Effect of remote ischemic preconditioning among donors and recipients following pediatric liver transplantation: A randomized clinical trial
2021-02-05BoQiXiaoQiangWangShuTingPanPeiYingLiLingKeChenQiangXiaLiQunYangWeiFengYu
Bo Qi, Xiao-Qiang Wang, Shu-Ting Pan, Pei-Ying Li, Ling-Ke Chen, Qiang Xia, Li-Qun Yang, Wei-Feng Yu
Abstract BACKGROUND Studies suggested that remote ischemic preconditioning (RIPC) may effectively lessen the harmful effects of ischemia reperfusion injury during organ transplantation surgery.
Key Words: Pediatric liver transplantation; Remote ischemic preconditioning; Postoperative complications; Ischemia reperfusion injury; Primary nonfunction; Hepatology
INTRODUCTION
Since first performed by Starzlet al[1]in 1963, liver transplantation (LT) has undergone remarkable progress and innovation over the last 50 years. Currently, LT remains the gold standard treatment for patients suffering from end-stage liver disease or metabolic liver disease, with an overall 3-year survival rate exceeding 80% due to advancements in immunosuppressive agents, surgical techniques and perioperative management[2-5]. Approximately 600 pediatric LTs were performed in the United States in 2018[2], with the first pediatric LT successfully performed in 1967 by Starzlet al[6]. Meanwhile, the development of pediatric LT in China has been rapid and prominent, with Renji Hospital becoming the major pediatric LT center, performing more than 400 pediatric LTs in 2019. According to recorded data from Renji Hospital, the overall 3-year survival rate of children in recent years had exceeded 90%.
Despite the outstanding achievements in pediatric LT, some complications, such as primary graft nonfunction (PNF), vascular complications, biliary complications and allograft rejection, still exist[3,5,7,8]. Accordingly, ischemia reperfusion injury (IRI) has been a well-known underlying cause for inducing or aggravating PNF, vascular complications and biliary complications[9-11]. Given that IRIs usually occur when temporarily cutting off and then restoring an organ or tissue’s blood supply, avoiding it during LT is challenging[12]. Although several studies have attempted to ameliorate hepatic IRI[11,13,14], the mechanisms of IRI still remain largely unclear with no definitive therapies having been established.
Remote ischemic preconditioning (RIPC), a simple noninvasive therapy for alleviating the harmful effects of IRI, has shown promise in protecting multiple organs, such as the kidneys, heart and liver[9,15,16]. RIPC is usually performed by inflating and deflating a standard blood pressure cuff placed on the upper arm or thigh to induce transient ischemia and reperfusion, providing systemic multiorgan protection[17]. A number of fundamental and clinical studies have suggested that RIPC can effectively reduce IRI in the liver[9,18-20]. For instance, Abu-Amaraet al[19,20]confirmed that RIPC successfully reduced IRI in a mouse model, while Wuet al[18]found that RIPC was able to reduce hepatic IRI among patients undergoing liver resection. Moreover, Junget al[9]suggested that RIPC might be beneficial for postoperative liver function among recipients after living donor LT. However, other studies have shown no benefits for RIPC in animal models or patients[17,21,22]. Therefore, more studies are needed to validate the effectiveness of RIPC.
Given the current lack of studies on the effect of RIPC on pediatric LT, the present single-center randomized clinical trial aimed to determine whether RIPC could be beneficial for reducing IRI among both donors and recipients undergoing pediatric LT.
MATERIALS AND METHODS
Study design and intervention
This single-center, randomized controlled study had been approved by the ethics committee of the Renji Hospital (2016-002K) and was registered with Clinical-Trails.gov (NCT02830841). Written informed consent was obtained from the donors and families of recipients. The study was conducted in accordance with the Declaration of Helsinki and the CONSORT criteria[23].
Randomization was achieved by using opaque envelopes in which allocations were stored, and random sequence was generated by an independent data manager. Patients who consent to enter this trial were randomly allocated into the S-RIPC group (no intervention to donors and recipients), D-RIPC group (donors received RIPC), RRIPC group (recipients received RIPC), and DR-RIPC group (both donors and recipients received RIPC) in a 1:1:1:1 fashion. No masking was applied except for data assessors.
Donors and recipients in the S-RIPC group underwent the same procedure without RIPC. Donors in D-RIPC group underwent RIPC in the right upper limb after induction of anesthesia and before abdominal skin incision. The cuff was placed in the upper third of the right upper limb, after which three 5-min cycles each of inflation at a pressure of 200 mmHg and subsequent reperfusion with the cuff deflated were performed. Recipients in the D-RIPC group underwent the same procedure except without RIPC. Recipients in the R-RIPC group underwent RIPC with the cuff being placed on the left lower limb at an inflation pressure of 150 mmHg. Donors in the RRIPC group underwent the same procedure except without RIPC. Both donors and recipients in the DR-RIPC group underwent RIPC as described.
Sample size calculation
According to plasma alanine transaminase (ALT) records from 235 children who previously performed LT without RIPC in Renji Hospital, we found that mean natural logarithm of maximum postoperative ALT (ALTmax) was 5.86; assuming the mean logarithm of ALTmaxdecreases to 5.3 after performing RIPC in recipients, which leads to effect sizef= 0.25. Combined with significance level ofα= 0.05, and power of 80%, each treatment group had to include at least 32 patients[24]. Considering 10% dropout rate, we decided to include at least 144 patients in total.
Participants and inclusion/exclusion criterion
A total of 220 patients with biliary atresia and family liver donors who underwent living pediatric LT from January 2016 to January 2019 at Renji Hospital Affiliated with Shanghai Jiao Tong University School of Medicine were eligible for enrollment. The inclusion criteria were as follows: (1) American society of anesthesiologists score of IIII; (2) Age of 3-72 mo; and (3) Elective living LT surgery. The exclusion criteria were as follows: (1) Peripheral vascular disease; (2) History of thromboembolism; (3) Systemic or local infection before surgery; (4) Autoimmune diseases; (5) Severe congenital heart disease, and (6) History of LT.
Variables and data sources
Donors and recipient characteristics were obtained from the electronic medical record system. Pediatric end-stage liver disease grade was calculated as described previously[25]. Early allograft dysfunction (EAD), PNF and acute kidney injury were defined according to published studies[26-28]; EAD was defined as in Olthoffet al[29]; and PNF was defined as graft loss, re-transplantation or death due to graft nonfunction within 30 d after surgery (except those induced by hepatic artery embolism, bile duct complications or recurrent liver disease)[30]. Postoperative complications were classified according to the modified Clavien Grading System[31]. Moreover, all recipients were followed up until July 1, 2019, while recipient survival was updated every 3 mo. Two trained research assistants oversaw data collection and recorded them using “Excel” or “Epidata”.
Anesthetic techniques
Recipients were monitored through regular electrocardiographic monitoring and underwent initial induction with 8% sevoflurane and 5 L/min of O2. After achieving silence, the peripheral veins of the upper limbs were opened, and tracheal cannulation was performed under induction with 0.05 mg/kg midazolam, 1 mg/kg rocuronium and 1 μg/kg sufentanil. The pressure support ventilation mode was selected, with a respiratory frequency of 16-20 times/min. The end tidal carbon dioxide tension was controlled at 35-40 mmHg. Intraoperative anesthesia was maintained using sevoflurane (anesthesia depth at 0.6 minimum alveolar concentration). Intraoperative analgesia and muscle relaxation were maintained using sufentanil (1 μg/kg/h) and rocuronium (0.15 mg/kg/h). Basic vital signs and circulation capacity were monitored and managed regularly. All recipients were sent to the intensive care unit (ICU) for postoperative care.
Donors were monitored through regular electrocardiographic monitoring. The peripheral veins and radial artery were opened for transfusion and invasive blood pressure measurement. Donors underwent induction with 0.05 mg/kg midazolam, 2 mg/kg propofol, 0.6 mg/kg rocuronium and 0.5 g/kg sufentanil. Endotracheal intubation and mechanical ventilation were performed with a tidal volume of 8 mL/kg, while the end tidal carbon dioxide tension was maintained between 35 mmHg and 45 mmHg. Intraoperative anesthesia was maintained using cisatracurium, sevoflurane and remifentanil. Following the right internal jugular vein puncture, an internal jugular vein catheter with double cavities was inserted for central venous pressure monitoring. After the operation, donors were sent to the anesthesia recovery room for resuscitation and extubation.
Surgical techniques
Donors were placed in the horizontal position with an inverted L abdominal incision being utilized according to the surgeon’s preference. Intraoperative doppler ultrasonography was used to confirm the anatomical structure of the hepatic portal vein and hepatic vein, while intraoperative cholangiography was performed to verify the division position of the hepatic parenchyma after cholecystectomy. After completing parenchymal dissection, the anesthetists administered intravenous heparin sodium (0.5 mg/kg). After the left hepatic artery and left portal vein were severed, 50 mg of protamine was used to reverse immediately heparinization. The graft was maintained at 4 °C, after which portal vein perfusion was started. After confirming that the color of the perfusate discharged from the hepatic vein had faded, the graft was transferred to the preserving solution for vascular structure examination and weight measurement. Details regarding the liver graft resection have been described previously[5,9,32].
Recipients were placed in the horizontal position with a straight-line abdominal incision being utilized. The original liver was initially resected, after which the surgery entered the anhepatic phase. Thereafter, the hepatic vein, portal vein and hepatic artery were inosculated and successively opened. The velocity and pattern of blood flow in the new hepatic portal vein, hepatic vein and hepatic artery were determined using color doppler ultrasound. Roux-en-Y biliary jejunostomy was then performed to replace the inosculation of recipients and donors’ biliary duct. Recipients were subsequently transferred to the ICU after confirming that all vessels were fluent and vital signs were stable.
Outcomes
Patients were followed up until July 1, 2019. The primary outcomes examined herein included ALTmaxand maximum aspartate aminotransferase (ASTmax). Secondary outcomes included EAD, PNF, postoperative complications and overall survival of recipients.
Statistical analysis
Statistical analyses were conducted using the IBM SPSS Statistics 26.0 (SPSS Inc., Armonk, NY, United States) and R software (Version 3.6.1). Categorical variables are presented as frequency (n) or proportion (%), while continuous variables were expressed as mean ± standard deviation or median (25% interquartile range, 75% interquartile range). Differences were analyzed through repeated measures/block randomized one-way analysis of variance, followed by post-hoc analysis (Tukey’s test) as appropriate. Moreover, non-parametric tests followed by the Kruskal-Wallis test were utilized for multiple groups comparisons. Categorical variables were compared using the2test with the Yates correction or Fisher’s exact test (when the total sample was < 40 or the expected frequency was < 1). Overall survival curves were created using Kaplan-Meier survival analysis, while the log-rankttest was used to compare differences between the four groups. Additionally, a post-hoc subgroup analysis was used to investigate possible effect modification of four groups. All statistical tests were two-sided withPvalues < 0.05 being considered statistically significant.
RESULTS
Patients were randomly assigned to the four groups (n= 55 per group). Twelve patients were excluded from the study owing to unexpected issues or changes in surgical plans (Figure 1). The remaining 208 patients [S-RIPC group (n= 55), D-RIPC group (n= 51), R-RIPC group (n= 51) and DR-RIPC group (n= 51)] were ultimately analyzed.
Demographic and preoperative/intraoperative characteristics of the recipients and donors are presented in Tables 1 and 2, respectively. No significant differences in demographic or preoperative/intraoperative characteristics were observed between recipients and donors. Recipients in all four groups showed good comparability and consistency.
Recipients were continuously monitored for changes in ALT, AST, total bilirubin, albumin, creatinine (Cr), white blood cell, neutrophil %, hemoglobin and platelet after surgery (0 d) until postoperative day 7, with a portion of the results being presented in Supplementary Table 1. Accordingly, our results found no differences in the aforementioned nine variables except for Cr-D0 (P= 0.029), suggesting a significant reduction in Cr levels at postoperative day 0, which was mainly attributed to the difference between the D-RIPC and S-RIPC group. For donors, no differences were found in all variables (Supplementary Table 2).
Clinical outcomes among recipients are summarized in Table 3. Accordingly, significant differences in ICU duration were observed (P= 0.041). No differences were found for other clinical outcomes. Our results indicated that RIPC did not improve clinical outcomes among recipients or shorten ICU and ventilation duration. On the contrary, those in the DR-RIPC groups seemed to have had longer ICU duration compared to those in the D-RIPC group. In addition, for postoperative complications, no significant differences were observed in donors before discharge (Supplementary Table 3).
Thereafter, the overall survival among recipients was analyzed. Accordingly, the SRIPC, D-RIPC, R-RIPC and DR-RIPC groups had a 3-year survival rate of 90.9%, 96.1%, 90.2%, and 92.2%, respectively, with no differences between all four groups (Figure 2).
Lastly, subgroup analyses were performed for recipients, with the results being similar to those for the primary endpoint and clinical outcomes among recipients (Table 4).
DISCUSSION
The present randomized clinical trial showed that RIPC did not significantly improve liver functions or decrease incidences of EAD, PNF and postoperative complications among both recipients or donors. The primary end points, ALTmaxand ASTmax, did not differ between the four groups regardless of whether donors or recipients received RIPC. Furthermore, no significant differences were found for incidences of EAD, PNF, postoperative complications and the overall survival of recipients. After further analyzing the effects of RIPC on donors, our still results suggested benefits were limited. Nonetheless, some protective effects of RIPC were observed in recipients,including a lower Cr level in the D-RIPC group than the S-RIPC group on postoperative day 0 (P< 0.05), although these were limited to alleviating IRI or improving the prognosis for patients who received LT.
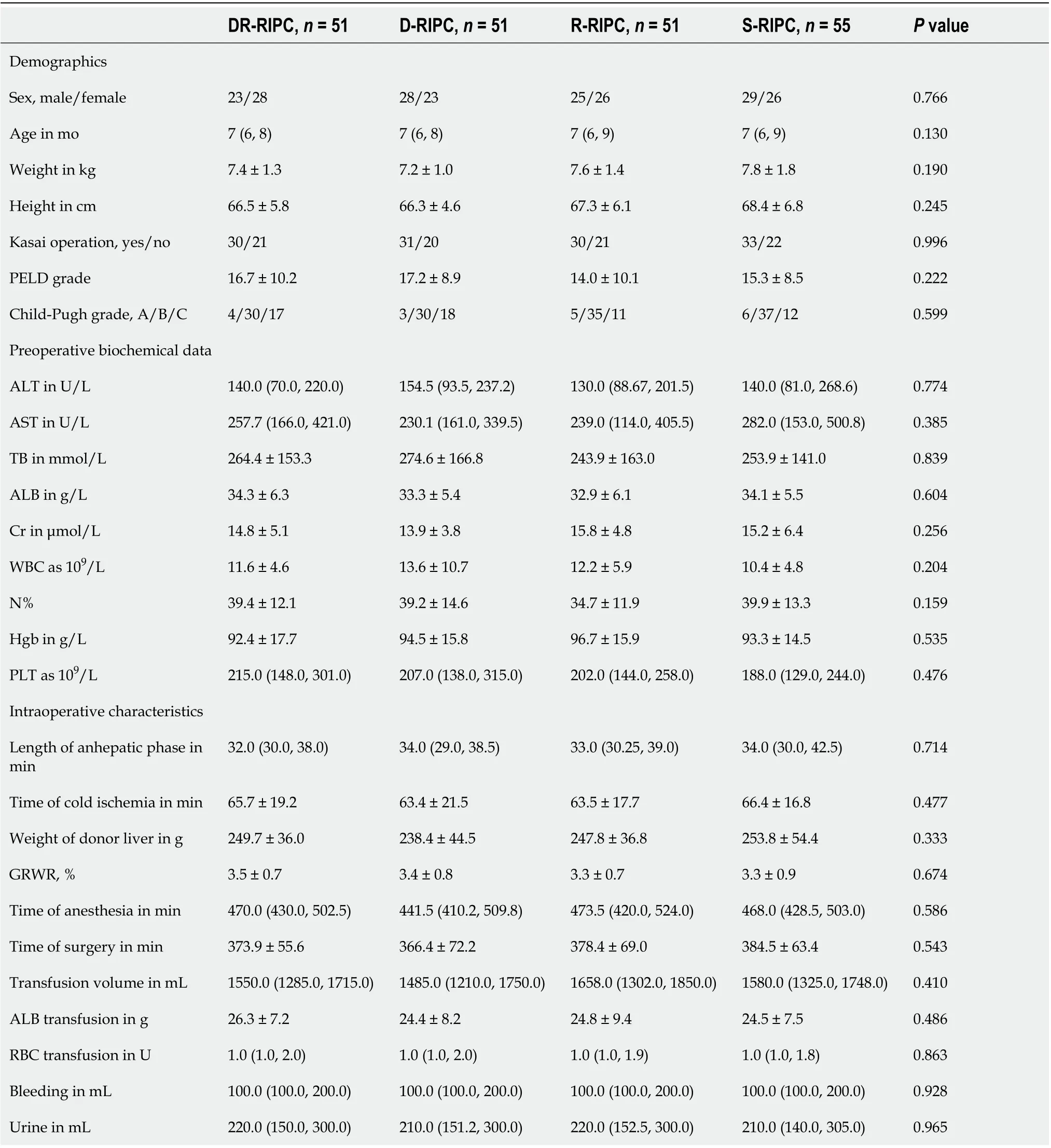
Table 1 Recipient demographics and preoperative and intraoperative characteristics
The discovery of possible protective effects of RIPC in reducing IRI and improving organ function highlights a new therapy for clinical treatment[33]. The most important advantages of RIPC include its low cost, ease of performance and almost impeccable safety for patients. Thus, numerous clinical studies have been conducted to explore effects and potential mechanism of RIPC in different areas, such as organ transplantation, cardiac surgery, hepatic surgery and neurosurgery[9,18,34-36]. Studieshave demonstrated that RIPC mainly occurs in two “windows,” one of which is the initial period following the preconditioning stimulus, which can last for 1-4 h[37,38], while the other happens at 24 h following preconditioning, which can last for 24-72 h[39]. Therefore, detecting related critical characteristics after surgery (0 d) is necessary until at least postoperative day 3. The present study continuously monitored liver function variables from day 0 to postoperative day 7 among recipients and day 0 to postoperative day 3 among donors. The ample amount of data has certainly helped us understand the dynamic changes in liver function, inflammatory response and kidney function of patients.
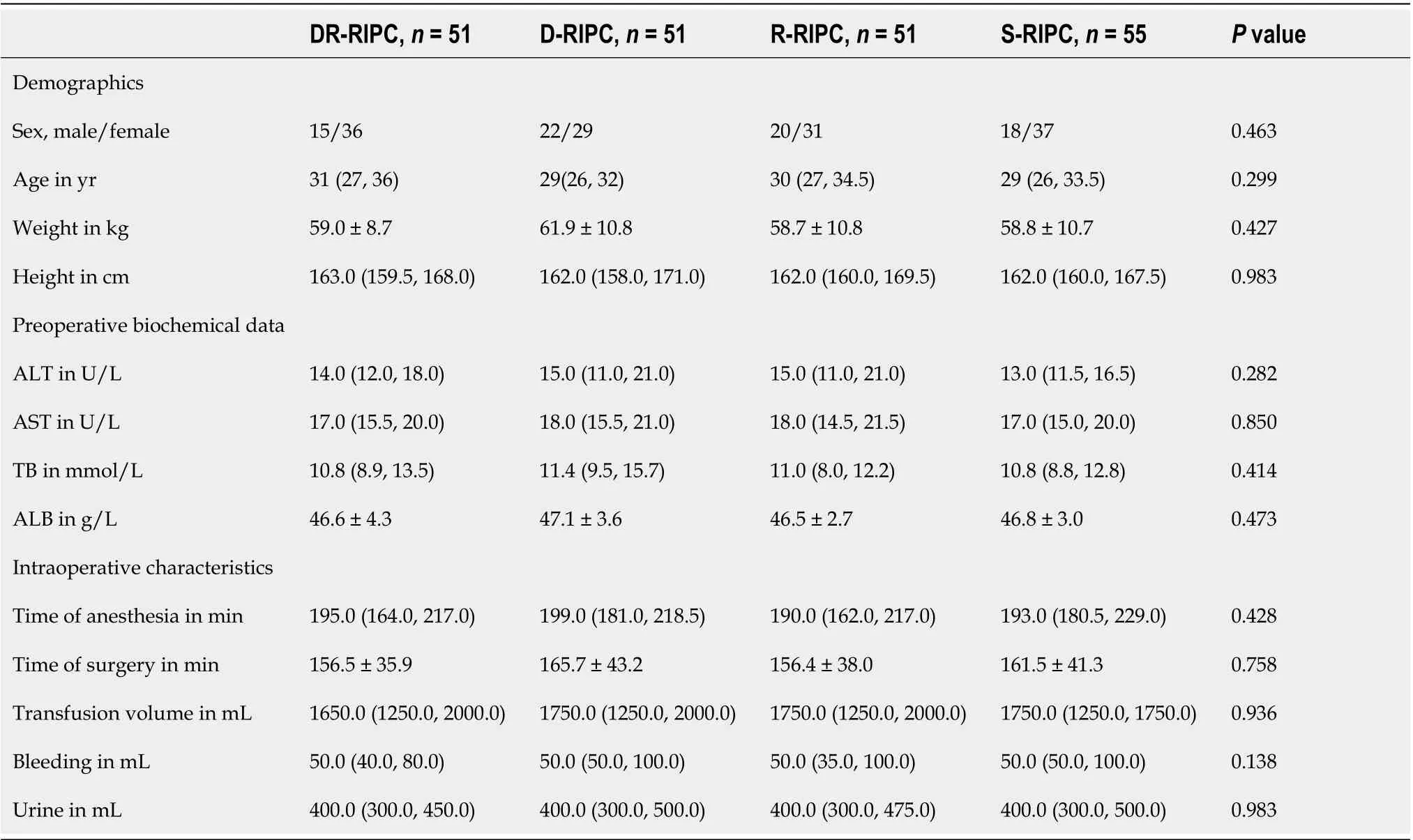
Table 2 Donor demographics and preoperative and intraoperative characteristics
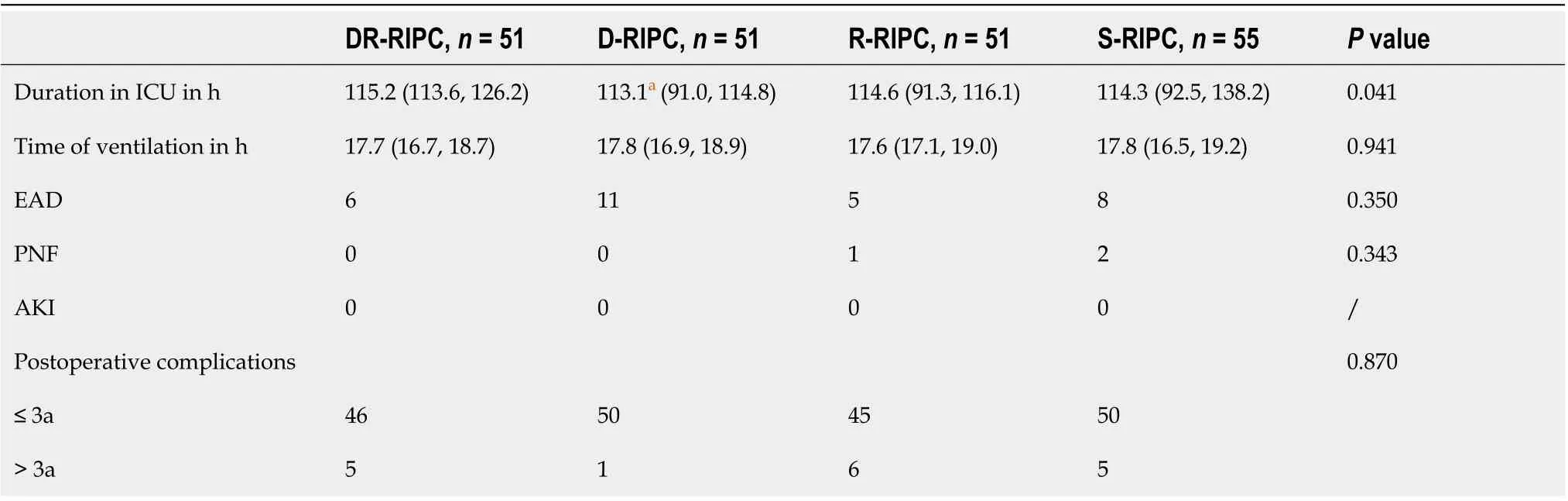
Table 3 Comparisons of clinical outcomes in recipients

Table 4 Subgroup analyses among four groups in recipients
Some potential mechanisms whereby RIPC offers protection have been discussed and can be summarized into three components: Triggers, signal transduction and endeffectors[40]. Accordingly, performing RIPC allowed the local release of certain factors, such as adenosine, cytokines and endogenous opioids, termed “triggers,” thereby activating related protein kinase mediators (e.g., phosphoinositol 3-kinase, janus kinase and signal transducer and activator of transcription and protein kinase C) and signaling pathways[41,42]. Signal transduction plays a critical role in exerting the protective effects of RIPC, with some hypotheses having been presented. The two main competing hypotheses regarding the mechanism of signal transduction include “humoral hypothesis” and “neural hypothesis”[43-45]. “Humoral hypothesis” is supported by evidence showing that protection can be transferred by serum transfusion from a rabbit that has undergone ischemic preconditioning (IPC) to one that has not[46]. Meanwhile, “neural hypothesis” is also supported by a series of studies, especially in the cardiovascular and neural field. Liederet al[44]found that RIPC could activate efferent vagal nerves to stimulate the spleen, which then releases humoral cardioprotective substances. Another study[47]showed that the cardioprotective effects of IPC were completely abolished by denervation of the limbs. To some extent, both the “humoral hypothesis” and “neural hypotheses” are reasonable and interact. After signal transduction, the end-effectors, which could be specific organs, cells or organelles, will finally be activated, and the protective effects induced by RIPC would be transformed into changes in cellular signal pathways[40,43].
A number of studies have focused on the effects of RIPC on graft transplantation. Accordingly, Junget al[9]found that RIPC might be beneficial for postoperative liver function among recipients after living donor LT. AST level on postoperative day 1 and maximal AST level within 7 postoperative days were significantly lower in recipients who received a preconditioned graft. However, their results did not show any definite beneficial effects among donors. Also, no differences were found in the incidence of EAD or graft failure among recipients. A systematic review[10]that summarized solid organ transplantation and RIPC studies found controversial results, with some studies suggesting improvements in graft function, while others not showing any effects. In another meta-analysis[48], the researchers found that donor IPC promoted a large reduction in recipient mortality and incidence of PNF. However, still, no statistically significant difference had been observed. Overall, studies regarding RIPC and LT have been insufficient, especially for RIPC and pediatric LT. Stronger and more convincing clinical trials are thus needed to clarify the effects of RIPC on adult and pediatric LT.
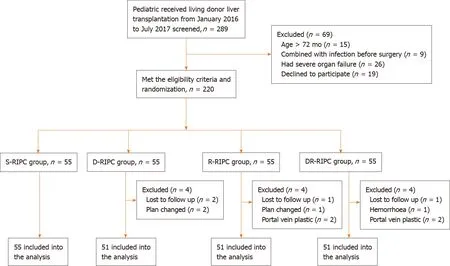
Figure 1 Flow diagram detailing the selection of patients included in the randomized clinical trial. S-RIPC: Remote ischemic preconditioning with no intervention; D-RIPC: Donors received remote ischemic preconditioning; R-RIPC: Recipients received remote ischemic preconditioning; DR-RIPC: Both donors and recipients received remote ischemic preconditioning.
To our knowledge, this has been the first randomized clinical trial to explore the effects of RIPC on pediatric LT. Moreover, we had discussed the effects of RIPC on recipients and donors simultaneously. Generally, RIPC had been performed on donors, while the grafts treated with RIPC were subsequently transplanted to recipients. However, the grafts were flushed to cleanse the organ of blood before storage and introduction into the recipients which could flush away potential protective “triggers” for alleviating IRI[49]. Therefore, RIPC among recipients seemed to promote better effects compared to RIPC among donors. Our study was designed such that patients were divided into four groups, which allowed us to understand comprehensively the effects of RIPC on both donors and recipients. Accordingly, our findings showed that RIPC might have fairly limited effects for protecting liver function or reducing incidences of EAD, PNF and postoperative complications among both donors and recipients. Though our study led to a negative result, it was of high significance and helped us understand the effects of RIPC in pediatric LT. Some reasons may help us understand these results. First of all, the muscle and neural system are relatively immature and undeveloped in children. As a result, the effects of RIPC may have been weakened when the RIPC was performed in recipients, compared with adults. Second, the potential protective “triggers” for alleviating IRI in grafts may have been flushed away before storage and introduction into the recipients. Given the differences in recipients, samples, interventions and group design, it is reasonable to assume that our findings may be inconsistent with those presented in studies that showed significant protective effects of RIPC[18,36].
Some limitations of the present study are worth noting. First, this was a singlecenter study. As such, the inclusion of more centers and more samples would strengthen the clinical significance of the study. Second, measuring more indicators of liver function and IRI, such as interleukin-2, interleukin-6, tumor necrosis factor, malonaldehyde and creatine phosphokinase, would provide more useful information. Third, owing to the lack of consensus regarding the optimal RIPC protocols for adults and children, the cycle and time could have been insufficient to yield the best beneficial effects. In future studies, we would like to attempt more intervention methods.
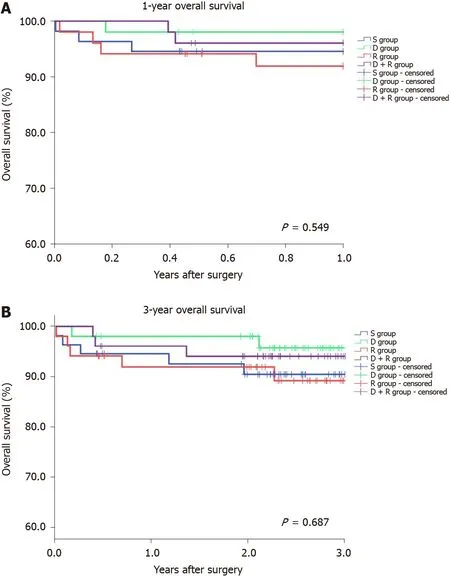
Figure 2 The 1-year (A) and 3-year (B) overall survival analyses of recipients among four groups.
CONCLUSION
In conclusion, the present study suggested that RIPC may have limited beneficial effects on liver and renal function, overall survival or incidences of EAD, PNF and postoperative complications among recipients undergoing LT, as well as liver function among donors. Nonetheless, more clinical trials regarding the effects of RIPC on pediatric LT are warranted.
ARTICLE HIGHLIGHTS
Research objectives
We performed this single-center randomized clinical trial to determine whether RIPC could be beneficial in reducing IRI among both donors and recipients undergoing pediatric living LT.
Research methods
Two-hundred-eight donors were recruited and randomly assigned to four groups: SRIPC group (no intervention), D-RIPC group (donors received RIPC), R-RIPC group (recipients received RIPC) and DR-RIPC group (both donors and recipients received RIPC). We primarily evaluated postoperative liver function among donors and recipients and incidences of early allograft dysfunction (EAD), primary nonfunction (PNF) and postoperative complications among recipients.
Research results
RIPC did not significantly improve alanine transaminase and aspartate aminotransferase levels among donors and recipients and decrease incidences of EAD, PNF and postoperative complications among recipients. Furthermore, RIPC had no effects on the overall survival of recipients.
Research conclusions
The protective effects of RIPC were limited for recipients who received living LT, and no significant improvement of the prognosis was observed in recipients.
Research perspectives
Our research suggested that RIPC may have limited beneficial effects for recipients undergoing LT as well as donors. Nonetheless, more clinical trials regarding the effects of RIPC on pediatric LT are warranted.
杂志排行

World Journal of Gastroenterology的其它文章
- Pleiotropy within gene variants associated with nonalcoholic fatty liver disease and traits of the hematopoietic system
- Preoperative maximal voluntary ventilation, hemoglobin, albumin, lymphocytes and platelets predict postoperative survival in esophageal squamous cell carcinoma
- Clinic-pathological features of metabolic associated fatty liver disease with hepatitis B virus infection
- Could saline irrigation clear all residual common bile duct stones after lithotripsy? A self-controlled prospective cohort study
- Duplication of the common bile duct manifesting as recurrent pyogenic cholangitis: A case report