Reforming Payment Methods for Basic Medical Insurance to Accommodate
2021-01-07ZhouFangZhangXiaohaoMaZhiguo
Zhou Fang Zhang Xiaohao Ma Zhiguo


Traditional Chinese Medicine (TCM) in China: A Case Study of Shaanxi Province
Abstract: Fair and moderate basic medical security is an inherent requirement for the realization of citizens' right to life and health. Improving the legalization level of medical insurance governance is one of the basic principles of the CPC Central Committee and the State Council to continuously promote the reform of medical insurance payment methods. Based on the analysis of the features of TCM, the article, taking Shaanxi Province as an example, studied the status quo of economic development, coverage of TCM diagnosis and treatment services by basic medical insurance, and implementation of payment methods for basic medical insurance in TCM medical institutions. It is pointed out that the current legislative construction process is lagging behind, the basic medical insurance payment method is not suitable for the characteristics of TCM, and the number of TCM medical institutions, service items and medicines covered by basic medical insurance is very limited. The advantages of TCM have not been fully utilized. Therefore, reform of payment methods is pressing. The article suggests accelerating the legislative process in the field of medical security, and forming a legal and regulatory system that is connected with the reform of medical security that is conducive to the establishment and perfection of the system. It recommends guiding health authorities to establish a rating system based on the effectiveness of medical institutions on disease treatment or prevention, and linking it with medical insurance payments. It further recommends promoting the construction of audit standardization in line with the characteristics of TCM, so as to include more qualified Chinese medical institutions, Chinese medicine diagnosis and treatment projects, Chinese medicine decoction pieces, Chinese patent medicines and Chinese medicine preparations in medical institutions into the designated institutions and payment scope of basic medical insurance. When determining the charging items and standards for TCM, the price authorities should seek the opinions of TCM experts, and dynamically adjust them according to the cost and professional technical value. It concludes with a recommendation to establish a list of diagnosis and treatment items that reflect the characteristics of TCM as soon as possible and include them in the scope of outpatient reimbursement for basic medical insurance.
Key words: traditional Chinese medicine (TCM); basic medical insurance; reform on payment methods; Shaanxi Province of P. R. China
CLC:D 912 DC:A Article ID:2096?9783(2021)06⁃0112⁃09
1 Background
Traditional Chinese medicine (TCM) is highly treasured in traditional Chinese culture[1]. It attaches importance to the philosophy of holism and disease prevention. Meanwhile, costs of TCM diagnosis and treatment services are relatively low. Such features of TCM cater to the needs of less developed countries and regions in their endeavor to prevent, diagnose and treat diseases, to increase the equity and accessibility of medical services, and to save basic medical insurance funds. Sadly, these features are not fully regarded in China's current payment system for basic medical insurance nationwide, which has, in turn, failed to incent the demand for and supply of TCM services.
In response to this problem, the state and relevant administrative departments issued a series of reform guidelines. On June 20th, 2017, China's General Office of the State Council issued the Guiding Opinions on Further Deepening the Reform of Payment Methods for Basic Medical Insurance (hereinafter the "Guiding Opinions"). The Guiding Opinions explicitly state that "……exploring payment methods that match the features of TCM services and encouraging the supply and use of appropriate TCM services"[2] are the main aspects of the next step of reform. In addition, the Guiding Opinions authorize local governments to vigorously explore localized medical insurance payment methods, taking into consideration factors such as the capacity of the basic medical insurance fund. On December 5th, 2018, the National Health Commission, along with five other departments, jointly issued the Notice on Launching a Pilot Program for Establishing a Comprehensive Modern Hospital Management System. The notice introduces the pilot tasks of "exploring payment methods that match the features of TCM services and promoting the supply and use of TCM services"[3]. On October 20, 2019, the Central Committee of the Communist Party of China and the State Council released Opinions on Promoting the Inheritance and Development of Traditional Chinese Medicine, further highlighting China's determination to reform payment methods for basic medical insurance tailored for TCM, to improve the equity and accessibility of TCM services, and to enhance public health care throughout the nation[4]. Moreover, the General Office of the State Council issued Guiding Opinions on Establishing and Improving the Outpatient Mutual Aid Guarantee Mechanism for Basic Medical Insurance for Employees on April 22, 2021. The opinion plans to gradually include outpatient expenses in the payment scope of the employee medical insurance fund within three years, establish a sound outpatient mutual aid guarantee mechanism, and gradually reduce the burden of the medical expenses of the insured persons[5].
It should be said that the above?mentioned reform guidelines express the Chinese government's determination to deepen the reform of medical insurance payment methods. However, on the one hand, the path to reform the medical insurance payment method that meets the characteristics of TCM has not yet been clarified. On the other hand, the construction of related medical security legislation lags behind the process of medical security reform, leading to the lack of legalization and guidance in the reform of medical insurance payment methods. Therefore, a feasible path to effectively advance the reform of medical insurance payment methods that conform to the characteristics of TCM is to formulate local medical security legislation at first, and to implement new medical insurance payments that not only reflect the characteristics of TCM, but also meet the actual needs of regional economic development and public health services. At the same time, it is conducive to accumulating practical experience for the formulation and improvement of relevant legislation in our country.
2 Methods
2.1 Study Design
The study takes as its theoretical basis a scientific interpretation of the features of TCM. Shaanxi Province is chosen as a sample for economically underdeveloped regions of China and comparative analysis is made of statistics related to economic development, public health care and coverage of TCM services by basic medical insurance among Shaanxi Province, the nation, and Shanghai Municipality (the region with the highest disposable income per capita in China) in order to ascertain the status of Shaanxi Province in the hierarchy of economic development in China and the gap between Shaanxi Province and economically developed regions. Attention is given to the lack of coordination between payment methods for basic medical insurance in Shaanxi Province and the features of TCM, after which the necessity and significance of reforming such payment methods are highlighted. The study concludes with a proposal for a novel payment method accommodating TCM.
2.2 Data Resource
The data in this study are mainly from China Statistical Yearbook 2020, the newest annual statistical publication available that reflects comprehensively the economic and social development of China. This yearbook covers data for 2019 together with key statistical data in recent years and some historically important years at both the national level and local levels such as provinces, autonomous regions and municipalities directly under the central government[6].
In addition, from August 1 to September 30, 2019, the Shaanxi Administration of TCM conducted a survey of the implementation of the reformation of medical insurance payment methods in 81 public TCM institutions in Shaanxi Province (hereinafter SATCM Survey). The SATCM Survey mainly included: (1) coverage of TCM services by basic medical insurance, (2) adoption of basic medical insurance payment methods, and (3) opinion as to the friendliness of medical insurance payment methods to TCM. In the survey, a total of 81 questionnaires were mailed to 81 public TCM institutions, and a special person was assigned to be in charge of the recovery of questionnaires and data entry. All questionnaires were finally recovered (100.0%), according to which, 79 institutions (97.5%) attempted to reform their present payment methods for basic medical insurance. The data were entered in parallel with EipData3.1 and logical proofreading, and SPSS19.0 was used for data processing and analysis. Based on the survey, this paper analyzes the current reformation of basic medical insurance payment methods in public TCM institutions in Shaanxi Province and their adaptability to TCM services.
3 Overview of Features of TCM
Compared with western medicine, for which most of the present payment methods for basic medical insurance have been tailored, TCM has many unique features and advantages, which is why China holds TCM in high regard and is eager to have it play a more important role in disease prevention and treatment.
3.1 Philosophy of Holism
Based on the concept of holism, TCM regards the human body as an integrated and interconnected system[1], not as dissected parts, and provides disease prevention and treatment services based on syndrome differentiation, aiming to achieve a balance between yin and yang. A good example is San?Fu⁃Tie, a sticking⁃plaster to treat bronchial asthma. San⁃Fu⁃Tie embodies the dialectic and holistic philosophy of TCM's "nourishing yang in spring and summer, and treating winter diseases in summer"[7]. Although the symptoms of bronchial asthma patients usually aggravate in winter and the suffering is alleviated in summer, the period between early July and early September with sultry weather of summer (San⁃Fu Period) is when yang reaches its peak. During this period, the application of San⁃Fu⁃Tie is conducive to strengthening yang of the patients so that in winter new or aggravated symptoms will ease or even disappear, thus achieving the purposes of curing diseases and health preservation. This example points to the challenge to examine TCM diagnosis and treatment services by applying the standards of modern clinical medicine.
3.2 Health Preservation and Disease Prevention
In addition to diagnosis and treatment after a patient falls ill, TCM emphasizes health preservation and disease prevention. Since ancient times, TCM has advocated "countering diseases by preventing them before they begin, just like a good government or emperor is known for taking necessary steps to avert war, while treating diseases after contraction is similar to suppressing a revolt after a breakout"[7]. For instance, San⁃Jiu⁃Tie, a follow⁃up treatment to San⁃Fu⁃Tie, not only enhances the treatment of San⁃Fu⁃Tie, but also aims to prevent disease by strengthening physique[8].
3.3 Effects of Medical Services Heavily Reliant on TCM Doctors' Skills and Quality of Chinese Medicinal Materials
TCM diagnosis is conducted by means of observation (wàng), olfaction (wén), inquiry (wèn), and palpation (qiè), and Chinese medicinal materials, acupuncture, and massage are applied for treatment[9]. Consequently, the effect of TCM diagnosis and treatment is subject to human endeavor, such as knowledge, experience, and level of skill of TCM doctors, as well as the quality of the Chinese medicinal materials prescribed.
3.4 Individualized Treatment Plans
TCM holds that even for the same disease, the symptoms may vary greatly on the basis of the age, gender, and physical conditions of individual patients. In light of this, the therapeutic plans for various patients with the identical disease often differ according to the "verification of the syndromes"[1]. Even in the course of treatment for the same patient, the assorted Chinese medicinal materials in the same prescription will be adjusted from time to time as the phase of disease and condition of the patient may require. For example, in the fight against the novel coronavirus pneumonia (COVID?19) outbreak in China in 2020, TCM doctors implemented an individualized treatment method of "one person, one prescription", and the cure rate has been clinically verified.
3.5 Less Costly Diagnosis and Treatment Services
Based on statistics from the White Paper: Chinese Medicine in China, with relatively low cost, TCM has contributed a higher share of services in relation to the resources it is entitled to. In 2015, outpatient expenses and inpatient expenses per visit to public TCM institutions were, respectively, 11.5 percent and 24 percent lower than those to non⁃TCM public institutions [1]. Furthermore, due to the emphasis on disease prevention, TCM diagnosis and treatment activities are more suitable for outpatients. Therefore, active and steady promotion of the coverage of TCM institutions by basic medical insurance will not only help to promote the development and inheritance of TCM services in accordance with TCM's own laws, but also reduce the economic burden on patients, reduce hospitalization rate, and save medical insurance funds.
4 Analysis
4.1 Reformation in Payment Methods to Accommodate TCM in Shaanxi Province: A Pressing Task
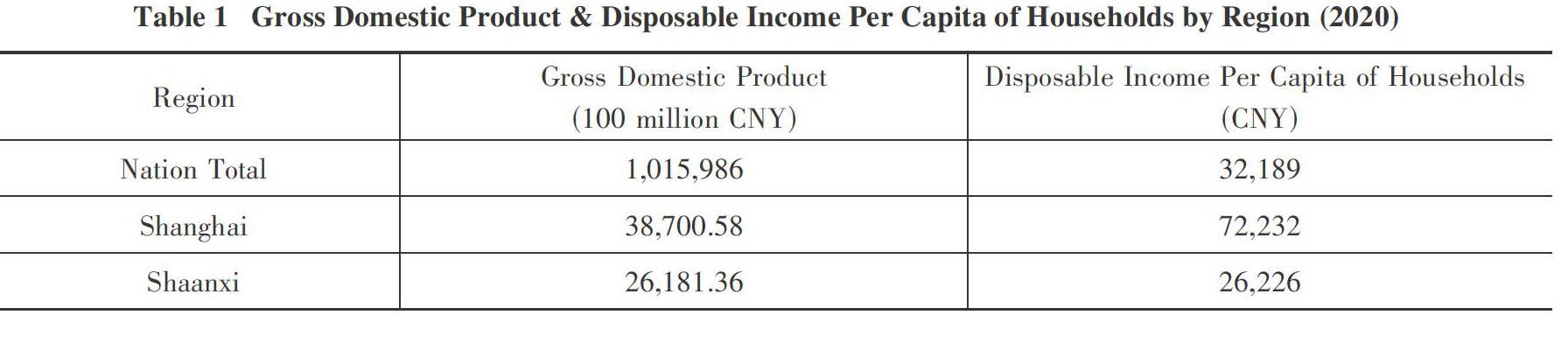
Shaanxi province is located in central China and covers an area of 205,600 km2 with a population of 38.76 million by 2019[6]. Though known for its rich TCM resources, Shaanxi Province is categorized as an economically underdeveloped region in China due to its low GDP and disposable income per capita of households. In 2019, the disposable income per capita in Shaanxi Province was 24,666 CNY (as compared to the national average of 30,733 CNY nationwide) [6]. The corresponding figure in 2020 was 26,226 CNY, once again below the national average of 32,189CNY, and roughly one⁃third of that in Shanghai Municipality (Table 1) [10].
Moreover, the public health care in Shaanxi Province is problematic. Corresponding to its economic development, the annual revenue of basic medical insurance in Shaanxi Province is comparatively low, even less than half of Shanghai Municipality. The same is true with the surplus of basic medical insurance fund at year?end in Shaanxi Province where the revenue and the expense are roughly balanced. (Table 2)
As for coverage by basic health insurance, there are 163 TCM institutions, with a total of 30,815 beds in Shaanxi Province, but only 17 institutions are covered by basic medical insurance at provincial level in 2019⁃2020[11]. This low rate is echoed by the SATCM Survey. According to the survey, from January to December 2018, the numbers of outpatients and inpatients in the 81 institutions were respectively 9,600,253 (92.96% of total) and 727,306 (7.04% of total). The number of discharged patients covered by basic medical insurance was only 422,041, only taking up 4.09% of the total cases since no outpatients are eligible for basic medical insurance reimbursement.
Therefore, to achieve accessibility and fairness of public medical services and to save basic medical insurance funds significantly, it is necessary to reform the payment methods for basic medical insurance in Shaanxi Province to accommodate TCM, so as to optimize such TCM adavantages as lower costs and disease prevention. Furthermore, the experience of designing and implementing such reform can provide a reference for other provinces and regions with similar economic development.
4.2 Between Current Payment Methods and TCM Services: Big Gap to Fill
On September 30, 2017, the General Office of the People's Government of Shaanxi Province issued the Implementation Scheme of Deepening the Reform of Payment Methods for Basic Medical Insurance in Shaanxi Province (hereinafter Implementation Scheme). The Implementation Scheme confirms the goals of the reform as follows: "From 2017, we will further enhance the budget management of basic medical insurance, and gradually advance the reform in payment mechanism featured by diversified and differentiated payment methods based on the principle of total quantity control with payment by disease type as the preferable method. The reform will improve various other payment methods like payment by per capita, quotas, and bed⁃days. We encourage regions with favorable conditions to explore pilot payment methods based on diagnosis⁃related groups."[12] On May 14, 2018, the Department of Human Resources and Social Security of Shaanxi Province issued the Notice to Further Advance of the Reform of Payment Methods for Basic Medical Insurance, which further explains that in 2018, the types of diseases covered by basic medical insurance in each city shall be no less than 100 [13].
However, in the process of reformation in Shaanxi Province, the payment methods being adopted are obviously not yet ready to embrace TCM.
4.2.1 Total Quantity Control Method: Failing to Mirror Costs for TCM
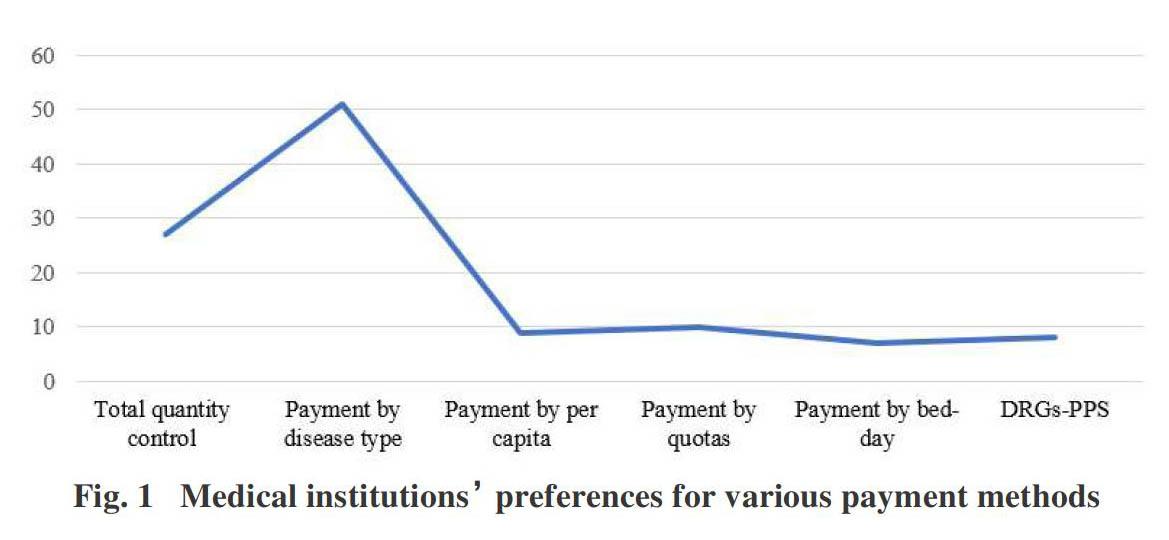
The total quantity control method is the practice of fixing the current payment amount by referring to historical data of cost on the part of medical institutions and payment capacity on the part of basic medical insurance funds, aiming to achieve the goal of cost control. However, in recent years, market prices of Chinese medicinal materials have increased more markedly than those of western medicines due to factors like environmental depredation and soaring labor costs [8]. The price increase is especially dramatic for high⁃quality authentic Chinese herbal medicines. Besides, it is very challenging to foresee fluctuations in prices for the purpose of cost estimation. Thus, a presumption based on historical data may more often than not result in insufficient compensation to medical institutions, incapacitating them for meeting expenses and consequently damping the enthusiasm of medical institutions and their personnel for TCM services. The relevant policies and laws lack a dynamic price adjustment mechanism that adapts to the characteristics of TCM. Among the 81 public TCM institutions participating in the SATCM Survey, 43 institutions put in place total quantity control payment method. The number of cases settled in 2018 was 192,308 (Table 3), accounting for 45.57% of the 422,041 cases covered by basic medical insurance throughout the year. From the perspective of the number of cases settled, it can be said that the total quantity control method is the most popular method adopted by public TCM institutions in Shaanxi Province. However, at the same time, only 27 of the 81 institutions (33.33%) responded in the survey that the total quantity control method can reasonably reflect the cost of TCM doctors/institutions' services, and can in turn effectively mobilize the doctors' enthusiasm to inherit and practice TCM (Fig. 1).
4.2.2 Payment by Disease Type: Inconsistent with TCM's Philosophy of Holism
Payment by disease type is the payment method to determine fixed payment amounts based on universal disease categories, the "clinical path" of a single disease, and to calculate inpatients' costs relating to a specific disease[9]. Because TCM diagnosis and treatment services highlight the philosophy of holism and syndrome differentiation, disease?type⁃based payment not only undermines the integrity of TCM services, but also puts unreasonable restraint on the capacity of the TCM treatment process to make adjustments according to the phase of diseases and individual patients' conditions. The SATCM Survey, on the one hand, found that although 69 public TCM institutions had been reimbursed by disease types, the number of disease types paid was quite limited in general (only 7 institutions had been reimbursed for more than 100 disease types). On the other hand, the number of cases settled by the disease type payment method was also limited: in 2018, a total of 81,669 cases were settled, accounting for only 19.35% of the total cases (Table 3). Of the 81 institutions, 51 (62.96%) agreed that payment by disease type can reasonably reflect the cost of TCM doctors/institutions' services, and can in turn effectively mobilize the doctors' enthusiasm to inherit and practice TCM (Fig. 1). Although the survey shows that most medical institutions prefer this payment method, due to the limited number of disease types, the actual number of cases paid is relatively small.
4.2.3 Payment by Per Capita, Bed⁃day, or Quotas: A Poor Guide for TCM Services
Payment by per capita (i.e., the number of visits multiplied by the approved average outpatient fee), by bed⁃day (i.e., the number of bed⁃days multiplied by the rigorously calculated daily fee or pre⁃calculated fixed item fee), and by quotas (i.e., pre⁃calculated fixed item fee) are in essence all payment methods of fixed amounts. TCM services rely heavily on the doctors' knowledge, experience, and skill to diagnose and treat diseases, which are time⁃consuming and labor⁃intensive processes. TCM diagnosis and treatment are patient⁃specific as well. In practice, the fixed payment that ignores the effect of diagnosis and treatment prompts TCM doctors to substitute traditional diagnosis based on doctors' personal judgments with machine⁃based test results[9]. This will not only result in the dying out of many traditional diagnostic and treatment methods, but also undermine the reputation of TCM services. Moreover, such payment methods increase the financial burden of patients and meanwhile cause the waste of medical insurance funds. The SATCM Survey revealed that neither payment by per capita nor payment by bed⁃day was widely adopted in public TCM institutions: 10 institutions settled on a per⁃capita basis 39,576 cases (9.38% of total) and 3 institutions settled on a bed⁃day basis 13,177 cases (3.12% of total). Relatively more institutions adopted payment by quotas: 26 institutions took this method, with a total of 92,555 cases paid (21.93% of total) (Table 3). However, among these institutions, only 9, 10, and 7 institutions responded respectively in the survey that paying by per capita, bed⁃day, or quotas can reasonably reflect the cost of TCM doctors/institutions' services, and can in turn effectively mobilize the doctors' enthusiasm to inherit and practice TCM (Fig. 1).
4.2.4 DRGs?PPS: Incapable of Reflecting the Value of TCM Services
DRGs⁃PPS is a prospective payment system (PPS) based on diagnosis⁃related groups (DRGs). In this method, a scientific calculation of payment standard for each group is made first, and then advance payment based on such payment standard will be made to medical institutions[14]. The DRGs classify and then group patients with similar principal diagnoses, the assumption being that these diagnoses require similar treatment protocols and hence consume a similar reservoir of resources[15]. In order for the DRG scheme to be practical and meaningful, there should be a manageable number of DRGs encompassing all patients seen on an in⁃patient basis, and each DRG should contain patients both with a similar pattern of resource intensity and similar from a clinical perspective[15].
The International Classification of Diseases (ICD), the diagnostic classification standard for all clinical and research purposes, is the basis and criteria for DRG grouping[16]. WHO was entrusted with the creation of ICD in 1948 and has published 11 versions by now. ICD⁃10, endorsed in May 1990 by the Forty⁃third World Health Assembly, has been widely cited and adopted by more than 100 countries around the world. The latest version, ICD⁃11, was released on 18 June 2018 to allow member states to prepare for implementation. There are 26 chapters in ICD⁃11: chapters 1⁃24 encode various disease classifications, chapter 25 encodes special purposes, and chapter 26 encodes a supplementary chapter for "Traditional Medicine Conditions ⁃ Module I". This supplementary chapter refers to disorders and patterns which originated in ancient Chinese Medicine. But the description of the chapter says that this supplementary chapter is a subclassification for optional use and not intended for mortality reporting. Coding should always include also a category from chapters 1⁃24 of ICD[17].
TCM prescribes individualized treatments based on each patient's physical conditions and syndromes[1], therefore contradicting the grouping practice of DRGs. Consequently, it would be impossible to design payment groups for TCM diagnosis and treatment services in line with the categories in ICD, and the principles of whether there exists a significant complication or comorbidity. That is, DRGs, which determine payment rates based on the difficulty in diagnosis and the differences in costs, cannot accurately group TCM services. According to the SATCM Survey, only 3 out of the 81 public TCM institutions were paid by DRGs?PPS, with 2,756 cases (0.65% of total) settled in 2018. However, 8 institutions (9.88% of total) responded that payment by DRGs can reasonably reflect the cost of TCM doctors/institutions' services, and can in turn effectively mobilize the doctors' enthusiasm to inherit and practice TCM (Fig. 1).
In conclusion, the reformation of payment methods for basic medical insurance in Shaanxi TCM medical institutions is highly unsatisfactory. The fundamental reason lies in the fact that in the absence of a medical security legal system that reflects the characteristics of TCM, the existing payment methods fail to take into consideration the striking differences between TCM and western medicine in terms of concept, manners of diagnosis and treatment, and use of medicine.
5 Discussion
A fair and moderate basic medical security is an inherent requirement for the realization of citizens' right to life and health. Improving the legalization level of medical insurance governance is one of the basic principles of the CPC Central Committee and the State Council to continuously promote the reform of medical insurance payment methods. In light of the disharmony between the present payment methods for basic medical insurance and TCM, it is urgent to initiate reforms that accommodate TCM in Shaanxi Province. Such reforms, by optimizing the advantages of TCM, will not only enhance equity and accessibility of medical services to the public, but also reduce medical costs. They will also help save basic medical insurance funds and provide a reference for other underdeveloped areas in China. To this end, we suggest, accelerating the legislative process in the field of medical security, and forming a legal and regulatory system that is connected with the reform of medical security and is conducive to the establishment and perfection of the system. In particular, we recommend the following initiatives:
The first, to guide government to adopt a novel payment method based on the overall effectiveness of medical services in legislation. The government should strengthen the process supervision of medical activities in medical institutions, establish an evaluation system and a list of negative issues focusing on evaluating the effects of disease prevention and treatment, rewarding medical institutions with excellent evaluations and punishing those with unqualified evaluations by fee reduction. By focusing on the health conditions of the insured, and attaching importance to holism and disease prevention, this new payment method fits in perfectly with the features of TCM. It has the rights and interests of patients at its core, and meanwhile ensures the efficient use of basic medical insurance funds.
The second, to establish a departmental coordination mechanism. The basic medical insurance administrations shouldcooperate with TCM administrations to establish auditing standards fit for TCM, and cover more qualified TCM institutions in basic medical insurance. Additionally, these administrations should adjust the mechanism of negotiations with the medical insurance institutions, expanding the scope of payment of basic medical insurance funds to cover all qualified TCM diagnosis and treatment programs, herbal decoction pieces, formulated medicines, and TCM preparations produced by medical institutions.
The third, to establish expert assistance and a dynamic price adjustment mechanism. In deciding what items to charge and fee standards for TCM services, the price management department should solicit opinions from TCM experts. Besides, the price is to be adjusted dynamically with the costs and values of professional techniques to ensure the continuity and extensive innovation of TCM services.
Last but not least, to produce legislation that will clarify the legality of basic medical insurance covering outpatient clinics. This will not only highlight the advantages of TCM diagnosis and treatment services, but also help reduce the financial burden on patients and save medical insurance funds in general. This will greatly improve the accessibility and equity of TCM services and in turn public health care to patients in less⁃developed areas. Therefore, legislation should guide the medical insurance management department to coordinate with the Chinese medicine management department to establish a list of diagnosis and treatment items that reflect the characteristics of TCM (including disease prevention, treating winter diseases in summer, and so on), and include it in the scope of outpatient reimbursement for basic medical insurance as soon as possible.
6 Conclusion
In conclusion, this article proposes to promote the construction of relevant local legislation, deepen the reform of basic medical insurance payment methods by introducing a novel payment method accommodating the features of TCM diagnosis and treatment services in economically less developed regions like Shaanxi Province. The reform aims to optimize such advantages/benefits of TCM services as disease prevention and relatively low cost by first designing evaluation indicators for effects of medical services, taking into consideration the value and cost of TCM diagnostic and treatment services, and paying for TCM services on the basis of a comprehensive evaluation of medical services, and then, to ensure coverage of outpatient diagnosis and treatment services and more qualified TCM medical institutions, diagnosis and treatment services, and medicines by basic medical insurance.
References:
[1] China's State Council Information Office. White Paper on Traditional Chinese Medicine in China[EB/OL]. [2021?2⁃20]. http://www.china.org.cn/chinese/2017⁃01/17/content_40120942.htm.
[2] General Office of the State Council of PRC. Guiding Opinions on Further Deepening the Reform of Payment Methods for Basic Medical Insurance[EB/OL]. [2021⁃4⁃08]. http://www.gov.cn/zhengce/content/2017⁃06/28/content_5206315.htm.
[3] National Health Commission, along with five other departments of PRC. Notice on Launching a Pilot Program for Establishing a Comprehensive Modern Hospital Management System[EB/OL]. [2021⁃4⁃08]. http://www.nhc.gov.cn/tigs/s7848/201812/8ff748fb0c404a5c8eb9e7b3c1a64ee3.shtml.
[4] Central Committee of the Communist Party of China and the State Council. Opinions on Promoting the Inheritance and Development of Traditional Chinese Medicine[EB/OL]. [2021?4⁃08]. http://www.gov.cn/gongbao/content/2019/content_5449644.htm.
[5] General Office of the State Council. Guiding Opinions on Establishing and Improving the Outpatient Mutual Aid Guarantee Mechanism for Basic Medical Insurance for Employees[EB/OL]. [2021⁃5⁃08]. http://www.gov.cn/zhengce/content/2021⁃04/22/content_5601280.htm?gov.
[6] National Bureau of Statistics. China Statistical Yearbook (2020)[EB/OL]. [2021⁃6⁃18]. http://www.stats.gov.cn/tjsj/ndsj/2020/indexch.htm.
[7] Yellow Emperor. Canon of the Yellow Emperor: Basic Questions[M]. Beijing, China: People's Medical Publishing House, 2012.
[8] Zhu J. Awkward Situation and Development of TCM under the Existing System of Medical Insurance[J]. Tianjing Social Insurance, 2017(5): 53⁃55.
[9] Xie Junming, Zhang Qiqin, Wang Zhongyan, Qiu Wanru. Consideration on the Payment Methods and Standards of Medical Insurance Service in Traditional Medicine Service[J]. China Medical Insurance, 2017(7): 51⁃53.
[10] National Bureau of Statistics. Residents' Income and Consumption Expenditures in 2020 [EB/OL]. [2021⁃1⁃18]. http://www.stats.gov.cn/tjsj/zxfb/202101/t20210118_1812425.html.
[11] Shaanxi Provincial Healthcare Security Administration. List of the Basic Medical Insurance Institutions of Shaanxi Province 2019⁃2020[EB/OL]. [2021⁃1⁃18]. http://ybj.shaanxi.gov.cn/zwgk/sjfb/qgyljgcx/959.htm.
[12] General Office of the People's Government of Shaanxi Province. Implementation Scheme of Deepening the Reform of Payment Methods for Basic Medical Insurance in Shaanxi Province[EB/OL]. [2021⁃4⁃08]. http://www.shaanxi.gov.cn/zfgb/97485.htm.
[13] Department of Human Resources and Social Security of Shaanxi Province. Notice to Further Advance of the Reform of Payment Methods for Basic Medical Insurance[EB/OL]. [2021⁃1⁃18]. http://219.144.222.219:8899/html/100253/1013499.html.
[14] Zhu Shijun, Bao Yurong. Brief Introduction to DRGS: Reform on the Payment Methods of Medical Costs[J]. China Journal of Hospital Administration, 2006, l22 (20): 664⁃665.
[15] Centers of Medicare & Medicaid Services (USA). Design and Development of the Diagnosis Related Group (DRG)[EB/OL]. [2020?4⁃18]. https://www.cms.gov/icd10m/version37⁃fullcode⁃cms/fullcode_cms/Design_and_development_of_the_Diagnosis_Related_Group_(DRGs).pdf.
[16] Zhang Xi. Function of ICD for Implementing DRGs in Hospitals[J]. Huaxia Medicine, 2018, 31(5): 152⁃155.
[17] WHO. Classification of Diseases[EB/OL]. [2020⁃1⁃08]. https://www.who.int/classifications/icd/en/.
适应中医药特点的基本医疗保险支付方式改革:以陕西省为例
周方 张小号 马治国
(1. 西安交通大学 法学院,西安710049;2.西安外国语大学 高级翻译学院,西安710128)
摘 要:公平适度的基本医疗保障是实现公民生命健康权的内在要求。提高医保治理法治化水平是党中央、国务院持续推进医保支付方式改革的基本原则之一。文章以陕西省为例,在分析中医药特点的基础上,研究了当前经济发展现状、基本医疗保险对中医药诊疗服务的覆盖范围以及中医药基本医疗保险支付方式的实施状况。指出当前立法进程滞后,现行基本医疗保险支付方式并不适应中医药的特点,所覆盖的中医医疗机构、服务项目和药品数量也非常有限,中医药优势并未得到充分发挥。因此,支付方式改革迫在眉睫。文章建议:加快推进医疗保障领域立法进程,形成与医疗保障改革相衔接、有利于制度定型完善的法律法规体系。引导卫生主管部门根据医疗机构对疾病治疗或者预防的效果建立评级制度,并与医保支付相挂钩。推进符合中医药特点的审核标准化建设,将更多符合条件的中医医疗机构、中医诊疗项目、中药饮片、中成药和医疗机构中药制剂纳入基本医疗保险定点机构及支付范围。物价主管部门在确定中医药服务收费项目和标准时,应当征求中医药专家的意见,且需根据成本和专业技术价值动态调整。尽快建立反映中医药特色的诊疗项目清单,并将其纳入基本医疗保险门诊报销范围。
关键词:中医药; 基本医疗保险;支付方式改革;陕西
