Contained local compression on peri-ascending aortic area for postoperative bleeding control: a case report
2021-03-13SuYoungYoonSiWookKimDohunKimJongMyeonHong
Su Young Yoon, Si-Wook Kim, Dohun Kim, Jong-Myeon Hong,✉
1Department of Thoracic and Cardiovascular Surgery, 2Trauma Center, Chungbuk National University Hospital,College of Medicine, Chungbuk National University, Seowon-Gu, Cheongju 28644, Republic of Korea.
Abstract
Keywords: uncontrollable bleeding, contained local compression, aortic dissection, aortic root repair
Introduction
Intractable bleeding from the anastomotic sites of the fragile dissected tissues or aortic root area could be a catastrophic result of type A acute aortic dissection (AAD) repair or modified Bentall procedure. Large amount of transfusion with coagulation factors and reoperation for the bleeding control is mostly needed.
This procedure was reviewed and approved by the Institutional Review Board of Chungbuk National University Hospital, and the ethical standards of the responsible institutional committee on human experimentation and the Helsinki Declaration were followed.
Case reports
Case 1
A 53-year-old man diagnosed with annuloaortic ectasia (66 mm in root diameter) and severe aortic regurgitation with Marfan syndrome (Fig. 1)underwent modified Bentall procedure using valved graft (29 mm Valsalva valved graft, 29 VAVGI-515,St. Jude Medical, USA). The operation proceeded smoothly until cardiopulmonary bypass (CPB)weaning, when a significant bleeding from the sawing ring site could not be controlled by reinforced suturing and BioGlue (CryoLife, USA). Gauze packing was done at the bleeding points and the patient was moved to intensive care unit (ICU). Despite lots of coagulation factor transfusion, significant chest tube bleedings occurred the following day and the patient had to receive the second operation for bleeding control. During the operation, CPB was restarted because of the overall oozing from the whole valve sawing ring and the exact bleeding points couldn't be clarified. Reinforcement suturing over the whole sawing ring with pericardial band was done under the cardiac arrest with the infusion of cardioplegic solution, and the second operation ended with smooth pump weaning. But after cardiac beating restored and arterial pressure up, quite a lot of oozing of blood from the sawing ring still continued. Another gauze packing was done and the patient was sent back to ICU. The next day the third operation was planned due to excessive tube drainage, and the operative findings were very similar to previous ones in that there was still significant oozing from the sawing ring.At this time, bovine pericardial patch (BP0209 Periborn Bovine Pericardium, Taewoong, Republic of Korea) was attached to the upper half of the heart to induce contained local compression, using 5-0 Prolene continuous suturing from upper part of the right ventricle at lower margin excluding right coronary artery to just above the innominate vein for the upper,and from right border of superior vena cava (SVC) to left border of main pulmonary artery (MPA) with closing both ends of transverse sinus by gauze packings (Fig. 2). Without any further trial of the sawing ring area the patient came back to ICU. The condition of the patient was stable with little need for postoperative transfusion, and wound closure was done 2 days later. The patient recovered well and has been followed up at out-patient clinic with a good condition for 19 months after discharge.

Fig. 1 Preoperative chest computed tomography (CT). This CT finding showed dilated aortic root (66 mm in maximum diameter) and ascending aorta with effacement of the sinotubular junction.
Case 2
An 82-year-old woman received an emergent operation due to type A AAD with impending tamponade (Fig. 3)at night. Hemiarch graft replacement of the ascending aorta (using 30 mm branched Hemashield graft, Hemashield Platinum,Intervascular SAS, France) was done under short period of circulatory arrest, and pump was smoothly weaned with a good cardiac function except uncontrolled bleeding from the distal anastomotic site of fragile native dissected aortic area. Several reinforcement sutures with pericardial pledgets were used to stop bleeding, but failed. At this case, bovine pericardial patch was applied over the upper part of aortic area for contained local compression, in a very similar fashion of the first case without any hesitation(Fig. 2). The patient moved to ICU with sternal &simple skin closure with chest tubes and the bleeding came to be stopped overnight, and final wound closure was done two days later.
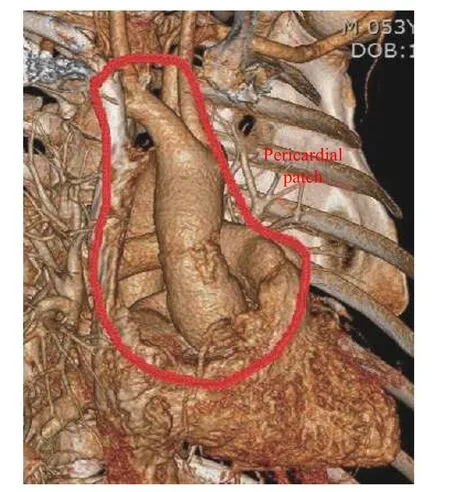
Fig. 2 Pericardial patch for induced-tamponade. Pericardial patch was covered to make contained local compression of upper half of the heart from upper part of the right ventricle at lower border to just above the innominate vein for the upper, and from right border of superior vena cava to left border of main pulmonary artery using bovine pericardium with closing both sides of transverse sinus.
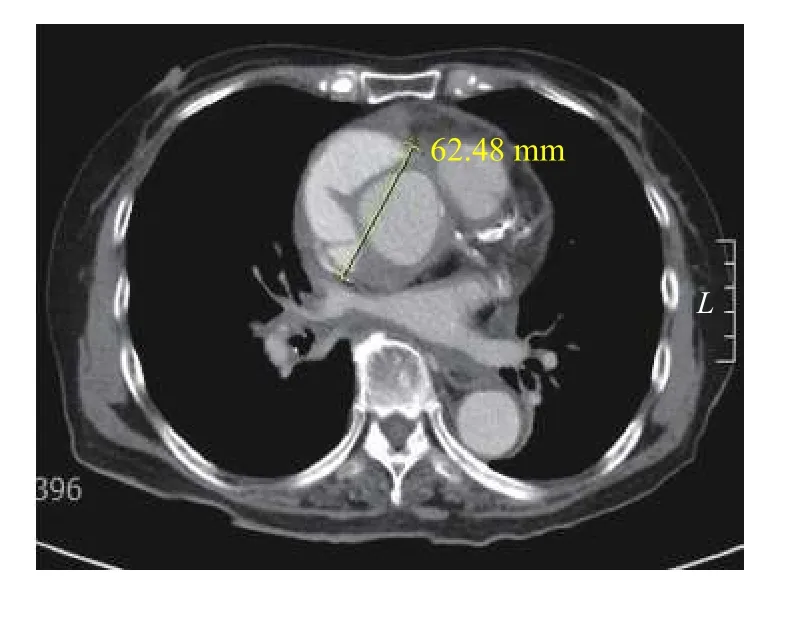
Fig. 3 Preoperative chest computed tomography. This picture showed aortic dissection at ascending aorta (Stanford type A) with a small amount of hemo-pericardium.
Discussion
Uncontrollable cardiac bleeding after aortic root procedures or from the anastomotic sites of the fragile dissected tissues of AAD repair is a nightmare to a cardiac surgeon and his patient. For postoperative care, lots of blood transfusion with strict monitoring on the patient all night and subsequent reoperation for the bleeding control is usually needed. Cabrol and colleagues firstly succeeded in controlling this malignant bleeding after aortic procedure using periaortic to right atrial shunt[1]. And since then some modifications of this kind of Cabrol's shunt has been published[2-4]. But this kind of left-to-right shunt,especially after extravasation of the arterial blood from the native vessel, might cause some extent of thromboembolism through the pulmonary circulation and volume loading of right ventricular which could make postoperative ventricular recovering difficult.
We tried to make contained local compression of upper half of the heart from upper part of the right ventricle to just above the innominate vein, and from right border of SVC to left border of MPA using bovine pericardium with closing both sides of transverse sinus in two cases of uncontrolled postoperative bleedings (bleeding from distal anastomotic site at AAD and from valve sawing ring after modified Bentall procedure). After completion of this patch, quite high pressure was felt under the patch, and effective compression was expected to the bleeding points. Even though reoperations of the two patients were needed usually two days after patch application, the patients were free of the bleeding troubles of massive transfusion, and the surgeon could be back to usual schedule. In conclusion, contained local compression trial could be an alternative strategy for dealing with the malignant uncontrolled bleeding from the fragile aortic tissue or root area after acute dissection or aortic root repair.
杂志排行

THE JOURNAL OF BIOMEDICAL RESEARCH的其它文章
- nNOS-mediated protein-protein interactions: promising targets for treating neurological and neuropsychiatric disorders
- A comparative genomics analysis of lung adenocarcinoma for Chinese population by using panel of recurrent mutations
- Identification of four novel prognosis biomarkers and potential therapeutic drugs for human colorectal cancer by bioinformatics analysis
- α-ketoglutarate promotes the specialization of primordial germ cell-like cells through regulating epigenetic reprogramming
- The testis-specifically expressed gene Trim69 is not essential for fertility in mice
- Valproic acid therapy decreases serum 25-hydroxyvitamin D level in female infants and toddlers with epilepsy— a pilot longitudinal study