Postural control quantification in minimally and moderately impaired persons with multiple sclerosis:The reliability of a posturographic test and its relationships with functional ability
2020-12-18DavidBarbadoRamonGomezIllanPedroMorenoNavarroGregoriValeroConesaRaulReinaFranciscoVeraGarcia
David Barbado,Ramon Gomez-Illan,Pedro Moreno-Navarro,Gregori Valero-Conesa,Raul Reina,Francisco J.Vera-Garcia*
Department of Sport Sciences,Sports Research Centre,Miguel Hern′andez University of Elche,Elche(Alicante)03202,Spain
Abstract Background:Postural control has been associated with the functional impairment in persons with multiple sclerosis(pwMS).However,there is a need for reliable methods to assess postural control in early stages of the disease,when subtle changes can be difficult to detect.The aims of this study were to assess the absolute and relative reliability of a standing and a sitting posturographic protocol in minimally(Expanded Disability Status Scale≤2)and moderately(2.5≤Expanded Disability Status Scale≤4)impaired pwMS,and to analyze relationships among postural control and functional mobility and gait performance.Methods:To assess postural control in an upright stance,14 minimally and 16 moderately impaired pwMS performed six 70 s trials in tandem stance,3 with their weaker leg behind(TSWL)and 3 with their stronger leg behind(TSSL).Additionally,participants completed five 70 s trials using an unstable sitting protocol(US)to assess trunk stability.The mean radial errors of TSWL,TSSL,and US trials were calculated as postural control indexes.Furthermore,participants performed the Timed Up and Go test(TUG)and the Timed 25-foot Walk test(T25FW)to measure their functional mobility and gait speed,respectively.Reliability was evaluated using the intraclass correlation coefficient(ICC3,1)and the standard error of measurement(SEM).Analyses of variances were carried out to assess between-group differences.Hedges'g index(dg)was used to estimate the effect size of differences.Pearson correlation analyses(r)were performed to examine the relationships among the postural control and the functional tests.Results:Posturographic tests showed a high reliability in both minimally(0.87≤ICC≤0.92;9.32%≤SEM≤11.76%)and moderately(0.80≤ICC≤0.92;10.33%≤SEM≤15.33%)impaired pwMS.Similarly,T25FW and TUG displayed a high consistency in minimally(0.89≤ICC≤0.94;3.43%≤SEM≤5.17%)and moderately(0.85≤ICC≤0.93;5.57%≤SEM≤6.56%)impaired individuals.Minimally impaired pwMS showed a better performance on the TUG,T25FW,and TSWLthan moderately impaired individuals(p<0.05;dg≥0.8).The TSWL,TSSL,and US variables correlated with TUG scores(0.419≤r≤0.604;p<0.05),but TSWLalso correlated with T25FW scores(r=0.53;p<0.01).Furthermore,US scores correlated with both tandem stance parameters(TSWL:r=0.54,p<0.01;TSSL:r=0.43,p<0.05).Conclusion:TandemandsittingposturographictestsprovidereliablemeasuresofposturalcontrolinpwMS,eveninindividualswithahomogeneousdisease pro file.Gait speed,functional mobility,and weaker leg status seem decisive in assessing the degree of physical activity limitation in pwMS.Finally,although trunk stability does not seemto be so affected by the course of the disease,it remains relevant for postural control and functional capacity.
Keywords:Balance;Consistency of the assessment;Core stability;Functional mobility
1.Introduction
Multiple sclerosis(MS)is an immune-mediated neurodegenerative disease that affects the central nervous system,which frequently results in postural control impairments.1These impairments are an important concern for persons with MS(pwMS),because they have a severe impact on their ability to perform mobility-related activities during their daily life2,3(e.g.,manual activities while standing,rising from a chair,walking,and turning),which in turn may increase the probability of suffering a fall.4,5A precise postural control evaluation in pwMS is needed for a better understanding of its impact on functional parameters and also to facilitate an early detection of balance de ficits,which may help to implement more aggressive therapeutic interventions.
Posturography is considered an objective and accurate technique to assess postural control because it discriminates between pwMS and matched healthy individuals;6-13more important,it reveals subtle postural control decreases in pwMS that would usually be untraceable using common clinical scales.8,9,11,14,15Some reliability studies have shown that posturographic protocols have good relative consistency(intraclass correlation coefficient(ICC):0.62-0.93),allowing a proper classification of pwMS according to their postural control level.7,16,17However,the samples of pwMS in these studies were very heterogeneous(as participants showed a broad range of Expanded Disability Status Scale(EDSS)scores)that,owing to ICC sensitivity to sample heterogeneity,18could have artificially increased the relative reliability of these protocols and thus facilitated the classification of the patients.Moreover,to the authors'best knowledge,there are no studies that have assessed the absolute reliability of the posturographic protocols(i.e.,trial-to-trial variation);therefore,their ability to discriminate between clinically relevant changes in postural control(caused by the disease progression)and normal day-to-day variability remains unknown.Therefore,future studies should analyze the absolute and relative reliability of posturographic protocols in pwMS,especially in patients with similar EDSS scores.
Most posturographic protocols used in this population measure the stability of the whole body in upright stance;15however,posturography has been scarcely used to assess the extent to which trunk control is impaired in pwMS.Because of the upper body's large mass and height above the ground,19the control of this structure is an important factor for balance,especially in challenging conditions,such as when the support surface is narrow or the individual is exposed to sudden and forceful perturbations.20,21Moreover,it has been proven that trunk stability is a main element of gait and functional mobility in patients with different neurologic disorders(such as cerebral palsy,22,23stroke,24,25and Parkinson's disease26).However,to the authors'best knowledge,only 2 studies have used posturography in a sitting position to assess trunk postural control in pwMS.27,28In comparison with the upright stance protocols,these posturographic tests decrease the in fluence of the lower limbs on task performance,while they increase the role of the upper body in postural control.Although several studies have shown the reliability of these sitting protocols in other populations,19,29-32only 1 study has analyzed the reliability of an unstable sitting test in pwMS.28This study showed the relative reliability of the protocol,but the absolute reliability was not analyzed.Thus,new,reliable posturographic protocols should be developed to assess trunk postural control in pwMS,especially considering that none of the posturographic studies performed in a sitting position were carried out on ambulatory pwMS27,28and,consequently,the role of trunk control on balance and gait in these less impaired MS individuals remains unclear.A correlation analysis between trunk control and functional performance in this population would help to determine how much emphasis should be placed on improving the control of the core structures during rehabilitation or training programs.
Based on these limitations,the main objective of this study was to assess the absolute and relative reliability of a standing(tandem stance(TS)balance test)and a sitting(unstable sitting(US)balance test)posturographic protocol in minimally and moderately impaired pwMS.The second aim was to analyze the potential relationship between standing and sitting postural control parameters on functional mobility and gait performance in pwMS,assessed by two of the most common clinical tests used in this population:the Timed Up and Go Test(TUG)33and the Timed 25-foot Walk Test(T25FW),34respectively.
2.Methods
2.1.Participants
hirty pwMS(Table 1)were recruited from regional patient associations based on the following inclusion criteria:(1)medical diagnosis of MS,(2)relapse-free in the previous 90 days before the tests,(3)an EDSS of≤4,and(4)the ability to stand in a tandem position and walk without an assistive an device.Additionally,participants were excluded if they needed an orthosis for stance control of the foot,ankle,and/or knee.After their recruitment,participants were stratified according to their EDSS score as minimally(EDSS of≤2)or moderately(2.5≤EDSS≤4)impaired pwMS.Experimental procedures were in accordance with the Declaration of Helsinki and were approved by the Miguel Herna´ndez University of Elche Office of Research Ethics(DPS.RRV.05.15).All participants provided informed written consent before their participation.Demographic and clinical descriptive data were derived from medical records(Table 1).
2.2.Experimental procedures
Participants completed 2 assessment sessions separated by 15 days in a biomechanics laboratory with quiet and highly illuminated conditions and a temperature ranging between-25°C and 20°C.To decrease fatigue effect on postural control and clinical tests,all participants were instructed to refrain from doing exercise 48 h before testing.
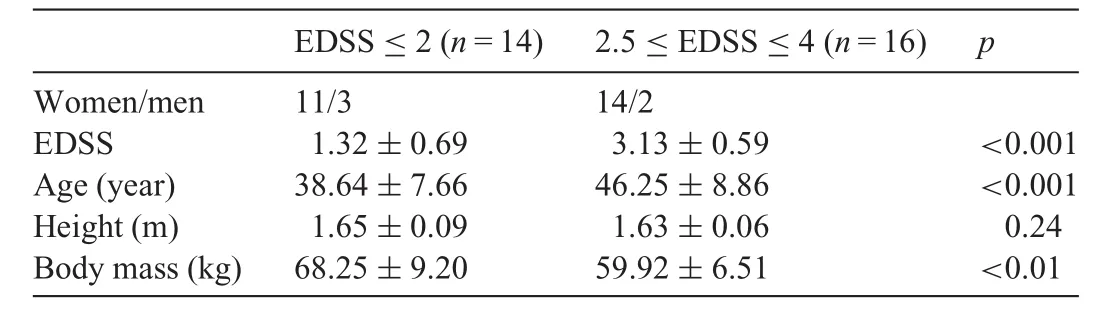
Table 1Demographic and clinical characteristics of the participants stratified according to their EDSS(mean±SD).
During the testing sessions,participants first performed the protocols to evaluate postural control in TS and sitting position.Second,they carried out the TUG and T25FW to assess the functional mobility and gait performance,respectively.
2.2.1.TS balance test
To assess the participants'ability to control their body in an upright stance,they performed the TS.A similar test has previously been proven as a valid and reliable measure to detect balance de ficits in people with vestibular disorders.35In this study,the TS consisted of an anterior-posterior movement task while standing in the tandem position on a force-platform(9286AA;Kistler,Winterthur,Switzerland),sampling at 1000 Hz.During this test,feedback related to the center of pressure(CoP)displacement was provided to the participants in real time(Fig.1).In addition,a target point was shown to the participants to assess their ability to adjust their CoP position to that point,which moved repeatedly over an anterior-posterior trajectory,taking 20 s to complete a cycle(0.05 Hz).The displacement amplitude of the target point corresponded with an inclination angle of the whole-body center of mass of 2°.The body center of mass was established as 55%of body height.36The initial position of the target point was readjusted before each trial by averaging the CoP position during a 6-s static data collection without visual feedback.Participants performed 6 trials of 70 s with 1-min rest between trials,3 trials with their right leg placed behind their left leg andvice versa.The leg order was randomized between subjects.No familiarization trials were carried out to homogenize practice time between participants.
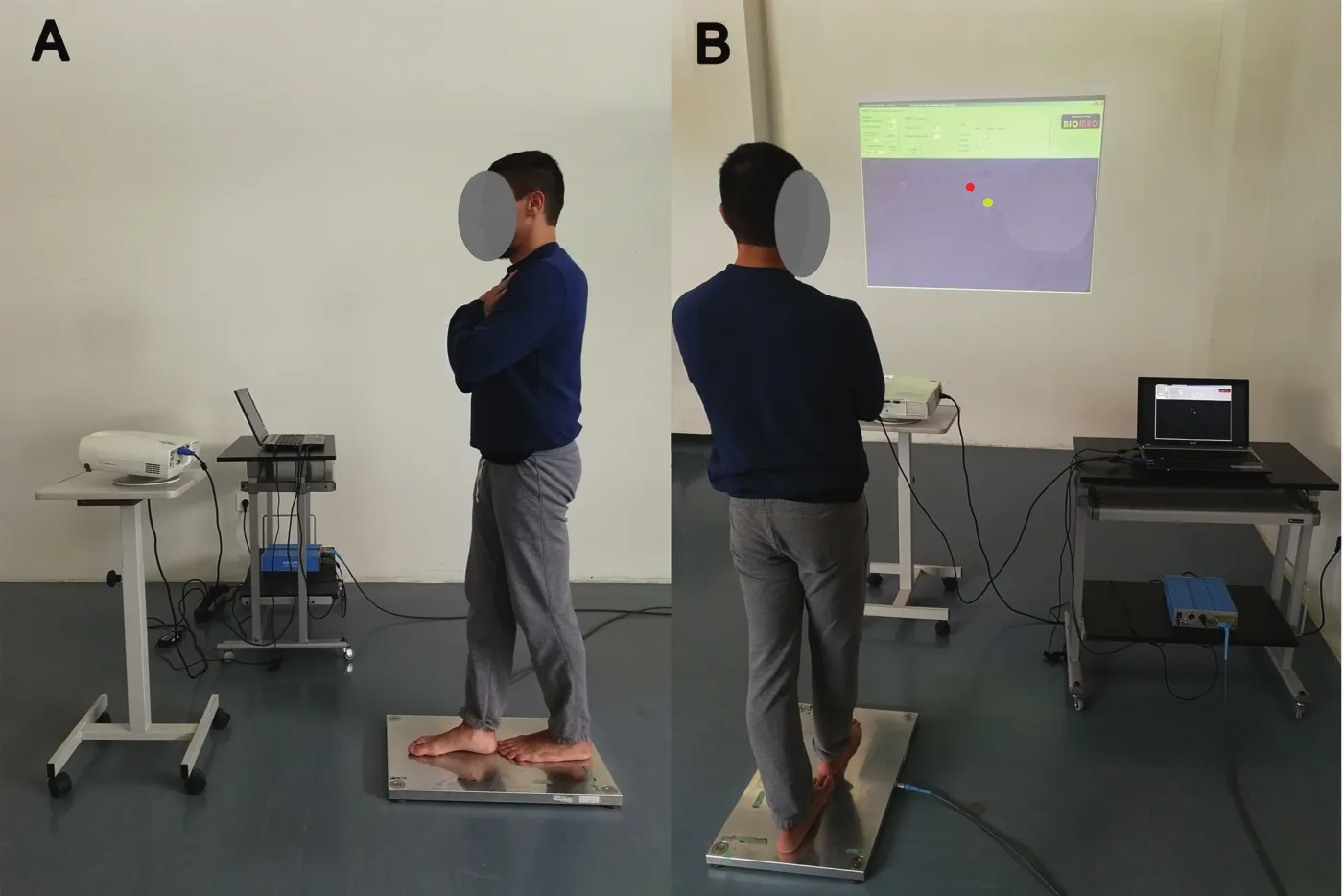
Fig.1.Lateral(A)and back view(B)of an individual performing the tandem stance balance test with visual feedback in real time(yellow dot,center of pressure;red dot,target point).
2.2.2.US balance test
Participants performed a sitting balance test29,37on an unstable seat placed on the force platform(sampling at 1000 Hz)to assess trunk postural control(Fig.2).A similar protocol has previously been used to identify trunk control de ficits in people suffering from Parkinson's disease38but,to the authors'knowledge,no study has explored the reliability of unstable sitting balance tests in people with degenerative neurologic diseases.In this study,the unstable seat was a wooden chair with a polyester-resin hemisphere(diameter=35 cm;height=12 cm)attached to its bottom.Participants were placed in the unstable seat with their arms crossed over their chest and their lower limbs strapped to the seat(90°knee flexion).Similar to the TS,the feedback of the CoP and target point displacements was provided to the participants in real time(Fig.2).They were requested to adjust their CoP to the target point,which moved repeatedly over a circular trajectory,taking 20 s to complete a cycle(0.05 Hz).The displacement amplitude of the target point corresponded with the upper-body center of mass inclination angle of 4°.The upper body center of mass was calculated as 62.6%of the distance between the greater trochanter and the acromioclavicular joint.36The target point position was readjusted before each trial by averaging the CoP position during a 6-s static data collection without visual feedback.Participants performed 5 trials of 70s with 1-min rest between trials.No familiarization trials were carried out to homogenize practice time between participants.All participants were able to maintain the sitting position without grasping a support rail placed around them to prevent participants from falling.
2.2.3.Functional mobility and gait speed
Participants carried out the TUG33and T25FW34to obtain clinical scores of their functional mobility and gait speed,respectively.Both tests have previously shown concurrent and predictor validity,33,39,40and high test-retest reliability39,40in pwMS.The TUG consisted of standing up from a chair,moving forward 3 m,turning around a cone,and sitting back down on the chair as fast as possible.Similarly,the T25FW consisted of covering a distance of 25 feet(7.62 m)in the shortest time possible.In both tests,the time(in seconds)was recorded using a digital chronometer(HS-30W-N1V;CASIO,Tokyo,Japan).Unlike previous versions of these protocols,participants were asked to perform the tests as quickly as they could,allowing them to run if they were able to,because greater neuromuscular efforts tend to decrease outcome variability(aiding in the improvement of test reliability).29Participants carried out 3 consecutive repetitions of the TUG and the T25FW with 1-min rests between trials.
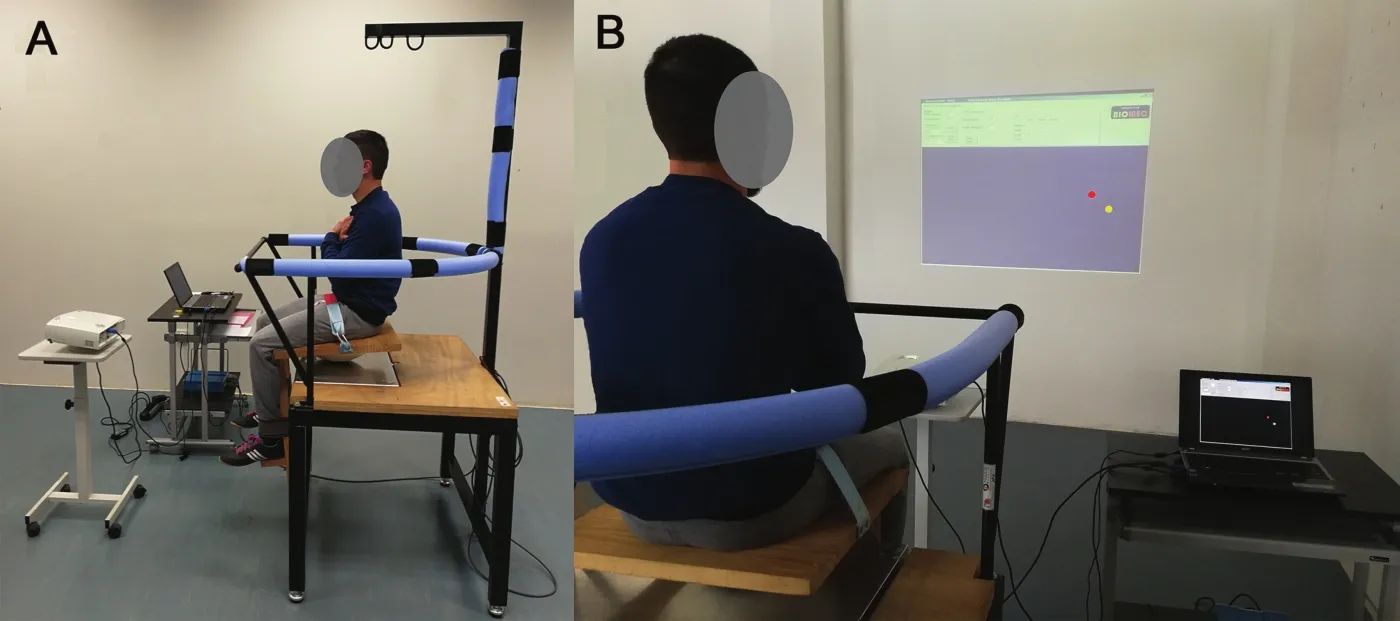
Fig.2.Lateral(A)and back view(B)of an individual performing the unstable sitting balance test with visual feedback in real time(yellow dot,center of pressure;red dot,target point).
2.3.Data reduction
For the TS and US,the CoP signal was low-pass filtered(4th order,0 phase-lag,Butterworth,5 Hz cutofffrequency)41and subsampled at 20 Hz.42The first 10 s of each 70 trial were discarded to avoid nonstationarity related to the beginning of the trial.19To quantify postural control performance while standing and sitting,the mean radial error was calculated as the average of the CoP vector distance magnitude(in millimeters)from the target point.43For the posturographic and clinical tests,the average of the 2 best trials was used for subsequent statistical analyses.
Finally,taking into account that weaker leg muscle strength in fluences walking performance in moderately impaired pwMS(2.5≤EDSS≤4)more than the stronger leg muscle strength,44TS outcomes were categorized as TS performance with the stronger leg placed behind the weaker leg(TSSL)or with the weaker leg placed behind the stronger leg(TSWL).The scores obtained by each participant in the TS during the first testing session were used to establish which leg was considered the stronger leg and which the weaker leg.Specifically,the stronger leg was defined as the leg placed behind in the TS trials in which the participant obtained her or his best scores.Conversely,the weaker leg was defined as the leg placed behind in the TS trials in which the worst scores were obtained.
2.4.Statistical analysis
Descriptive statistics(mean±SD)were calculated for all variables and groups(minimally and moderately impaired pwMS)in both sessions.The normality of the data was examined using a Kolmogorov-Smirnov statistical test.To analyze the intersession absolute reliability of each test,the standard error of measurement(SEM)was calculated45as the standard deviation of the difference between Trials 1 and 2 divided by√2.46This SEM method was selected to avoid the in fluence of sample heterogeneity and to decrease the effect of systematic error(e.g.,learning effect).47SEM values were expressed as a percentage of the mean score,which facilitates the extrapolation of the results to other individuals and the reliability comparisons with other protocols.47Although SEM is task dependent,45SEM values of<20%were considered acceptable for posturographic parameters.48The relative reliability of the different measures was analyzed using the ICC3,1,calculating 90%con fidence limits.The ICC values were categorized as follows:excellent(0.90-1.00),high(0.70-0.89),moderate(0.50-0.69),and low(<0.50).49Reliability analyses were carried out using a spreadsheet designed by Hopkins.50
One-way repeated-measures analyses of variance(ANOVA)were performed to assess the repetition effect,with session being the within-subject factor(Session 1,Session 2).Additionally,one-way repeated-measures ANOVAs were performed to assess TS balance differences between the stronger and the weaker legs in each group.Moreover,one-way independent-measuresANOVAswere performed to assess between-group differences for all variables,with group being the between-subject factor(EDSS≤2,2.5≤EDSS≤4).Hedges'gindex(dg)was used to estimate the effect size of within and between-group differences.51This index is based on Cohen'sdindex,but it provides an effect size estimation,decreasing the bias caused by small samples(n<20).Effect sizes were interpreted as trivial(dg<0.2),small(0.2≤dg<0.5),moderate(0.5≤dg<0.8),and large(dg≥0.8).52Finally,the Pearson correlation coefficient(r)was used to analyze the relationship among measurements in the whole sample.To decrease the potential in fluence of learning effect on the results,ANOVA and correlational analyses were performed using the participants'scores obtained in the second session.ANOVAs and correlational analyses were performed using SPSS(Version 22.0;IBM Corp.,Armonk,NY,USA),establishing significance atp=0.05.
Before performing the ANOVAs and correlational analyses,the sampling software package G*Power 3.153was used to calculate the minimum sample size needed to detect significant results.A sample size of 10 participants per group was found to be necessary to detect subtle within-group differences(dg=0.3)caused by learning in the test-retest reliability analysis(r=0.6;power=80%;α=0.05).For between-group comparisons,a sample size of 12 participants per group was needed to detect moderate differences between minimally and moderately impaired pwMS(dg=0.6;power=80%;α=0.05).
3.Results
As Table 2 shows,all the parameters assessed in this study showed high to excellent relative reliability(ICC≥0.80)and good absolute reliability(postural control tests,SEM≤15.33%;clinical tests,SEM≤6.56%)in both minimally and moderately impaired pwMS.Nevertheless,it should be noted that moderately impaired pwMS showed worse SEM values for TS and TUG scores(TSWL:12.84%;TSSL:15.33%;TUG:6.56%)than minimally impaired pwMS(TSWL:11.76%;TSSL:9.32%;TUG:3.43%).Regarding ANOVA results,TSWLand US showed a significant decrease(i.e.,higher postural control)from Session 1 to Session 2 in both MS groups,but the effect sizes were small(TSWL:0.37≤dg≤0.43;US:0.42≤dg≤0.44).
Concerning TS balance performance,although significant differences(p<0.05;dg=0.40)between TSWLand TSSLin the 1st session were observed,they were not maintained(p=NS)in the 2nd session.
Concerning the between-group comparison(Table 3),the minimally impaired pwMS group showed better performance in TUG,T25FW,and TSWLthan the moderately impaired pwMS group(p<0.05;-1.00≤dg≤-0.85).Nevertheless,no statistical differences were found for TSSLand US variables.
As shown in Table 4,except for the US,all parameters significantly correlated with EDSS scores significantly,mainly the TUG scores,which showed the highest correlation(r=0.69;p<0.01).Standing and sitting postural control parameters showed significant correlations with TUG scores(0.42≤r≤0.60;p<0.05);nonetheless,only TSWLcorrelated with T25FW scores(r=0.53;p<0.01).Although the US correlated with both TS parameters,the correlation was higher for TSWL(r=0.54;p<0.01)than for TSSL(r=0.43;p<0.05).
4.Discussion
The absolute and relative reliability of the TS and US were analyzed to provide clinicians and researchers with useful posturographic protocols to detect clinically relevant changes in postural control caused by the MS progression,as well as to be able to classify minimally and moderately impaired pwMS based on their postural control impairment.In addition,the potential in fluence of postural control parameters on functional mobility(TUG)and gait performance(T25FW)were assessed.
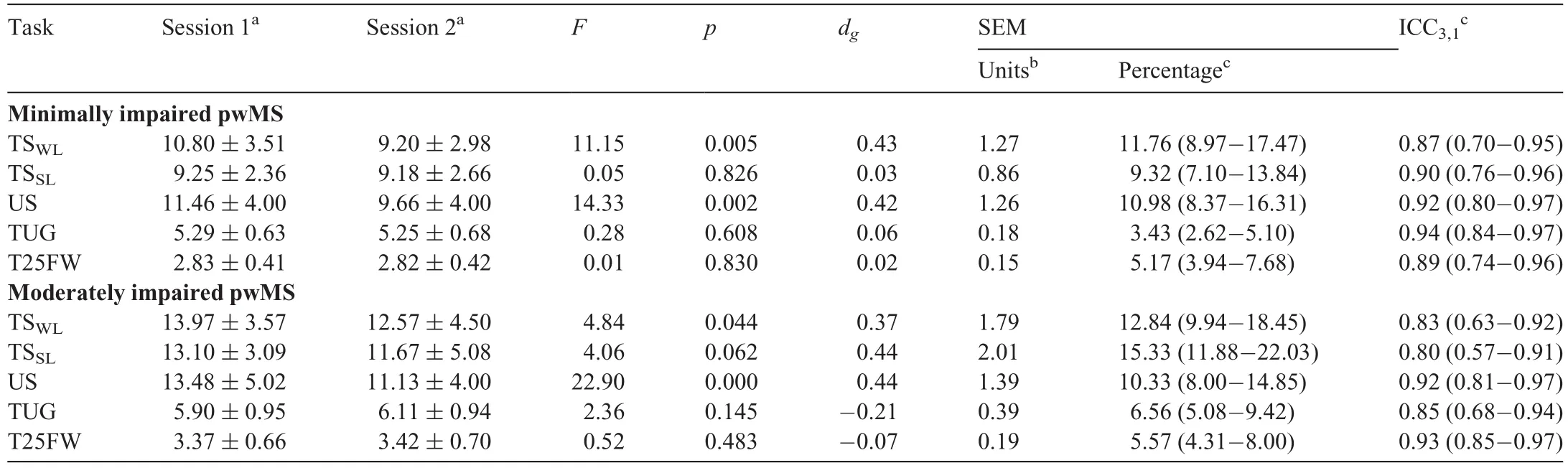
Table 2Reliability scores for the different parameters obtained from the posturographic and clinical tests in minimally(EDSS≤2;n=14)and moderately(2.5≤EDSS≤4;n=16)impaired pwMS.
4.1.Reliability of posturographic and clinical tests
Both posturographic tests showed high to excellent relative and absolute reliability in both groups,namely,minimally and moderately(Table 2)impaired pwMS.Our ICC results support previous findings that showed a high relative reliability of posturographic tests performed in standing7,16,17and in sitting positions.28In addition,our results con firmed that posturography is a consistent tool for classifying individuals with MS according to their postural control,even in homogeneous MS samples.Regarding absolute reliability,SEM values obtained in TS and US(≤15.33%)were lower than the reference value of 20%.48Consequently,these tests provide reliable parameters to identify subtle changes in postural control produced by the disease progression(variations of>1 and 2 mm in minimally and moderately impaired pwMS,respectively;see Table 2).Based on these results,posturographic protocols may play an important role in quantifying postural control deterioration and in verifying treatment effectiveness,especially in minimally impaired pwMS,who in our study showed lower session-to-session balance variability.Interestingly,these differences between MS groups con firm that patients'postural control shows higher between-day variations as the disease progresses.8,54Moreover,based on ANOVA results(Table 2),only TSWLand US scores decreased significantly between sessions,suggesting that those parameters are largely susceptible to improvement owing to learning;thus,a familiarization period seems to be necessary to decrease the learning effect.32
Regarding clinical tests,the current results(0.85≤ICC≤0.94)support previous studies that have shown that T25FW and TUG have an excellent ability to classify pwMS according to their gait speed and functional mobility,39,55-57but the ICC results obtained in our study were obtained with a more homogeneous sample.In addition,the SEM scores(3.43%≤SEM≤6.56%) were lower than those obtained in previous work,39,55-57perhaps because participants were asked to accomplish the clinical tests as fast as they could,even allowing them to run,which could decrease the within-subject variability.According to our data(Table 2),time decreases of>0.2 s for T25FW and>0.4 s for TUG should not be attributed to normal day-to-day variability in individuals with an EDSS of≤4.
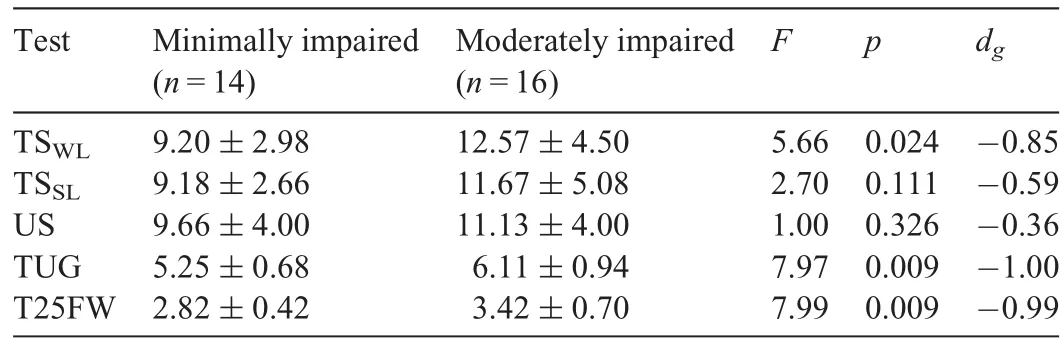
Table 3Comparison of postural control parameters and functional scores between minimally(EDSS≤2)and moderately(2.5≤EDSS≤4)impaired pwMS(mean±SD).

Table 4Pearson correlations between EDSS scores,postural control parameters,and functional scores in pwMS.
4.2.Between-group differences and correlations
Regarding between-group differences,only the TSWL,TUG,and T25FW were able to discriminate between minimally and moderately impaired pwMS(p<0.05;0.85≤dg≤1.00).The relevance of these protocols for the assessment of the degree of disability caused by MS disease progression in early disease stages was con firmed by the correlational analysis,which showed that the TUG,T25FW,and TSWLreached the highest correlations with EDSS scores(Table 4).In addition,although no significant differences were observed between TSSLand TSWL,the correlations found between the TSWLand both clinical tests support previous findings on lower limb strength,44,58,59which highlighted that the degree of impairment of the weaker leg seems to be more relevant for walking and functional mobility than the impairment of the stronger leg.However,this is a cross-sectional survey,and longitudinal studies should assess the extent to which all the analyzed parameters are affected by MS disease progression.
The correlational analysis showed a significant relationship between US and both tandem conditions(US-TSWL:r=0.54,p<0.01;US-TSSL:r=0.43,p<0.05),which supports the in fluence of trunk stability on standing postural control.In addition,US positively correlated with functional mobility(US-TUG:r=0.42,p<0.05),but it did not correlate with gait speed(US-T25FW:r=0.24,p>0.05).The authors believe that the lack of correlation between trunk control and T25FW could be related to the relatively low balance demands of walking(in a straight line)for our sample of patients with MS(EDSS≤4).Nevertheless,balance demands were higher during the TUG(i.e.,standing with a small base of support,rising,turning)and consequently trunk control could play a more important role in the performance of this test.60These results support a pilot study conducted by Freeman et al.61that analyzed the effects of a trunk stability training program on functional mobility and gait performance in pwMS.However,they do not fully agree with the results obtained by Fox et al.,62who did not observe positive effects of a trunk stability exercise program either on gait speed or on functional mobility.Although further research is needed to properly describe the relationship between trunk postural control and functional capabilities in pwMS,our results and those obtained in other populations with balance de ficits(e.g.,stroke),63suggest that trunk stability should be evaluated in clinical settings to obtain a more comprehensive knowledge of the postural control status of each patient with MS.This information may also be useful to individualize training programs that help to improve balance and performance during daily life activities in which pwMS are at risk of suffering a fall.
Finally,it must be pointed out that this study has some limitations that must be considered before applying its results to clinical settings.For instance,the sample was small,which limits the generalizability of these results.In addition,our balance assessment using a biofeedback in real time of the CoP displacement did not provide an ecological measure of pwMS postural control.Nevertheless,the authors considered these protocols valuable because(1)they improved the reliability of CoP parameters reducing the nonstationary behavior of CoP displacement,29,64and(2)they facilitated the development of more challenging and easy-to-quantify tests,in which postural control could be evaluated in dynamic conditions.Last,the dynamic tasks performed in the posturographic tests may be too difficult for patients with an EDSS of>4 to perform.Consequently,it would be necessary to modify these protocols using easier tasks for those individuals with severe forms of MS.
5.Conclusion
The results of this study provide clinicians and researchers with 2 posturographic tests to perform reliable measures of postural control in pwMS with a homogeneous disease pro file,even in minimally impaired individuals(i.e.,EDSS≤2).In addition,this study supports the consistency of T25FW and TUG for quantifying gait speed and functional mobility,respectively,even in early stages of the disease.
Based on the comparison between minimally and moderately impaired pwMS and correlationalanalysis,the impairment offunctional mobility,gait performance,and weaker leg condition are relevant symptoms to evaluate the physical activity limitation caused by the disease progression.Trunk stability,although it does not seem so affected by the course of the disease,remains relevant for postural control and functional capacity.
Acknowledgment
This study was supported by TEMPE GRUPO INDITEX,S.A.This funding source had no involvement in the design of the study;the collection,analysis and interpretation of data;the writing of the report;or the decision to submit the article for publication.
Authors’contributions
DB,RGI,and PMN designed and conducted the study,collected and analyzed the data,and drafted the manuscript;GVC collected and analyzed the data;RR and FJVG designed and conducted the study,and drafted the manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- Isokinetic trunk flexion-extension protocol to assess trunk muscle strength and endurance:Reliability,learning effect,and sex differences
- Effects of compression garments on surface EMG and physiological responses during and after distance running
- Residual force enhancement due to active muscle lengthening allows similar reductions in neuromuscular activation during position-and force-control tasks
- Health-related fitness knowledge growth in middle school years:Individual-and school-level correlates
- Habitual physical activity levels and sedentary time of children in different childcare arrangements from a nationally representative sample of Canadian preschoolers
- Walking-friendly built environments and objectively measured physical function in older adults