Correlation between scapulohumeral periarthritis and cervical spondylotic radiculopathy
2020-11-16XiaoliWangJunshengYangGuanghuiMaKuiliYingTan
Xiaoli Wang , Junsheng Yang, Guanghui Ma , Kui li , Ying Tan
1 Department of Pathology, Puyang City People’s Hospital, Puyang 457000, Henan Province, China
2 Department of Rehabilitation Medicine, Pudong New Area People’s Hospital,Shanghai 201200 , China
3 Department of Rehabilitation Medicine, Shaanxi Provincial People’s Hospital, Xi’an 710068, Shaanxi Province, China
4 Bone and Joint Rehabilitation Ward, Guangdong Work Injury Rehabilitation Hospital, Guangzhou 510440, Guangdong Province, China
5 Department of Rehabilitation Medicine, Mianyang Hospital of Traditional Chinese Medicine,Mianyang 621000, Sichuan Province, China
Abstract
Key words: scapulohumeral periarthritis; cervical spondylosis; correlation
Introduction
Scapulohumeral periarthritis, abbreviated as periarthritis,refers to the symptom group with shoulder pain and limited shoulder movement as the main clinical manifestations[1-2]. Due to the onset of shoulder periarthritis around 50 years old, it is called “fifty shoulders” in field of traditional Chinese medicine.According to the 2014 ISAKOS Upper Limb Committee consensus[3], it defines unexplained shoulder pain as periarthritis or primary frozen shoulder; Periarthritis of the shoulder is caused by a variety of reasons. It is an adhesive shoulder cystitis that is clinically characterized by shoulder pain, limited movement, narrowing of the joint cavity and mild osteoporosis. The incidence of shoulder periarthritis accounts for 2%-5%[4]of the total population,and it gradually increases and becomes younger[5].Periarthritis occurs in the age of 40-65 years, with a peak incidence of 51-55 years on average. The incidence is slightly higher in women than in men[6]. It is more prevalent on the left shoulder and often occurs on one side as the initial symptoms, and 14% of cases are affected simultaneously on both sides[7-8].
At present, the etiology of periarthritis of the shoulder remains unclear, and clinical treatment is mostly symptomatic, and the effect is not satisfactory. Moreover,other types of periarthritis of the shoulder are easily misdiagnosed as simple periarthritis of the shoulder, and treatment on the shoulders alone results in poor efficacy or delays the timing of treatment. Therefore, further exploring the etiology of periarthritis of the shoulder has important diagnostic significance, and provides some guidance for the diagnosis and treatment of this disease.
Many scholars[9]have discovered that most patients with periarthritis have a previous history of cervical spondylosis,and believe that the main cause of periarthritis is cervical spondylosis. Some experts and scholars[10-11]demonstrate that, when cervical spondylosis compresses the shoulderrelated nerve roots, causing it to be stimulated and stretched, it causes spasm and pain in the soft tissue around the shoulder, pain during the movement of the shoulder joint, which reduces its movement or even no movement. Over time, disuse atrophy occurs, eventually leading to the occurrence of periarthritis of the shoulder.Some scholars have found that treating neck and shoulder together during the treatment of periarthritis of the shoulder can often achieve better results. However, some patients with periarthritis may not suffer from cervical spondylosis, so it is necessary to determine the presence of cervical spondylosis during clinical diagnosis and treatment. Therefore, further research is needed to verify the relationship between the occurrence of periarthritis of the shoulder and cervical spondylosis, to provide a certain basis for clinical treatment of cervical and shoulder, and to improve the curative effect of periarthritis, especially cervical periarthritis.
The team led by Director Yang Junsheng of the Department of Rehabilitation Medicine of Shaanxi Provincial People’s Hospital has been devoted to the traditional Chinese medicine research of fifty shoulders for many years. Based on years of clinical experience and previous research, it is concluded that the fifty shoulders were the result of resonance caused by changes in hormone levels on the basis of cervical spondylosis in the case of long-term strain.
In this study, we aim to explore the correlation of scapulohumeral periarthritis with cervical spondylopathy(especially cervical spondylotic radiculopathy, CSR)by analyzing cervical spine image data of patients with periarthritis. After the relationship between periarthritis and CSR is clearly defined, the relationship between cervical spine imaging and the laterality of periarthritis can be clinically examined to determine whether patients with periarthritis need to undergo related cervical spine treatment (such as traction) at the same time, thereby improving the symptomatic treatment of periarthritis of the shoulder, shortening the course of treatment,and improving the curative effect. Meanwhile, it is also possible to avoid misdiagnosing cervical periarthritis of the shoulder as simple periarthritis of the shoulder, and to fundamentally treat the cause of the disease and achieve better results.
Materials and Methods
Diagnostic criteria
The diagnostic criteria of periarthritis of the shoulder refer to the main points of the diagnosis of periarthritis of the shoulder mentioned in the chapter of Rehabilitation of Periarthritis of the Shoulder, in the current 5thEdition of Rehabilitation Medicine published by People’s Medical Publishing House[12]. The diagnostic criteria for CSR refer to the expert consensus for the standardization of diagnosis and treatment of CSR[13]. Positive criteria: (1)X-ray film of cervical spine: lateral film showing C3-5 narrowing of cervical spine space, double oblique films show that the side of the C3-5 intervertebral foramen becomes smaller or the side of the smallest intervertebral foramen is the same as the side where periarthritis occurs; (2) CT and MRI of the cervical spine: the C3-5 plane intervertebral disc on the affected side bulges and herniates, with prominent nerve root compression signs, and the bulge and protrusion are the same as the periarthritis side; comprehensive positive is defined as one that meets one of the above criteria.
Inclusion and exclusion criteria
Inclusion criteria: (1) Case group: Patients meet the diagnostic criteria for periarthritis of the shoulder and unilateral periarthritis of the shoulder; age ≥18 years old; those who are willing to participate in this study.(2) Control group: Patients with no symptoms such as shoulder pain and limited shoulder joint movement, which do not meet the diagnostic criteria for periarthritis of the shoulder; age ≥18 years old; those who are recruited during the same period as the case group, are within ± 2.5 years of age, of the same gender, and 1:1 matched normal people; those who are willing to participate in the study.
Exclusion criteria: Patients aging <18 years; those with periarthritis on both sides; those with a history of shoulder trauma or internal fixation of the shoulder joint; those with a history of cardiovascular and cerebrovascular disease, or history of diabetes, malignancy, autoimmunity,or hematological system; those with poor compliance or those with mental illness who cannot cooperate.
General information
This study was approved by the hospital’s ethics committee,and the patient’s consent was obtained.
From March 2018 to February 2019, 87 patients with periarthritis who were admitted to the Outpatient Department of Rehabilitation Medicine of Shaanxi Provincial People’s Hospital with the complains of shoulder pain and limited shoulder movement, and met the inclusion and exclusion criteria were included as case groups; 87 relatively normal people who were treated during the same period were selected as the control group,they had no symptoms of shoulder pain and limited shoulder movement, were within ± 2.5 years of age, of the same gender, and at a 1: 1 ratio to the case group.
Statistical analysis
The data was processed using SPSS 19.0 software. The age results were expressed as±Sand analyzed by thettest.The results of gender, periarthritis, and disease duration were expressed as percentages. For the analysis of the relationship between the groups and the variables within the group, thex2test was used,P<0.05 is considered statistically significant. When the difference is statistically significant, rank correlation analysis is performed to determine whether it is positive or negative correlation and the strength of its correlation.
Results
According to the inclusion and exclusion criteria, 87 cases were included in the case group and another 87 cases in the control group, totally 174 cases. There were no shedding cases or excluded cases, and the results of data collection and statistical analysis were listed as follows.
Results of general information

Table 1 Results of gender analysis in two groups

Figure 1 Gender analysis
The descriptive statistics of gender (Figure 1) showed that, both the case group and the control group were 69% female and 31% male. The results ofx2test of the gender in the case group (Table 1) showed that there were more women than men suffering from periarthritis (x2= 1.521,P= 0.217> 0.05).
Table 2 Results of age analysis in case group (n=87) and control group (n=87)
A single samplet-test analysis of the age in the two groups(Table 2) showed that, the average age of the control group(=51.78 years old) is equal to the age of high incidence(=50 years old) (t=1.573,P=0.119>0.05, 95% confidence interval: 0.47-4.03).

Figure 2 The laterality of periarthritis
Table 3 Results of incidence analysis of periarthritis of the shoulder in case group (n=87)
Descriptive statistics of the laterality of periarthritis of the shoulder (Figure 2) showed that, the left side accounted for 49.4% and the right side accounted for 50.6%. Results of chi-square test (Table 3) showed that the incidence of periarthritis on the left and right sides in the case group was basically the same (x2= 0.011,P=0.915>0.05).
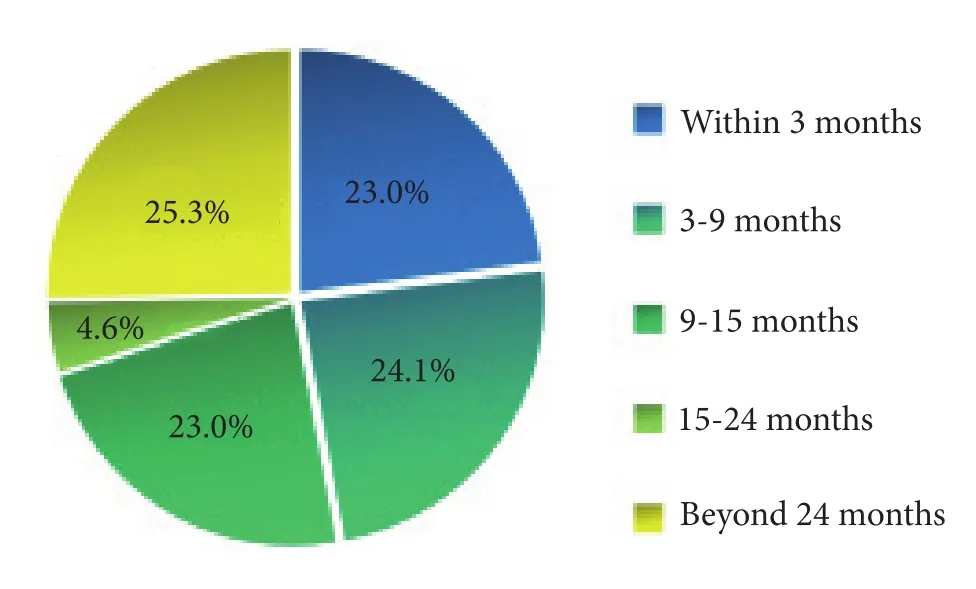
Figure 3 The course of periarthritis
The descriptive statistics of the course of the patients in the case group (Figure 3) showed that, the duration of treatment of patients with periarthritis of the shoulder ranged from 1 week to 10 years, 23.0% within 3 months,24.1% from 3 to 9 months, 23.0% from 9 to 15 months,4.6% from 15 to 24 months, and 25.3% beyond 24 months.
Comparison of the incidence of nerve root cervical spondylosis between the case group and the control group
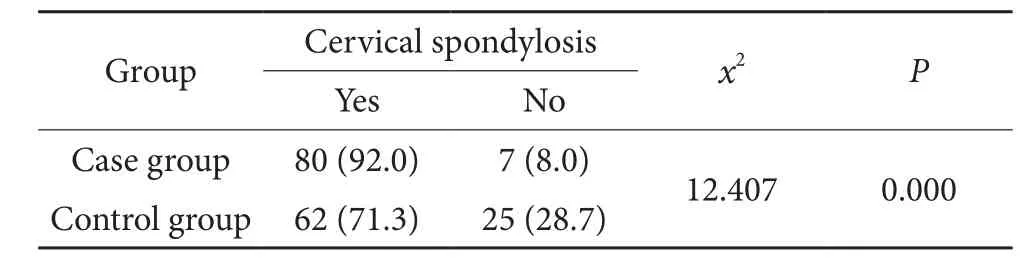
Table 4 x2 test results between the case group and the control group (n=174)
The effect of periarthritis on the incidence of CSR was analyzed by usingx2test of homogeneity (Table 4), and results showed that the difference in the incidence of CSR between the case group and the control group was statistically significant (x2=12.407,P=0.000<0.05),indicating that the incidence of CSR in the two groups was different, and the incidence of cervical spondylosis in the case group (92.0%) was significantly higher than that in the control group (71.3%).
Results of the relationship between the occurrence of periarthritis and the occurrence of radiculopathy
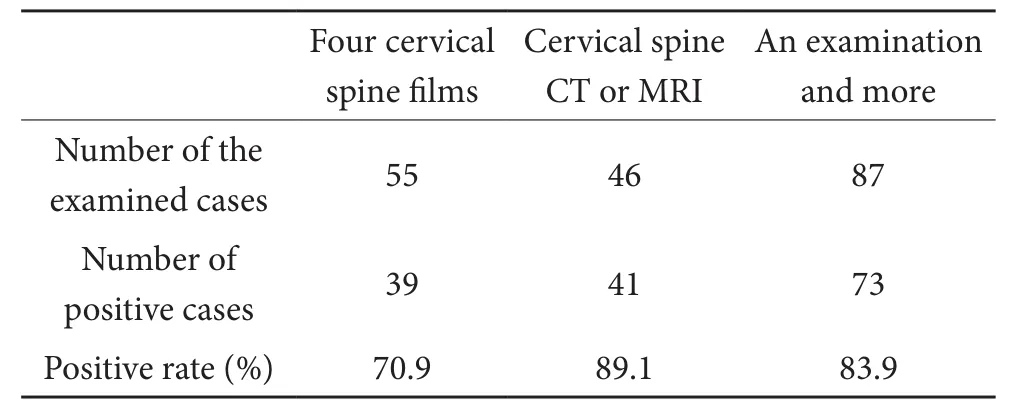
Table 5 Positive results of three tests
Descriptive statistics of the positive results of three tests in the case group (Table 5) showed that, the positive rate of the four cervical spine films was 70.9%, and the positive rate of CT or MRI of the cervical spine was 89.1%. The comprehensive positive rate of this study was 83.9%.

Table 6 x2 test results for the occurrence of periarthritis and cervical spondylotic radiculopathy (CSR)

Table 7 Correlation between periarthritis and cervical spondylotic radiculopathy (CSR) (n=87)
The homogeneous chi-square test was performed on the side of the periarthritis of shoulder and the side of CSR in the case group (Table 6), and results showed that the difference between the periarthritis side and the CSR side was statistically significant, indicating a correlation between the two (x2=55.782,P=0.000<0.05).A rank correlation analysis was performed to explore the relationship between the two (Table 7), and results showed that there was a positive correlation between the occurrence of periarthritis and CSR (rs=0.738,P=0.000<0.05).
Typical cases
(1)Patient Wang xx, female, 54 years old, presented with a complaint of intermittent right shoulder pain for 10 years,right shoulder pain for 3 years, aggravation for 3 days. Past medical history: She denied any history of cerebrovascular disease, cardiovascular disease, autoimmune system disease, diabetes, malignant tumor, etc. She had previous symptoms of intermittent neck discomfort and no recent history of shoulder trauma. Examination: cervical muscle tension, tenderness on the inner edge of the right scapula(+), restricted movement of the right shoulder, and tenderness around the shoulder (+). The right shoulder joint was shown in the lateral position: the bone structure of the right shoulder joint was intact, the density was reduced, the bone cortex was thinned, the trabeculae were thin, and no abnormalities were found. MRI plain scan of the right shoulder showed: 1. Degenerative changes of the right shoulder joint (bone hyperplasia, femoral head subcapsular changes); 2. Local abnormalities of the right superior supraspinalis, infraganglia, and subscapularis tendons, considering the rotator cuff injury and the partial tear of the superior tendon; 3. A small amount of fluid in the joint cavity, biceps longus tendon sheath fluid. Cervical spine MRI showed: 1. Degenerative changes of cervical spine, cervical spine curvature straightened and partial retroflexion; 2. C3-4, C4-5 central disc herniation, and signs of compression of the right nerve root.
(2)Patient Li xx, male, 60 years old, presented with a complaint of right shoulder pain with limited activity for more than half a year, aggravated for more than three months. Past medical history: Cerebrovascular disease,cardiovascular disease, autoimmune system disease,diabetes, malignant tumor and other medical history were denied. He had a history of cervical spondylosis for 10 years, and no recent history of shoulder injuries.Examination: Shoulder joint mobility: 75° abduction on the right, 45° extension on the right and unrestricted forward flexion; normal movement on the left. Neck tenderness was negative. MRI plain scan of the right shoulder showed: 1. Degeneration of the right shoulder(hyperplasia of the humerus, edema of the bone marrow below the joint surface); 2. Joint cavity and biceps longus tendon sheath effusion. MRI plain scan of the cervical spine showed: 1. Mild osteogenesis of the cervical spine;2. C3-4, 5-6, 6-7 disc bulging with signs of compression of the right nerve root; 3. Slender right vertebral artery.Four cervical spine films showed: degenerative changes.Cervical vertebral body margins became sharp and rough,and the cervical 5-6 vertebra space was slightly narrowed.The hyperplasia of the articular process of the neck 4-7 and the hyperplasia of the articulation of the vertebrae caused the corresponding intervertebral foramen to become smaller, and the right side was smaller than the left side.
Discussion
Discussion of general information
According to the statistics of the gender and age characteristics in the case group, the incidence of periarthritis of the shoulder in women is slightly higher than that in men, and most often occurs at the age of 40-62 years old, and the highest age is 50 years old. These findings are consistent with previous conclusions about the onset age and gender characteristics of the periarthritis of the shoulder[14]. It is a paired case-control study, the control group consisted of concurrent visits, without shoulder pain and dyskinesia, and their gender and age(difference ± 2.5 years) were matched with the case group at a 1:1 ratio. Therefore, the influence of age and gender in the study of the correlation between periarthritis and cervical spondylosis was excluded. Due to the relationship between the control group and the case group in this study and other factors, it can’t yet conclude that in the general population,the age of cervical spondylosis is also 40-60 years old,although the epidemiological study does indeed[15].
According to the results of the fit test, the probability of left and right periarthritis in this study is basically equal. This is different from the results obtained in many previous studies which demonstrated that the left side is more prevalent than the right side, the difference may be related to small sample size of the study. Therefore, a large sample of evidence-based research is still needed on the probability of the periarthritis on the left and right sides in order to obtain fair, scientific, and rigorous conclusions.Contralateral shoulder joints can be affected in months or years after periarthritis of the shoulder occurring on one side. Occurrence of both sides is rare[16], but it is reported that 14% can occur simultaneously[1,8,17]. In order to obtain more obvious and clear results, this study directly excluded patients with bilateral shoulder pain or limited mobility.Patients with periarthritis of both shoulders have not been studied, so the characteristics of the occurrence of bilateral periarthritis cannot be verified.
According to the history of natural diseases, the disease course of patients with periarthritis in the case group was artificially divided into 5 groups: within 3 months,3-9 months, 9-15 months, 15-24 months, and beyond 24 months. Among them, the number of cases within 3 months, 3-9 months, 9-15 months, and beyond 24 months was basically the same, with only 4 cases in 15-24 months.Therefore, due to the small number of cases in this group,the functional characteristics of each shoulder joint may not be obvious or even biased. In this study, the disease duration of more than 24 months accounted for 25.3% of the case group, indicating that the shoulder joint function of a considerable number of patients did not fully return to normal during the thawing period. L. Hollmann et al[18]believed that periarthritis of the shoulder is a common cause of severe and long-term dysfunction, which is characterized by spontaneous pain and progressive limitation of shoulder movement. Li Jun and other studies[19]found that after conservative treatment, the pain and limited mobility of the patients have been improved to the greatest extent,but most patients still fail to fully return to the normal state. In the end, the adverse consequences of shoulder dyskinesia will remain. It can be seen that although there is a self-limiting process of periarthritis of the shoulder,some patients still have symptoms of pain and/or limited mobility[8].
Discussion of the incidence of cervical spondylosis in the case group and the control group
According to the results of the homogeneityx2test between the case group and the control group, the incidence of CSR in the case group was significantly higher than that in the control group. This study was a paired case-control study.The control group recruited normal person with the same gender and a 2.5-year age difference comparing to the case group in the same period. This recruitment method excluded the effect of gender and age on the incidence of CSR in the two groups. Therefore, the variable comparing the incidence of CSR between the two groups in this study can be considered to be only with or without periarthritis.The incidence of CSR in the control group was 71.3%,which was higher than that in the general population of CSR epidemiology (the incidence of cervical spondylosis was 50%-70%, and CSR accounted for 60%-70%)[14]. This result is considered because the control group was selected based on the case-group pairing, so that the average age of the relatively normal person in the control group was about 50 years old. With the increase of age, the incidence of cervical spondylosis will also increase (the incidence of 50-70 years old can even reach 90%), eventually leading to a higher incidence of cervical spondylosis in the control group than normal people. However, this study did not collect, statistics, and analyze general data such as work and living habits of the tested subjects. These factors can also affect the occurrence of cervical spondylosis.At the same time, there may be some technical defects and insufficient funding in this research. This is the shortcoming of this study, and it is necessary to improve it in the related research if conditions permit.
Discussion of the relationship between periarthritis and CSR
After statistical analysis of the three tests was performed,the comprehensive positive rate of the three tests was 83.9%, that is, the probability of periarthritis occurring on the same side as that of CSR is very high. Therefore, after performing four-point examination of cervical spine, CT or MRI on patients with periarthritis, we can directly infer the occurrence or possible side of periarthritis from the side of CSR. Therefore, this method can suggest the side of periarthritis also reflects the possible correlation between periarthritis and CSR, which may provide some basis for clinical comprehensive treatment of neck and shoulder.The affected side of periarthritis localizes diagnosis by this method. Although there isn’t as high as 95% or higher the positive rate of shoulder MRI, CT, arthrography,arthroscopy, and “gold standard” arthroscopy[20]. However,it can reduce the cost of multi-site examination, and it is a non-invasive examination and an etiology examination.It can not only locate the diagnosis, but also determine the cause, so that the neck and shoulder can be treated simultaneously. Cervical treatment for patients who have not shown symptoms such as shoulder pain or shoulder movement disorders may play a certain role in preventing the occurrence of periarthritis of the shoulder. There are still deficiencies in this study, that is, the authenticity,reliability, and practicability of this diagnostic test were not evaluated in this study, and only the positive rate was analyzed. Therefore, further evaluation of diagnostic test is needed.
According to the results of homogeneityx2test and rank correlation analysis between the periarthritis side and the CSR side, there is a strong positive correlation between the periarthritis side and the CSR side. This result is consistent with previous studies[10-11,21]. This study is a case-control study that can prove the correlation and closeness of the relationship between the two, and can explain the significance of CSR in the etiology and disease prevention of periarthritis. However, it cannot be inferred that cervical spondylosis is the sole or main cause of periarthritis. To determine whether cervical spondylosis is the cause of periarthritis of the shoulder, further research is needed in a cohort study. At the same time, the effects of neck and shoulder treatment, shoulder-only local treatment, and neck-only local treatment on patients with periarthritis of the shoulder were compared to further explain the correlation between the two.
Conclusion and Outlook
Conclusion
(1)Periarthritis occurs frequently around the age of 50 years old, with more women than men, and more on the left side than on the right side.
(2)Periarthritis is a pathological continuum with a selflimiting process, but some patients may have varying degrees of joint pain and/or limited mobility.
(3)The imaging data of the cervical spine may play a certain role in the diagnosis of the bilateral periarthritis.
(4)There may be a close positive correlation between periarthritis and CSR.
(5)The cervical spine imaging examination of patients with periarthritis may provide a certain basis for the clinical treatment of neck and shoulder.
Outlook
Frozen shoulder is a common disease of middle-aged and elderly people. In recent years, there is an onset trend of younger people, which seriously affects the quality of life and work of patients. The problem of frozen shoulder needs to be solved urgently. Although there are many clinical studies and various methods for the treatment of periarthritis of the shoulder, symptomatic treatment is still predominant, resulting in poor treatment effect and limited long-term residual activity in some patients.Therefore, in order to solve the problem of periarthritis of the shoulder, not only symptomatic treatment is needed to ameliorate the symptoms, but also the cause must be clarified.
At present, the etiology of periarthritis of the shoulder has been definite or is being researched and proven. A view that cervical spondylosis is one of the causes of periarthritis of shoulders has been recognized by most scholars, but in the clinical treatment process, it has not been possible to clarify its etiology, and comprehensive treatment of neck and shoulder is performed. Although this study has drawn a strong positive correlation between periarthritis and CSR, it provides a basis for the study of the correlation between periarthritis and cervical spondylosis, and for the clinical treatment of cervical vertebrae in patients with periarthritis. However, this evidence is insufficient to prove that CSR is the cause of the onset of periarthritis of the shoulder, and further grouping and expanding samples are needed to study. And the neck and shoulder can be studied for the treatment effect of this disease, further explaining that cervical spondylosis is the cause of its problem. At this stage, although some scholars believe that the occurrence of periarthritis of the shoulder may also be related to changes in hormone levels, there is no direct conclusion on the correlation between the two.Therefore, research and verification on this issue can be conducted to guide the treatment and prevention of the disease.
There are many researches on the problem of periarthritis of shoulders, and there are various methods for its diagnosis, and the positive rate is very high. However,these examinations are targeted on the local manifestations of the joints, and there are few methods to perform the diagnosis from the source site. This study aims to explore the cause of periarthritis of the shoulder, which is a cervical spondylosis. Through the cervical imaging findings, the onset of the periarthritis of the shoulder was diagnosed directly, and the positive rate was high. From the etiology perspective, this method may not only help locate the periarthritis of the shoulder, but also provide a certain basis for guiding clinical treatment, and provide a basis for the combined use of etiology treatment with local symptomatic treatment. At the same time, for patients with cervical spondylosis who have not yet experienced shoulder symptoms, timely treatment of cervical spondylosis may also have a certain effect on preventing or slowing down the occurrence of periarthritis of the shoulder.
杂志排行
Global Traditional Chinese Medicine的其它文章
- Rheumatoid arthritis and JAK2/STAT3 signaling pathway: How does the TCM works?
- Effects of nine saponins of Aralia echinocaulis root on the viability of bone marrow-derived macrophages
- Bushen Huoxue methods combined with amiodarone in the treatment of coronary atherosclerotic heart disease with severe frequent premature ventricular contractions: a case report
- Research status, countermeasures and recommendations of emergency management system for TCM prevention and control of major epidemics#
- Mechanism of prevention and treatment of osteoporosis with traditional Chinese medicine