Occult hepatitis C virus infection in the Middle East and Eastern Mediterranean countries: A systematic review and meta-analysis
2021-04-08MohammadRezaHedayatiMoghaddamHosseinSoltanianSanazAhmadiGhezeldasht
Mohammad Reza Hedayati-Moghaddam, Hossein Soltanian, Sanaz Ahmadi-Ghezeldasht
Mohammad Reza Hedayati-Moghaddam, Hossein Soltanian, Sanaz Ahmadi-Ghezeldasht, Blood Borne Infections Research Center, Academic Center for Education, Culture and Research (ACECR), Razavi Khorasan Branch, Mashhad 91779-49367, Iran
Abstract BACKGROUND The presence of hepatitis C virus (HCV) RNA in liver tissue or peripheral blood mononuclear cells with no identified virus genome in the serum has been reported worldwide among patients with either normal or elevated serum liver enzymes.The characterization of occult HCV infection (OCI) epidemiology in the Middle East and Eastern Mediterranean (M and E) countries, a region with the highest incidence and prevalence rates of HCV infection in the world, would be effective for more appropriate control of the infection.AIM To estimate the pooled prevalence of OCI in M and E countries using a systematic review and meta-analysis.METHODS A systematic literature search was performed using international, regional and local electronic databases.Some conference proceedings and references from bibliographies were also reviewed manually.The search was carried out during May and June 2020.Original observational surveys were considered if they assessed the prevalence of OCI among the population of M and E countries by examination of HCV nucleic acid in peripheral blood mononuclear cells in at least 30 cases selected by random or non-random sampling methods.The meta-analysis was performed using Comprehensive Meta-analysis software based on heterogeneity assessed by Cochran’s Q test and I-square statistics.Data were considered statistically significant at a P value < 0.05.RESULTS A total of 116 non-duplicated citations were found in electronic sources and grey literature.A total of 51 non-overlapping original surveys were appraised, of which 37 met the inclusion criteria and were included in the analysis.Data were available from 5 of 26 countries including Egypt, Iran, Pakistan, Saudi Arabia, and Turkey.The overall prevalence rate of OCI was estimated at 10.04% (95%CI: 7.66%-13.05%).The lowest OCI rate was observed among healthy subjects (4.79%, 95%CI: 2.86%-7.93%).The higher rates were estimated for patients suffering from chronic liver diseases (12.04%, 95%CI: 5.87%-23.10%), and multi-transfused patients (8.71%, 95%CI: 6.05%-12.39%).Subgroup analysis indicated that the OCI rates were probably not associated with the studied subpopulations, country, year of study, the detection method of HCV RNA, sample size, patients’ HCV serostatus, and sex (all P > 0.05).Meta-regression analyses showed no significant time trends in OCI rates among different groups.CONCLUSION This review estimated high rates of OCI prevalence in M and E countries, especially among multi-transfused patients as well as patients with chronic liver diseases.
Key Words: Occult hepatitis C; Prevalence; Review; Meta-analysis; Middle East; Eastern Mediterranean region
INTRODUCTION
The World Health Organization set the global health sector strategy on viral hepatitis in 2015 and established some service coverage targets, including the diagnosis of 90% of persons with chronic hepatitis C and treatment of 80% of the diagnosed cases to eliminate hepatitis C as a public health concern by 2030[1].Occult hepatitis C virus (HCV) infection (OCI) was introduced as a new and challenging form of this infection in 2004[2].OCI is characterized by the presence of HCV RNA in the liver samples of patients who were seronegative for the viral RNA[2].Although liver biopsy is the most accurate way to diagnose OCI cases[3], a reliable and non-invasive alternative method is the examination of the peripheral blood mononuclear cells (PBMCs) for the presence of HCV genome[4,5].
Occult hepatitis C has been proposed to occur in two different clinical conditions.The first category has been described in people reactive to HCV antibodies (anti-HCV) but with normal serum levels of liver enzymes.The majority of these patients are those with HCV infection treated with antiviral drugs or cleared spontaneously.In the second type of OCI, called serologically silent, cryptogenic, or secondary OCI, both anti-HCV and serum HCV-RNA are consistently negative but an increase in liver enzymes is observed[6].Cryptogenic OCI is found mostly in patients with cryptogenic liver disease; however, the incidence of this type of OCI was also reported among blood donors[7].
Occult hepatitis C might be a long-standing infection[8].OCI appears to be milder than classic chronic HCV infection; however, it is likely related to the development of liver cirrhosis or even hepatic cancer[3,9,10].Additionally, patients with OCI may benefit from antiviral therapies[11].OCI is a common condition worldwide and all HCV genotypes can be involved in this form of infection[11].This infection has been described in high-risk populations, such as patients with chronic liver disease, dialysis patients, those infected with HBV or HIV, the family members of patients with HCV infection, and even apparently healthy populations[3].
The Middle East and Eastern Mediterranean (M and E) region has been reported to have the highest rates of HCV infection in the world, with an incidence of 62.5 per 100000 person-years and prevalence of 2.3% among the general population (GP).In 2015, it was estimated that approximately one-fourth of 1.75 million newly HCVinfected persons and one-fifth of 71 million chronically infected individuals in the world resided in M and E countries[12].The median of the anti-HCV seropositivity rate in the GP of this region ranged broadly from 0.3% in Iran[13]to 13.0% in Egypt[10].In addition, the rate of HCV viremia among anti-HCV positive individuals in M and E countries varies widely from 9% to 100% with a median of 68.8%; the overall pooled rate was averagely estimated as 67.6% (95%CI: 64.9 ± 70.3%)[14].
The prevalence rate of OCI ranged from zero to 60% among the different studied populations in various M and E countries[15-17].To our knowledge, no review has yet been performed to provide a pooled estimate for the OCI prevalence rate in this region.In the current systematic review and meta-analysis, we aimed to determine OCI epidemiology among both healthy and risk populations in this region by (1) providing pooled mean estimates for the OCI rate through systematically reviewing and analyzing existing data in various subpopulations; (2) assessing the possible factors contributing to between-study heterogeneity; and (3) evaluating the change in OCI prevalence in different studied populations over time.The results of the present review would help professionals to make appropriate decisions for the detection and management of OCI, particularly in at-risk patients.
MATERIALS AND METHODS
Literature search
We performed this review and meta-analysis following the PRISMA 2009 statement[18].The main object was the presence of HCV RNA in PBMCs detected by a reverse transcription-PCR (RT-PCR) technique in the blood samples of healthy individuals or different patient categories from M and E countries.The search strategy included “Occult Hepatitis C” or “Occult HCV” along with “Middle East”, “Eastern Mediterranean”, or the names of M and E countries.In this study, the Middle East and Eastern Mediterranean region consisted of 26 countries: Afghanistan, Algeria, Bahrain, Cyprus, Djibouti, Egypt, Iran, Iraq, Israel, Jordan, Kuwait, Lebanon, Libya, Morocco, Oman, Pakistan, Palestine, Qatar, Saudi Arabia, Somalia, Sudan, Syria, Tunisia, Turkey, United Arab Emirates, and Yemen.The considered terms were searched in the title, abstract, and keywords using Web of Science and SCOPUS and in the text using PubMed, ScienceDirect, and ProQuest databases.Likewise, some regional and local databases were searched as “Occult Hepatitis C” or “Occult HCV” to find the articles published in the English language.These databases included the Index Medicus for the Eastern Mediterranean Region, Scientific Information Database, Iranian Database of publication (Magiran), and Iranian Databank of Medical Literature.In addition, some appropriate available abstract booklets and conference proceedings were manually reviewed.The search was performed from 21 May to 08 June 2020 and then expanded by manual cross-checking all references found from bibliographies of retrieved citations.
Study selection and data extraction
The two authors screened the titles and abstracts of the documents identified in the electronic and grey literature.Duplicate and overlapping surveys (the same studied population, methods, and findings) were excluded.Regarding articles, which reported the OCI prevalence in the region, various methodological aspects of the studies were assessed using a 10-items checklist, specifically developed to evaluate both internal and external validity of the prevalence studies[19].These aspects encompassed the representativeness of the target population, sampling methods, sample size, data collection methods and instruments, response rate, and statistical analysis.The main inclusion criteria were detection of the HCV genome in PBMCs of at least 30 healthy or high-risk subjects selected by probable or non-probable sampling methods in an original observational survey.Review articles, case reports, editorials, or letters were removed.Surveys that evaluated OCI in hepatocytes or other samples except PBMCs were not included.In addition, studies were not entered into the meta-analysis if they did not use an acceptable case definition and/or not apply an appropriate numerator and denominator for calculating the event rates.
The full texts, tables, and figures of all relevant articles were reviewed for data extraction by the two authors.The following variables were listed for each study: First author, year of publication, years of data collection, study type, study location, studied population, sampling method, the number of cases with anti-HCV and HCV RNA seropositivity, methods used to assess HCV genome, and the number and demographic features of cases with detectable HCV RNA in their PBMCs samples.Since the surveys in this field were restricted, no specific exclusion criteria were set for the studied population, year of data collection, and patients’ age and sex.
Statistical analysis
The meta-analysis was performed using Comprehensive Meta-analysis software 2.2.064 (Biostat, Englewood, NJ, United States).With inverse variance weighting, a random-effect model was applied using the DerSimonian and Laird method if heterogeneity between studies was observed based on Cochran’sQtest (P< 0.05) andI-square statistics (I2, values of > 50%).Forest plots were applied to demonstrate the point prevalence rates and the 95% confidence intervals (CIs).Subgroup and metaregression analyses were implemented to identify the possible factors related to heterogeneity between surveys.HCV serostatus was classified as seronegative (negative results for both anti-HCV and serum HCV RNA) and seropositive (tested positive for anti-HCV but negative for serum HCV genome).All statistical data were considered significant at aPvalue < 0.05.
RESULTS
Study selection
Among 151 citations retrieved from electronic sources, 107 non-duplicated items were selected to review the titles and abstracts (Figure 1).Fifty-two surveys discussed the prevalence of OCI in M and E countries[15-17,20-68], of which 5 review articles and 2 letters were excluded[62-68].In addition, 4 pertinent documents were identified following a review of abstracts[69-72], and 5 documents were found by a manual screening of bibliographies[73-77].After removing 3 overlapping surveys[71,72,75], 51 original articles were chosen for a thorough review of the full-text[15-17,20-61,69,70,73,74,76,77].Most of the surveys had used a non-probable method to select studied samples and none of them had discussed non-response bias.Fourteen articles were not included owing to methodological difficulties, small sample size, and/or analysis of liver tissue or centrifuged serum[20,24,28,30,32,34,37,40,52,56,61,70,73,77].
Finally, 37 non-duplicate and non-overlapping articles met the inclusion criteria and were included in the analysis[15-17,21-23,25-27,29,31,33,35,36,38,39,41-51,53-55,57,58,59,60,69,74,76].All studies were cross-sectional investigations and almost all of them were based on consecutive samples selected by a non-random convenience sampling method.The mean sample size was 141 (range: 30-1280); less than 100 cases in 23 studies, 100-200 cases in 11 surveys, and more than 200 cases in three studies.
The overall prevalence of occult hepatitis C in M and E countries
Of the 26 included countries, data were available only from five countries.Egypt (n= 17) and Iran (n= 17) were the countries with the largest number of studies reporting OCI prevalence but Pakistan, Saudi Arabia, and Turkey contributed to only one data point.These five countries had surveyed OCI prevalence among a total of 5200 individuals between 2009 and 2019 (Table 1).The studied population included blood donors, patients for whom HCV infection was resolved following antiviral treatment or spontaneously, patients with cryptogenic chronic liver diseases (LDs), autoimmune hepatitis, thalassemia, hemophilia, lymphoproliferative disorders, or anemia, patients undergoing hemodialysis (HD), HIV positive individuals, and injecting drug users (IDUs).Five surveys had collected data from mixed populations, mainly healthy volunteers as well as those suffering from chronic diseases.
The studied subjects were aged 4 to 89 years and their mean age was between 26 ± 9.31 and 58.9 ± 14.7 years.In 23 studies, 53.2%-98.4% of the participants were males, in 10 surveys, 50.0%-58.1% of them were females, and sex distribution of the samples was not stated in four documents.
As shown in Table 2, the rate of OCI prevalence in this region ranged widely from 0.0% to 44.44%, with a median of 10.14%.The overall mean prevalence was estimated to be 10.04% (95%CI: 7.66%-13.05%).Across subpopulations, the pooled average OCI rate was highest at 21.70% (95%CI: 11.26%-37.72%) among patients with cryptogenic liver disease, followed closely by 18.18% (95%CI: 11.07%-28.39%) among HIV positive IDUs and 18.15% (95%CI: 10.20-30.20%) in the mixed population.The rate of OCI in Egypt (12.34%; 95%CI: 8.32-17.92%) was higher than in Iran (8.48%; 95%CI: 5.51%-12.84%); however, the difference was not statistically significant (P= 0.157).Subgroup analysis showed that the rate of OCI was probably not related to the disease subpopulations (P= 0.066), year of data collection (P= 0.786), the detection method of HCV RNA (P= 0.507), sample size (P= 0.057), patients’ HCV serostatus (P= 0.178) and sex (P= 0.953).Furthermore, meta-regression analysis showed no significant (P= 0.580) time trend in the OCI rate among the total population of this region.

Table 1 Selected studies for systematic review and meta-analysis of occult hepatitis C virus infection prevalence in the Middle Eastern countries and Eastern Mediterranean Region

ALT: Alanine transaminase; AST: Aspartate aminotransferase; HBV: Hepatitis B virus; HCV: Hepatitis C virus; HIV: Human immunodeficiency virus; Is-PCR: In situ-PCR; PCR: Polymerase chain reaction; RT-PCR: Reverse transcription PCR; rRT-PCR: Real time RT-PCR; SVR: Sustained virologic response.
Occult hepatitis C prevalence among healthy populations
Four studies conducted in the M and E area reported OCI prevalence among 300 apparently healthy subjects, such as healthy volunteers, blood donors, and healthy sexual partners of patients with chronic HCV infection.All four studies had been performed among Egyptian HCV-seronegative cases, of which three had studied less than 100 cases, and three had been conducted after 2014.Assessment of HCV RNA in PBMCs had been carried out using RT-nested PCR in three surveys and real-time RTPCR in another research.Based on the fixed-effect model (Q= 0.77,P= 0.857,I2= Zero), the pooled estimation of OCI prevalence among healthy populations was 4.79% (95%CI: 2.86%-7.93%, Figure 2).No evidence was found for a significant trend in the OCI rate in this population over time (P= 0.802).
Occult hepatitis C prevalence among multi-transfused patients
Seventeen studies reported the OCI rate among 2217 multi-transfused patients (MTPs), including 1480 HD patients, 450 hemophilia patients, and 287 thalassemia patients in the region.Fifteen surveys evaluated the presence of viral genome among HCV seronegative samples.As shown in Table 3, the prevalence rate was estimated to be 8.71% (95%CI: 6.05%-12.39%) among this population (Figure 3).Based on 14 surveys, the estimated OCI rate among HD patients was 9.52% (95%CI: 6.30%-14.12%).

aP < 0.001.bP < 0.01.1Four studies investigated occult hepatitis C virus infection among healthy volunteers along with hemodialysis patients, patients with chronic hepatitis C, or patients with hematologic and lymphoproliferative disorders.Also one study investigated both the patients with chronic hepatitis C and patients with cryptogenic liver disease.2Based on the last year reported for the data collection.If the collection date was not clear, publication year was considered instead.CI: Confidence interval; Min: Minimum; Max: Maximum; PCR: Polymerase chain reaction; RT-PCR: Reverse transcription polymerase chain reaction; OCI: Occult hepatitis C virus infection.
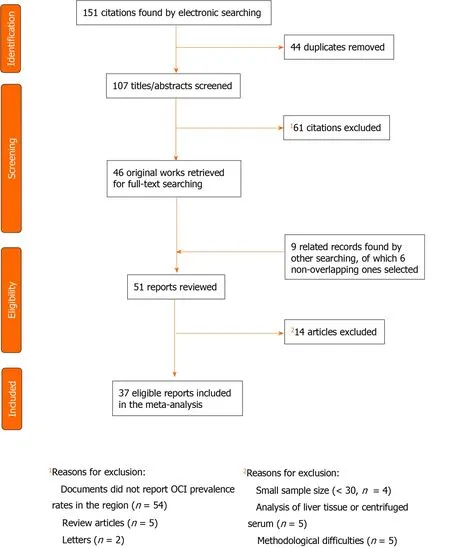
Figure 1 Study selection for the systematic review and meta-analysis of occult hepatitis C prevalence across the Middle East and Eastern Mediterranean countries.
Subgroup analysis revealed that the rate of OCI in Egypt (11.43%; 95%CI: 6.55%-19.17%) was higher than in Iran (5.93%; 95%CI: 3.09%-11.09%), but the difference was not statistically significant (P= 0.125).The rate of OCI frequency was not associated with year of study (P= 0.732), the detection technique of HCV RNA (P= 0.618), sample size (P= 0.470), and patients’ sex (P= 0.859).Moreover, meta-regression analysis showed no significant (P= 0.520) changes in the OCI rate among MTPs patients over years.

Table 3 Subgroup-specific pooled estimates of occult hepatitis C virus infection prevalence among multi-transfused patients across the Middle Eastern and Eastern Mediterranean countries
Occult hepatitis C prevalence among patients with chronic liver diseases
In total, 11 surveys reported the OCI prevalence among 2065 patients with chronic LDs in M and E countries.These patients included 1778 with chronic hepatitis C, including those who achieved sustained virologic response after treatment with antiviral drugs, 252 patients with cryptogenic LDs (persistently abnormal liver tests and/or liver cirrhosis with unknown etiology), as well as 35 patients with autoimmune hepatitis.The rate of OCI prevalence among these patients was estimated to be 12.04% (95%CI: 5.87%-23.10%, Table 4).The rate in the subgroup of cryptogenic patients (20.81%; 95%CI: 6.87%-48.35%) was double the value calculated for post-HCV non-viremic cases (9.14%; 95%CI: 3.02%-24.53%,P= 0.276).Figure 4 displays the forest plot of OCI among patients with chronic LDs based on the type of the disease.In addition, the rate of OCI among cases detected by RT-nested PCR (21.38%; 95%CI: 11.73%-35.75%) was considerably higher than cases identified using real-time RT-PCR (6.29%; 95%CI: 2.73%-13.84%,P= 0.052).Furthermore, there was no difference in the OCI frequency based on the year of data collection (P= 0.962), study location (P= 0.178), sample size (P= 0.416), patients’ HCV serostatus (P= 0.750) and sex (P= 0.749).According to metaregression analysis, no significant (P= 0.943) link was detected between the OCI rate among this population and data collection time.Figure 4 displays the forest plot of OCI among patients with chronic LDs based on type of the disease.

Figure 2 Meta-analysis forest plot of occult hepatitis C among healthy populations across the Middle East and Eastern Mediterranean countries.

Figure 3 Meta-analysis forest plot of occult hepatitis C among multi-transfused patients across the Middle East and Eastern Mediterranean countries.

Table 4 Subgroup-specific pooled estimates of occult hepatitis C virus infection prevalence among patients with chronic liver diseases across the Middle Eastern and Eastern Mediterranean countries
Occult hepatitis C prevalence among other high-risk categories
Regarding OCI prevalence among HIV-positive subjects in the M and E region, three surveys reported the rate among 417 HCV-seronegative and seropositive samples.All studies had been conducted in Iran after 2014 and evaluated HCV RNA in PBMCs using the RT-nested PCR method.Using the fixed-effect model (Q= 3.1,P= 0.208,I2= 36.3%), the pooled mean prevalence of OCI was estimated at 12.95% (95%CI: 9.56%-17.32%) among this population.
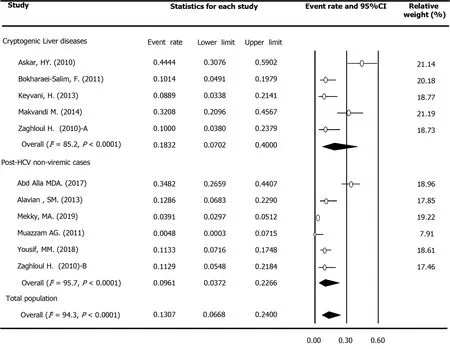
Figure 4 Meta-analysis forest plot of occult hepatitis C among patients with chronic liver diseases across the Middle East and Eastern Mediterranean countries based on type of disease.
Concerning occult hepatitis C among IDUs, one study recently identified HCV RNA in PBMCs in 18.18% of 77 Iranian HIV-positive IDUs.Moreover, another study from Iran reported an OCI rate of 9.57% among 115 HBV- and HIV-negative IDUs.Both surveys detected HCV genome among both HCV seronegative and seropositive samples by the RT-nested PCR method.
A total of three surveys, including two studies from Egypt and one survey from Iran, focused on OCI among patients with hematologic disorders, such as lymphoma, leukemia, and anemia.All OCI cases were detected by the RT-nested PCR technique among 171 HCV seronegative samples.Using the random-effect model (Q= 29.9,P< 0.001,I2= 93.3%), the pooled estimate of OCI among this population was estimated at 19.57% (95%CI: 3.22%-63.99%).
DISCUSSION
Through a comprehensive description and detailed analysis of occult hepatitis C epidemiology among the various populations in M and E countries, we found a considerably high rate of overall OCI prevalence across the region (10.04%; 95%CI: 7.66%-13.05%).The lowest rate (4.79%) was estimated among apparently healthy volunteers and blood donors.On the other hand, the higher rates were estimated for MTPs (8.71%), patients with chronic LDs (12.04%), HIV-positive subjects (12.95%), and those with lymphoproliferative and hematologic disorders (19.57%).Although the rate varied significantly across the studies, the pooled mean rate of OCI was not dissimilar regardless of subpopulation, location and year of study, the detection method of HCV RNA, patients’ HCV serostatus or sex.Lastly, meta-regression analysis could not ascertain a declining or rising trend for OCI prevalence as a whole or among the different subpopulations of the region.
The incidence of OCI in each area is affected by various factors, mainly the prevalence and risk factors of HCV infection in the community as well as in the studied population.Some investigators believed that there is a geographical pattern for OCI that is probably related to HCV endemicity distribution[3].The majority of all chronically HCV infected people in the M and E region reside in the two countries most affected by the infection,i.e.Egypt and Pakistan[78].In the current review, we noted that the Egyptian population had the highest rates (12.34%; 95%CI: 8.32%-17.92%) of OCI in this region.Likewise, based on four studies from Egypt, we calculated the pooled OCI rate among healthy populations to be 4.79 (95%CI: 2.86%-7.93%).Egypt is one of the countries highly affected by HCV and with high anti-HCV prevalence in almost all population groups[10].Based on the Egypt Demographic and Health Surveys, anti-HCV prevalence among the adult Egyptian population was 10.0% in 2015[10].Similarly, a recent systematic review estimated a pooled mean rate of 11.9% (95%CI: 11.1%-12.6%) for anti-HCV prevalence among the general Egyptian population[10].Another systematic review estimated an average pooled HCV viremic rate of 67.0% (95%CI: 63.1%-70.8%) among anti-HCV positive individuals in this country[14].In other words, the prevalence of chronic hepatitis C in Egypt is around 8%, which is close to the rate (6.3%) reported previously in 2015[79].Moreover, four-fifths of hepatocellular carcinoma (HCC) patients in this country are infected with HCV— which ranks first in the world[80].On the other hand, Iran has one of the lowest rates of HCV infection worldwide, particularly in the M and E region[81].In this country, where HCV spread is dominated by transmission through injecting drug use[81], the pooled rates of anti-HCV positivity and viremic HCV among the GP have been estimated as low as 0.2%-0.3% and 0.4%-0.6%, respectively[13,79,81,82].Correspondingly, we identified a lower overall rate of OCI among the Iranian population (8.48%) in comparison with the Egyptian population (12.34%).
Occult hepatitis C is primarily identified among populations at higher risk of health-care-related exposure, such as people who received repetitive transfusions particularly HD patients[66].Our analysis estimated an average pooled OCI rate among MTPs of 8.7% (95%CI: 6.0%-12.4%); a higher level was calculated for HD patients (9.5%, 95%CI: 6.3%-14.1%) than for thalassemia patients (4.3%, 95%CI: 2.5%-7.5%).The rates of OCI prevalence among HD patients ranged from zero to 45% in different studies across the world[66].In a survey by Barrilet al[83], 45% of 109 Spanish HD patients with abnormal serum levels of liver enzymes had detectable HCV-RNA in their PBMCs.The patients with OCI had significantly higher mean levels of serum alanine aminotransferase.In addition, a significantly higher percentage of OCI patients died during the follow-up period compared with patients without OCI (39%vs20%;P= 0.031).It is expected that HD patients are at higher risk of HCV infection owing to shared dialysis machines[84].Some researchers suggested that the duration of dialysis is associated with the increased probability of HCV infection among HD patients[83,85].In the M and E region, Harfoucheet al[86]showed that about one-fifth of HD patients are chronic HCV carriers and can potentially spread the infection through the dialysis machine.They suggested that their findings may reflect the higher HCV incidence in the communities along with poor standards of dialysis in this area.Despite the decrease in the prevalence of HCV infection in HD patients, OCI could be the culprit for the constant distribution of HCV among this population[3].
Furthermore, our review estimated a two-fold higher rate of OCI among Egyptian MTPs patients (11.4%, 95%CI: 6.5%-19.2%) than Iranian patients (5.9%, 95%CI: 3.1%-11.1%).These findings were consistent with the reported rates for anti-HCV prevalence among this population in both countries.In a systematic review and metaanalysis of data from 10 countries in the Middle East, the pooled HCV prevalence among HD patients was estimated to be 25.3% (95%CI: 20.2%-30.5%); a much higher rate was reported from Egypt (50%, 95%CI: 46%-55%) in comparison with Iran (12%, 95%CI: 10%-15%)[87].Indeed, medical care appears to be the main route of both past and new HCV transmission in Egypt[10].On the other hand, in another recent review, the overall anti-HCV prevalence was estimated at a considerably lower rate (20.0%, 95%CI: 16.4%-23.9%) across Iranian populations at high risk of healthcare-related exposures, such as HD, hemophilia, and thalassemia patients[13].
The rate of occult hepatitis C is considerably higher among populations with liver involvement who were seronegative for HCV RNA[2,61,64].In a recent survey in Egypt, the rate of OCI among 112 post-HCV non-viremic cases, including 55 non-cirrhotic and 57 cirrhotic patients (34.8%) was significantly higher than 62 healthy control individuals (3.23%)[35].Likewise, our review indicated a high frequency of OCI among patients with LDs, including individuals with unexplained elevated liver enzymes and cryptogenic hepatitis as well as those with a history of exposure to HCV in the past (12.04%, 95%CI: 5.87%-23.10%); the highest rate was observed in patients with cryptogenic LDs (20.81%; 95%CI: 6.87%-48.35%).High rates of OCI among LD patients have been reported from countries with both low and high HCV endemicity in the community[21,22,41,48].Consistently, our analysis revealed that the rate of OCI among LD patients in Egypt (16.08%; 95%CI: 5.81%-37.35%) did not significantly (P= 0.178) differ from Iranian patients (11.46%; 95%CI: 3.64%-30.73%).Regarding active HCV infection among populations with LDs, high rates have also been reported from both countries.A detailed analysis of HCV epidemiology in the Middle East found a pooled mean prevalence of 35.5% (95%CI: 31.7%-39.5%) in all patients with LDs; the highest rates were estimated for HCC (56.9%; 95%CI: 50.2%-63.5%) and hepatic cirrhosis (50.4%; 95%CI: 40.8%-60.0%).The pooled rate was 58.8% (95%CI: 51.5%-66.0%) in Egypt, 55.8% (95%CI: 49.1%-62.4%) in Pakistan, and 15.6% (95%CI: 12.4%-19.0%) in other countries[88].The rate of HCV infection in each LD population of each country was strongly correlated with HCV prevalence among their GP.The authors concluded that their findings highlight how the role of this infection in liver diseases is a reflection of its background level in the GP[88].Moreover, in countries like Egypt and Pakistan, high rates of infections among various populations with LDs may support the contribution of HCV to the occurrence of liver disease[9,10].On the other hand, a significantly lower HCV rate has been reported for Iranian patients with liver-related conditions (7.5%, 95%CI: 4.3%-11.4%)[13].Another systematic review underlined the different etiology of HCC in countries of the Eastern Mediterranean region; Four-fifths of HCC patients in Egypt and half of the patients in Pakistan were infected with HCV; however, this value was as low as 8.5% for Iranian patients[80].
Our study had several limitations.Almost all of OCI reports (34 of 37) were from Iran and Egypt, and we did not find any data from 21 countries in the M and E region.Our study is also limited by the number of available documents for both healthy subjects and specific at-risk populations, such as IDUs, HIV-positive persons, and thalassemia or hemophilia patients.Other limitations of our review were the quality of retrieved evidence as well as the representativeness of the target populations.The findings of the majority of studies were based on examination of less than 100 consecutive samples selected by a non-random convenience sampling method.There was a wide heterogeneity in OCI rates even within specific subpopulations; nonetheless, there was no evidence that study location, data collection date, the detection technique of HCV RNA, patients’ HCV serostatus, and sex-group representation in the sample affected the prevalence rates.Despite these shortcomings, we found a large amount of data in two countries, which contributed to the lowest and highest rate of chronic HCV infections in the region (namely, Iran and Egypt, respectively) that allowed us to conduct an analysis among different population categories and settings.
CONCLUSION
Our systematic review and meta-analysis quantified high levels of OCI prevalence, especially across risk populations in M and E countries.Recommendations include more appropriate OCI screening programs to target individuals who are at high risk for HCV infection, especially the patients undergoing dialysis and those with cryptogenic liver diseases.Besides, further investigations are needed regarding OCI among other risk populations, such as HIV- and HBV-infected subjects, IDUs, and thalassemia and hemophilia patients.
ARTICLE HIGHLIGHTS
Research background
Occult hepatitis C virus (HCV) infection (OCI) is defined as the presence of HCV genome in the liver samples or peripheral blood mononuclear cells despite a negative test for serum viral RNA.OCI, a common condition worldwide, might be associated with significant morbidities such as liver cirrhosis or hepatocellular carcinoma.No review has yet been performed to provide a pooled estimate for the OCI prevalence rate in the Middle East and Eastern Mediterranean (M and E) countries, a region with the highest rates of HCV infection in the world.
Research motivation
In this systematic review and meta-analysis, we tried to characterize a clear feature of OCI epidemiology in 26 countries of the M and E region based on documents found by searching international and regional electronic sources as well as some local grey literature.We hope our findings help researchers to perform more investigations on diagnosis, management, and control of OCI, particularly in high-risk populations such as patients with chronic liver disease, multi-transfused patients, those infected with HIV, injecting drug users,etc.
Research objectives
The main objective of this review is to provide pooled mean estimates of the OCI rate and assess the contribution of potential variables on the between-study heterogeneity in the M and E region.The results would help professionals, investigators and policy makers to organize suitable activities regarding OCI, particularly in high-risk patients.
Research methods
A systematic review and meta-analysis was performed following PRISMA guidelines.A comprehensive search of electronic databases was conducted up to June 2020 in the Web of Science, PubMed, SCOPUS, ScienceDirect, ProQuest, the Index Medicus for the Eastern Mediterranean Region, Scientific Information Database, Iranian Database of publication (Magiran), and Iranian Databank of Medical Literature.Also some conference abstracts and all references from bibliographies of retrieved articles were manually reviewed.Forest plots were applied to demonstrate the point prevalence rates and the 95% confidence intervals, and subgroup and meta-regression analyses were applied to identify the factors contributing to heterogeneity between surveys.
Research results
Thirty-seven studies involving 5200 participants from Egypt, Iran, Pakistan, Saudi Arabia, and Turkey were analyzed.The overall pooled prevalence rate of OCI was 10.04%.The pooled rate among healthy populations was 4.79%, but the rate was much higher among patients with hematologic disorders (19.57%), HIV-positive subjects (12.95%), patients with chronic liver diseases (12.04%), and multi-transfused patients (8.71%).The rate of OCI was not significantly related to the country, disease subpopulations, year of study, the method of HCV RNA detection, sample size, patients’ HCV serostatus and sex, and no significant change was detected in the OCI rate over time (P> 0.05).
Research conclusions
This review and meta-analysis demonstrates high rates of OCI prevalence, especially across risk populations in the M and E region.Some appropriate OCI screening programs are recommended to target individuals who are at risk of HCV infection.
Research perspectives
According to this systematic review and meta-analysis, further investigations are required in order to collect more data on the OCI frequency in M and E countries other than Egypt and Iran, two nations with the highest and lowest rates of chronic HCV infection in the region, respectively.Moreover, large scale studies are needed to evaluate OCI prevalence among less studied populations such as injecting drug users, HBV-infected patients, and thalassemia and hemophilia patients.
杂志排行

World Journal of Hepatology的其它文章
- Meeting report of the editorial board meeting for World Journal of Hepatology 2021
- Extrahepatic cholangiocarcinoma: Current status of endoscopic approach and additional therapies
- Adult human liver slice cultures: Modelling of liver fibrosis and evaluation of new anti-fibrotic drugs
- Production and activity of matrix metalloproteinases during liver fibrosis progression of chronic hepatitis C patients
- Awareness of non-alcoholic steatohepatitis and treatment guidelines: What are physicians telling us?
- Two-stage hepatectomy with radioembolization for bilateral colorectal liver metastases: A case report