Complexities of diagnosis and management of COVID-19 in autoimmune diseases:Potential benefits and detriments of immunosuppression
2020-09-18TsvetoslavGeorgievAlexanderKrasimirovAngelov
Tsvetoslav Georgiev,Alexander Krasimirov Angelov
Tsvetoslav Georgiev,Clinic of Rheumatology,University Hospital "St.Marina",First Department of Internal Medicine,Medical University - Varna,Varna 9010,Bulgaria
Alexander Krasimirov Angelov,Clinic of Rheumatology,University Hospital "St.Ivan Rilski",Medical University - Sofia,Sofia 1612,Bulgaria
Abstract
Key words:Autoimmune diseases;Autoimmunity;COVID-19;Coronavirus;Serologic Tests;Cross reactions
INTRODUCTION
The prevalence of coronavirus disease 2019 (COVID-19) has exponentially increased not only in numbers but in range of distribution causing a global threat to modern societies across the globe.Classified as a pandemic by the World Health Organization,the COVID-19 outbreak has taken the lives of approximately 280000 people contracting more than 4 million,as of May 13,2020[1].The seriousness of this catastrophe necessitates an urgent,international,and multidisciplinary approach to bring about a change in the status quo achieving the much-needed catharsis in the theory and practice of diagnosis and management of COVID-19.
Advances in our understanding of COVID-19 have shown that tissue injury in severe and critically-ill patients is mediated by an overexuberant immune-mediated inflammatory response.This finding supports the rationale for searching a COVID-19-modifying drug not only in the long list of known antivirals but also among immunemodulating/suppressing drugs used in the management of autoimmune diseases(ADs)[2,3].Our hypothesis is supported by a quick trial search through the United States National Library of Medicine (ClinicalTrials.gov) and the Chinese Clinical Trial Registry (http://www.chictr.org.cn) where clear intentions for the repurposing of multiple immunosuppressive drugs could be found.The preliminary results look promising but further trials are warranted.
Our narrative review aims at presenting the complexities in diagnosis and management when dealing with patients with ADs amidst the COVID-19 crisis and commenting on the potential benefits and detriments of immunosuppression according to the leading societies dealing with ADs.
SEARCH METHODOLOGY
We conducted a literature search in the scientific databases Medline (PubMed) and Scopus and used the search engine Google Scholar to identify preprints.In PubMed and Scopus,both MeSH and relevant free-text terms were used.Recommendations for COVID-19 management from leading societies and teams handling ADs were retrieved.Given the innovative character of the data,relevant information was also included from preprints based on the authors’ perspective.Recommendations for writing a narrative review were followed[4].Our search was confined to articles published from January 2020 to May 2020.Older publications were also cited to provide contextual background.References of retrieved publications were further hand-searched for supplements.
DIAGNOSIS OF COVID-19 IN PATIENTS WITH ADS
With the expansion of the COVID-19 outbreak,its coexistence with an autoimmune disease is not a special case anymore.As of May 13,2020,the COVID-19 Global Rheumatology Alliance has reported 872 cases of rheumatic patients infected withsevere acute respiratory syndrome coronavirus 2 (SARS-CoV-2)[5]and this number probably represents only the tip of the iceberg.
COVID-19:Mimicking the flare of an autoimmune disease
Diagnosing a viral infection in patients with an already established immune-mediated disease might present a major challenge to the practicing physician.This assumption comes from the fact that its first symptoms could resemble a possible AD flare[3].However,in the case of COVID-19,there are further issues that need to be addressed.
Given the range of manifestations,the concept of COVID-19 has recently evolved from a monochromic disease to a “spectrum of disease” - a term that is commonly used in polysyndromic ADs.In fact,without any clear epidemiological data suggesting the diagnosis of COVID-19,the manifestation of nonspecific symptoms such as fatigue,fever,myalgia,and arthralgia in a rheumatic patient would normally alert the rheumatologist for a possible relapse of the underlying autoimmune disease.Furthermore,lymphopenia and thrombocytopenia,present in approximately 2/3 of the cases[6],interstitial lung disease,generalized rashes and vasculitis-like manifestations may further resemble an AD flare[7].Importantly,this assumption poses an undefined threat to those contracting the virus.Escalation of immunosuppressive treatment may put the patient at higher risk for severe viral infection by suppressing the adaptive immune system and thus inhibiting viral clearance[8].Therefore,it is of utmost importance to differentiate COVID-19 manifestations from relapse in patients with established autoimmune disease.
COVID-19 lung involvement and interstitial lung disease in ADs
Lung hyperinflammation and associated acute respiratory distress syndrome (ARDS)is thought to be the leading cause of death in patients with COVID-19[9].Pathological changes in the lungs of patients with COVID-19 driven ARDS are dominated by overreacted T-cells[10]causing a "cytokine storm" which plays an essential and commanding role in the disease pathogenesis and clinical outcome[6].These pathological findings remind us of a severe immune-mediated disorder.Interestingly,the patchy or diffuse pattern of the COVID-19 interstitial pneumonia sounds like “deja vu” to rheumatologists mimicking connective tissue disease-associated interstitial lung diseases (CTD-ILDs).More importantly,it has already been suggested that CTD-ILDs and COVID-19 ARDS share the same histomorphological,serological,and radiological features triggering organ-specific autoimmunity in predisposed patients[11].It should be also noted that hyperferritinemia,until recently reserved for a group of diseases with predominantly autoimmune genesis[12],has become a pathognomic feature of the cytokine storm mainly confined to the lung parenchyma[13].
Hypergammaglobulinemia in ADs and serological tests - a prerequisite for crossreactivity
Although reverse transcription-polymerase chain reaction (RT-PCR) remains the “gold standard” for diagnosing COVID-19[14],serological tests could serve as a complement to nucleic acid testing for the detection of suspected cases with negative RT–PCR results and in screening for asymptomatic contagious individuals in close contacts[15].Those antibody tests are widely available and have relatively lower costs,require almost no highly-specialized equipment,and are time-sparing,therefore affordable.
Notwithstanding that false-negative tests are a major concern at the population level,false positivity may present a diagnostic issue pertaining to patients with ADs.Diagnostic concerns come from the fact that,as a result of polyclonal hypergammaglobulinemia,patients with immune-mediated diseases and particularly those with autoimmune conditions may produce false-positive results for SARS-CoV2-IgG and IgM.Virus-specific antibody detection testing for the SARS-CoV-IgG and IgM has already shown false-positive results in patients with the following ADs - systemic lupus erythematosus,Sjogren’s syndrome,systemic sclerosis,mixed connective tissue disease,and rheumatoid arthritis[16].This list is probably inconclusive since crossreaction may be common in ADs with polyclonal hypergammaglobulinemia(Figure 1).Further studies are warranted to confirm or reject this hypothesis.Interestingly,the “vice versa” phenomenon has already been observed:Low titers of transient ADs-specific or -associated autoantibodies may be present in common viral infections[17].In a small study taking place in intensive care units,elevated serum titers of antinuclear autoantibodies were observed in over 90% of COVID-19 patients[12].Furthermore,anticardiolipin IgA antibodies and anti–β2-glycoprotein I IgA and IgG antibodies present frequently in sera of patients with COVID-19 and no previous history of ADs[18].Another recent study showed that 20% of patients with COVID-19had a prolonged activated partial thromboplastin time due to lupus anticoagulant associated with thromboses[19].
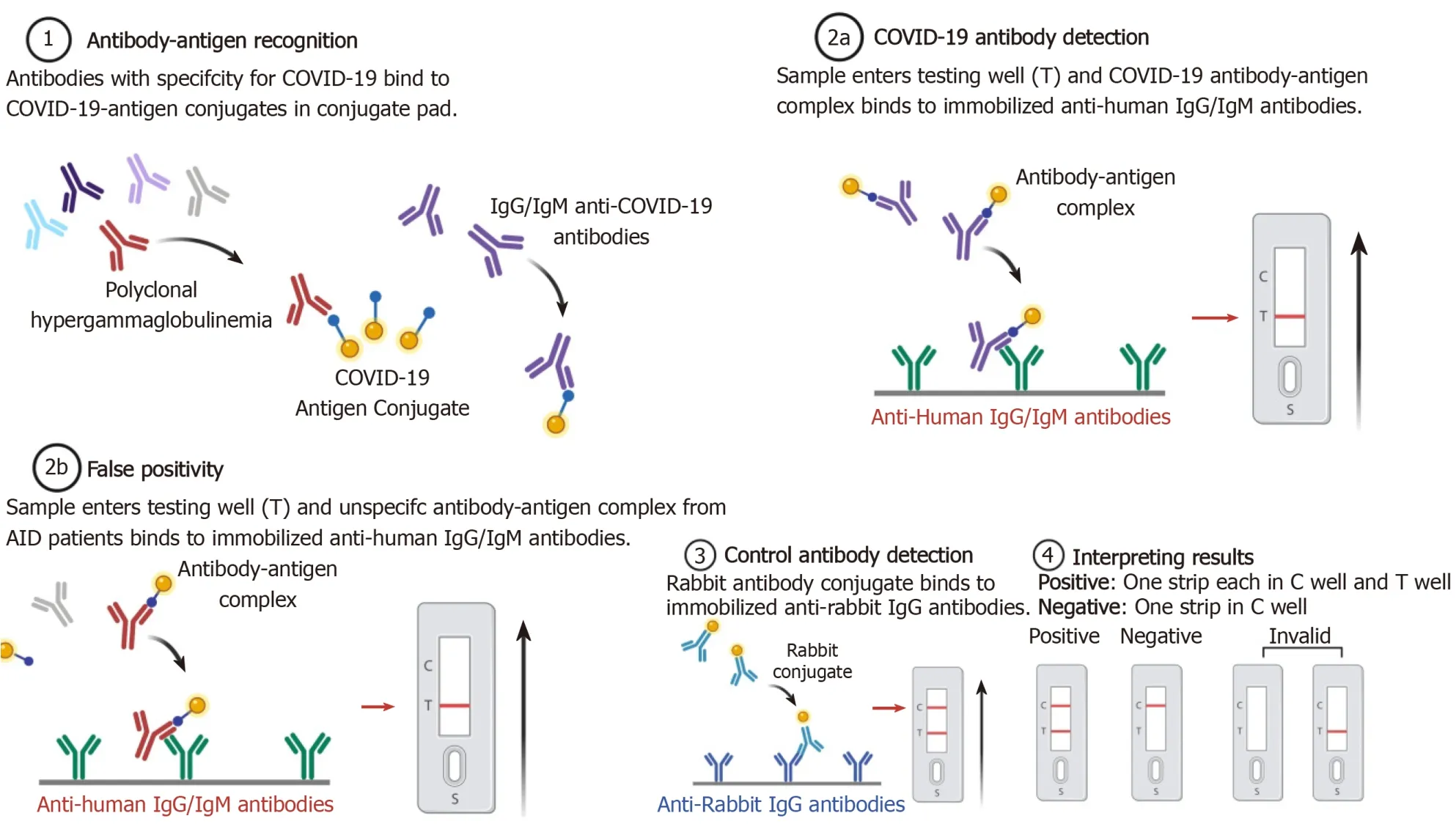
Figure 1 Viral antibody detection testing and hypothetical case of false-positive cross-reactivity in patients with autoimmune diseases and related polyclonal hypergammaglobulinemia (created with BioRender.com).COVID-19:Coronavirus disease 2019.
MANAGEMENT OF PATIENTS WITH ADS AMIDST THE COVID-19 PANDEMIC
Patients with ADs may have increased susceptibility to COVID-19 due to the underlying disorder,increased comorbidity,and ongoing therapy with immunosuppressive,immunomodulating,and/or glucocorticoid agents.Decisions about treatment should be made by an interdisciplinary team of experts because data is insufficient and recommendations are made on a speculative basis[20].Reduction of visits to the clinic and maximum utilization of tele-medicine should be made when appropriate.This is a ripe time for building a good infrastructure for a more convenient and cost-effective way to treat patients forthwith and in the future[21-39](Table 1).
Psychological and physical management
It is well established in the literature that a large percentage of people with ADs suffer from depression and other health-related quality of life impairments[40].As the pandemic situation progresses the data is relatively limited for how this restricted lifestyle will affect the population,but it can be presumed that it will unlock or exacerbate existing mental health conditions.The problem must be tackled on multiple levels with a wide array of interventions[41].Applicable/appropriate recommendations should be made on the usage of all available online platforms,hotlines,mindful practices,local or national resources for dealing with mental health issues.With today’s available technology isolation should only be physical not social,mental,spiritual,or emotional[42].However,measures on restriction of free movement do not mean limitation of physical activity and all forms of exercise.All kinds of exercise regimens should be emphasized to counter the lack of everyday dynamics as prolonged sedentary behavior can increase anxiety and depression[43].High-tech tools as mobile applications,games,and video formats can be utilized to meet the recommended levels of activity[44].Physical activity and exercise can be a very versatile intervention as it addresses the mental state,comorbidity and manages disease activityin ADs[45,46]Attention should be given to patients in a more frail state and joint conditions with specific exercise regimens.Because the lack of direct access to treatment and physician care implementation of online platforms is warranted,but a major limitation remains the lack of digital savviness/proficiency and the absence of technology in certain groups like the elderly.

Table 1 Guidance,recommendations,and statements for management of patients with autoimmune diseases
Pharmaceutical management
Treatment of COVID-19 is a rapidly developing matter,as for now,there is no highquality evidence to back a concrete regimen[47].The potential effect of immunosuppressive and anti-cytokine drugs has been extensively discussed but the potentially detrimental consequences of reducing inflammation in a critically ill patient should be carefully weighed[8,48-52].Consensus for the treatment of patients with a rheumatic disease with presumptive COVID-19 is that immunosuppression should be stopped temporarily but chloroquine/hydroxychloroquine (HCQ/CQ) may be continued[23].In the ideal clinical practice,monitoring the immune system status of the patient would provide useful insight into the polyphasic nature of COVID-19 and give us an opportunity to apply adequate therapy depending on the stage:Specific antivirals and stimulation of type-I Interferon in the early phase,suppression of hyperinflammation in the subsequent phase[50].Modulation of the inflammatory state with Interleukin-6 (IL-6) antagonists and JAK/STAT inhibitors among others is a potentially viable strategy to treat CRS and ARDS that is being intensively researched[50,52-54].
The antimalarial drugs CQ and HCQ are one of the medications that arguably gained the most traction for the possible treatment of COVID-19.With promising theoretical and small clinical study data,it sparked a hope for the sought after miracle cure.However,overall data on the subject is conflicting[55].As the evidence for the treatment of COVID-19 progressed a problem emerged facing the patients with ADs –medical supply shortage particularly for HCQ[56].Stopping intake can lead to a disease flare which can have deleterious effects that can increase morbidity and mortality[57].As for the potential benefits of the treatment from data on patients without ADs,we may extrapolate that there may be a possible effect on large number of patients who develop radiographic progression and reduction of symptomatic days,but an additional benefit of the addition of Azithromycin (AZ) to therapy is uncertain[58].A retrospective analysis of 1061 patients concluded that HCQ and AZ combination is safe and is correlated with a low fatality rate[59].An observational study of 1446 patients showed no significant effect and suggested removal of HCQ from the clinical guide[60].More data from high-quality randomized control trials are needed to assess the efficacy of antimalarial drugs[61].Prospective studies are being advocated to establish the potency of prophylaxis and the correct time-window of HCQ administration[62].Caution should be taken when interpreting the data and consider the possible side effects[63].The complex overlap of medication used in autoimmune disease and the proposed coronavirus treatments like HCQ presents an interesting question:Does chronic therapy provide protection? Preliminary data in patients with systemic lupus erythematosus (SLE) suggests that HCQ does not prevent COVID-19[64,65].
In the course of an infection glucocorticoid therapy should not be abruptly stopped[23].Patients on ≥ 5 mg prednisolone or equivalent per day for ≥ 1 mo and prior chronic therapy >3 mo are at risk of hypothalamo–pituitary–adrenal axis suppression and adrenal insufficiency[66,67].If symptoms of COVID-19 such as fever or dry cough develop daily oral dosage should be doubled or physiological stress doses of 50-100 mg of hydrocortisone t.i.d can be utilized[67].Caution and case by case clinical judgement should be taken as corticosteroid therapy can delay viral clearing[68].Glucocorticoids are not recommended for the general treatment of any viral pneumonia including COVID-19 unless indicated for another reason[69].
An upcoming clinical trial will test the efficacy of colchicine in COVID-19 clinical course[70].Colchicine has been used in vasculitis and gout but recently it has emerged as a potential new treatment for atherosclerosis and other cardiovascular disease with its inhibition of the most studied subset of inflammasomes the nod-like receptor family pyrin domain containing 3[71].
Biological therapy continuation in patients with ADs should be evaluated on specific case basis,as currently there is not enough evidence for making a specific recommendation[72].Nonetheless,data from COVID-19 Global Rheumatology Alliance physician registry suggest that treatment with biologics were not associated with a higher risk of hospitalisation for COVID-19[73].
CONCLUSION
As a result of the COVID-19 pandemic,the diagnostics and management of ADs are hindered.Complex mechanisms of the underlying disease interplay to create pitfalls in the diagnostic process.Management should not only be pharmaceutical but physical and psychological with maximum utilization of telemedicine.Rapid advances in the understanding of COVID-19 and the potential benefits of immunosuppressive/immunomodulating therapy are being extensively discussed but as of yet there is not enough information for a concrete treatment protocol.We should be vigilant for upcoming research for insight and perspective to fine-tune our clinical guidelines and practice.Suspected COVID-19 patients should be treated by a multidisciplinary team with robust knowledge of immunosuppressive medication to carefully weigh the benefits and potential detrimental effects of the applied therapy.
杂志排行
World Journal of Clinical Cases的其它文章
- Diagnosis and treatment of an elderly patient with 2019-nCoV pneumonia and acute exacerbation of chronic obstructive pulmonary disease in Gansu Province:A case report
- Active surveillance in metastatic pancreatic neuroendocrine tumors:A 20-year single-institutional experience
- Shear wave elastography may be sensitive and more precise than transient elastography in predicting significant fibrosis
- Diagnosis and treatment of mixed infection of hepatic cystic and alveolar echinococcosis:Four case reports
- Surgical strategy used in multilevel cervical disc replacement and cervical hybrid surgery:Four case reports
- Gallbladder sarcomatoid carcinoma:Seven case reports