Incidental anal 18fluorodeoxyglucose uptake:Should we further examine the patient?
2020-09-18AnneSophieMoussaddaqCharlneBrochardXavierPalardNovelloEtienneGarinTimothWallenhorstEricLeBalcAlexandreMerliniheritierThomasGrainvilleLaurentSiproudhisAstridLivre
Anne-Sophie Moussaddaq,Charlène Brochard,Xavier Palard-Novello,Etienne Garin,Timothée Wallenhorst,Eric Le Balc’h,Alexandre Merlini L’heritier,Thomas Grainville,Laurent Siproudhis,Astrid Lièvre
Anne-Sophie Moussaddaq,Charlène Brochard,Timothée Wallenhorst,Eric Le Balc’h,Alexandre Merlini L’heritier,Thomas Grainville,Laurent Siproudhis,Astrid Lièvre,Department of Gastroenterology,University Hospital of Rennes,Pontchaillou,Rennes 35000,France
Charlène Brochard,Laurent Siproudhis,Inphy CIC 1414 University Hospital of Rennes,Pontchaillou,Rennes 35000,France
Xavier Palard-Novello,Etienne Garin,Department of Nuclear Medicine,Cancer Institute Eugène Marquis,Rennes 35000,France
Etienne Garin,Laboratoire Traitement du Signal et de l'Image-UMR1099,University of Rennes,Inserm,Rennes 35000,France
Abstract
Key words:Incidental anal 18fluorodeoxyglucose uptake;Anorectal disease;Rare
INTRODUCTION
18F-fluorodeoxyglucose (18FDG) positron-emission tomography/computed tomography (PET/CT) is a medical imaging technique based on the study of glucose metabolism.The use of this method has increased in oncology for the initial staging of cancer,monitoring treatment response and detecting early recurrence of a previously treated malignant tumour[1].It is also used in the management of infectious or inflammatory diseases[2].As a result of the increased indications for and availability of18FDG PET/CT,unexpected18FDG uptake has been identified in a variety of sites[3-6].In the field of gastroenterology,several studies have focused on colorectal locations[7-17].Incidental focal colorectal18FDG uptake on18FDG PET/CT imaging was associated with endoscopic lesions in two-thirds of the cases,with a high rate of advanced neoplasms[7],but no metabolic parameter has been identified to distinguish neoplasms from benign lesions[7,18].Thus,a complete colonoscopy tends to be recommended for all patients.
Within the field of gastroenterology,no studies to date have investigated incidental anal18FDG uptake.However,anorectal examinations are nevertheless simple and minimally invasive,and the diagnosis of anal pathologies is often based on the patient’s history or data obtained during the clinical examination.It seems important then to assess the rate of incidental anal18FDG uptake and to identify their aetiologies.Finally,no recommendations have been established in this particular situation.
The aims of this study were as follows:(1) To assess the rate of incidental anal18FDG uptake;(2) To identify the aetiologies of incidental anal18FDG uptake;and (3) To evaluate the correlation between18FDG PET/CT parameters and the diagnosis of an anorectal disease and the management of the disease.
MATERIALS AND METHODS
Patients
The database of18FDG PET/CT scans from a tertiary referral centre of nuclear medicine (January 2005 and December 2018) was reviewed.Among 4302018FDG PET/CT reports,those containing the terms “anal” or “anus” were identified.Then,we selected examinations with incidental anal18FDG uptake.Patients with personal histories of anal cancer were excluded.Patients with a history of pelvic radiation within 3 months or anal surgery within 6 weeks before the18FDG PET/CT were also excluded.The patient demographic data,past medical histories,indications for18FDG PET/CT and results concerning the initial oncological pathology report were extracted from the database.
18FDG PET/CT imaging protocol and analysis
The patients fasted for at least 4 hours before18FDG PET/CT imaging.The blood glucose level was controlled before the FDG injection.The acquisition ranged from the base of the skull to the proximal thighs and was performed 60 to 90 min after an intravenous injection of FDG.From January 2005 to May 2016,18FDG PET/CT exams were performed with a hybrid PET/CT scanner (Discovery LS,GE Medical Systems Inc.,Waukesha,WI,United States) after an intravenous injection of 4 MBq/kg FDG.From June 2016 to December 2018,18FDG PET/CT exams were performed with a hybrid PET/CT scanner (Siemens Biograph system,Siemens,Knoxville,TN,United States) after an intravenous injection of 3 MBq/kg FDG.For both PET systems,the data were reconstructed using an ordered-subsets expectation maximization iterative algorithm with corrections (attenuation,dead time,randoms,scatter,and decay).The standardized uptake value (SUV) was calculated and adjusted by the mean injected dose according to the tissue activity concentration and patient body weight.To include patients with focal incidental anal18FDG uptake,all18FDG PET/CT images from patients identified with incidental anal uptake were retrospectively reassessed by a nuclear medicine physician at the Department of Nuclear Medicine who was blinded to the anorectal findings.Anal18FDG uptake was defined as uptake located in the anal canal relative to the background activity.Incidental anal18FDG uptake was defined by the existence of anal hyperfixation in patients with no known anal pathology before the18FDG PET/CT.A 3-D volume of interest (VOI) was manually drawn to extract metabolic parameters (Syngo.via software;Siemens).The metabolic parameters extracted were the SUVmax(the highest SUV of all SUVs measured in the VOI),SUVmean(the mean of all SUVmeanmeasurements from the tumour VOIs with a local SUVmaxthreshold of 41%),and different metabolic volumes (MVs) defined as the volume produced by segmentation at the following fixed SUVmaxthresholds:50% (MV50),41%(MV41),and 30% (MV30)[1,14].In patients with anal uptake described on several18FDG PET/CT scans,the metabolic parameters selected were those that corresponded to the18FDG PET/CT with the largest SUVmax.
Management of incidental anal 18FDG uptake
The data about management after the discovery of incidental anal18FDG uptake were collected from the patient records from the Department of Nuclear Medicine.The data were compared with the patient records from the general practitioner and/or the specialist,if applicable.
The data collected from patients who further investigated were as follows:Symptoms,practitioner who performed the evaluation (oncologist,radiotherapist,surgeon,gastroenterologist,or colorectal specialist),evaluation modality (rectal examination,anoscopy),further examinations (CT scan,magnetic resonance imaging,endoanal ultrasound,and examinations under general anaesthesia,colonoscopy,or histology) and results,if available.The diagnosis was recorded and classified as follows:Haemorrhoidal disease,anal fissure,neoplasia,fistula,anal condyloma,or other diagnosis.Each proctologic report was reviewed by a specialist in proctology from the University Hospital of Rennes.Treatments were offered in case of symptomatic disease or if there was a risk of extension and/or aggravation of the disease.The treatment was chosen according to the habits of the practitioner.Patients who were offered treatment were identified and compared to those who were not treated.The proposed treatments were collected.
Among the patients with incidental anal18FDG uptake,the patient data were compared according to the occurrence of anorectal investigations.
Statistical analyses
The quantitative variables are presented as means and percentiles (interquartile range of 25% and 75%).The qualitative variables are presented as numbers and percentages.The qualitative variables were compared usingχ2tests or Fischer’s exact tests,as appropriate.The quantitative variables were compared using the non-parametric Wilcoxon’s test.Comparisons between patients who underwent examinations with those who had not were performed using the Wilcoxon test and theχ2test or Fisher’s exact test,as appropriate.The same tests were applied to compare patients who were offered treatment with those who were not.APvalue <0.05 was considered statistically significant.To measure the discriminatory accuracy of SUV and MV for diagnostic and therapeutic management,a receiver operating characteristic (ROC)analysis was performed,and the area under the ROC curve (AUROC) was calculated.Logistic regression analysis was performed with independent categorical items obtained atP<0.05 by univariate analysis using a forward method to identify factors associated to treatment.Pearson correlation coefficients and Fisher tests were performed to verify whether the Pearson coefficients were significantly different from 0.The tests were performed using JMP Pro software,version 13.0.0 (SAS,Cary,NC,United States).
RESULTS
Overall study population
Among the 4302018FDG PET/CT scans performed between January 2005 and December 2018,19718FDG PET/CT of 146 patients reported incidental anal uptake.Twelve patients were excluded;finally,134 patients were included in the study(Figure 1).The patient characteristics and18FDG PET/CT indications are summarized in Table 1.Twenty-one (15.7%) patients had the following past anorectal histories:Haemorrhoidal disease (7.8%),anal fistula (4.7%),anal fissure (1.6%),anal condyloma(1.6%),and faecal incontinence (0.7%).
Patients who underwent anorectal examinations
Among the 134 patients with incidental anal18FDG uptake,48 (35.8%) underwent anorectal examinations to explore the anomaly.The characteristics of the patients who underwent examinations are depicted in Table 1 and Table 2.The patients were examined most frequently by a colorectal specialist (62.5%) or a gastroenterologist(20.8%).The clinical examinations ranged from a simple inspection of the anal margin(95.8%) to anoscopy (51.1%).More than half (54.2%) of the patients had at least one other examination.Patients who underwent examinations were compared with those who did not undergo examinations (Table 1).The two groups were comparable in terms of age,sex,indication for18FDG PET/CT,primitive cancer,history of pelvic radiotherapy and18FDG PET/CT metabolic parameters.Patients who underwent examinations more frequently had a past history of anorectal disease than those who did not undergo examinations (P= 0.0002).Among the 48 patients who underwent examinations,33 (69%) had the following anorectal diseases:Haemorrhoidal disease (n= 19),anal fissure (n= 6),recurrence of rectal adenocarcinoma on the coloanal anastomosis (n= 2),condyloma (n= 3),faecal impaction (n= 1),suppuration (n= 1)and solitary rectal ulcer syndrome (n= 1) (Figure 2).
In our study group,no metabolic parameters were significantly associated with the presence or absence of a diagnosis;likewise,there were no significant differences between anorectal diseases according to the metabolic parameters.
Treated patients and therapeutic impact of metabolic parameters
Among the 48 patients who underwent examinations,18 (37.5%) were offered treatment (Table 3).The characteristics of the treated patients were compared with those of the untreated patients and are depicted in Table 2.All patients who received treatment had more frequent complaints than those who did not receive treatment and were examined by colorectal specialists or gastroenterologists.Of the asymptomatic patients,18/29 were diagnosed [haemorrhoidal disease (n= 12),anal fissure (n= 2),condyloma (n= 3) and solitary rectal ulcer syndrome (n= 1)] and 8/29 were offered treatment.Among the 29 asymptomatic patients,the18FDG PET/CT metabolic parameters differed significantly between treated and untreated patients.The group of asymptomatic patients that was offered treatment had higher SUVmaxand SUVmeanmeasurements (P= 0.03 for both) and lower MV41 and MV30 values than the groupasymptomatic patients without treatment (P= 0.02 andP= 0.03,respectively).Among the 15 patients with progressive PET-CT (considered poor prognosis),8 had treatment and 7 had no treatment (P= 0.46).The18FDG PET/CT metabolic parameters differed significantly between treated and untreated patients.The group of patients that was offered treatment had higher SUVmaxand SUVmeanmeasurements (P= 0.02 for both)and lower MV41 and MV30 values than the group without treatment (P= 0.05 andP=0.03,respectively).The ROC curves of the SUVmax,SUVmean,MV41 and MV30 as predictive factors for the treatment of examined incidental anal18FDG uptake are shown in Figure 3.According to the ROC curves,the optimal cut-off for SUVmax,SUVmean,MV41 and MV30 were 9.6,6.1,3.1 cm³ and 7.4 cm³,respectively.The SUVmaxmeasurements were inversely correlated with MV41 (r = -0.27,P= 0.0006) and MV30 (r= -0.18,P= 0.0002).In a multivariate analysis including the presence of symptoms,the diagnosis (yes) and the SUVmean>6.1 cm3,the factor significantly associated with the treatment was the SUVmean>6.1 cm3[OR = 6.87 (1.18-29.9),P= 0.03].
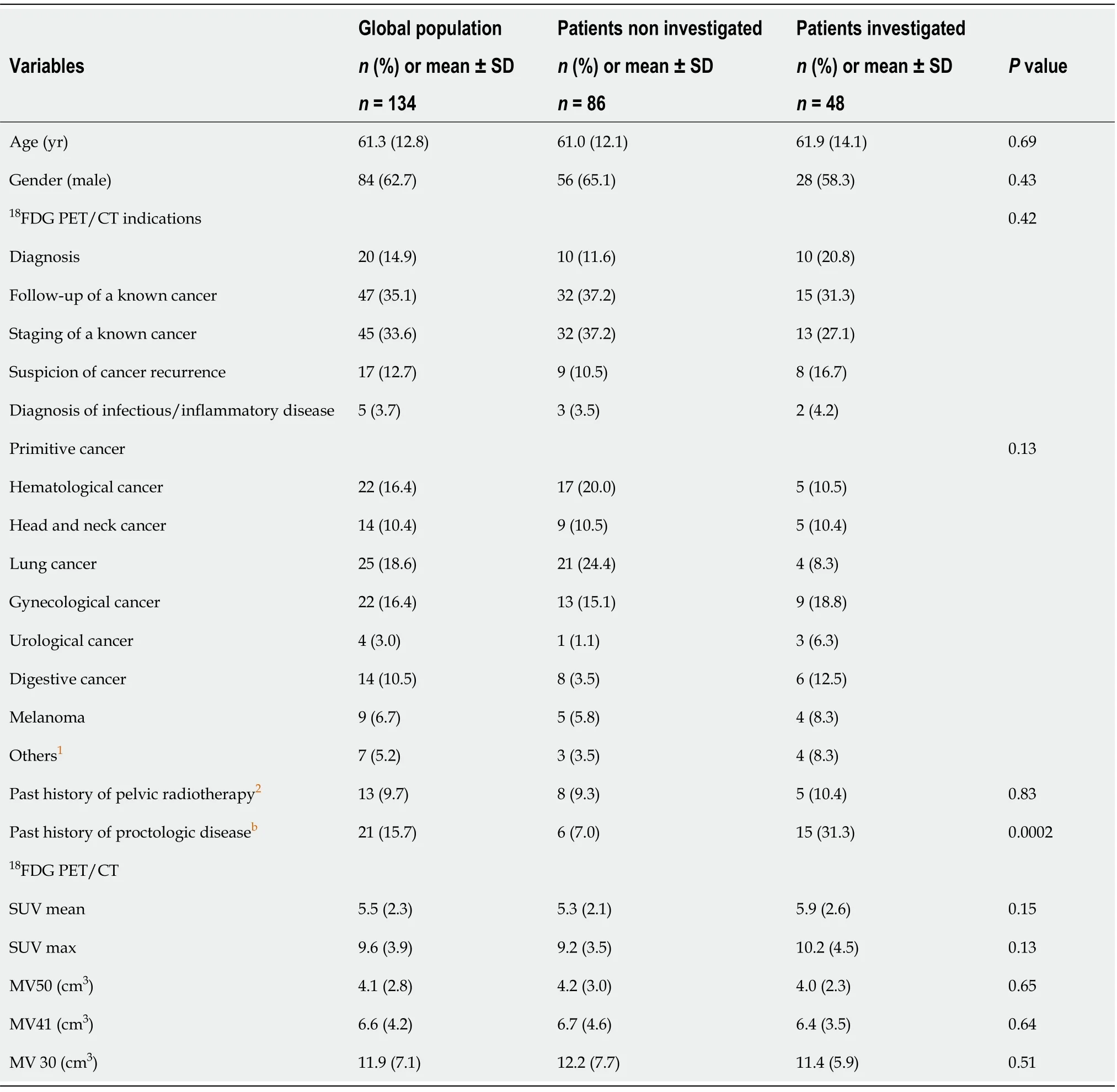
Table 1 Characteristics of the global population (n = 134)
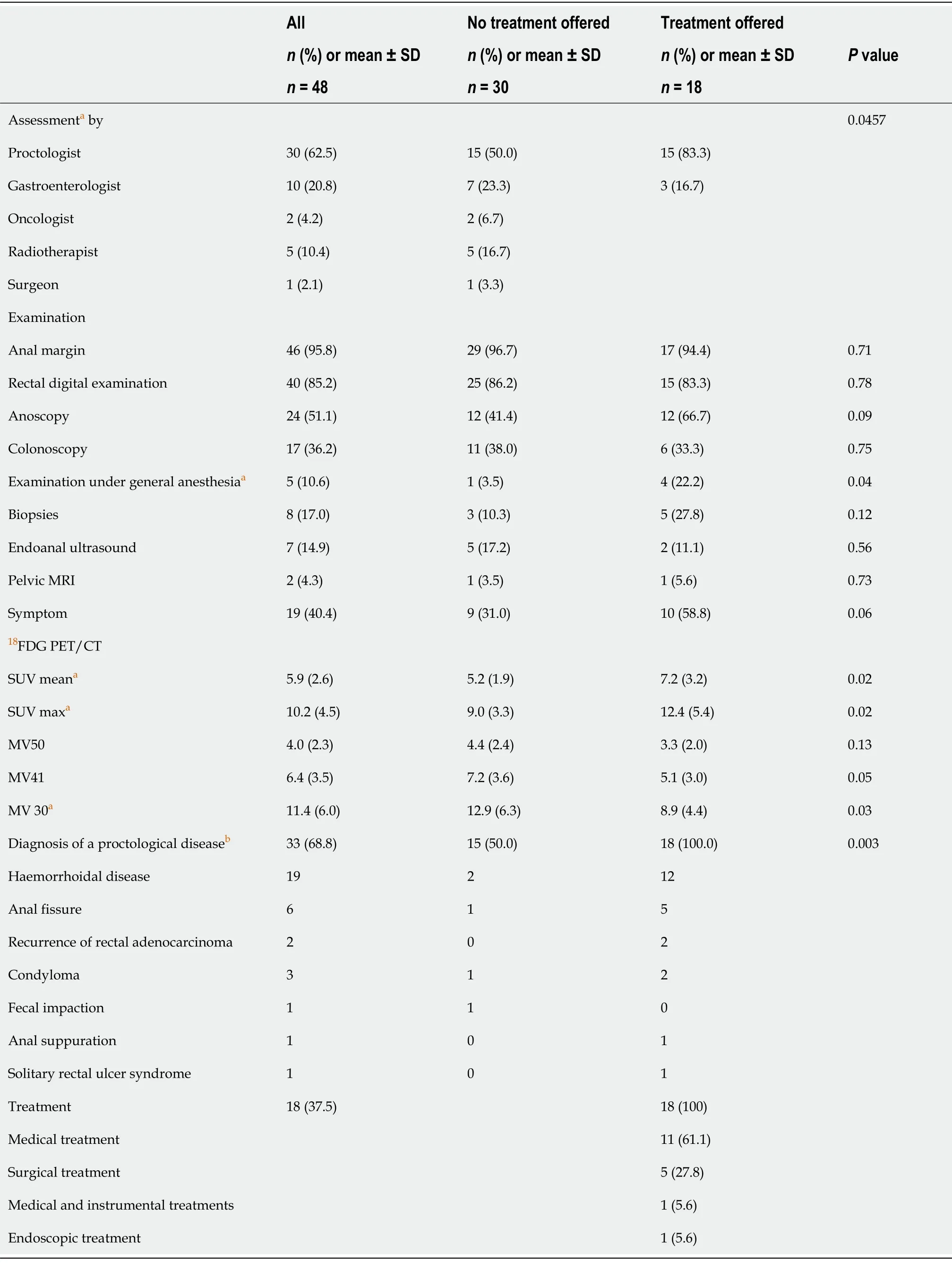
Table 2 Characteristics of population investigated (n = 48)

Table 3 Treatments
DISCUSSION
To the best of our knowledge,this is the first study to evaluate the rate of incidental anal18FDG uptake and its diagnostic and therapeutic impact in a large series of18FDG PET/CT scans performed over a 14-year period.
The present work highlights that incidental anal18FDG uptake is a rare event(0.45%) and is not systematically explored (36%).When examinations are performed,an anorectal disease was diagnosed in more than two-thirds of the patients (69%),and a specific treatment was proposed in almost 40% of these patients.Finally,we identified some metabolic parameters (SUVmax,SUVmean,MV41 and MV30) significantly associated with anorectal treatment,with SUVmaxhaving the best accuracy.Taken together,our data suggest that,although it is not frequent,incidental anal18FDG uptake should require anorectal examinations given its high diagnostic and therapeutic impact.
The main strengths of this work are the inclusion of a large number of18FDG PET/CT scans requested for various indications over a long period of time,reassessment of18FDG PET/CT images by a physician who was blinded to anorectal findings and exhaustiveness of the anorectal data collection.As previously mentioned,this is also,to the best of our knowledge,the first study to investigate the rate and management of incidental anal18FDG uptake.
In our series,incidental anal18FDG uptake was investigated in 36% of the patients,which means that it was not been taken into account in almost two-thirds of the patients.Several explanations are possible.First,incidental anal18FDG uptake was not mentioned in the conclusion but only in the details of the18FDG PET/CT report of many patients (58%),which suggests that many nuclear physicians considered this18FDG uptake to be non-clinically significant in the absence of data in the current literature.Furthermore,very few reports of consultations with the referring physician who prescribed the18FDG PET/CT mentioned the anal18FDG uptake,which may be explained by the following points:(1) No mention of the anal18FDG uptake in the conclusion of the18FDG/PET CT report;(2) The physician (an oncologist in the majority of cases) considered that the anal18FDG uptake was secondary compared to the pathology that motivated the18FDG PET/CT (tumour diagnosis,recurrence orprogression),regardless of whether the patients underwent examinations,and was comparable in each setting and (3) The physician did not dare to discuss this abnormality with the patient or the patient refused to be examined,as we know that anorectal complaints and examinations remain a taboo subject for both patients and physicians.
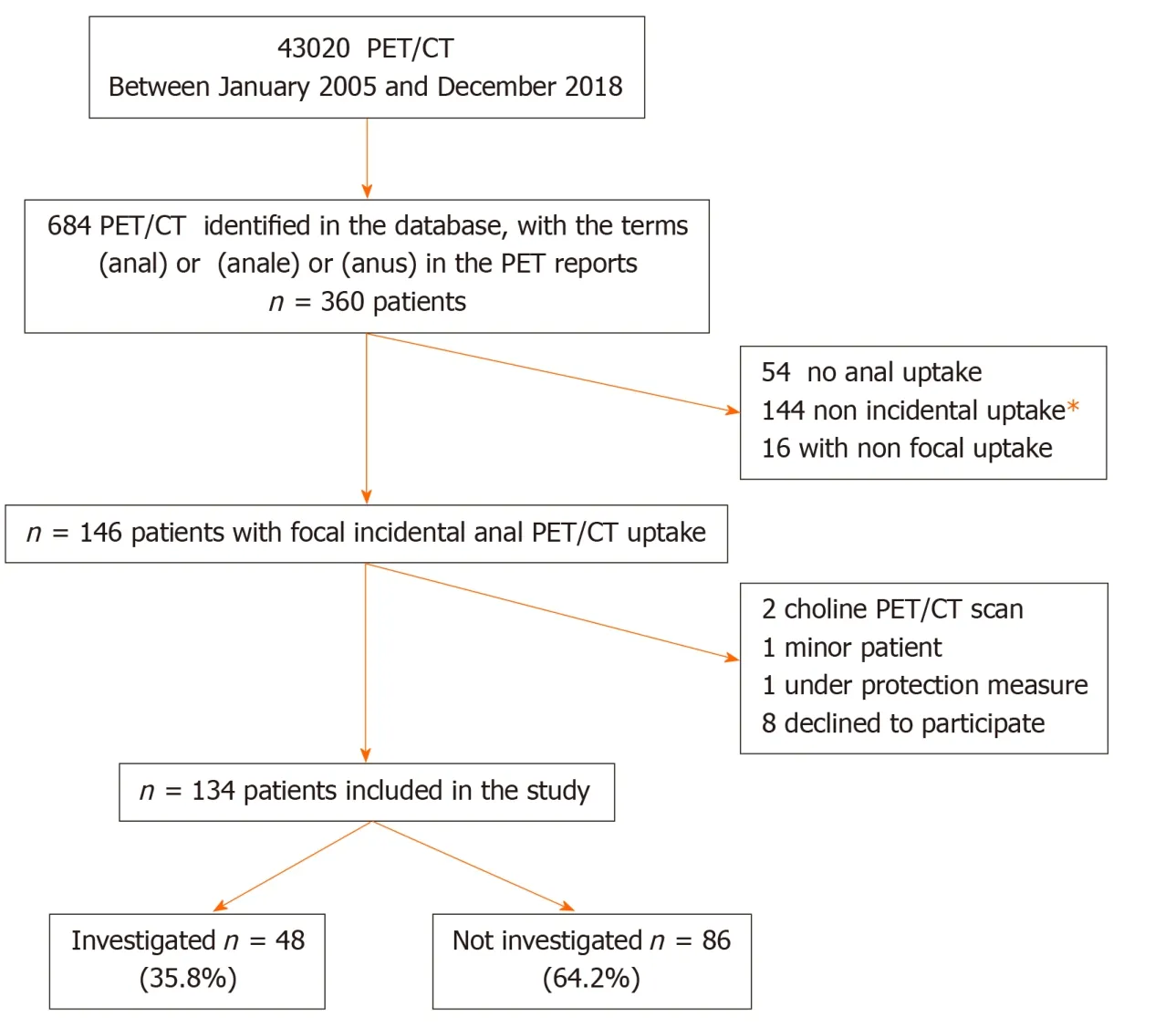
Figure 1 Flow chart.Among the 144 patients with non-incidental uptake,121 had known anal cancer;14 had pelvic cancer with known anal extension;2 had a known abnormality on anorectal examination at the time of the positron emission tomography with computed tomography;7 had recent pelvic radiotherapy or surgery.PET/CT:Positron emission tomography with computed tomography.

Figure 2 Incidental anal 18F-fluorodeoxyglucose uptake.A:An incidental anal 18F-fluorodeoxyglucose uptake in 1 study patient with hemo rrhoidal disease that required medical treatment (standardized uptake value max = 18.1);B:An incidental anal 18F-fluorodeoxyglucose uptake in 1 study patient without proctological diagnosis (standardized uptake value max = 4.9);C:An incidental anal 18F-fluorodeoxyglucose uptake in 1 study patient with hemorrhoidal disease that did not require treatment (standardized uptake value max = 8.8).
Importantly,patients who were examined underwent a specific anorectal treatment in almost 40% of the cases,including surgery in 28% (5/18) of these cases.Therefore,it seems justified to systematically seek anorectal complaints and propose an anorectal examination,which should include at least an anal margin and rectal digital examination.This first assessment is simple and minimally invasive and makes it possible to evaluate if the patient needs to be referred to a specialist.However,this strategy cannot assess haemorrhoidal diseases with enough sensitivity.Notably,40%of the examined patients in the present study had anorectal symptoms,which emphasizes the importance of a obtaining a good patient history to identify those who need to be directly addressed to a colorectal specialist.
Our study identified SUV and MV measurements as factors associated with the anorectal examination having a therapeutic impact,with SUVmaxhaving the bestaccuracy.Interestingly,patients who received treatment had significantly lower MV30 and MV41 values and higher SUVmaxand SUVmeanmeasurements than patients who did not receive treatment.These conclusions are different from those of colorectal positive uptake.In the studies on incidental focal colorectal18FDG uptake on18FDG PET/CT images,the metabolic parameters could not differentiate between true positives and false positives,with acceptable sensitivity and specificity,and therefore had no diagnostic or therapeutic impact[7,17-19].
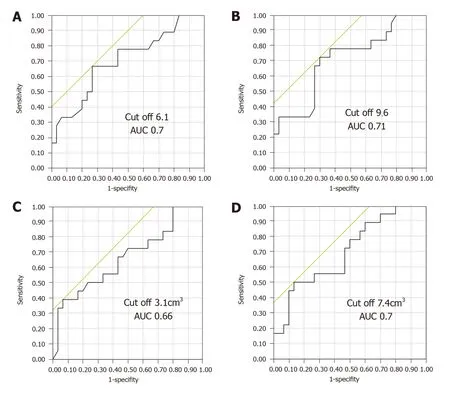
Figure 3 Receiver operating characteristic curve.A:Standardized uptake value mean;B:Standardized uptake value max;C:Metabolic volumes 41;D:Metabolic volumes 30,to differentiate patients requiring treatment from others.AUC:Area under the curve.
In our study,the diagnoses correspond more to inflammatory or infectious processes than to other conditions.In this field,the diagnostic,therapeutic or prognostic impact of metabolic parameters has not been identified,except for SUVmax,which has been shown to have a prognostic impact on cardiovascular events and corticosteroid response in patients with cardiac sarcoidosis[20].However,in oncology,the metabolic tumour volume (MTV) has a prognostic impact on diseases in several locations (head and neck cancers or anal cancers,for example),with a prognosis that worsens as the MTV increases[1,21-27],which is sometimes also the case for SUVmax[28-31].These parameters also have a role in monitoring therapy response[1,32-34].Paradoxically,our results showed that smaller MVs are associated with treatment.We have not found any similar cases in the literature.Additionally,a lesion does not necessarily require more treatment because it has a larger volume.
Our study results,however,should be interpreted with caution for several reasons.The main limitations of this study are its retrospective and monocentric design.Moreover,it is possible that the rate of anal18FDG uptake we reported is underestimated because it cannot be excluded that this anomaly is not systematically described by all nuclear physicians,given the lack of clinical significance described so far.In addition,62% of the patients included did not undergo anorectal examinations;thus,the aetiology of their anal18FDG uptake remains unknown.It would have also been interesting to investigate a control group of patients without anal18FDG uptake to better demonstrate the diagnostic and therapeutic impact of anal18FDG uptake.In our study,the proportions of patients who underwent examinations and those who received treatment were low,which led to a lack of power,even though this is the largest series reported.Due to the small sample size,we were unable to analyse the relationship between metabolic parameters and a precise diagnosis.The role of haemorrhoidal disease in anal18FDG uptake remains somewhat speculative since haemorrhoids cushions are a normal compound of anal anatomy.Finally,symptomatic complaints not recorded (retrospective analyses) may bias the results(high proportion of treated anorectal lesions).
In conclusion,incidental anal18FDG uptake is a rare event and is rarely explored.However,when explored,a diagnosis is made in more than two-thirds of the cases,and treatment is proposed in more than one-third of the cases.Some metabolic parameters associated with a therapeutic impact have been identified.These data should encourage practitioners to explore incidental anal18FDG uptake systematically because some patients may recover well from an anal pathology.
ARTICLE HIGHLIGHTS
Research background
The use of18F-fluorodeoxyglucose (18FDG) positron-emission tomography/computed tomography (PET/CT) has increased in oncology and in the management of infectious or inflammatory diseases.As a result of the increased indications for and availability of18FDG PET/CT,unexpected18FDG uptake has been identified in a variety of sites.In the field of gastroenterology,several studies have focused on incidental focal colorectal18FDG uptake.No studies to date have investigated incidental anal18FDG uptake.Anorectal examinations are nevertheless simple and minimally invasive,and the diagnosis of anal pathologies is often based on the patient’s history or data obtained during the clinical examination.
Research motivation
It seems important to assess the rate of incidental anal18FDG uptake and to identify their aetiologies.Finally,no recommendations have been established in this particular situation.
Research objectives
The objectives of this study were as follows to assess the rate of incidental anal18FDG uptake,to identify the aetiologies of incidental anal18FDG uptake,and to evaluate the correlation between18FDG PET/CT parameters and the diagnosis of an anorectal disease and the management of the disease.
Research methods
We carried out a retrospective observational single-centre study.The data from patients with incidental anal18FDG uptake were analysed.Patients who underwent anorectal examinations were identified and compared to those who did not undergo examinations.Patients who were offered treatment were then identified and compared to those who did not receive treatment.Comparisons between patients were performed using the Wilcoxon test and the chi-squared test or Fisher’s exact test,as appropriate.APvalue <0.05 was considered statistically significant.
Research results
Among the 4302018FDG PET/CT scans performed,19718FDG PET/CT scans of 146 patients reported incidental anal uptake:The rate of incidental anal18FDG uptake was 0.45%.Among the 134 patients included,48 (35.8%) patients underwent anorectal examinations and anorectal diseases were diagnosed in 33 (69.0%) of these patients haemorrhoidal disease (n= 22),anal fissure (n= 6),recurrence of rectal adenocarcinoma on the coloanal anastomosis (n= 1),condyloma (n= 3),faecal impaction (n= 1),suppuration (n= 2) and solitary rectal ulcer syndrome (n= 1).Eighteen/48 (37.5%) received treatment.Among the examined patients,those with a pathology requiring treatment had significantly smaller metabolic volumes (MV) 30 and MV41 values and higher maximal and mean standardized uptake value measurements than those who did not require treatment.
Research conclusions
Incidental anal18FDG uptake is a rare event and is rarely explored.However,when explored,a diagnosis is made in more than two-thirds of the cases,and treatment is proposed in more than one-third of the cases.Some metabolic parameters associated with a therapeutic impact have been identified.These data should encourage practitioners to explore incidental anal18FDG uptake systematically because some patients may recover well from an anal pathology.
Research perspectives
Further large-scale prospective studies are needed.We would like to investigate a control group of patients without anal18FDG uptake to better demonstrate the diagnostic and therapeutic impact of anal18FDG uptake.
杂志排行

World Journal of Clinical Cases的其它文章
- Autoimmunity as the comet tail of COVID-19 pandemic
- Gender medicine:Lessons from COVID-19 and other medical conditions for designing health policy
- Complexities of diagnosis and management of COVID-19 in autoimmune diseases:Potential benefits and detriments of immunosuppression
- Emergency surgery in COVID-19 outbreak:Has anything changed?Single center experience
- Somatostatin receptor scintigraphy in the follow up of neuroendocrine neoplasms of appendix
- Efficacy of stool multiplex polymerase chain reaction assay in adult patients with acute infectious diarrhea