Development and evaluation of the Directive and Nondirective Support Scale for Patients with Type 2 Diabetes
2020-11-26XuxiZhngXingZhngFenginWngShiynWuKngHuMyinuerYusufuXinyingSunEdwinFisher
Xuxi Zhng ,Xing Zhng ,Fengin Wng ,Shiyn Wu ,Kng Hu ,Myinuer Yusufu ,Xinying Sun ,*,Edwin B.Fisher
a Department of Social Medicine and Health Education,School of Public Health,Peking University,Beijing,China
b Beijing Tongren Hospital,Capital Medical University,Beijing Tongren Eye Center,Beijing Institute of Ophthalmology,Beijing Key Laboratory of Ophthalmology and Visual Science,China
c Gillings School of Global Public Health,University of North Carolina,North Carolina,USA
Keywords:Diabetes mellitus Directive support Nondirective support Patient preference Self-management Social support
ABSTRACT Objectives:This study aims to develop the Directive and Nondirective Support Scale for Patients with Type 2 Diabetes (DNSS-T2DM) to measure diabetes-specific support and patients’ preference as well as evaluate the construct validity and reliability of the DNSS-T2DM.Methods:A cross-sectional study was conducted in Tongzhou District,Beijing,China from July to September 2015.A total of 474 participants who had been diagnosed as type 2 diabetes by physicians and completed the DNSS-T2DM were included.The original 11-item DNSS-T2DM contains five items on nondirective support (Items 1-5) and six items on directive support (Items 6-11).There were two parallel questions for each item with one to measure the preference for support(Preference part)and the other to measure the perception of support in reality (Reality part).The final DNSS-T2DM was determined based on the results of the exploratory factor analysis (EFA).The construct validity of the final DNSS-T2DM was evaluated by the confirmatory factor analysis (CFA).The reliability was evaluated by internal consistency with Cronbach’s α coefficients.Results:A final 7-item DNSS-T2DM loaded on 2 factors with four items representing nondirective support and three items representing directive support was determined based on the EFA.The CFA indicated a satisfactory construct validity.The internal consistency of the 7-item DNSS-T2DM as well as the nondirective support items was satisfactory with Cronbach’s α ≥0.70.Conclusions:Our study supported the validity and reliability of the 7-item DNSS-T2DM.Further studies on the application of the DNSS-T2DM in different settings and population are needed.
What is known?
· Social support can be classified into directive support and nondirective support.The effect of directive and nondirective support in different circumstances might be different.
· The association between high perceived diabetes-specific support and increased self-management behaviors has been reported by previous studies.
· None of the existing measurements to assess directive and nondirective support was developed for patients with diabetes specifically,so diabetes-specific support from the perspective of directive and nondirective support cannot be assessed by the existing measurements.
What is new?
· To the best of our knowledge,Directive and Nondirective Support Scale for Patients with Type 2 Diabetes(DNSS-T2DM)is the first scale designed specifically to measure directive and nondirective support from family and friends among patients with T2DM.
· All items of the DNSS-T2DM have descriptions related to diabetes management to measure the diabetes-specific support.
· The DNSS-T2DM measures not only the perception of directive and nondirective support in reality but also patients’preference.
1.Introduction
Diabetes is a chronic disease with significant morbidity and mortality,and over 90%patients with diabetes have type 2 diabetes(T2DM)[1].An essential component in the treatment of diabetes is self-management [2].One of the most effective ways to improve self-management among patients with diabetes has proved to be social support [3].
Social support encompasses one’s formal and informal support relationships with family,friends,and significant others [4].Social support can be conceptualized from different perspectives such as types,roles,effects and measurement methods [5,6].The effectiveness of social support is,to some extent,influenced by the ways in which the support is perceived and delivered[7].
Based on the ways of delivering support,social support can be classified into two approaches:directive support and nondirective support [8-12].Directive support is prescriptive and guided by rules.The provider takes the responsibility for the whole process,such as making decisions and developing tasks,and the recipient follows the instructions of the provider [11].In contrast,with nondirective support,the recipient’s thoughts and choices play an important role in the whole process.The relationship between the provider and the recipient is cooperative,with the recipient retaining responsibility for making decisions and developing tasks according to the goals [11].
Previous studies have shown positive effect of nondirective support on health behavior improvement and better management of diseases compared with directive support [7-11].A study on directive and nondirective support in diabetes management showed that nondirective support was significantly associated with better metabolic control [8].Nevertheless,there are certain circumstances in which directive support may be more effective,such as when faced with challenges that the patient has no experience dealing with [11].Therefore,it is necessary to study a patient’s preference for directive and nondirective support in different scenario so as to provide better social support.
The self-management routines of diabetes are rigorous and complex:they include blood glucose monitoring,medication or insulin-treatment adherence,physician visits,a healthy diet,and regular physical activity [4,13].The association between high perceived diabetes-specific support and increased selfmanagement behaviors has been reported by previous studies[4,14].Therefore,studies on how to provide diabetes-specific support from the perspective of directive and nondirective support could enable support providers to understand the demand of patients with diabetes better and to provide more patient-centered care.However,the existing measurements to assess directive and nondirective support,such as the Social Support Interview developed by Fisher(1997),the Inventory of Nondirective and Directive Instrumental Support (INDIS),and the Social Support Inventory(SSI) [9-12],are not developed for patients with diabetes specifically; accordingly,diabetes-specific support from the perspective of directive and nondirective support cannot be assessed by the existing measurements.
Therefore,we aim to develop a new scale,namely the Directive and Nondirective Support Scale for Patients with Type 2 Diabetes(DNSS-T2DM),to measure the diabetes-specific support and patients’ preference from the perspective of directive and nondirective support.We also aim to evaluate the construct validity and reliability of the DNSS-T2DM.
2.Materials and methods
2.1.Scale development
According to the definition that“social support can come from a variety of sources and is defined as the help one receives from family,friends,and significant others”,the authors designed DNSST2DM for the measurement of directive and nondirective support from family or friends among patients with type 2 diabetes[3].
A pool of 11 items on directive and nondirective support from family and friends (in Chinese language)were generated based on the theoretical categories of directive and nondirective support developed by Fisher et al.(1997) through structured interviews among patient with diabetes[8].Supplementary Table S1 presents the detailed categories developed by Fisher et al.(1997) through structured interviews:1) categories of nondirective support included‘Do with’,‘Help out’,‘Cooperation’,‘Information’,‘Neutral monitoring’and‘Noncontingent praise and encouragement’;and 2)categories of directive support included ‘Do for’,‘Intrusive facilitation’,‘Contingent raise’and‘Remind’.However,there were some exceptions of some categories,for example,in ‘Cooperation’,“if avoiding tempting the recipient or protecting from stress is too indulgent,however,this may be scored as Intrusive Facilitation”,and in ‘Neutral monitoring’,“keeping track to nag or in a ‘smothering’manner would be Intrusive Facilitation”.Combined with the key elements in diabetes management as well as the theoretical categories of nondirective and directive support mentioned above,we developed the current scale within a Chinese frame of reference.An expert panel consisting of 5 specialists in the field of health promotion and health education from Peking University comprehensively reviewed the primary draft to evaluate the content validity of items.The 11-item DNSS-T2DM was then checked and revised according to recommendations of the specialists.
In the 11-item DNSS-T2DM,Items 1-5 represented nondirective support,including 1)“Do what I should do to manage my diabetes with me (e.g.management of diet together and do exercises together)”,2)“Help me when I am in a situation that I cannot deal with by myself (e.g.give me sugar during hypoglycemia)”,3)“Provide information or suggestion on diabetes”,4)“Supervise my management of diabetes in a nonintrusive way”and 5)“Encourage me without implying insufficient performance (e.g.saying ‘Well done’ or ‘You did a great job’ to encourage me)”.Items 6-11 presented directive support,including 6) “Do what I should do to manage my diabetes (e.g.prepare dishes for me,make insulin injection for me and record examination results for me)”,7)“Ask me to do what I should do instead of doing these things together with me”,8) “Tell me what I should do to manage my diabetes”,9)“Supervise my management of diabetes in an intrusive way”,10)“Encourage me with implying insufficient performance (e.g.encourage me to do more exercise)” and 11) “Remind me to do what I should do (e.g.remind me to monitor blood glucose everyday)”.
Moreover,there were two parallel questions for each item.One question asking “how much do you like such kind of support?” to measure the preference for support(Preference part),and the other asking “how often do you get such kind of support in your daily life?”to measure the perception of support in reality(Reality part).Both questions of each item were assessed with five-point Likert scoring system with score range of 1-5 respectively (Preference part:1=Not at all,2=A little,3=Somewhat,4=Almost very much,5=Very much; Reality part:1=Never,2=Occasionally,3=Sometimes,4=Frequently,5=Always).In Preference part,a score of directive/nondirective support can be determined by adding up the items of the directive/nondirective subdomain,with higher scores representing a higher level of preference.Similarly,in Reality part,a score of directive/nondirective support can be determined by adding up the items of the directive/nondirective subdomain,with higher scores representing a higher level of support perceived in reality.
2.2.Design,participants and procedures of the study
The Community Diagnosis in Tongzhou District of Beijing(CDTB)project,a cross-sectional study,was conducted in Tongzhou District,Beijing,China between July and September 2015.Probability proportional to size (PPS) sampling and proportional quota sampling were adopted to select residents aged 18 years or older in Tongzhou District according to demographic characteristics such as age and gender.Residents were not eligible to participate if they are diagnosed with mild or serious cognitive impairment or were not able to make an informed decision regarding participation in the study.A total of 7000 residents,5‰ of the total population in Tongzhou District of Beijing,were enrolled in the study.The data collection was done by means of a questionnaire,physical examinations and biochemical tests.Investigators who have received standard training conducted face-to-face survey on each patient enrolled in this study.Health professionals conducted physical examinations and biochemical tests with uniform standard.This study was approved by Peking University Institutional Review Board,approval No.IRB00001052-15041.Written informed consent was obtained from all participants.
The current study included participants in the CDTB project who had been diagnosed as T2DM by physicians and completed the DNSS-T2DM in the analyses (N=474).
2.3.Measures of characteristics of participants
Age was categorized into four groups(≤49 years;50-59 years;60-69 years; ≥70 years).Education level was measured by asking the highest level of education completed and was categorized into three categories:primary or less,secondary or equivalent and tertiary or higher.Disease duration was categorized into two groups(≤5 years; >5 years).Body mass index (BMI)was calculated based on weight and height and was categorized into three groups including 18.5 kg/m2≤BMI < 24.0 kg/m2(normal),24.0 kg/m2≤ BMI < 27.0 kg/m2(overweight),and BMI ≥27.0 kg/m2(obesity).Glycated hemoglobin(HbA1c)were categorized into two groups (<7.0%,≥7.0%) based on Standards of Medical Care in Diabetes,a reasonable HbA1c goal for non-pregnant adults is <7.0%[15].
2.4.Statistical analyses
The exploratory factor analysis (EFA) was adopted to evaluate the construct validity of the original 11-item DNSS-T2DM and determine the final version of DNSS-T2DM.The confirmatory factor analysis(CFA)was adopted to evaluate the construct validity of the final version of DNSS-T2DM.
Univariate tests of normality were conducted with the Kolmogorov-Smirnov test (P < 0.05) and the Shapiro-Wilk test(P<0.05),which revealed that the distribution of the data was nonnormal.Therefore,we chose the Unweighted Least Squares(ULS)as the factor extraction method in the EFA[16].We chose the Varimax solution as the rotation method in the EFA of current study because:1)rotations are performed for a better interpretation and always have an equal mathematical quality regardless of solution type[17,18];2)the Varimax solution produced the clearest defined factor structure in current study [18]; and 3) the judgement and decision on reliability and validity of the researcher are crucial throughout the study on the development of a new instrument[18,19].The Kaiser-Meyer-Olkin (KMO) and Bartletts’s Test of Sphericity were used to assess the appropriateness of sample for the EFA.The number of factors was determined based on eigenvalues above 1 and scree plot.Items were removed if they did not load on either factor at or above 0.30,or they cross-loaded with a difference in loadings less than 0.10 [3,9].Furthermore,we designed Items 1-5 as the nondirective support and Items 6-11 as the directive support according to the concepts and theoretical categories of directive and nondirective support,which were our theory hypothesis.If the items conflicted with the theory hypothesis (loaded in a factor category different from its original design),then it would be excluded.For example,if one item was designed as directive support but it loaded on a factor that covered most nondirective support items,then this item would be excluded.
In the CFA,fit indices including relative Chi-square (χ2/df),Comparative Fit Index (CFI),Non-Normed Fix Index (NNFI/TLI),Root Mean Square Error of Approximation (RMSEA),and Standardized Root Mean Square Residual (SRMA) were used to assess the fitness of a model.It was recommended that the value of Chisquare of less than 3 could represent an acceptable fitness [3,20].The value of the CFI and the NNFI/TLI could range from 0 to 1,and values closer to 1 could indicate better fitness[3,21].A value of the RMSEA between 0.08 and 0.10 could reveal an acceptable fitness and below 0.08 could reveal a good fitness [3,22].A value of the SRMR between 0.05 and 0.08 could reveal an acceptable fitness and below 0.05 could reveal a good fitness [23].Four fit indices with good or acceptable fitness out of the five mentioned above could reveal a good fitness of a model,which indicated a satisfactory construct validity.
Scale scores of the final version DNSS-T2DM were described by conventional descriptive statistics [24].
The internal consistency was adopted to evaluate the reliability of the final version of DNSS-T2DM with Cronbach’s α coefficient.A value of Cronbach’s α between 0.7 and 0.9 was considered as a satisfactory internal consistency [25,26].
Analyses were performed with SPSS version 19.0 and Mplus version 7.0.Participants enrolled in current study were divided into two samples randomly with SPSS.The EFA was performed in EFA sample(N=234)with SPSS,and the CFA was performed in the CFA sample (N=240) with Mplus.Conventional descriptive statistics and analyses of the internal consistency were performed with SPSS in the total sample (N=474).A P-value <0.05 was considered as statistically significant.
3.Results
3.1.Participants
Table 1 shows the general characteristics of the study population and the comparison between the EFA sample and the CFA sample.The mean age of the participants (N=474) was 57.5 (SD 12.1) years,and 56.1% (266/474) were female.No statistically significant differences between the EFA sample(N=234)and the CFA sample (N=240) were found.
3.2.Exploratory factor analysis (EFA)
Table 2 shows the EFA of the two parallel parts of the original 11-item DNSS-T2DM as well as the 7-item DNSS-T2DM conducted in the EFA sample (N=234).
Regarding the original 11-item DNSS-T2DM,the values of KMO(0.86 for the Preference part and 0.85 for the Reality part; both >0.6) and the Bartletts’s Test of Sphericity (P < 0.001 for both)revealed the sampling adequacy for the EFA.A 2-factor structure with seven items in factor 1 and four items in factor 2 in two parallel parts was indicated respectively,which explained 55.72% of variance in the Preference part and 52.13%of variance in the Reality part.However,items conflicted with the theory hypothesis were removed.According to the theory hypothesis,three items (Item 6,Item 10 and Item 11)in factor 1 of both the Preference part and the Reality part were irrelevant to another four items (Item 1,Item 2,Item 3 and Item 5),so they were removed.Item 4 in factor 2 of both the Preference part and the Reality part was irrelevant to another three items(Item 7,Item 8 and Item 9),so it was removed.Finally,we determined the 7-item version of the DNSS-T2DM.
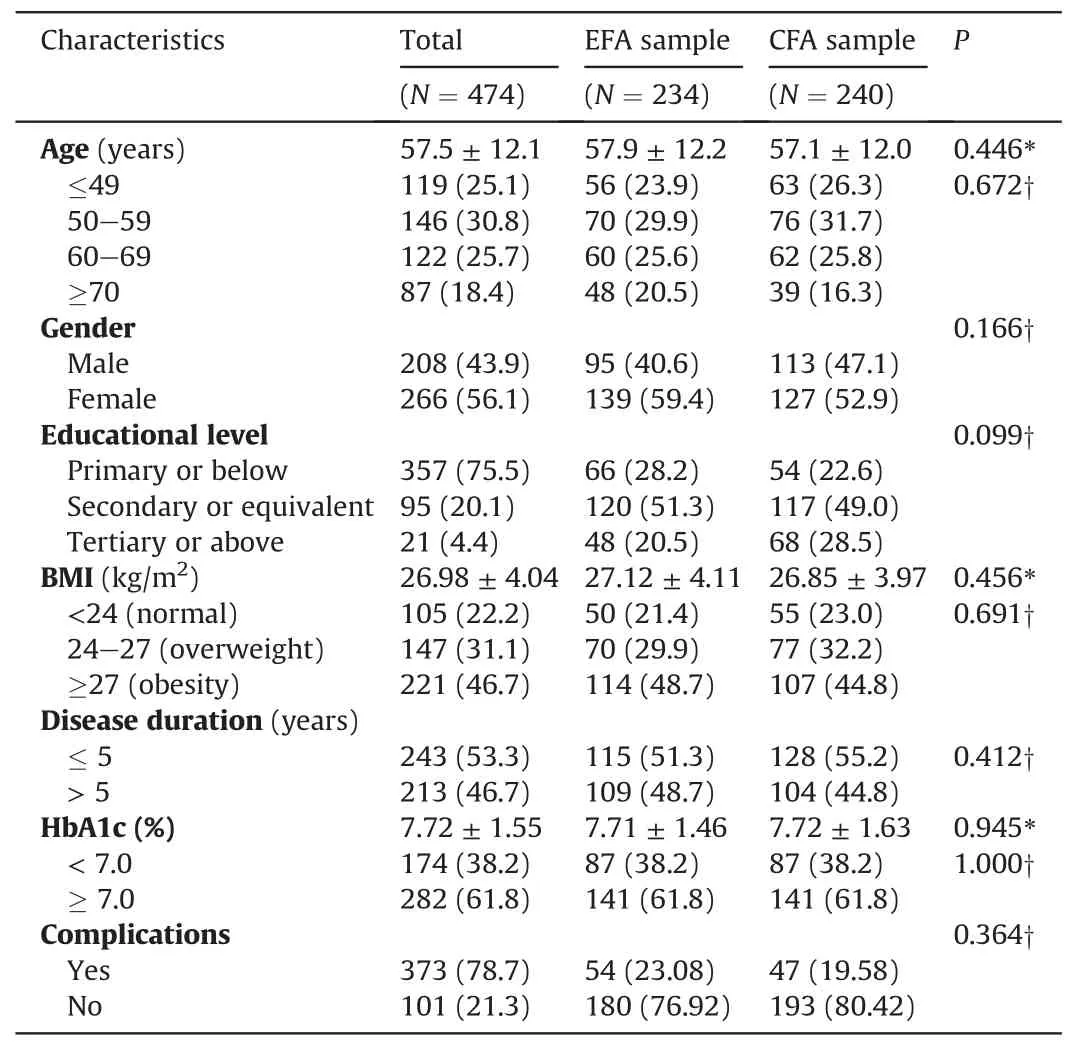
Table 1 Characteristics of the participants.
Regarding the 7-item DNSS-T2DM,the values of KMO (> 0.6)and the Bartletts’s Test of Sphericity (P < 0.001) revealed the sampling adequacy for the EFA.A 2-factor structure in two parallel parts was indicated respectively,which explained 61.86% of variance in the Preference part and 57.70% of variance in the Reality part.However,in the Reality part,Item 5 and Item 7 cross-loaded on two factors with a difference in loadings less than 0.10.We kept Item 5 in factor 1 and Item 7 in factor 2 based on our theory hypothesis,and we conducted the CFA to evaluate the construct validity of the 7-item DNSS-T2DM.
3.3.Confirmatory factor analysis (CFA)
Fig.1 shows the CFA on the Preference part of the 7-item DNSST2DM conducted in the CFA sample (N=240).The relative Chisquare (χ2/df) was 38.95 (P < 0.001),the CFI was 0.93,the NNFI/TLI was 0.89,the RMSEA was 0.09 (90%CI=0.06,0.13),and the SRMR was 0.05.The values of the CFI and the NNFI/TLI revealed a good fitness.The values of the RMSEA and the SRMR revealed an acceptable fitness.Therefore,four indices out of the five revealed a good or acceptable fitness,which indicated a good fitness of the Preference part and a satisfactory construct validity.
Fig.2 shows the CFA on the Reality part of the 7-item DNSST2DM conducted in the CFA sample (N=240).The relative Chi-square(χ2/df)was 39.18(P<0.001),the CFI was 0.93,the NNFI/TLI was 0.89,the RMSEA was 0.09 (90%CI=0.06,0.13),and the SRMR was 0.05.The values of the CFI and the NNFI/TLI revealed a good fitness.The values of the RMSEA and the SRMR revealed an acceptable fitness.The values of the CFI and the NNFI/TLI revealed a good fitness.The values of the RMSEA and the SRMR revealed an acceptable fitness.Therefore,four indices out of the five revealed a good or acceptable fitness,which indicated a good fitness of the Reality part and a satisfactory construct validity.
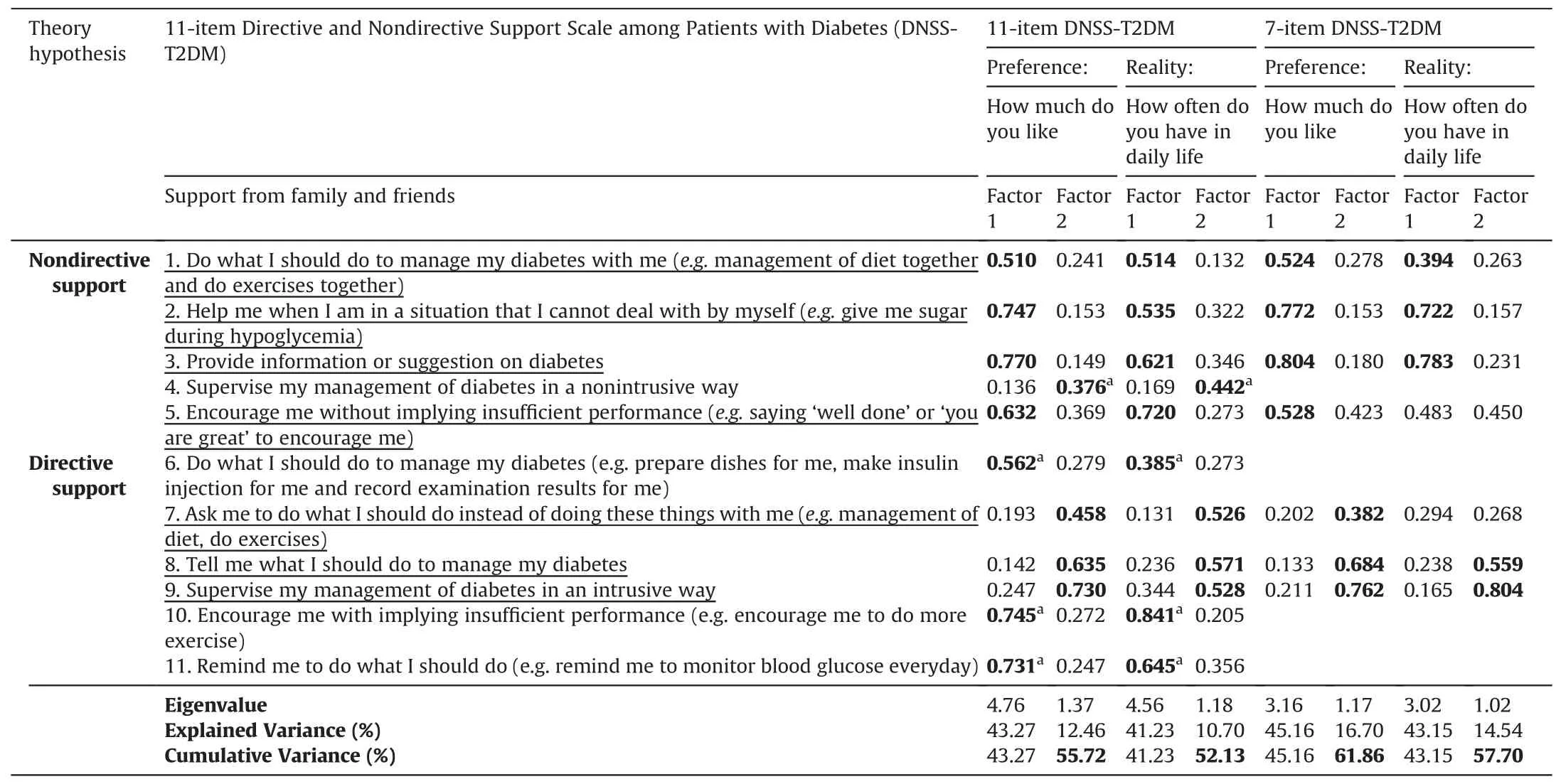
Table 2 Factors loading of the Directive and Nondirective Support Scale among Patients with Type 2 Diabetes(DNSS-T2DM) based on the exploratory factor analysis (N=234).
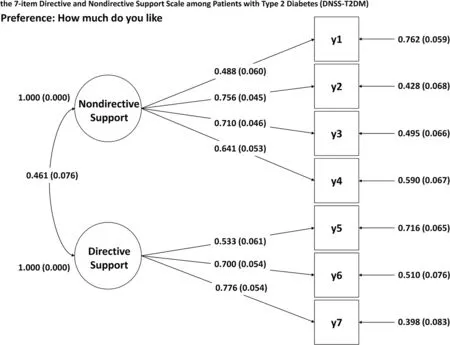
Fig.1.Two-factor models obtained from the confirmatory factor analysis(CFA)on the Preference part of the 7-item Directive and Nondirective Support Scale among Patients with Type 2 Diabetes (DNSS-T2DM) (N=240).
Supplementary Table S2 shows the 7-item DNSS-T2DM in both Chinese and English with Items 1-4 representing nondirective support and Items 5-7 representing directive support.
3.4.Score distribution
Table 3 shows the score distributions of the 7-item DNSS-T2DM in the total sample (N=474).No floor effect (>20% of the respondents had the lowest possible score [27]) or celling effect(>20%of the respondents had the highest possible score[27])was observed.
3.5.Internal consistency
Table 3 shows the internal consistency of the 7-item DNSST2DM in the total sample (N=474).The Cronbach’s α coefficient of the nondirective support(Items 1-4)was 0.76 for the Preference part and 0.75 for the Reality part.The Cronbach’s α of the directive support (Items 5-7) was 0.51 for the Preference part and 0.48 for the Reality part.The Cronbach’s α coefficient of the full 7-item DNSS-T2DM was 0.74 for both the Preference part and the Reality part.
4.Discussion
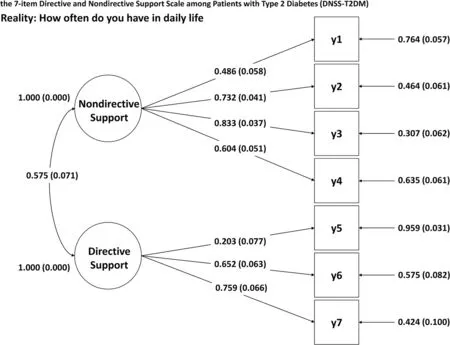
Fig.2.Two-factor models obtained from the confirmatory factor analysis(CFA)on the Reality part of the 7-item Directive and Nondirective Support Scale among Patients with Type 2 Diabetes (DNSS-T2DM) (N=240).

Table 3 Score distributions and internal consistency of the 7-item Directive and Nondirective Support Scale among Patients with Type 2 Diabetes (DNSS-T2DM) (N=474).
In summary,we developed an original 11-item DNSS-T2DM which contains five items on nondirective support (Items 1-5)and six items on directive support (Items 6-11).There were two parallel questions for each item with one to measure the preference for support (Preference part) and the other to measure the perception of support in reality (Reality part).The final 7-item DNSS-T2DM with four items (Items 1-3 and 5 of the 11-item DNSS-T2DM) representing nondirective support and three items(Items 7-9 of the 11-item DNSS-T2DM) representing directive support was determined based on the EFA.The construct validity of the 7-item DNSS-T2DM was evaluated by the CFA.The reliability of the 7-item DNSS-T2DM was evaluated by internal consistency with Cronbach’s α coefficient.
The construct validity of both the Preference part and the Reality part of the 7-item DNSS-T2DM was supported by the CFA results,which indicates a good distinction between nondirective support and directive support of the DNSS-T2DM.However,since this is the first time that the 7-item DNSS-T2DM has been evaluated,more studies on the validity of the DNSS-T2DM are needed to confirm our findings.
Regarding the full 7-item DNSS-T2DM as well as the nondirective support items(four items),the reliability was satisfactory with an internal consistency of Cronbach’s α coefficient ≥0.70 for both the Preference part and the Reality part.However,regarding the directive support items(three items),the internal consistency was not satisfactory with Cronbach’s α coefficient of 0.51 for the Preference part and 0.48 for the Reality part.The Cronbach’s α increases with the number of items[26].The low internal consistency of the directive support items might be due to the small number of items.A total of three items originally designed as directive support were removed due to the conflicts with the theory hypothesis based on the EFA results.Since all the original 11 items of the DNSS-T2DM were developed based on previous studies among the American population,the understanding of directive and nondirective support might be different in our study population because of the cultural differences.Therefore,we need to pay attention to sociocultural differences in the interpretation of individual items.Moreover,cultural adaptation of directive support items could be conducted in further studies through cognitive interview,and adding items of directive support might be beneficial to improve the internal consistency.
Social support may play an important role in nursing for patients with diabetes.During the process of nursing,better understanding patients’ need and preference of directive and nondirective support approach may help people who provide support to offer more appropriate health education and care.The Preference part in the DNSS-T2DM plays an instructive role in further studies on patients’ preference to find better supportive way for patients with different characteristics,and more studies in this field are needed.In particular,studies related to the effect of directive and nondirective support on important elements of diabetes control,such as self-management,glucose control and weight loss,could be conducted by applying the DNSS-T2DM.Moreover,exploration on how patients’preference may influence the effect of directive and nondirective support on changes of health behaviors could also be an important and interesting study direction for the application of the DNSS-T2DM in the future.
Strengths and limitations
To the best of our knowledge,the DNSS-T2DM is the first scale designed specifically to measure directive and nondirective support from family and friends among patients with T2DM.All items of the DNSS-T2DM have descriptions related to diabetes management to measure the diabetes-specific support.In addition,the DNSS-T2DM measures not only the perception of directive and nondirective support in reality but also patients’ preference.
However,this study also has some limitations.Firstly,we did not evaluate the test-retest reliability of the DNSS-T2DM with a subsample due to the limitation of time and funding.Secondly,regarding the content validity,expert panel assessment was adopted without scoring each item quantitatively.We suggest more studies to measure the content validity to confirm our findings.Thirdly,although we paid specific attention to developing the items within a Chinese frame of reference,the categories of directive and nondirective support were developed based on previous studies among the American population.Therefore,there might be sociocultural differences in the interpretation of individual items of directive and nondirective support.Further studies on the cultural adaption of the items through cognitive interview,especially the directive support items,are needed.In addition,we suggest a pilot test of the DNSS-T2DM before applying to a large population.Finally,we conducted the current study in primary care and community settings in a Chinese population,and further studies on the application of the DNSS-T2DM in other settings such as hospitals as well as in other countries are needed.
5.Conclusion
Our study supported the reliability and validity of the 7-item DNSS-T2DM.The 7-item DNSS-T2DM could be utilized to study social support from the perspective of directive and nondirective support.The application of DNSS-T2DM in measuring patients’preference for and corresponding reality of directive and nondirective support may facilitate the delivery of better personalized education and support for patients with T2DM.Furthermore,there should be more studies on the DNSS-T2DM to confirm our findings,and further studies on the application of the DNSS-T2DM in different settings and countries are needed.
CRediT authorship contribution statement
Xuxi Zhang:Conceptualization,Methodology,Formal analysis,Writing -Original Draft.Xing Zhang:Methodology,Validation,Formal analysis.Fengbin Wang:Methodology,Validation,Data curation.Shiyan Wu:Methodology,Validation,Data curation.Kang Hu.Methodology,Validation,Software.Mayinuer Yusufu:Methodology,Writing -Review & Editing.Xinying Sun:Supervision,Conceptualization,Methodology,Writing-Review&Editing.Edwin B.Fisher:Conceptualization,Writing -Review & Editing.
Funding
This research was supported by National Natural Science Foundation of China.The Grant No.is 71673009.
Declaration of competing interest
The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
Appendices.Supplementary data
Supplementary data to this article can be found online at https://doi.org/10.1016/j.ijnss.2020.09.007.
杂志排行

International Journal of Nursing Sciences的其它文章
- An exploration of the breastfeeding behaviors of women after cesarean section:A qualitative study
- The risk factors of postpartum urinary retention after vaginal delivery:A systematic review
- Demands of experiential training for ICU nurses in Hunan of China
- Understanding autism spectrum disorder and coping mechanism by parents:An explorative study
- Association of swallowing problems with frailty in Chinese hospitalized older patients
- Theory-guided interventions for Chinese patients to adapt to heart failure:A quasi-experimental study