative sample of Chinese children and adolescents.The prevalence found in this study is consistent with level of prevalence found among youth in the USA(5%).42Although the level of prevalence of meeting the 24-h movement guidelines in our study was higher than that among children and adolescents in Hong Kong,China(1%),21South Korea(3.2%);43and Canada(<3%),19it is lower than the prevalence found in other previously published studies using international12and national samples.20,42These variations may be attributed to differences in measurements.For example,some studies used accelerometers to estimate the prevalence,12,21,30while others used self-reported questionnaires.19,29Considering the cumulative health benefits of meeting the 24-h movement guidelines,12,22,27our study can provide insightful information for developing programs that will improve movement behaviors in a young Chinese population.
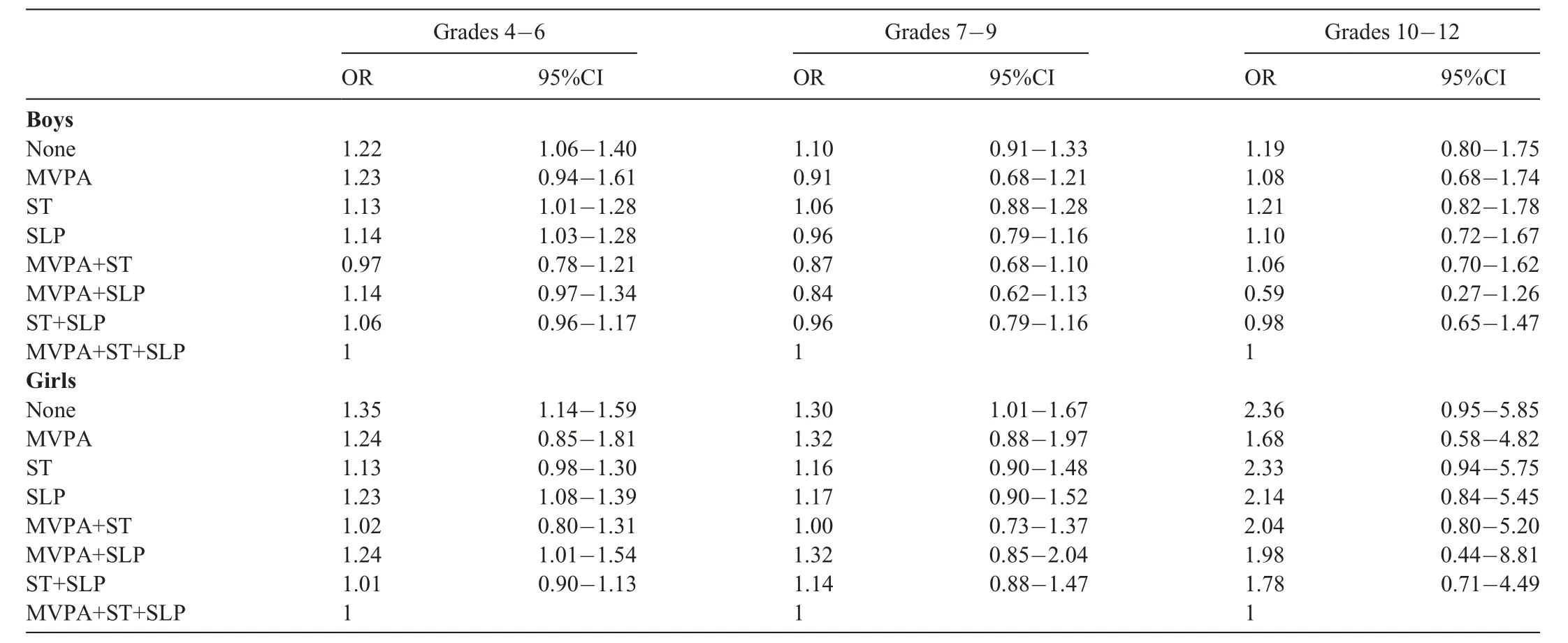
Table 5ORs for overweight and obesity associated with meeting different 24-h movement guidelines by sex and grade levels.
The low prevalence in our study of meeting the 24-h movement guidelines was due mainly to the low prevalence in meeting the PA guidelines(which was lowest compared to meeting the ST and SLP guidelines by themselves).This finding is supported by studies conducted in Hong Kong,China,21and internationally.12The low prevalence of meeting the PA guidelines by Chinese children and adolescents is also consistent with previous national surveys.18,37It is also important to recognize that the main driver of low prevalence in meeting the 24-h movement guidelines varies.For UK youth,the low prevalence of meeting the ST guidelines is a primary contributor.20Thus,studying the time-use patterns and their distribution for children and adolescents12and identifying the main driver of low prevalence is a necessity in movement-behavior and time-use research.25Our study has identified a lower PA level as possibly being a main driver for the lower prevalence of meeting the 24-h movement guidelines and,thus,offers some practical implications for promoting movement behaviors among Chinese children and adolescents.
Understanding the correlates of meeting the 24-h movement guidelines is of vital importance for designing effective public health initiatives and targeting populations with health risks.25,32Some recently published studies have examined the correlates of meeting the 24-h movement guidelines in children and adolescents.30,31In our study,age,parental education level,and family income were key correlates of meeting the 24-h movement guidelines.Increasing age was negatively associated with the prevalence of meeting the guidelines.Compelling evidence has shown that there are age-related declines in MVPA,18,37increases in ST,6,18and lower SLP duration44,45in children and adolescents.To secure improved education,the increased academic pressure that comes with increasing age often results in more time spent studying,46which perhaps displaces PA opportunities and SLP.Furthermore,older Chinese children and adolescents typically have mobile smart devices,which increases the probability of sedentary screen-based behaviors.46These 2 factors may have contributed to our findings that very few Chinese children and adolescents met the 24-h movement guidelines.Parental education level and family income can be considered strong indicators of SES and have been shown to be significantly correlated with children’s and adolescents’MVPA,47,48ST,49,50and SLP.44,51The underlying mechanism may be that parents in higher SES categories have better awareness of their children’s health behaviors and help them pursue healthy lifestyles.They may also be able to provide better financial support,which helps to facilitate healthful PA and sport opportunities.However,family SES is hard to modify.Therefore,reinforcing the importance of equitable access to interventions for children and adolescents from different SES levels is necessary.51Although our study provides some preliminary evidence for understanding time use in a 24-h timeframe by Chinese children and adolescents,additional studies that explore the association between 24-h movement behaviors and multidimensional factors are encouraged.32
It has been suggested that it is inappropriate to examine the relationship between a single behavior(e.g.,MVPA,ST,or SLP)and health.32Therefore,if researchers use 24-h movement guidelines,they can better examine the relationship between integrated behaviors within a 24-h cycle and health outcomes,and the implications of their findings for promoting young people’s health will be increased.23,24,32The relationships between meeting the 24-h movement guidelines and OW and OB have been reported in previous studies.12,21,27,33,34A systematic review by Saunders and colleagues22indicated that the combination of sufficient MVPA,limited ST,and adequate SLP may result in lower odds of being OW/OB.Our study supports their findings,which are also supported by other empirical evidence.12,33,34We found that MVPA may not be an effective predictor of OW and OB,which is inconsistent with other studies that suggest that MVPA is a strong predictor of these conditions.34Possible reasons for this inconsistency may lie in the fact that different measures of PA were used.However,our finding that those not meeting the 24-h movement guidelines had the highest OR for OW/OB compared with those who met the guidelines is consistent with the findings of Roman-Vi~nas et al.12and Laurson et al.33Our finding reinforces the importance of combining MVPA,ST,and SLP in the prevention of OW/OB in Chinese children and adolescents rather than promoting a single behavior(MVPA,ST,or SLP)in isolation.Our study supports the time-use epidemiological framework,25in which combinations of sufficient MVPA,limited ST,and appropriate SLP lead to improved health conditions in young people.Because our study design does not establish a true cause-and-effect relationship,future studies should address this research issue.
In our study,the relationship between meeting the 24-h movement guidelines and OW/OB varied by age and sex.This finding is in line with previous research.52Sex and age differences in biological growth are responsible for different trajectories of weight status among young people.1In our study,we found that among children and adolescents in Grades 7-12,there generally was no significant relationship between meeting the 24-h movement guidelines and OW/OB,irrespective of sex,a finding that is not supported by previous studies.Some potential explanations for this inconsistency are useful.First,measurement errors caused by the use of self-reported questionnaires may result in inaccurate measures of movement behaviors,which may skew the link between movement behaviors and OW/OB.Second,evidence has been presented that questions the independent link between ST and SLP and OW/OB in a young population.53,54This implies that ST and SLP may not be determinants of OW/OB.Yet another explanation may be diet.It has been found that childhood and adolescent OW/OB is related to nutrition and diet,especially in developing countries(e.g.,China).55Diet can cause excessive energy intake,thus contributing to OW/OB.Therefore,it is possible that despite meeting the 24-h movement guidelines,children and adolescents who have unhealthful diets can be at increased risk for OW/OB.These findings may be useful in informing sex-and age-tailored weight interventions.
The strengths of our study include the following.First,we used a large survey sample,which could lead to a wider generalization of the findings for China.Second,our study was the first to examine the association between movement behaviors and weight status in Chinese children and adolescents and,thus,can inform the design of effective interventions,prevention strategies,and policies.Third,we included additional sociodemographic factors related to meeting the 24-h movement guidelines,which could help researchers to better understand the patterns of movement behaviors.Some limitations,however,should also be mentioned.First,the cross-sectional design of this study precludes conclusions regarding causality between behaviors and weight status.Second,a self-reported questionnaire was used to collect data;therefore,measurement errors could have occurred.Third,our study considered only a few confounders influencing children’s and adolescents’weight status;some other significant cofounders(e.g.,diet and nutrition)12were not included.
5.Conclusion and clinical implications
The prevalence of meeting the 24-h movement guidelines among Chinese children and adolescents was relatively low.Unhealthful lifestyles were associated with increasing age,lower parental education level,and lower family income.Meeting the 24-h movement guidelines was related to lower ORs for OW/OB.This relationship was obvious among boys in Grades 4-6 and among girls in Grades 7-9.Future studies should use improved study designs(e.g.,longitudinal designs)to determine the correlates/determinants of meeting the 24-h movement guidelines among Chinese children and adolescents.To better understand the relationship between meeting the 24-h movement guidelines and OW/OB,interventional studies should control for more confounders(e.g.,diet and nutrition)while considering sex and age differences.
From a clinical perspective,our study suggests that promoting positive 24-h movement behaviors is needed urgently among Chinese children and adolescents because positive behaviors may,in turn,improve their future health outcomes.Older children and adolescents,especially those with lower parental education levels and lower family incomes,should be targeted as a priority.To address the health issue of OW/OB among children and adolescents,increasing MVPA,limiting screen time and improving sleep duration concurrently may be an effective approach,with sex-and age-specific strategies being encouraged.
Acknowledgments
We thank the students,parents,and staff for participating in the data collection and data entry.The study design and data collection were supported by the Key Project of the National Social Science Foundation of China(No.16ZDA227).The first and corresponding authors(STC and YL)are supported by grants from the National Social Science Foundation of China(No.19BTY077),the Philosophy and Social Science Foundation of Shanghai(No.A1904),and the Shanghai Key Laboratory of Human Performance(Shanghai University of Sport,No.11DZ2261100).
Authors’contributions
STC,YL,JTH,YT,and PC conceptualized,designed this study,analyzed the data,interpreted the data,and drafted the manuscript;MST provided intellectual guidance in improving the manuscript;ZBC,JZ,ZZ,XW,LW,and YC assisted in revising the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin