Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
2021-05-22AntonioGrHermosoYsminEzztvrRobinsonRmrezelezJoriOlloquequiMikelIzquiero
Antonio Gr′ı-Hermoso,Ysmin Ezztvr,Robinson Rm′ırez-V′elez,Jori Olloquequi,Mikel Izquiero
a Navarrabiomed,Navarra Hospital Complex(CHN),Public University of Navarra(UPNA),IdiSNA,Pamplona 31008,Spain
b University of Santiago of Chile(USACH),Sciences of Physical Activity,Sports and Health School,Santiago 71783-5,Chile
c Exercise Intervention for Health Research Group(EXINH-RG),Department of Physiotherapy,Universitat de Val`encia,Valencia 46010,Spain
d Institute of Biomedical Sciences,Faculthy of Health Sciences,Universidad Aut′onoma de Chile,Talca 3460000,Chile
Abstract Objective:This study sought to analyze the prospective association between vigorous-intensity physical activity(VPA)and health-related outcomes in children and adolescents. Methods:Studies reporting associations between device-measured VPA and health-related factors in children and adolescents aged 3-18 years were identified through database searches(MEDLINE,EMBASE,and SPORTDiscus).Correlation coefficients were pooled if outcomes were reported by at least 3 studies,using DerSimonian-Laird random effects models. Results:Data from 23 studies including 13,674 participants were pooled using random effects models.Significant associations were found between VPA at baseline and overall adiposity(r=-0.09,95%confidence interval(95%CI):-0.15 to-0.03;p=0.002;I2=89.8%),cardiometabolic risk score(r=-0.13,95%CI:-0.24 to-0.02,p=0.020;I2=69.6%),cardiorespiratory fitness(r=0.25,95%CI:0.15-0.35;p<0.001;I2=57.2%),and total body bone mineral density(r=0.16,95%CI:0.06 to 0.25;p=0.001;I2=0%). Conclusion:VPA seems to be negatively related to adiposity and cardiometabolic risk score and positively related to cardiorespiratory fitness and total body bone mineral density among children and adolescents at follow-up.Therefore,our findings support the need to strengthen physical activity recommendations regarding VPA due to its health benefits in children and adolescents.
Keywords:Accelerometry;Adiposity;Fitness;Physical activity
1.Introduction
There is robust evidence that physical activity(PA)in youth,specifically moderate-to-vigorous PA(MVPA;i.e.,a combination of moderate and vigorous PA),is strongly associated with several favorable health-related outcomes.1Accordingly,many national and international organizations have developed guidelines recommending that children and adolescents accumulate at least 60 min of MVPA daily.1-3These guidelines also recommend the inclusion of vigorous-intensity,bone-strengthening,and muscle-strengthening PAs at least 3 times weekly.1-3
Most exercise-related research in youth has been focused on MVPA,4,5and there is less evidence for a link between vigorous PA(VPA)and health outcomes in this population.In this regard,2 narrative reviews suggested that VPA may be especially beneficial for youth and may even bring more benefits than moderate-intensity activities.6,7However,the findings supporting the favorable associations between VPA and health-related outcomes in youth are typically derived from cross-sectional studies,and it is unclear whether the relationship is temporal in nature.
The sporadic nature of PA in youth is characterized by daily brief intermittent bouts of VPA.8Several studies suggest that every minute of VPA favors the same improvements in adiposity as 2 min or 3 min of moderate PA,9,10and it therefore seems reasonable to think that this type of PA is more attainable by children and adolescents;that is,VPA may be more attainable simply because a health-improving dose is less time consuming to attain.Because each PA intensity seems to provide different benefits,11this type of study could provide important information for those who develop national and international PA guidelines and determine how much daily VPA children and adolescents should be acquiring.To date,however,only a limited number of longitudinal studies have analyzed associations between VPA and health-related outcomes among youth,with inconsistent results.6,12Thus,the purpose of the present study was to analyzes the prospective association between VPA and health-related factors in children and adolescents.
2.Methods
The protocol was published in the International Platform of Registered Systematic Review and Meta-analysis Protocols under registration number(INPLASY202060082)and was conducted in accordance with Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)guidelines.13
2.1.Search strategy
The search was performed independently by 2 authors(AGH and YE)in the electronic databases MEDLINE,EMBASE,and SPORTDiscus,from inception to September 2020.Studies had to be observational prospective reports on the associations between device-measured VPA and healthrelated outcomes in children and adolescents.We combined variations of terms related to children and adolescents(e.g.,pediatrics,child,adolescent,youth*,paediatr*or pediatr*or infant*or child*or teenage*or adolescen*or pre-schooler*or pre-schooler*or schoolchild*or girl*or boy*or teen*),VPA(e.g.,vigorous physical activity,vigorous exercise),device-measured VPA(e.g.,accelerometer,heart rate monitor),and health-related factors(e.g.,body mass index,body fat,fat mass index,waist circumference,bone health,cardiometabolic risk factors,health-related physical fitness)(Supplementary Material 1).Hand-searching of reference lists of potentially eligible studies was undertaken to identify additional articles.Only studies published in peer-reviewed English-language journals were considered.
2.2.Selection criteria
To be included in our systematic review and meta-analysis,each article had to include the following elements:(1)exposure:device-measured VPA(e.g.,accelerometers,heart rate monitors,or similars);(2)population:children and adolescents aged 3 years up to 18 years at baseline(mean age);(3)outcomes:health-related factors,including adiposity(e.g.,body mass index,body fat,fat mass index,waist circumference),cardiometabolic outcomes(e.g.,cardiometabolic risk score,systolic blood pressure,homeostatic model assessment for insulin resistance),bone outcomes(e.g.,total body bone mineral density(BMD)and bone mineral content),and/or healthrelated physical fitness(e.g.,cardiorespiratory fitness,muscular fitness,speed-agility);and(4)study design:observational prospective cohort studies.Disagreements or uncertainties were discussed and resolved by consensus with 2 other authors(RRV and MI),and reasons for exclusions were recorded.
2.3.Data collection process and data items
Two authors(AGH and YE)extracted the following information for each study:study characteristics(e.g.,country,follow-up duration),population characteristics(e.g.,sex,age),VPA data reduction(e.g.,wear time in terms of days,number of valid days,epochs,cut-points),and analysis and study results(e.g.,adjusted variables,outcome of interest).Study authors were contacted to retrieve any missing data or to seek clarification if inadequate or insufficient information was detected.
2.4.Risk of bias and quality assessment in individual studies
The risk of bias was assessed by the Quality Assessment Tool for Observational Cohort and Cross-sectional Studies.14This methodological tool is composed of 14 items classified as“yes”,“no”,or“not reported”.Two authors(YE and AGH)conducted the risk-of-bias assessment independently.If necessary,a third author(RRV)was consulted.For Item 9—“Were the exposure measures(independent variables)clearly defined,valid,reliable,and implemented consistently across all study participants?”,and Item 14—“Were key potential confounding variables measured and adjusted statistically for their impact on the relationship between exposure(s)and outcome(s)?”,we have included additional details in order to consider specific and topic-relevant biases.For Item 9,it was considered“yes”if the study used an epoch≤15 s for the reduction of VPA data;15for Item 14,it was considered“yes”if the analysis was adjusted at least for baseline values of the outcome(the strongest confounder in prospective analyses)and sedentary time.
2.5.Meta-analysis
All analyses were performed using STATA Version 16.1(STATA Corp.,College Station,TX,USA).We used the correlation coefficient(r)as the main effect size for the present study.We converted other estimations(e.g.,standardized regression coefficients,unstandardized regression coefficients,standardized mean differences(Cohen’sd),and odds ratios)to correlation coefficients according to their corresponding formulas.16-18We selected fully adjusted models,partial models,or unadjusted models according to availability(i.e.,in that order).DerSimonian-Laird random effects models19were used to pool correlation coefficients if outcomes were reported by at least 3 studies.Separate pooled analyses were conducted on the following parameters based on the available data:overweight/obesity,body mass index,waist circumference,body fat,fat mass index,cardiometabolic risk score,systolic blood pressure,cardiorespiratory fitness,total body BMD,lumbar spine BMD,and femoral neck BMD.Also,we determined an overall effect on adiposity parameters according to Cliff et al.20To avoid duplication,we selected only 1 coefficient from each study using the following hierarchy:(1)body fat measured by dual-energy X-ray absorptiometry;(2)body fat measured by skinfolds thickness;(3)body fat measured by bioelectrical impedance analysis;(4)waist circumference;and(5)body mass index and overweight/obesity.
Random effects models19were used to account for anticipated between-study heterogeneity,calculated using the total variance(Q)and the inconsistency index(I2).21Inconsistency was considered insignificant forI2<25%,low for 25%≤I2<50%,moderate for 50%≤I2<75%,and high forI2≥75%.22
Publication bias was determined by visual examination of funnel plots(we have only used this visual test for overall adiposity due to the limited number of studies in the rest of the parameters).23Also,small-study effects bias was assessed using Egger’s test24in all of the parameters.
Finally,random-effects meta-regression analyses using method of moments25were estimated to independently evaluate whether results were different by length of follow-up(months).Sub-group analyses according to age and sex were not possible because most of the included studies used both sexes and ages(children and adolescents)in their analyses.
3.Results
3.1.Study selection
A total of 3612 potentially relevant articles were identified,and,after screening for duplicates,601 full-text studies were assessed for inclusion after checking titles and abstracts.Finally,23 studies met the eligibility criteria and were included in the systematic review26-48and 21 in the metaanalysis.The reasons for exclusion based on full texts are reported in Supplementary Material 2.The PRISMA flow diagram illustrating the number of studies excluded at each stage of the systematic review and meta-analysis is shown in Fig.1.
3.2.Study characteristics
The end points for all 23 prospective cohort studies are listed in Table 1.The studies involved a total sample of 13,674 children and adolescents with mean ages between 4.5 years and 17.5 years at baseline(mean age:10.0 years).Most studies included boys and girls(49.7%and 50.3%,respectively),with the exception of 5 studies that included only boys29,33,36,45,47and two only girls.39,42Sample sizes across studies ranged from 8833to 477044participants.The mean follow-up time was 38.5 months(between 7 and 120 months).

Fig.1.Preferred Reporting Items for Systematic Reviews and Meta-Analyses(PRISMA)flow chart.
The correlation coefficient was presented in 4 studies33,43,45,47.Other effect sizes were converted from studies reportingβcoefficients(n=17),analysis of variance(ANOVA)(n=1),and odds ratio(n=1).Most of the studies analyzed associations between VPA at baseline and the dependent variables at follow-up(n=19)(i.e.,a determinant model);other studies also analyzed the association between changes in the VPA and changes in the dependent variables during follow-up(n=8)(i.e.,a change model).Regarding the covariates used in the statistical models applied,there was much heterogeneity between studies and few of these included baseline values of the outcomes or other important covariables such as maturation or time spent in other intensity domains.
3.3.Measurements
All studies device-measured VPA using accelerometers placed on the hip,waist,or wrist,and 2 studies used an Actigraph chestworn monitoring device.35,43The VPA data reduction across studies was diverse,with different cut-off points characterizing VPA,epochs,total days of use,criteria for non-wear time and minimum wear time per day used for analysis.
Regarding health-related outcomes,most studies reported data on adiposity,26-28,32,34,35,37,38,41-44,47,48cardiometabolic risk factors,26,30,32,35,38bone outcomes,29,31,33,36,39,40,45,46and health-related physical fitness27,38,41,48(Table 1).
3.4.Risk of bias and quality assessment within studies
All 23 studies met at least 8 criteria(between 8 and 12 criteria)and were considered to have low-moderate methodological quality.Overall,all studies satisfied Items 1,2,6,7,8,and 11.In contrast,only 2 studies34,43fulfilled Item 12(regarding assessors blinding),and no studies fulfilled Item 14(i.e.,regarding potential confounding variables and it adjust in the analyses).The average score was 9.6 of 14(Supplementary Table 1).
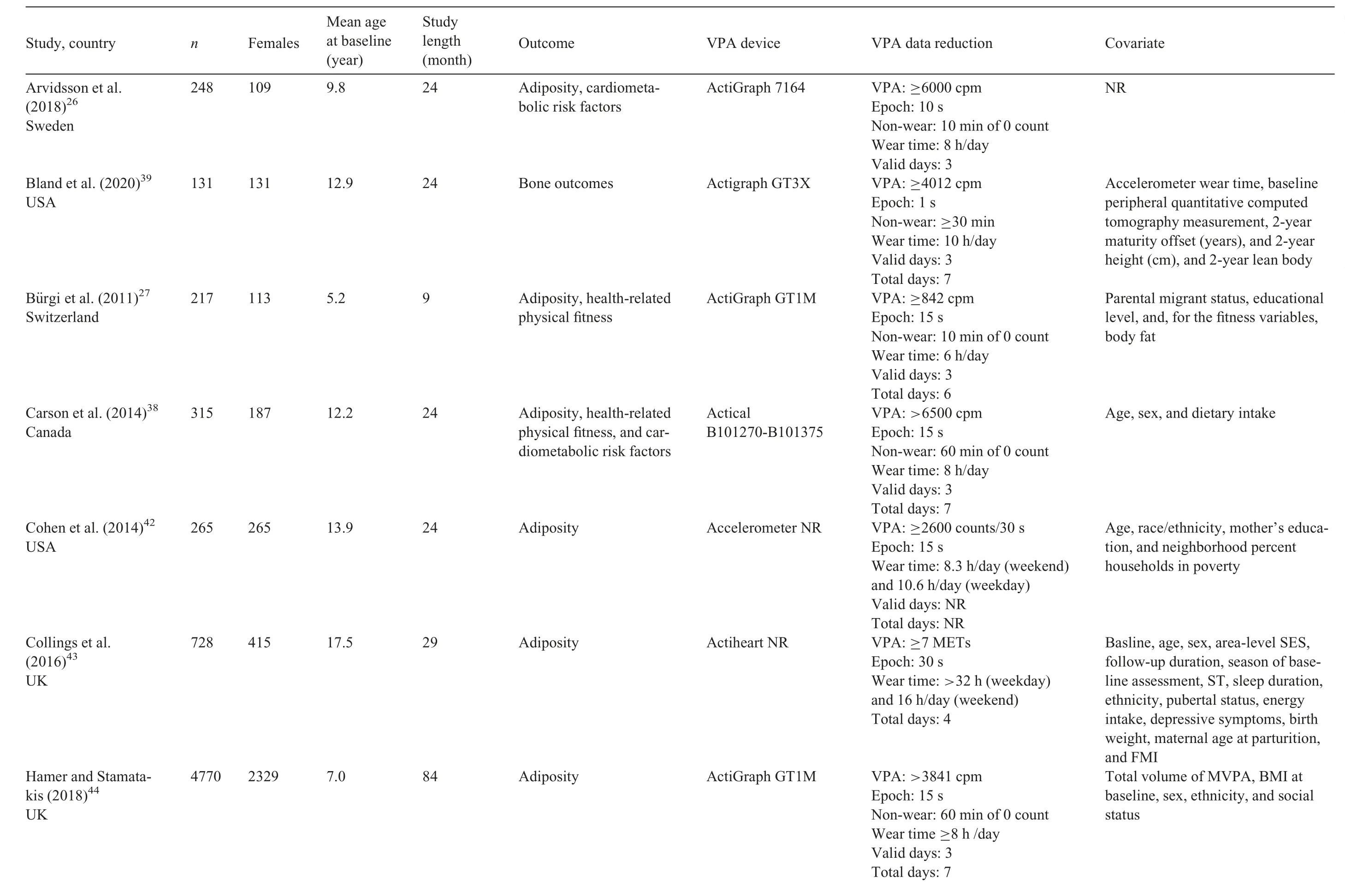
Table 1Study characteristics
(continued on next page)(continued on next page)
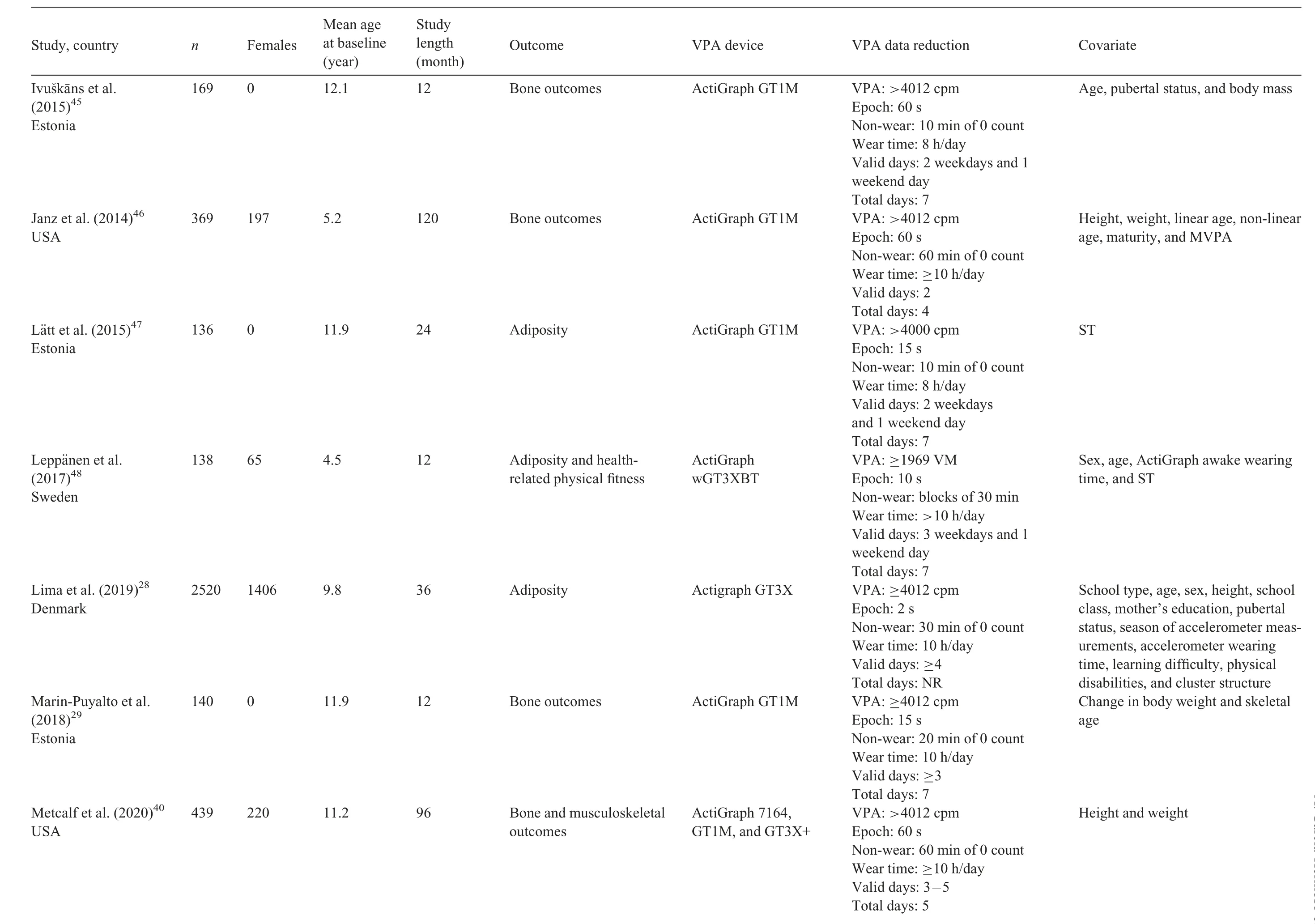
Table 1(Continued)
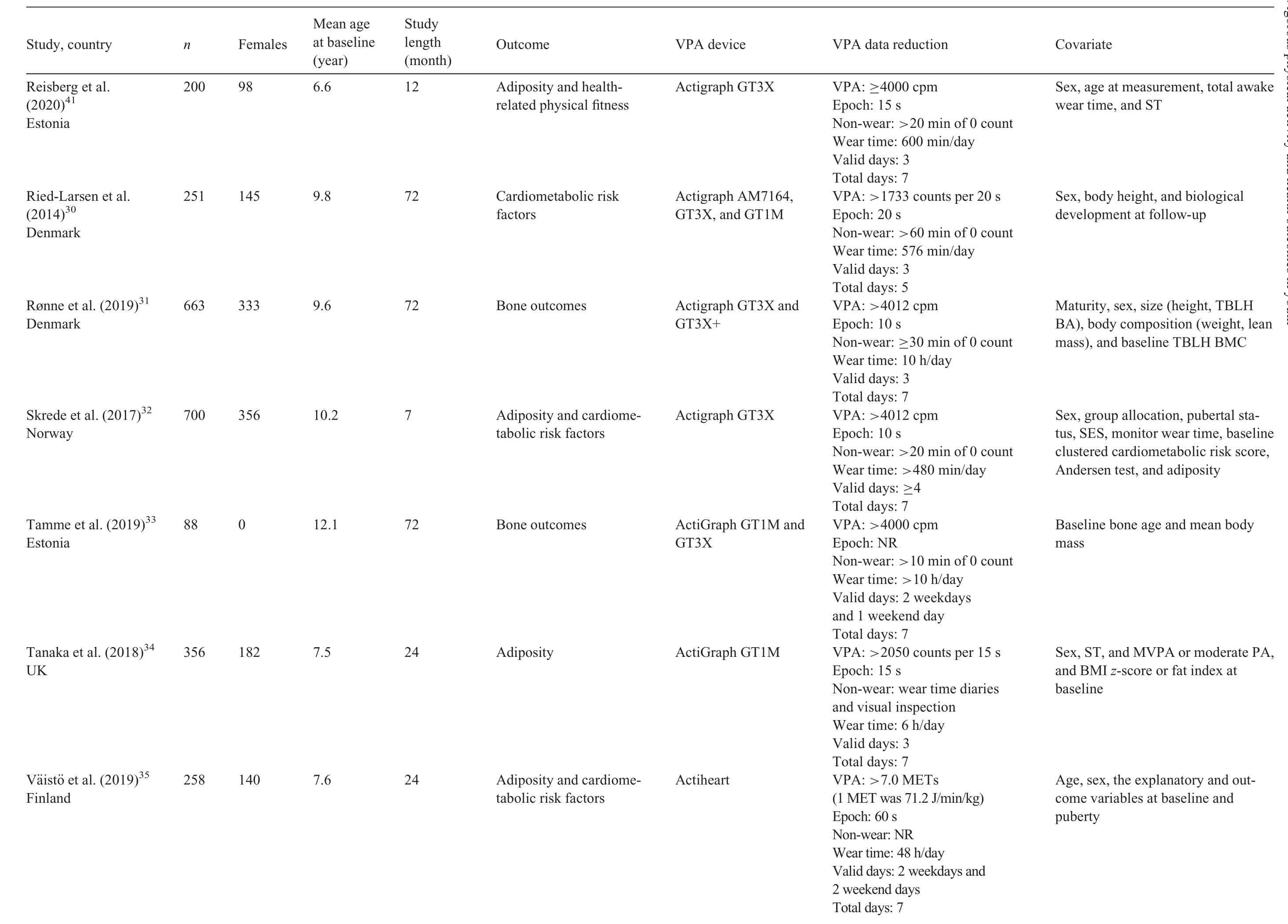
Table 1(Continued)
(continued on next page)
3.5.Synthesis of results
The association between VPA and overall adiposity was statistically signifi cant(r=-0.09,95% confi dence interval(95%CI):-0.15 to-0.03;p=0.002;I2=89.8%;n=14)(Fig.2).For each adiposity outcome separately,VPA was negatively associated with overweight/obesity(r=-0.20,95%CI:-0.38 to-0.03;p=0.022;I2=82.2%;n=4)and waist circumference(r=-0.06,95%CI:-0.10 to-0.01;p=0.016;I2=25.7%;n=5)(Supplementary Fig.1).Analyzing changes along time,change in VPA was not negatively related to change in overall adiposity(r=-0.11,95%CI:-0.26 to 0.04;p=0.139;I2=84.7%;n=4)(Supplementary Fig.2).
Regarding cardiometabolic risk factors,there was a negative relationship between VPA and cardiometabolic risk score(r=-0.13,95%CI:-0.24 to-0.02;p=0.020;I2=69.6%;n=3)(Fig.3).Also,VPA was positively related to cardiorespiratory fi tness(r=0.25,95%CI:0.15-0.35;p<0.001;I2=57.2%;n=4)(Fig.4).Finally,the results indicated a positive association between VPA and total body BMD(r=0.16,95%CI:0.06-0.25;p=0.001;I2=0%;n=3)(Fig.5).
Based on meta-regression analysis,there was no signifi cant effect of length of follow-up(β=0.001,95%CI:-0.004 to 0.006,p=0.663)on the correlation coeffi cient estimate for overall adiposity(Supplementary Fig.3).
Egger’s test indicated no small-study effects bias for any outcome(overall adiposity,p=0.117;cardiometabolic risk factors,p=0.273;cardiorespiratory fi tness,p=0.378;speedagility,p=0.057;and bone and musculoskeletal outcomes,p=0.756).The funnel plot for overall adiposity also showed no asymmetry(Supplementary Fig.4).
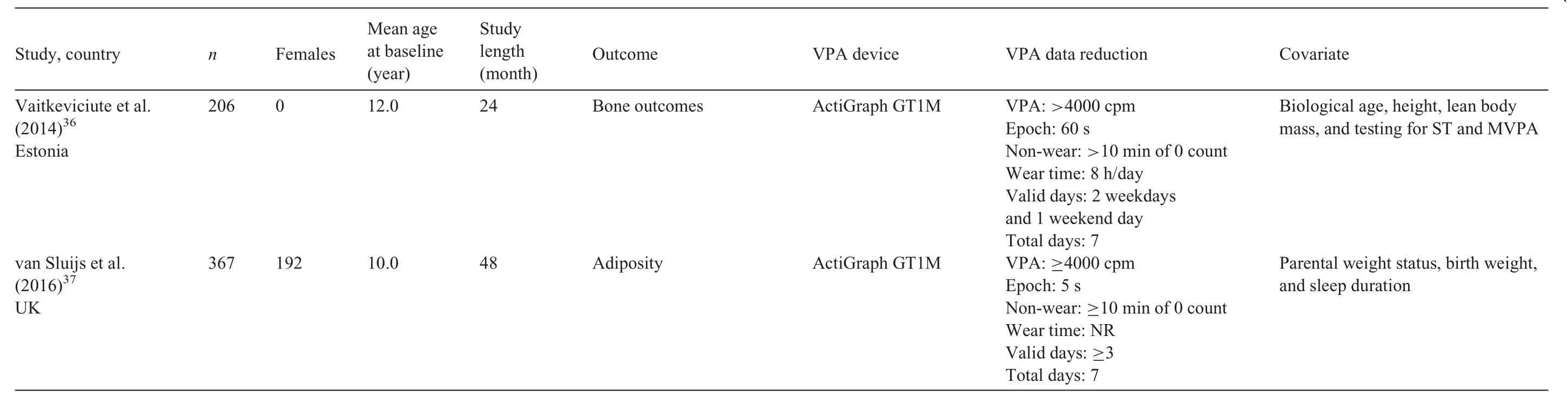
Table 1(Continued)
4.Discussion
The present systematic revie w and meta-analysis summarizes the evidence for the prospective association between VPA and health-related factors among children and adolescents.Overall,VPA seems to be negatively related to adiposity and cardiometabolic risk score and positively related to cardiorespiratory fi tness and total body BMD later in life.
Our results are consistent with prior reports in the literature given that a number of previous reviews have emphasized that time spent in higher intensities of PA is a signifi cant predictor of levels of adiposity in children and adolescents.6,11,12Owens et al.12suggested that VPA provided adiposity-related benefi ts to children and adolescents over and above those obtained from moderate or light PA.Specifi cally,the authors stated that every minute of VPA favors the same improvements in adiposity as 2 or 3 min of moderate PA,in accordance with cross-sectional studies.9,10This is also consistent with a review published by Gralla et al.,6which reported favorable associations between VPA and adiposity in children and adolescents,particularly in studies where participants engaged in an average of at least 10 min of VPA.The majority of the studies included in the aforementioned reviews are,however,cross-sectional in nature,and therefore the directionality of the relationship between VPA and fatness parameters cannot be established;34it is possible that excess adiposity may cause less VPA.
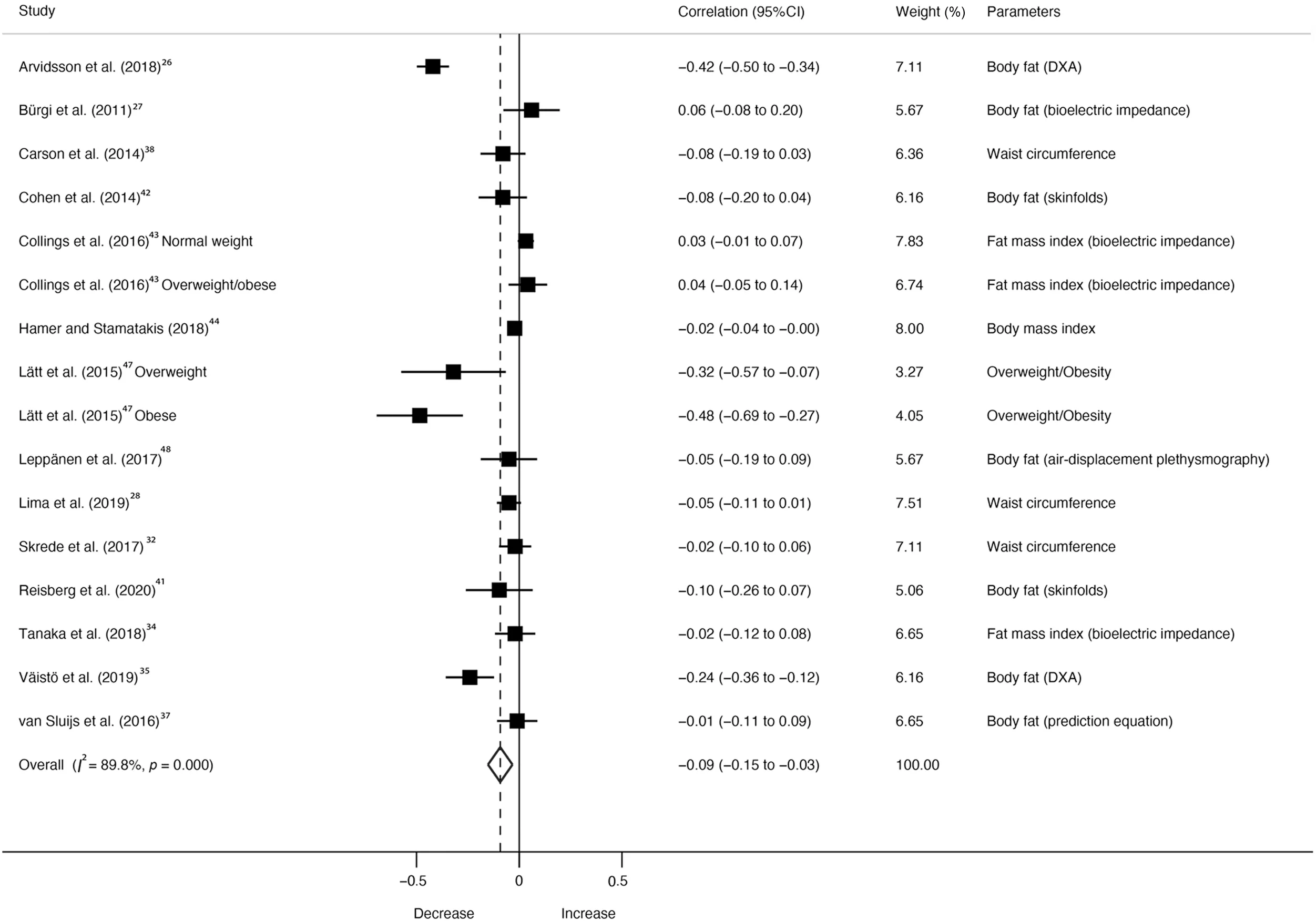
Fig.2.Forest plot showing the correlation of vigorous physical activity at baseline on adiposity at follow-up for each adiposity study.Weights are from random effects analysis.p value represents significance for the heterogeneity test.95%CI=95%confidence interval;DXA=dual energy X-ray absorptiometry.
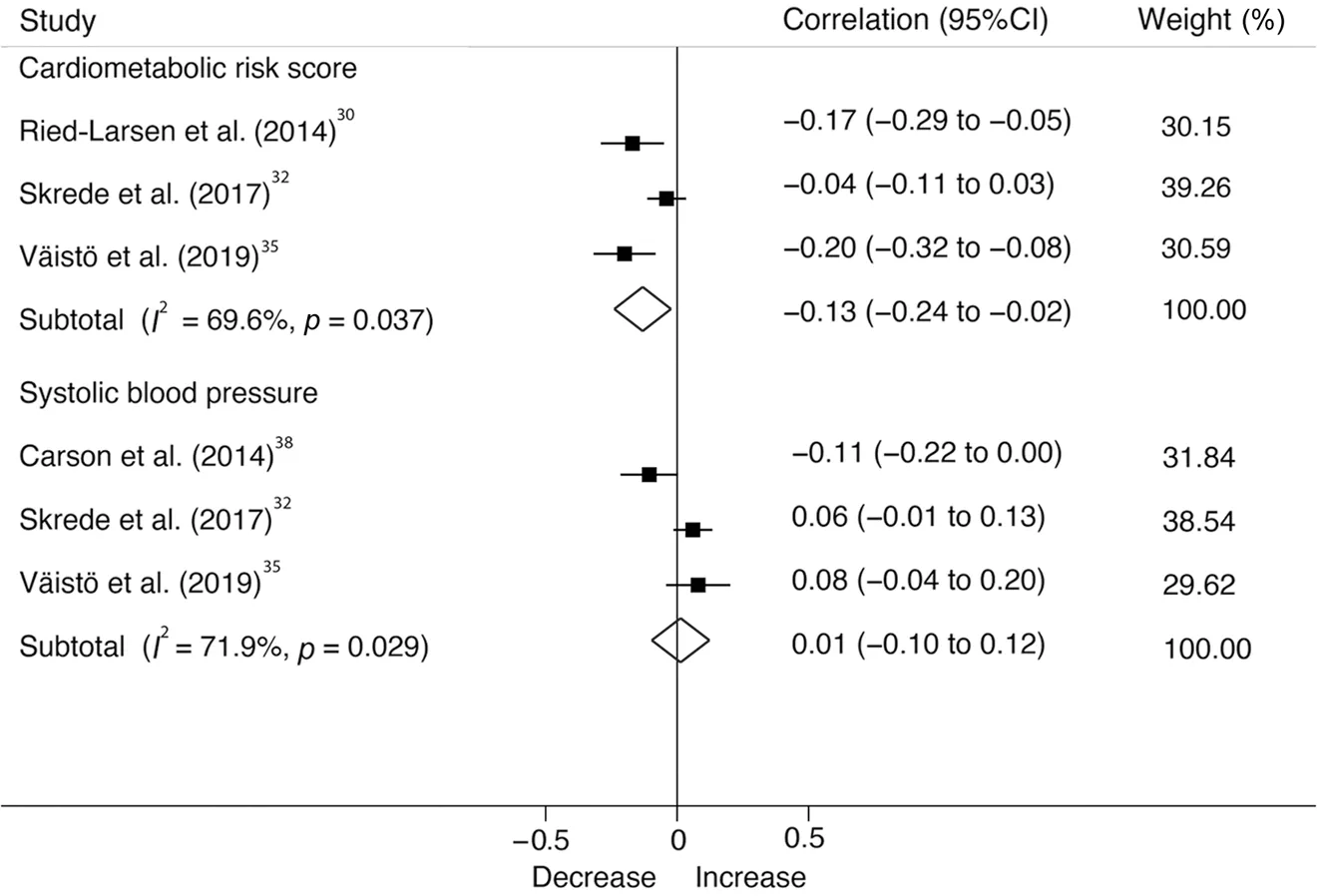
Fig.3.Forest plot showing the correlation of vigorous physical activity at baseline on cardiometabolic risk score and systolic blood pressure at follow-up for each study.Weights are from random effects analysis.p value represents significance for the heterogeneity test.95%CI=95%confidence interval.
There is also a growing body of evidence suggesting that VPA may favor a healthier cardiometabolic profile among youth,7but equivocal findings were reported in the aforementioned reviews.For example,Gralla et al.6reported that VPA does not have a strong relationship with cardiometabolic risk score in youth.By contrast,Owens et al.12suggested that VPA is associated with a more favorable blood lipid and glucose-insulin profile,which matches the results of Väistö et al.35Consistent with the literature about combined moderate and VPA,4our meta-analysis reveals that VPA is inversely related to cardiometabolic risk score,which is also supported by experimental studies.49There are several possible biological mechanisms that explain our results.For example,PA improves insulin action in skeletal muscle and glucose transport,50and also improves fat metabolism and increases blood flow and oxygen supply through the increased density of capillaries and vasodilatation by nitric oxide.51In contrast to earlier findings,51however,no relationship between VPA and systolic blood pressure was detected in our study,which differs from studies using high-intensity training52or even moderate-intensity training among obese youths.53This inconsistency may be due to the initial health status of youth in various studies,which may greatly affect the observed association54(i.e.,associations are more likely to occur in high-risk participants such as obese children and adolescents).53
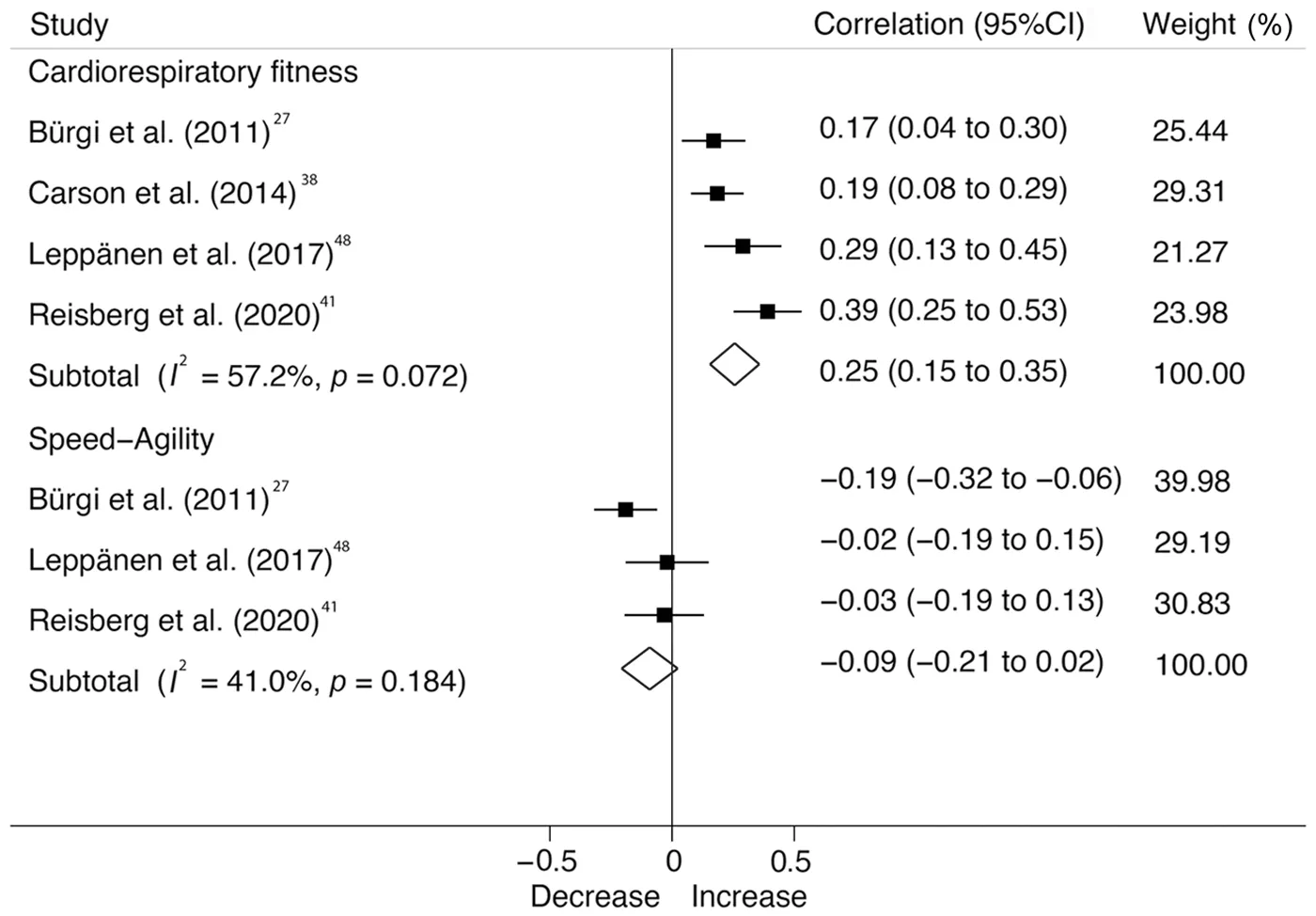
Fig.4.Forest plot showing the correlation of vigorous physical activity at baseline on cardiorespiratory fitness and speed-agility at follow-up for each study.Weights are from random effects analysis.p value represents significance for the heterogeneity test.95%CI=95%confidence interval.
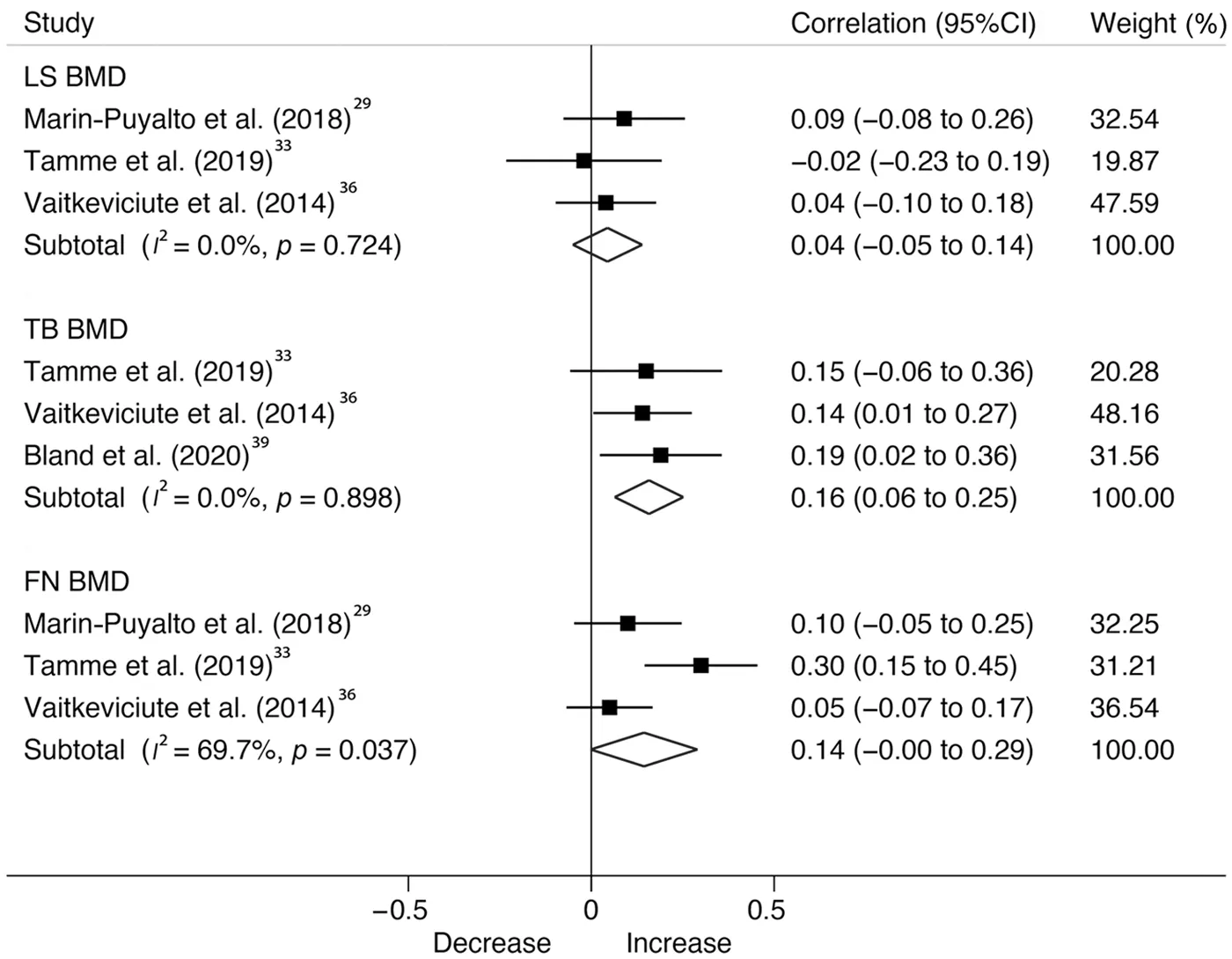
Fig.5.Forest plot showing the correlation of vigorous physical activity at baseline on bone outcomes at follow-up for each study.Weights are from random effects analysis.p value represents significance for the heterogeneity test.95%CI=95%confidence interval;BMD=bone mineral density;FN=femoral neck;LS=lumbar spine;TB=total body.
In line with previous reviews,6,12we found that VPA is consistently associated with cardiorespiratory fitness.Published experimental studies also indicate that VPA is as effective,55or even superior,to moderate PA for improving cardiorespiratory fitness among children and adolescents.53For example,a randomized controlled trial in children with obesity reported that 6 weeks of high-intensity interval training using gamesbased exercises led to an improvement in cardiorespiratory fitness.55In addition,a meta-analysis of randomized controlled trials suggested that high-intensity training in children with obesity is considered a more effective intervention for improving cardiorespiratory fitness than other training protocols with lower intensities.53PA at a higher intensity could favor an increase in oxygen availability through central effects(such as maximal cardiac output,total hemoglobin,and blood plasma volume).56VPA also seems to increase muscle oxidative potential and the ability to extract and use available oxygen,reflecting peripheral adaptations.57Our findings have important implications since cardiorespiratory fitness is a central marker of health status during childhood and adolescence,and also in later life.58In light of the small number of studies involving muscular fitness parameters in the meta-analysis,the results could not be pooled to determine their relationship with VPA.However,Leppänen et al.48reported that VPA among children 4.5 years old was related to higher muscular strength(r=0.20 andr=0.36 in handgrip and standing long-jump tests,respectively)1 year later.
Regarding bone health,it is generally acknowledged that weight-bearing activities,more specifically high-impact activities,during youth are effective for promoting bone health.59,60Our meta-analysis suggests that VPA favors higher total body BMD later in life.The results of a recent 8-year prospective study by Metcalf et al.40showed that accumulating 5 extra minutes per day of VPA was associated with up to 3.0%and 5.1% greater bone structural outcomes by age 19 years in boys and girls,respectively.The Rønne et al’s.study31meta-analyzed here and the aforementioned Metcalf et al.’s study40underpin the notion that greater attention should be placed on promoting high-impact VPA throughout adolescence and emerging adulthood to maximize bone strength and reduce fracture risk.Indeed,Ivuˇska ns et al.45also found that increases in VPA during a 12-month period favors bone mineral acquisition in peripubertal boys.Therefore,although we have included limited studies,the existing data from longitudinal designs and experimental trials59point to bone health advantages for children and adolescents engaged in daily high-impact VPA.
Overall,several methodological factors could have potentially influenced our study results and heterogeneity.First,there are discrepancies regarding the reduction of accelerometer data;VPA cut-offs varied from≥842 counts per minute27to≥6500 counts per minute38in our meta-analysis,which could result in significantly different estimates of time spent in VPA.Also,a recent study recommends the use of short epochs when analyzing accelerometry data in youth in order to mirror their activity patterns and capture VPA correctly.61A majority of the included studies in our review used 10-60-s epochs,and therefore we could have underestimated the VPA levels.62These choices related to data reduction could impair the true association between VPA and health parameters and complicate comparability between studies.Unfortunately,evidence on reaching consensus on VPA data reduction protocols is currently lacking.Second,and no less important,are the statistical models applied in the included studies.Most of the studies used a determinant model,in which the follow-up outcome or its change is regressed on a baseline value;however,not all studies adjusted for baseline values of the outcome,which is the strongest confounder in prospective analyses.4Also,few studies34,36,43,47,48adjusted their analysis by time spent in other intensity domains.Conversely,these intensities are codependent and difficult to separate statistically;recent studies suggest more appropriate analytical methods such as compositional data analysis.63Therefore,not including both confounding variables could be considered a major methodological flaw.Third,our findings should be interpreted with caution given the short duration of follow-up time in the included studies(the mean follow-up time was 38.5 months).Fourth,many prospective studies in the literature only include MVPA and/or sedentary time levels in their results,creating one of the strongest biases in our study(i.e.,selection bias).Fifth,correlation coefficient could be a poor metric because it is difficult to translate into clinical findings;however,this coefficient is standardized and can itself serve as an effect size.25Finally,reverse causality could also be possible given that the prospective design of the included studies did not eliminate the possibility of bi-directional associations.
5.Conclusion
Overall,VPA seems to be negatively related to adiposity and cardiometabolic risk score and positively related to cardiorespiratory fitness and total body BMD among children and adolescents at follow-up.Our results support the need to further strengthen VPA recommendations for children and adolescents.However,more studies are warranted,including rigorous experimental trials,to confirm the optimal dose of VPA for overall health status among youth.
Acknowledgments
AGH is a Miguel Servet Fellow(Instituto de Salud Carlos III-CP18/0150).RRV is funded in part by a Postdoctoral Fellowship Resolution ID 420/2019 of the Universidad P′ublica de Navarra.
Authors’contributions
AGH and YE conceptualized and designed the study,drafted the initial manuscript,and reviewed and revised the manuscript;RRV and JO designed the data collection instruments,collected data,carried out the initial analyses,and reviewed and revised the manuscript;MI conceptualized and designed the study,coordinated and supervised data collection,and critically reviewed the manuscript for important intellectual content.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found,in the online version,at doi:10.1016/j.jshs.2020.12.001.
杂志排行

Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Conceptual physical education:A course for the future Charles B.Corbin
- The impact of the coronavirus disease 2019 pandemic on physical activity in U.S.children