The impact of the coronavirus disease 2019 pandemic on physical activity in U.S.children
2021-05-22KirstnTulhinFrnisWilshwStvnsJrXinliGuToZhnHthrRobrtsJnKllrDnDmpsyJustinBorhrKllyJnsJonthnVnPlt
Kirstn Tulhin-Frnis,Wilshw Stvns Jr.,Xinli Gu,To Zhn,Hthr Robrts,Jn Kllr,Dn Dmpsy,Justin Borhr,Klly Jns,Jonthn VnPlt
a Division of Movement Science,Research Department,Scottish Rite for Children,Dallas,TX 75219,USA
b Department of Health Care Sciences,School of Health Professions,University of Texas Southwestern Medical Center,Dallas,TX 75235,USA
c Department of Kinesiology,University of Texas at Arlington,Arlington,TX 76019,USA
d Departrment of Kinesiology,Health Promotion and Recreation,College of Education,University of North Texas,Denton,TX 76201,USA
e Department of Occupational Therapy,Texas Woman’s University,Denton,TX 76204,USA
f Division of Clinical Research,Research Department,Scottish Rite for Children,Dallas,TX 75219,USA
g Therapeutic Recreation Department,Scottish Rite for Children,Dallas,TX 75219,USA
Abstract Background:Daily moderate-to-vigorous physical activity(MVPA)is vital to the physical,mental,and social well-being of children.Early restrictions during the coronavirus disease 2019(COVID-19)pandemic included the closure of schools and physical activity(PA)amenities across the US.This study aimed to examine the impact of the pandemic on the PA and play behavior of U.S.children and to provide evidencebased recommendations to improve their PA. Methods:A cross-sectional,online,parent-reported survey was conducted of children aged 3-18 years between April and June 2020 to assess light PA and MVPA using a modified Godin Leisure-Time Exercise Questionnaire.Additional items included family/child socioeconomic demographics,child adaptability to the pandemic,and community access.The survey was shared through social media and snowball sampling distribution. Results:Analysis of 1310 surveys indicated child PA scores declined significantly during the pandemic(from 56.6 to 44.6,max 119,p<0.001).Specifically,MVPA score decreased(from 46.7 to 34.7,max 98,p<0.001)while light PA remained the same.Age-based changes were seen in the quantity,variety,and intensity of PA,with the lowest pandemic-related impact seen in preschoolers and the highest in high schoolers(-4.7 vs.-17.2,p<0.001).Community-based peer PA decreased across all age groups. Conclusion:This study shows decreased PA levels in U.S.children,according to parent reporting,during the COVID-19 pandemic.Recommendations for community leaders,educators,and parents to improve PA in children are provided.With continued spread of COVID-19,these results and recommendations may be imperative to the physical well-being of U.S.children.
Keywords:Adolescents;COVID-19;Moderate-to-vigorous physical activity;Pediatric;Youth
1.Introduction
Severe acute respiratory syndrome coronavirus 2 and the coronavirus disease 2019(COVID-19)have led to social distancing restrictions across the US.Early pandemic responses included stay-at-home and/or shelter-in-place mandates in many counties and states,resulting in the closure of indoor/outdoor physical activity(PA)settings.1For children,this included the shutdown of schools,closure of public playgrounds,and cancellation of organized sports and recreational activities.
Health guidelines recommend children achieve 60 min of moderate-to-vigorous PA(MVPA)daily,2or approximately 12,000 steps,3to ensure healthy development.4Unfortunately,18%-20% of U.S.children aged 2-19 years are classified as obese.5,6Achieving recommended daily MVPA is a vital component of each child’s healthy lifestyle.Regular PA has multiple well-being benefits that extend beyond physical fitness,2including improved mental health,7-9and a reduction in anxiety and depression symptoms.8,9Furthermore,peer-to-peer interaction during PA is critical for social development.10-12
A recent strategic research agenda outlined objectives to understand the impact of the COVID-19 pandemic on PA in children and adults,1including the establishment of interventions and policy guidelines to increase PA during a pandemic.While many editorials and commentaries agree that restrictions/closures will have a significant impact on children,13-17there have been few self-or parent-reported studies on the impact of the pandemic on children’s PA.A study from China found that only 17% of children achieved sufficient levels of PA,with 66%rated as inactive during the pandemic.18Similar PA reductions were reported in Canadian children.19At the time of this paper,only 1 study had reported on quantitative(wearable sensor-based)PA levels in children during COVID-19 restrictions.20The impact of stay-at-home orders on the PA of U.S.children remains unclear.
While stay-at-home mandates in most U.S.communities have relaxed,there is speculation that spikes in COVID-19 cases or mediation to prevent future increases may lead to additional public closures and other restrictions in the coming months.21,22The aims of this study were to understand the impact of the early COVID-19 pandemic on PA and play behavior of U.S.children,along with changes in family dynamics and environmental access,as well as to provide recommendations to improve PA in U.S.children during a pandemic.Given the numerous health benefits of regular PA,the findings of this study will be foundational for policies developed by local,state,and federal leaders to address healthcare and educational needs impacting children/families.
2.Methods
Recruitment for this cross-sectional study focused on the state of Texas,with national distribution accomplished through social media(Twitter/Facebook)and snowball sampling,where participants were encouraged to freely share the survey link.This study was approved by the University of Texas Southwestern Medical Center Institutional Review Board.Flyers were emailed to schools,youth groups(sport teams,scouting groups,etc.),support groups for parents of children with special needs,cultural/religious organizations,and personal/professional contacts of the study team.Interested parties were encouraged to distribute flyers to their memberships.
The survey was active between April 4 and June 27,2020,while most U.S.areas were under government-mandated activity restriction,including social distancing,stay-at-home and/or shelter-in-place orders.Participants were at least 18 years of age and self-identified as a parent/guardian of a child(3-18 years of age)living in their household.A waiver of written informed consent was obtained from the University of Texas Southwestern Medical Center Institutional Review Board,which allowed participants to provide electronic consent upon survey initiation.
2.1.Survey construct
This anonymous survey used a socioecological model as its theoretical framework(Supplementary Fig.1)23and was managed using a research electronic data capture(REDCap)tool,24,25a secure,web-based software platform(https://project redcap.org/software/),hosted at Scottish Rite for Children.The survey took 1015 min to complete and consisted of 3 sections(Supplementary Table 1).Section 1 included an Institutional Review Board-approved study information letter and questions to confirm inclusion criteria/consent.Participants completed the survey for their household(Section 2)and for a single child(Section 3);they could repeat Section 3 for additional children.
Queried household information included type of dwelling and community,total household income,and highest parental education level.Child demographics included sex,race/ethnicity,and school grade/setting.A modified Physical Activity Neighborhood Environment Scale26built environment score(6 items,Cronbach’sα=0.800)and 4 subscores were determined.Scores ranged from 0 to 4,and higher values indicated more resources/safer environment.Subscores included:pedestrian(2 items,Cronbach’sα=0.864),cycling(2 items,Cronbach’sα=0.831),and recreational(2 items,Cronbach’sα=0.699)infrastructures;and neighborhood safety(2 items,Cronbach’sα=0.544).
Pre-pandemic and 7-day recall by parent report were used to estimate light,moderate,and strenuous intensity child PA volumes using modified 5-point Likert scales:none(0 point),1-2/week(1 point),3-4/week(3 points),5-6/week(5 points),and 7+/week(7 points).Responses were multiplied by 3(light),5(moderate),and 9(strenuous)to create a weighted Leisure-Time Score Index(unvalidated,modified Godin Leisure-Time Exercise Questionnaire(mGodin)).27Higher scores indicated more PA(mGodin Leisure-Time Score Index(LSI),3 items,range 0-119,Cronbach’sα=0.657).A moderate-strenuous subscore(mGodin-MVPA,2 items(moderate and strenuous items only),range 0-98,Cronbach’s α=0.657)was used to align with established PA guidelines for public health.2The mGodin-light PA was also evaluated.
Parents were queried on their child’s specific participation in organized sports/recreation,indoor and outdoor PA,and educational activities.PA was defined as yard,neighborhood or community outdoor PA and child-or parent-led and live or pre-recorded online,indoor PA.For each type of PA,parents were asked if the child participated in the activity pre-pandemic and within the last 7 days and,if so,with whom(alone,siblings,friends,parent,or family(2+household members)).Similarly,the child’s participation in educational activities(EduA)(writing,electronic,and fine art activities)were also recorded with respect to who led the activity(child-or parent-led,online-live,and online-video options)both pre-pandemic and for a 7-day recall.Parental PA levels(pre-pandemic and 7-day recall,10-point Likert scale)were also assessed.
Additional questions prompted parents to rate pandemicbased changes in their child’s daily activities,roles/responsibilities,and relationships with their siblings or parents,as well as the parent’s roles/responsibilities using 5-point Likert scales(strongly disagreetostrongly agree).Child-based items were averaged as a Family Dynamics score(4 items,Cronbach’s α=0.702).Higher values indicated more disruption to routines.Adjustment to the pandemic was assessed using an 11-point Likert scale measuring their child’s ability to transition to social distancing and shelter-in-place and child/parent stress levels.A Child Transition score was determined using the average of the 3 child-based items(Cronbach’sα=0.827).
2.2.Statistical analysis
Dependent measures included child mGodin-LSI,mGodin-MVPA,and mGodin-light PA scores,changes in the type of PA,EduA,and organized sport participation,parental PA level,and the Family Dynamic and Child Transition scores.Descriptive analysis was conducted with results reported as percentile frequencies or median/mean with associated 95% confidence intervals(95%CIs).Pre-to during-pandemic changes were compared using paired,two-tailed,Student’st/Wilcoxon signed-rank test.Welch’sttest was used to assess sex-based differences,and an analysis of variance(Tukeypost hoctest)was used to determine age group differences and age-sex interactions.Statistical significance SPSS(Version 26.0;IBM Corp.,Armonk,NY,USA)was set atα<0.05.
3.Results
There were 1696 surveys initiated by participants.Of those,84 responses were excluded for lack of consent or failure to meet inclusion criteria(Supplementary Fig.2),and another 302 were excluded due to respondents’failure to complete the first half of the survey on household demographics.The remaining 1310 surveys from 48 U.S.states and the U.S.Virgin Islands were included in the community resource analysis.Parents completed the child demographic and mGodin items in 1212 surveys and added 84 completions for additional children in the home.A total of 1296 responses were included in the child PA analysis.Overall 82.7% of included respondents(1083/1310)had fully completed child surveys.
3.1.Household and child demographics
Families tended to consist of 2 adults(80.1%)and 2 or more children(65.6%)living in detached,single-family homes(90.8%)in a suburban community(69.7%),with 98.0%having broadband internet access.The cohort was comprised of well-educated(4-year college degree or higher,88.3%)and middle/upper-income households(93.5%),with few low-income families(6.5%)(Table 1).
Children were predominately white(83.2%)and non-Hispanic(87.3%),evenly split by sex(51.3% female),with no mobility impairments(93.8%).Of the children,47.5%were in elementary school,with an even distribution of those remaining across preschool(15.2%),middle school(21.5%),and high school(15.7%).The majority of children attended public/charter(70.9%)or private school(22.3%)(Table 1).
3.2.Pre-pandemic built environment and changes in community PA resource usage
The Physical Activity Neighborhood Environment Scale score was 2.5(95%CI:2.5-2.6).Cycling infrastructure scores were the lowest(1.9,95%CI:1.8-1.9)when compared to pedestrian(2.6,95%CI:2.5-2.7)and recreation(3.1,95%CI:3.1-3.2)infrastructures(Supplementary Fig.3).Sidewalk and cycling path use increased in 60.1% and 42.8% of households,respectively;however,recreation facilities(58.3%)and organized sports(78.9%)were often inaccessible due to pandemic-based closures.
3.3.Child and parent PA levels
Child mGodin-LSI scores decreased significantly during the pandemic(from 56.6 to 44.6,p<0.001).More important,MVPA decreased(from 46.7 to 34.7,p<0.001),while light PA remained level(from 10.0 to 9.9,p=0.899).The median pre-pandemic parent PA level was 6.While this level did not change significantly(p=0.94),29.9% of parents reported decreases in PA of 2 points or more during the pandemic.
3.4.Child PA levels:age/sex differences
Boys had higher pre-pandemic LSI scores compared to girls(59.1,95%CI:56.7-61.4vs.54.0,95%CI:51.7-56.4;p=0.01)due to higher MVPA(49.2,95%CI:47.1-51.2vs.44.1,95%CI:42.1-46.1;p<0.001).Boys demonstrated a larger decrease in LSI scores(-14.5,95%CI:-17.2 to-11.9vs.-9.4,95%CI:-11.9 to-6.9;p=0.008),which lead to similar LSI scores compared to girls(44.6,95%CI:42.1-47.0vs.44.7,95%CI:42.3-47.2;p=0.915)during the pandemic.Age group comparisons indicated that pre-pandemic preschool LSI scores(61.3,95%CI:56.8-65.7)differed from those of middle school(53.5,95%CI:50.1-56.8;p=0.013)and high school students(49.2,95%CI:44.8-53.6,p<0.001).During the pandemic,there were significant decreases in LSI and MVPA scores across all ages(p<0.05).Decreases in LSI were smaller in preschoolers(-4.7,95%CI:-9.4 to-0.0)compared to all other groups,including high schoolers(-17.2,95%CI:-21.9 to-12.6;p<0.001),middle schoolers(-14.1,95%CI:-17.7 to-10.5;p<0.001),and elementary children(-11.6,95%CI:-14.3 to-8.9;p=0.04).More importantly,MVPA decreased across age groups,as it ranged from 42.7(95%CI:38.5-46.8)in preschoolers to 25.6(95%CI:22.1-29.0)in high schoolers(Fig.1).
3.5.Change in the type of PAs
Pre-pandemic,78.6% of children participated in org anized sports/recreation,of which 80.3% parents reported that these activities were cancelled due to the pandemic(Table 2).The type of PA that children participated in varied significantly with age and sex(Fig.2).Community based peer-play PA decreased across all groups(14.9%-27.7%,p<0.05).Preschool and elementary children also experienced decreased community activity with their parents and family members(8.3%-23.5%,p<0.05).Yard/neighborhood(18.1%-39.8%,p<0.05)and indoor child/parent led play(6.8%-23.4%,p<0.05)with peers decreased across age groups/sexes.Independent yard play increased for preschool and elementary girls(20.3% and 5.7%,respectively;p<0.05)as well as elementary and middle school boys(5.1%and 13.8%,respectively;p<0.05).High schoolers did not demonstrate significant increases in any outdoor PA.Independent online-based PA increased between 7.1% and 20.1%in preschoolers and elementary-aged children.
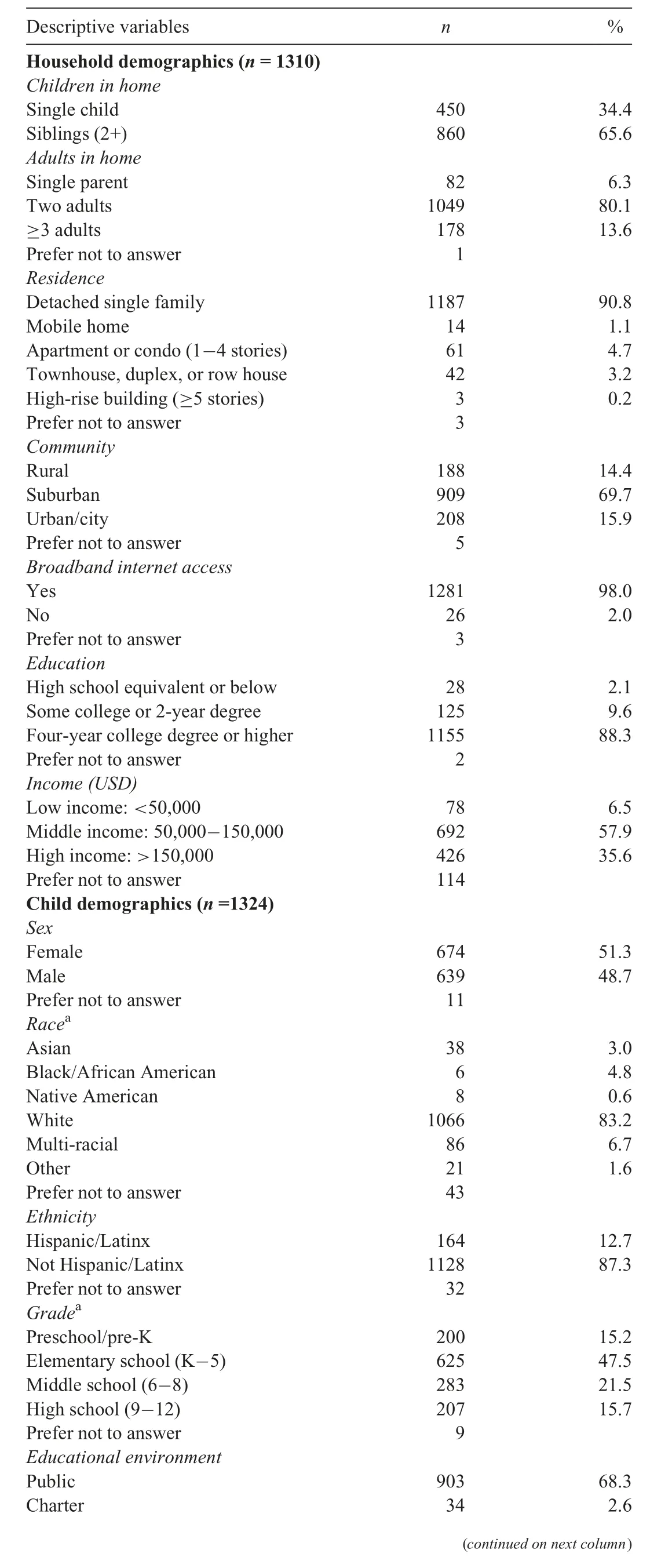
Table 1Household and child demographics based on a web-based,cross-sectional,parent report survey.
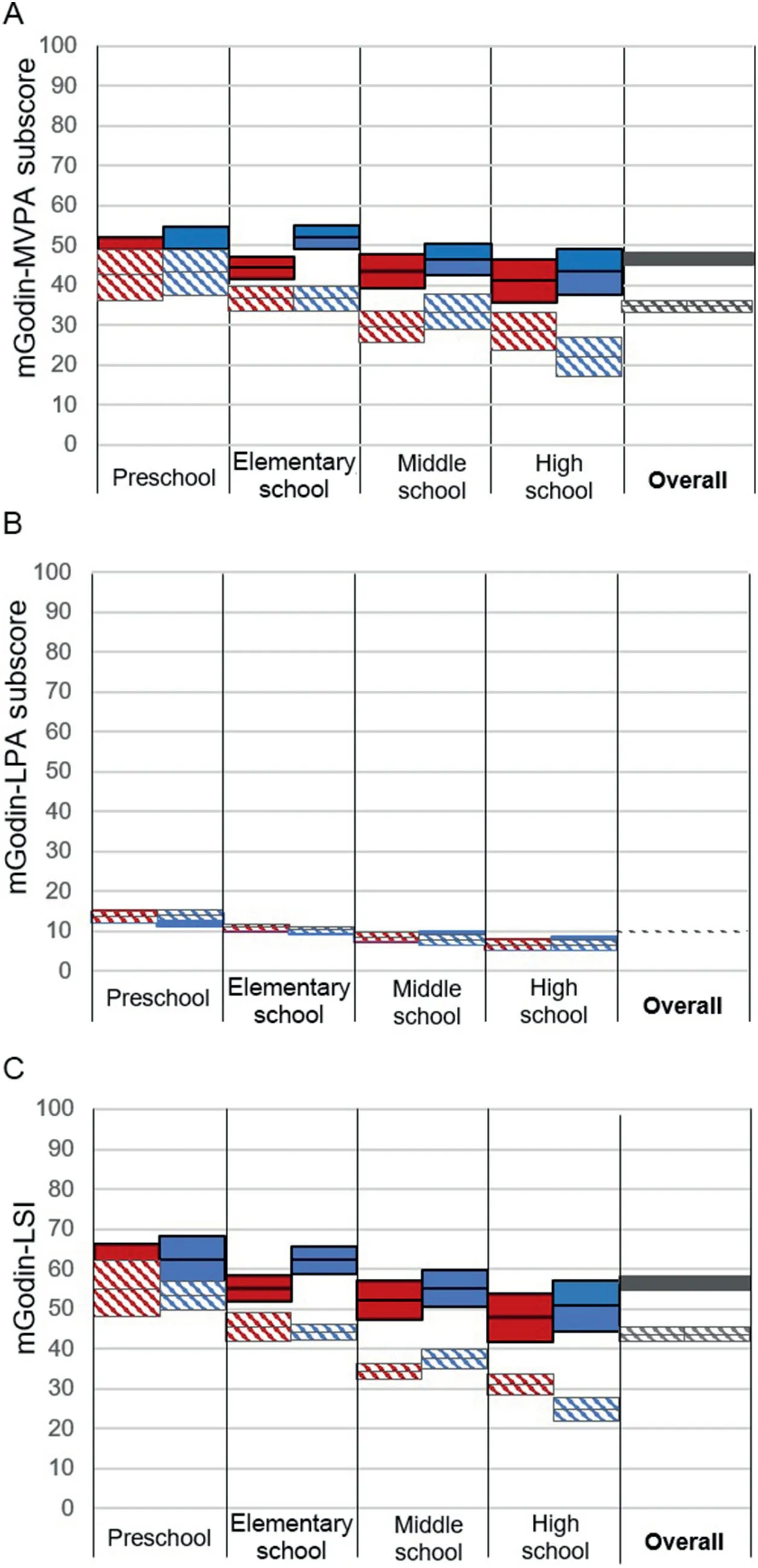
Fig.1.Child PA was assessed using a mGodin.For each child,(A)MVPA subscore and(B)LPA subscore were summed to calculate(C)the total LSI.Presented as mean±95%confidence interval.Solid denotes“pre-pandemic”;hashed denotes“during the coronavirus disease 2019(COVID-19)pandemic”;red denotes female;blue denotes male.LPA=light physical activity;LSI=Leisure-Time Score Index;mGodin=modified Godin Leisure-Time Exercise Questionnaire;MVPA=moderate-to-vigorous physical activity.
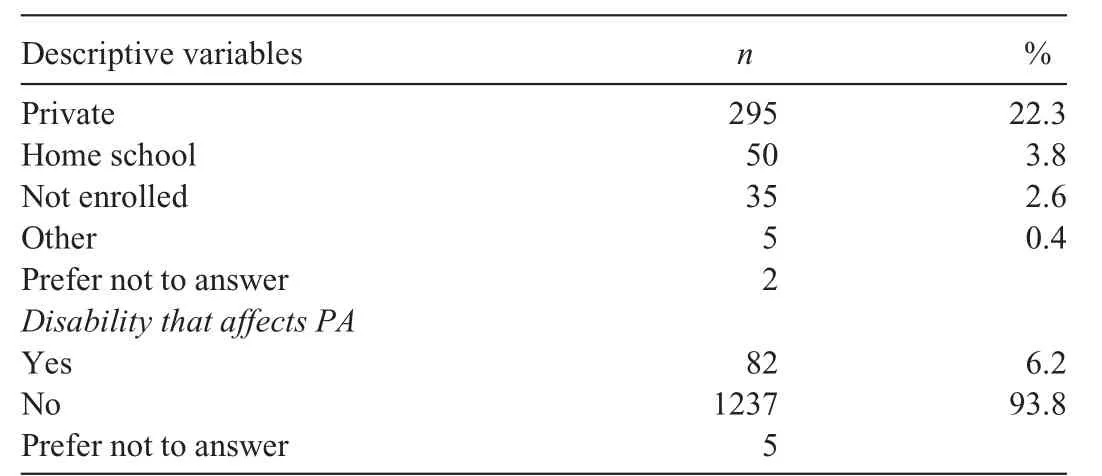
Table 1(Continued)
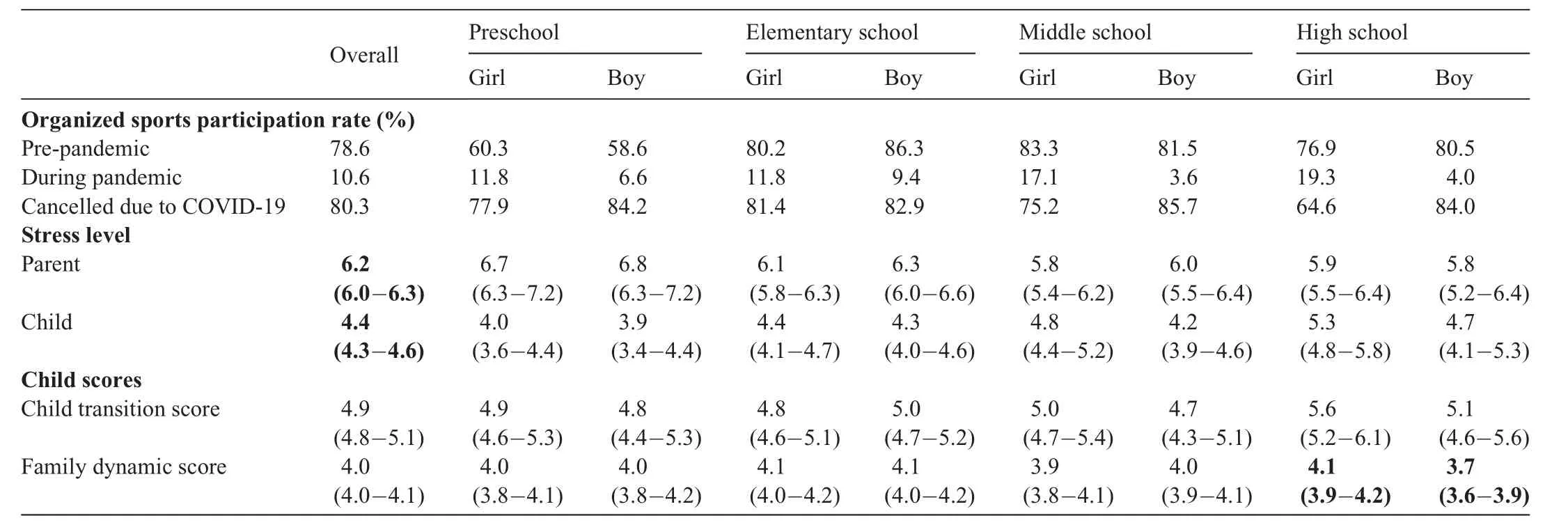
Table 2Organized sports and recreation participation rates(percent of valid responses)pre-and during the COVID-19 pandemic,parent and child(parent report)stress levels,and child transition and family dynamic scores(mean(95%CI)).
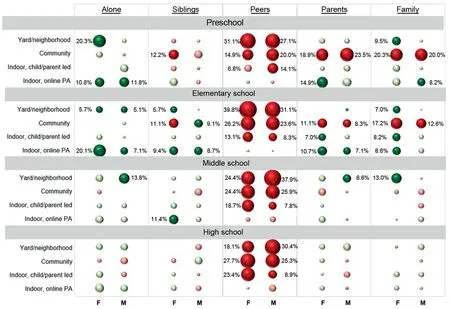
Fig.2.Change in participation rates(pre-vs.during-pandemic)across physical activity types varied by age and sex.Significant changes(p<0.05)are shown in darker colors with reported percent change;red denotes significant decrease in PA;green denotes significant increase in PA.F=female;M=male;PA=physical activity.
3.6.Changes in home-based educational activities
Based on parent report,82.6% of children participated in more electronic-based education during the pandemic,with only 38.5% and 31.7% reporting increased written and fine art activities,respectively.Child-led home EduA significantly decreased for elementary,middle,and high schoolers,while parent-led activities increased for young children(10.8%-16.5%,p<0.05)but not for older children.Online EduA increased significantly across all age groups(p<0.05)(Fig.3).
3.7.Impact on family dynamics and the child’s ability to transition
High school girls experienced greater change in their family dynamics compared to high school boys(4.1,95%CI:3.9-4.2vs.3.7,95%CI:3.6-3.9;p=0.003)per parent report.Parent self-stress was higher than their children’s stress(6.2,95%CI:6.0-6.3vs.4.4,95%CI:4.3-4.6;p<0.001).There were no differences in child stress level between boys and girls;however,stress level increased with age.There were no age-or sex-based differences apparent in a child’s ability to transition to the pandemic(Table 2).
4.Discussion
The aim of this study was to understand the impact that stay-at-home mandates had on PA in U.S.children during the COVID-19 pandemic and to provide evidence-based recommendations to parents/families,educators/school administrators,and policy makers to improve PA levels in children.Results showed that children had less MVPA,changed how and with whom they played,and that organized sports/recreational activities were cancelled.Pandemic-based changes in children’s PA varied significantly based on age,having less impact on preschool children.Middle and high school children had lower levels of PA than preschoolers pre-pandemic and exhibited greater reductions in PA during the pandemic,which is consistent with findings reported in Canadian children.19Preschool,elementary school,and middle school children significantly increased outdoor independent play;however,high school children did not.Adolescents,particularly boys,are less likely to participate in PA outside of team/peer settings.10-12,28-29The current study demonstrated that PA with friends decreased for outdoor activity,suggesting families were actively abiding by social distancing mandates and restricting peer interactions.
Based on the results of the current survey,several calls to action are recommended,aimed to improve PA in U.S.children if COVID-19 restrictions continue to limit access to PA opportunities(Table 3).While many federal,state,and local government agencies have publicly acknowledged social distancing and other health guidelines,there has been little if any focus on the important health benefits of maintaining a healthy,active lifestyle.A national public service announcement campaign aimed at encouraging children and their families to continue to strive to achieve the World Health Organization recommended 60 min of daily MVPA is highly encouraged.With colder weather expected in the winter,especially in northern U.S.states,it is important that local governments work within their jurisdictions to find safe,indoor spaces that allow for social distanced exercise classes or other PA opportunities such as indoor walking.School administrators and teachers have had to implement new safety protocols to ensure social distancing as in-person classes for many children across the country have resumed.Despite these necessary precautions,school districts should continue to assure children have adequate PA time through physical education classes and recess.While some may consider reducing recess time due to the difficulties of maintaining social distancing and cleaning playground equipment,the social and physical benefit of peer play in children is paramount.Lastly,families should be encouraged to engage in exercise together.Children with active role models tend to be more active themselves,therefore co-participation from family members can help to maintain or increase a child’s PA.Keep exercise equipment around the house,even small,inexpensive items such as balls that can be played with together on the sidewalk,in the yard,or at the park.Having a strategy to engage in healthy PA if COVID-19 pandemic spikes begin to reoccur in one’s local region may help families maintain their active lifestyles as the pandemic continues into 2021.
It should be noted that the time frame for“during-pandemic”questions ranged from April 4 to June 27,2020,and responses came from 48 states across the US.As such,the COVID-19 pandemic outbreak conditions may have been at different stages locally(test positivity rates,hospitalizations,and state/county/city restrictions),which may have impacted the parent-reported child PA at the time of individual survey responses.The time frame for all“during-pandemic”questions was“during the last 7 days”.However,all pre COVID-19 questions were phrased with a general time frame:“during a typical 7-day week pre-pandemic”.Given the almost 3-month time frame for the active survey link and the delayed start of the survey following the beginning of the pandemic(early-mid February to April 4 2020),the recall between“pre-pandemic”and survey completion may have been between 3 and 5 months(late January to either early April or late June 2020).This delay introduces a potential limitation in the reliability of pre-pandemic PA levels and survey responses.Furthermore,while the Godin Leisure Time Exercise Questionnaire has been previously validated in children,30,31a modified,unvalidated version of the survey was used for this study.Modifications to the PA questions included changing questions from open answer to Likert responses for the purpose of the online survey;however,it is unclear what impact this had on the validity of the survey questions.
The majority of households reported having pre-pandemic access to safe sidewalks and community resources such as parks and recreation centers.While many families reported increased use of community amenities,there was no change in median parental PA level during the pandemic.In contrast,the PA levels of children declined significantly,with similar reductions in outdoor play as Canadian children.19The current study found independent outdoor yard play increased in younger children,which helped minimize their decrease in overall PA;however,peer and community-based play decreased significantly.With public playgrounds and schools closed,peer-play opportunities for younger children were limited.Older children,who had lower levels of reported outdoor PA pre-pandemic,also showed larger decreases in overall PA during the pandemic.10-12,29,32Further analysis is needed to determine whether other factors such as location(rural/city)or type of dwelling(detached home/apartment)mediated or increased susceptibility of decreased PA in children during the pandemic.For example,children in single-family homes may have easier access to yards,32while those in apartments/townhomes may rely more heavily on neighborhood playground amenities,which were closed.
During the pandemic,some sport teams/organizations moved to online platforms with“virtual practices”.The current study reported a 10% increase in independent indoor PA during the pandemic.Increases in indoor PA were much lower than decreases in outdoor PA,supporting previous findings that indoor play does not adequately replace outdoor play.Children were therefore not able to maintain their pre-pandemic PA levels.19Multiple factors may lead to decreased online PA including space restrictions,depression/anxiety,and a lack of home exercise equipment and/or child-focused content.Most U.S.schools transitioned to virtual learning during the pandemic,increasing online EduA(15%-38%,current study),particularly for elementary and middle school students.When in-person peer activity was restricted,video/online chat became a common form of social communication between friends,increasing screen-time.19Parents must therefore balance their child’s screen-time between educational,social,and physical activities.
As was stated,the results of this study have indicated that changes in intensity and type of PA differed with the age of the child.The pandemic had less of an impact on preschoolers,who were more likely to“go outside and play”to maintain and/or increase their PA,while high schoolers reported greater decreases in MVPA and overall PA.These age-related findings suggest that pandemic-based restrictions may have a greater impact on PA in children already at a higher risk of obesity.The Centers for Disease Control and Prevention reports the prevalence of obesity in U.S.youth aged 2-19 years is 18.5%and increases with age from 13.9%(preschoolers)to 18.4%(elementary schoolers)to 20.6%(middle/high schoolers).5The current cohort was biased towards non-Hispanic white children from middle/upper class,2-parent households.The prevalence of obesity varies with race/ethnicity,with non-Hispanic black and Hispanic individuals having higher obesity rates than non-Hispanic white and Asian individuals.5,6Further analysis should assess the impact of the pandemic on PA in children with obesity risk factors.
It remains unclear whether children in households with physically-active parents/siblings experienced smaller declines in PA during the pandemic.Parental support and co-participation are important factors in children’s PA levels.5,33-35The current study found that children’s outdoor activity with a parent or as-a-family increased modestly during the pandemic,particularly in younger children.It is unknown whether children in single-parent or single-child households may be at greater risk of decreased PA.
Several studies have reported an increase in adverse mental health symptoms during the COVID-19 pandemic.36,37Moderate stress levels were reported in children(4.4/10.0),increasing with age.As adverse mental health symptoms increase with decreasing PA,7-9parents must actively engage with their children to ensure they have positive coping strategies,including PA,to mediate mental health challenges that may occur during the pandemic.
While this cross-sectional study cohort was biased towards middle-upper class,suburban,white households,the overarching reductions seen in PA levels are important to report.Children in families with different social,cultural,and/or economic situations may have varied access to neighborhood and community resources,which may greatly alter the influence of the pandemic on PA levels.Furthermore,the longitudinal impact of the COVID-19 pandemic on PA in children will depend on the duration of social distancing restrictions as well as changes in social and play interactions between peers during and outside of school.To that end,additional research,expanded to assess a more diverse sample,will be needed in the future.
The participant sample of the current study was socially and economically biased,most likely secondary to social media use as a main recruitment tool.While respondents were recruited nationally,the sample was not representative of U.S.diversity and cannot be generalized to all Americans or to other countries.Despite using a number of different social media distribution methods aimed to diversify the reach of recruitment,the study did heavily rely on a version of“snowball”sampling that allowed participants to share the survey link with others.This method of social network survey link distribution may have introduced an inherent homophily bias that contributed to the lack of social and economic diversity in our sample.This preliminary report did not include expansive associative statistical testing,examining factors only at the individual socioecological level(Supplementary Fig.1).Physical characteristics(height and weight)were not included in the survey,which limited interpretation of obesity as a covariate.While physical and educational participation were queried,leisure/social activities(game playing and reading)were not assessed.Future work should evaluate findings based on the full socioecological model,including the influence of natural,built,and social environments.Regional differences in COVID-19 outbreaks and subsequent responses,along with availability of neighborhood/community amenities,may have affected survey feedback.Limitations inherent with survey usage,including parent report of child activity/feelings and recall(pre-pandemic),may also influence findings.
5.Conclusion
This study reports empirical findings of decreased PA among U.S.children during the early stages of the COVID-19 pandemic,despite family reports of increased public greenspace use.Significant age-based changes were seen in the quantity,variety,and intensity of PA in children.Additional analysis is needed to identify predictors of which children are most vulnerable to PA changes during pandemic-related shutdowns.Recommendations for steps to improve PA in children as the COVID-19 pandemic continues,or in the case of future pandemics,are provided.This information will be significant if new COVID-19 cases continue and/or trend upwards in the coming months.
Acknowledgment
The authors wish to acknowledge Drs.John Birch and Anthony Herring for editorial review of the manuscript.
Authors’contributions
KTF conceptualized and designed the study,oversaw survey development and data collection,performed data analysis,drafted the initial manuscript,and reviewed and revised the manuscript;WS conceptualized and designed the study,assisted with data analysis,and reviewed and revised the manuscript;XG and TZ served as collaborating site principal investigations(PIs),conceptualized and designed the study,assisted with data analysis,and reviewed and revised the manuscript;HR and JK served as collaborating site PIs,conceptualized and designed the study,and reviewed and revised the manuscript;DD,JB,KJ,and JV conceptualized and designed the study and reviewed and revised the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
Supplementary materials
Supplementary material associated with this article can be found in the online version at doi:10.1016/j.jshs.2021.02.005.
杂志排行

Journal of Sport and Health Science的其它文章
- A critical review of national physical activity policies relating to children and young people in England
- The evidence for the impact of policy on physical activity outcomes within the school setting:A systematic review
- State laws governing school physical education in relation to attendance and physical activity among students in the USA:A systematic review and meta-analysis
- Handgrip strength and health outcomes:Umbrella review of systematic reviews with meta-analyses of observational studies
- Is device-measured vigorous physical activity associated with health-related outcomes in children and adolescents? A systematic review and meta-analysis
- Conceptual physical education:A course for the future Charles B.Corbin