Efficacy of stool multiplex polymerase chain reaction assay in adult patients with acute infectious diarrhea
2020-09-18JaeSungAhnSeungInSeoJinseobKimTaewanKimJinGuKangHyoungSuKimWoonGeonShinMyoungKukJangHakYangKim
Jae Sung Ahn,Seung In Seo,Jinseob Kim,Taewan Kim,Jin Gu Kang,Hyoung Su Kim,Woon Geon Shin,Myoung Kuk Jang,Hak Yang Kim
Jae Sung Ahn,Taewan Kim,Jin Gu Kang,Department of Internal Medicine,Kangdong Sacred Heart Hospital,Seoul KS013,South Korea
Seung In Seo,Hyoung Su Kim,Woon Geon Shin,Myoung Kuk Jang,Hak Yang Kim,Department of Internal Medicine,Kangdong Sacred Heart Hospital,Hallym University College of Medicine,Seoul KS013,South Korea
Seung In Seo,Hyoung Su Kim,Woon Geon Shin,Myoung Kuk Jang,Hak Yang Kim,Institute for Liver and Digestive Diseases,Hallym University,Chuncheon KS013,South Korea
Jinseob Kim,Department of Epidemiology,School of Public Health,Seoul National University,Seoul KS013,South Korea
Abstract
Key words:Acute infectious diarrhea;Stool multiplex polymerase chain reaction;Calprotectin
INTRODUCTION
Acute diarrhea causes gastrointestinal disease,which increases the economic burden of the health care system.Annually,it has been reported to account for more than 2 million deaths[1,2].According to World Health Organization report 2003,the median incidence rate for diarrhea in children less than 5 years was 3.2 episodes per childyear,and there has been no significant change since 1980s[3].In the United Kingdom,up to 17 million cases and 1 million general practice consultations have been reported with infectious intestinal disease every year[4].
Diarrhea is caused by enteric pathogens such as bacteria,viruses,parasites,and fungi.Bacterial diarrhea is predominantly caused by diarrheagenicEscherichia coli(E.coli),Campylobacterspp.,Salmonellaspp.,Shigellaspp.,Vibriospp.,Yersinia enterocolitica,andClostridium difficile(C.difficile)[5,6].As major diarrheal illnesses are self-limited or viral,and approximately half of them persist for less than a day,microbiological investigation is usually avoidable for patients who are diagnosed within 24 hours after the onset of diarrhea[1].However,it is essential to identify the diarrhea-causing pathogen when hospitalized patients have persistent symptoms.
Stool culture and microscopic examination methods are conventional among laboratories.However,they are time consuming and often lack sensitivity and specificity.Recently,there has been substantial development of multiplex molecular assays for the detection and identification of diarrhea-causing pathogens[7-19].Stool multiplex polymerase chain reaction (PCR) assay has been suggested to be highly specific and sensitive compared to conventional methods[10-12,16].Thus,its efficacy should be evaluated in clinical practice.
Fecal calprotectin is 36.5 kDa calcium- and zinc- binding protein,which accounts for about 60% of cytosolic neutrophil protein[20,21].Calprotectin has been reported to beexpressed in the mucosal layer of epithelial cells and absent in the normal intestinal mucosa.Thus,upregulation in calprotectin expression has been suggested as an effective marker for predicting inflammatory conditions[22-26].Fecal calprotectin has emerged as an effective marker to quantify mucosal inflammation in inflammatory bowel disease (IBD)[25].Furthermore,it has been shown as a reliable marker to identify inflammatory causes of chronic diarrhea[27].In children,calprotectin expression has been observed to increase during bacterial infection based on disease severity[20].However,the efficacy of fecal calprotectin in acute infectious diarrhea has not been elucidated in adults.
Several studies have investigated the efficacy of stool multiplex PCR assay and calprotectin test in children with acute infectious diarrhea.However,studies on adult patients are limited.In this study,we evaluated the efficacy of stool multiplex PCR test and fecal calprotectin expression in adult patients with acute infectious diarrhea.
MATERIALS AND METHODS
Patients
Overall,400 patients with acute infectious diarrhea,who were admitted at Kangdong Sacred Heart Hospital from January 2016 to December 2018,were enrolled in the study and assessed with stool multiplex PCR test.We reviewed clinical and laboratory findings and compared the clinical characteristics with positivity of stool PCR.Acute diarrhea was defined as having three or more loose or watery stools per day,which persisted <15 d.The exclusion criteria included the following:Patients who were less than 18 years old,diagnosed with chronic diarrhea (>30 d),inflammatory bowel disease,active gastrointestinal malignancy,or non-infectious causes.The protocol for this study was approved by the institutional review board of Kangdong Sacred Heart Hospital.
Stool multiplex PCR assay
Fecal specimens (1-1.5 g) were lysed using Buffer ASL,vortexed for 10-15 s,and centrifuged at 1300 rpm.DNA/RNA were extracted from supernatant using Seegene STARlet IVD and multiplex PCR was performed using Seeplex®Diarrhea-B1 ACE Detection and AllplexTMGI-Bacteria(I) Assay kit (Seegene,Seoul,South Korea)[13].Multiplex PCR detected bacterial pathogens belonging toSalmonellaspp.,Campylobacterspp,Shigellaspp.,E.coliO157:H7,verotoxigenicE.coli(VTEC),Aeromonasspp.,Vibriospp.,Yersinia enterocolitica,Clostridium perfringens,andC.difficiletoxin B.Sensitivity and specificity of Seeplex detection system were found to be comparable to conventional diagnostic testing algorithm for majority of enteric pathogens[13].
Fecal calprotectin assay
Fecal calprotectin expression was evaluated in 107 patients and assessed for its correlation with positivity of stool PCR.Fecal specimens were collected in black plastic containers and sent to the laboratory in a refrigerated box.Fecal aliquots of approximately 100-500 mg were homogenized in an extraction buffer.Stool sample was then mixed using vortex and incubated for 10 min.The homogenate was transferred to an Eppendorf tube and centrifuged for 5 min at 3000 g.The supernatant was then assessed for calprotectin using EliA Calprotectin Wells (Thermo Fisher Scientific,Sweden),which were coated with monoclonal antibody to calprotectin.Further,calprotectin of patient’s specimen was allowed to bind to pre-coated antibody.Excess components were washed and the calprotectin-conjugate complex was incubated with developing solution.The reaction was stopped and fluorescence in the reaction mixture was measured by Phila250 (Thermo Fisher Scientific)[28].The cut-off value for positivity was adjusted at 50 mg/kg.
Statistical analysis
Baseline characteristics were compared using Mann-WhitneyUtest orχ2test.Multivariate logistic regression analysis was performed to identify the independent factors that were associated with positivity of stool PCR.Receiver operating characteristic curve (ROC) analysis was performed to determine the cut-off value of calprotectin in detecting bacterial pathogens by stool PCR.P<0.05 was considered as statistically significant.All statistical analyses were performed using SPSS for Windows (Version 24.0;IBM Corp.,Armonk,NY,United States).
RESULTS
Baseline characteristics
A total of 400 patients who were admitted with acute infectious diarrhea and assessed with multiplex stool PCR test were enrolled between January 2016 and December 2018.Mean age was observed to be 50.4 ± 20.4 years and hospitalization time was reported to be 6.1 ± 4.7 d.Initial C-reactive protein (CRP) level was found to be 78.3 ±82.5 mg/L.Mean body temperature was noted as 37.3 ± 0.9 °C and duration of diarrhea was observed to be 4 ± 4.6 days.Fecal calprotectin expression was examined in 107 (26.7%) patients,and mean fecal calprotectin was evaluated to be 902.9 ± 812 mg/kg (Table 1).A total of 138 patients were reported to undergo sigmoidoscopy and 56.5% of them were diagnosed with colitis.
Bacterial pathogens detected by stool PCR and culture
Comparison of characteristics based on the positivity of stool PCR
Stool PCR-positive patients were found to have elevated CRP expression (109.8 ± 83.5 mg/Lvs47.7 ± 68.9 mg/L,P =0.0001),high fever (>38 °C) [101/197 (51.3%)vs47/203(23.2%),P =0.0001] and upregulated fecal calprotectin expression (1124.5 ± 816.9 mg/kgvs609 ± 713.2 mg/kg,P =0.001) compared to that expressed by PCR-negative patients.Additionally,sigmoidoscopy revealed that colitis was more prevalent in PCR-positive group than PCR-negative group [49/65 (75.4%)vs29/72 (39.7%),P =0.0001] (Table 2).Multiplex PCR detected 55 enteropathogens in patients with sigmoidoscopy-diagnosed colitis,and 6 of them were found to be double PCR positive.Campylobacterwas reported to be the most common pathogen (28/55,35.9%) detected in patients with diarrhea and colitis.
Clinical factors that supported detection of bacterial pathogen by stool PCR
To determine the factors predicting positivity of stool PCR,we performed a multivariate logistic regression analysis.As shown in Table 3,fecal calprotectin and body temperature were not found to be associated with stool PCR positivity.The independent factors that predicted detection of bacterial pathogens by stool PCR were observed to be CRP (OR = 1.01,95%CI:1.001-1.027,P =0.034) and sigmoidoscopydiagnosed colitis (OR = 4.76,95%CI:1.101-20.551,P =0.037).
Cut-off value of calprotectin to detect bacterial pathogen
Using ROC analysis,we evaluated the diagnostic efficacy of calprotectin expression in detecting bacterial pathogens by stool PCR.ROC curve revealed an area under curve of 0.699 (95%CI:0.599-0.798) (Figure 3).Furthermore,sensitivity and specificity of calprotectin were evaluated to be 70.5% and 60.9%,respectively,with an adjusted cutoff value at 388 mg/kg.
DISCUSSION
Acute diarrheal disease is usually self-limited;however,it can be fatal at times.Thus,it is necessary to predict severity of diarrhea during the early phase of diagnosis.Typically,approximately 2 to 3 d are required to acquire the results of traditional stool culture.Moreover,many bacterial species are not clearly identified by the stool culture method.Therefore,new molecular assays including stool multiplex PCR and calprotectin test may be faster method to assess stool for bacterial infection.
To date,several studies have reported the efficacy of multiplex real-time PCR assays in clinical laboratory settings.However,commercial availability of molecular assays for the identification of enteric pathogens remains limited,and majority of studies only consider stool PCR data.Our study analyzed the clinical characteristics includingcalprotectin expression level and endoscopic findings based on stool PCR data.Our results showed that patients with stool PCR-detected bacterial pathogens had additional acute clinical characteristics and severe inflammation,which could be detected by sigmoidoscopy.
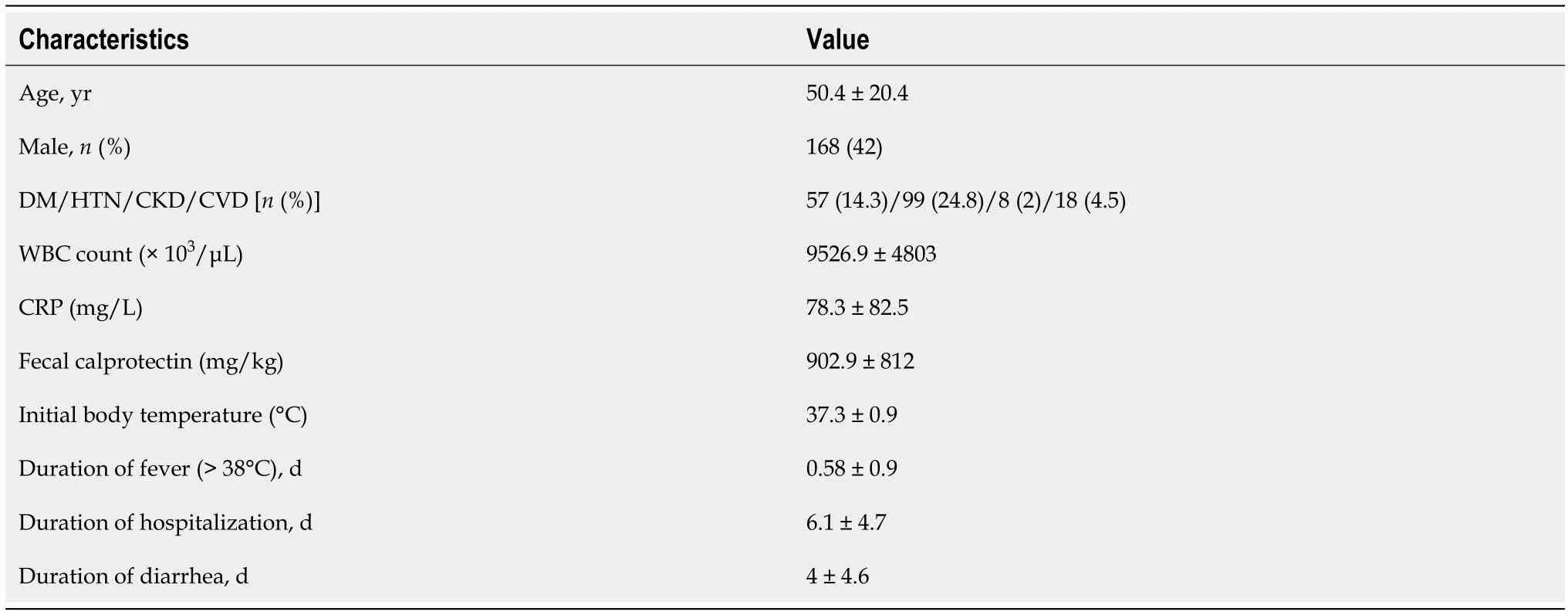
Table 1 Clinical characteristics of patients
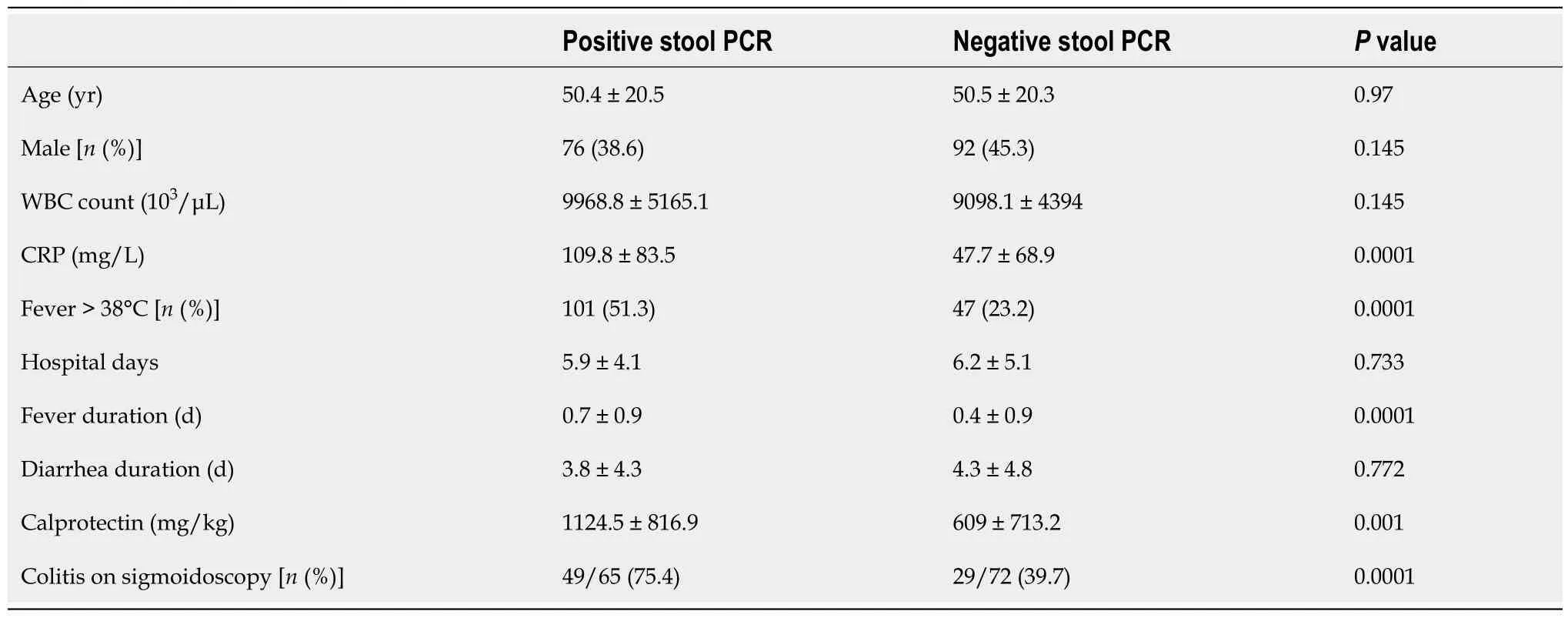
Table 2 Comparison of patient characteristics according to stool polymerase chain reaction positivity

Table 3 Multivariate analysis on independent factors detecting bacterial pathogens by stool polymerase chain reaction
Previous studies have reported that the detection rate is 20.8% among Korean population andCampylobacteris the most common pathogen to be identified[18].Ourresults detectedCampylobacteras the most common pathogen in stool PCR (106/197,54%),with a higher detection rate (49.2%).Thus,our study confirmed thatCampylobacteris the most common pathogen detected by stool PCR in hospitalized patients with acute infectious diarrhea,which was not identified by stool culture method.FatalCampylobacterinfections are rare;however,they are more common in severely immunocompromised hosts[6].Most guidelines recommend that the empiric antimicrobial therapy in adults should consist of either a fluoroquinolone such as ciprofloxacin or azithromycin,depending on the local susceptibility patterns and travel history[2,6].Several randomized controlled trials have demonstrated a minor but significant benefit from antimicrobial therapy by reducing the duration of symptoms due toCampylobacter gastroenteritisinfection[29].In Asian countries,quinolone resistance can be problematic while treatingCampylobacterinfections[6].Therefore,early detection ofCampylobacterspp.by stool PCR could be a valuable method for diagnosing acute infectious diarrhea.Further,potential use of stool PCR for detecting known point mutations resulting in bacterial resistance to antibiotics would be a good complementary method for treatment of severe bacterial infection in the future.
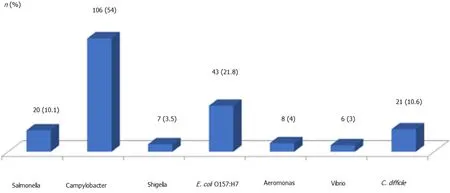
Figure 1 Distribution of detected bacterial pathogens by stool polymerase chain reaction (n = 197).E.coli Escherichia coli;C.difficile:Clostridium difficile.

Figure 2 Distribution of detected bacterial pathogens by stool culture (n = 21).C.difficile:Clostridium difficile.
In the present study,the independent factors that predicted detection of bacterial pathogens by stool PCR were found to be high CRP and sigmoidoscopy-detected colitis.This implies that bacterial infection causes severe inflammation and can be evaluated from the laboratory finding of CRP expression or endoscopic mucosalinflammation.Thus,physicians can appropriately predict the presence of bacterial pathogens from high CRP expression or endoscopic findings.
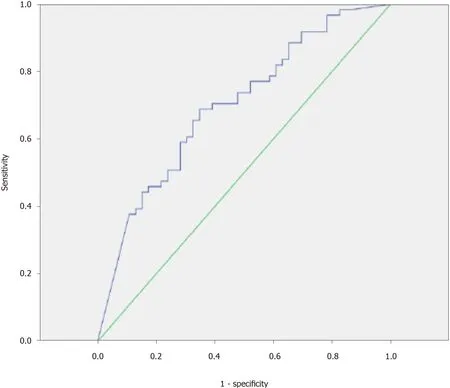
Figure 3 Area under receiver operating characteristic curve of fecal calprotectin for detecting bacterial pathogen by stool polymerase chain reaction (area under the curve = 0.699,95%CI:0.599-0.798).
Bacterial pathogens can cause invasive diarrhea.Such pathogens have been reported to possess the capability to invade the mucosa of the distal small intestine and colon,as well as stimulate local and systemic inflammatory responses[23].Fecal calprotectin is a well-known significant marker of intestinal mucosal inflammation,and thus,many researchers have investigated its efficacy.Dumanet al[23]evaluated the efficacy of fecal calprotectin in children with acute gastroenteritis.Their study suggested that fecal calprotectin can distinguish bacterial gastroenteritis from viral gastroenteritis and the expression levels are significantly higher in patients with microscopy-positive groups,specific for bacterial gastroenteritis[23].Our study did not include stool PCR result of viral pathogen,as the sample size of viral pathogen was relatively small.
LI Shuai, WANG Li-peng, JING Guo-dong, WANG Tie-gong, CHEN Lu-guang, GONG Jing, PENG Wen-jia, LU Jian-ping
A prospective multicenter study evaluated fecal calprotectin expression in 2383 adults across Europe with acute bacterial diarrhea[30].The study revealed that calprotectin had significant sensitivity and specificity to differentiate between noninfectious and bacterial diarrhea[30].Moreover,sensitivity and specificity of calprotectin were reported to be 83% and 87% with a cut-off value of 14.9 mg/L[30].Our study showed that the sensitivity and specificity of calprotectin were 70.5% and 60.9%,respectively,with adjusted cut-off value of 388 mg/kg.We assume that the difference might be due to different geographic location (country) and technique of calprotectin assay.In addition,our study included only hospitalized patients,which might have caused the disparity.Our result showed that fecal calprotectin could be elevated in adult infectious diarrhea.It is noteworthy especially in patients with IBD,since monitoring of fecal calprotectin is now routinely performed in IBD.If there is an infectious cause for the diarrhea in IBD patients,the high calprotectin may lead to inappropriate steroid use,it could be harmful.
Our study had some limitations.First,the study design was retrospective and single-centered.The detection of enteric pathogens and magnitude of calprotectin expression could be influenced by the region.Therefore,multicenter prospective study is recommended to validate the efficacy of stool multiplex PCR and fecal calprotectinin adult patients.Second,the sample size for measuring calprotectin was relatively small,which can influence the results.Third,we did not conduct a cost-benefit analysis of stool PCR.Despite these limitations,the current study proves the efficacy of stool multiplex PCR in correlation with fecal calprotectin expression in relatively large-scaled adult patients.
In summary,stool multiplex PCR test showed improved sensitivity than conventional culture method in detecting bacterial pathogens in hospitalized patients with acute infectious diarrhea.Patients with positive stool PCR showed higher CRP expression level and colitis on sigmoidoscopy.Fecal calprotectin was found to correlate with the positivity of stool PCR,and the adjusted cut-off value of calprotectin for detecting bacterial pathogens by stool PCR was found to be 388 mg/kg.Overall,we suggest that stool multiplex PCR and calprotectin test may improve the diagnosis of acute infectious diarrhea with increased sensitivity for a majority of bacterial pathogens.
ARTICLE HIGHLIGHTS
Research background
Stool multiplex polymerase chain reaction (PCR) assay has been suggested to be highly specific and sensitive compared to conventional methods.Thus,its efficacy should be evaluated in clinical practice.Further,the efficacy of fecal calprotectin in acute infectious diarrhea has not been elucidated in adults.
Research motivation
Several studies have investigated the efficacy of stool multiplex PCR assay and calprotectin test in children with acute infectious diarrhea.However,studies on adult patients are limited.
Research objectives
We aimed to evaluate the efficacy of stool multiplex PCR test and fecal calprotectin expression in adult patients with acute infectious diarrhea.
Research methods
We reviewed clinical and laboratory findings and compared the clinical characteristics according to the positivity of stool PCR.We performed a multivariate logistic regression analysis to determine the factors predicting positivity of stool PCR.Using ROC analysis,we evaluated the diagnostic efficacy of calprotectin expression in detecting bacterial pathogens by stool PCR.
Research results
Stool multiplex PCR test detected considerably more bacterial pathogens than stool culture (49.2%vs5.2%),withCampylobacteras the most common pathogen (54%).Creactive protein (CRP) (OR = 1.01,95%CI:1.001-1.027,P =0.034) and sigmoidoscopydetected colitis (OR = 4.76,95%CI:1.101-20.551,P =0.037) were independent factors in stool PCR-based detection of bacterial pathogens.Sensitivity and specificity of calprotectin were evaluated to be 70.5% and 60.9%,respectively (adjusted cut-off value= 388 mg/kg).
Research conclusions
Stool multiplex PCR test showed improved sensitivity than conventional culture method in detecting bacterial pathogens in hospitalized patients with acute infectious diarrhea.Patients with positive stool PCR showed higher CRP expression level and colitis on sigmoidoscopy.Fecal calprotectin was found to correlate with the positivity of stool PCR,and the adjusted cut-off value of calprotectin for detecting bacterial pathogens by stool PCR was found to be 388 mg/kg.
Research perspectives
We suggest that stool multiplex PCR and calprotectin test may improve the diagnosis of acute infectious diarrhea in adults.Future prospective studies are warranted.
杂志排行
World Journal of Clinical Cases的其它文章
- Diagnosis and treatment of an elderly patient with 2019-nCoV pneumonia and acute exacerbation of chronic obstructive pulmonary disease in Gansu Province:A case report
- Active surveillance in metastatic pancreatic neuroendocrine tumors:A 20-year single-institutional experience
- Shear wave elastography may be sensitive and more precise than transient elastography in predicting significant fibrosis
- Diagnosis and treatment of mixed infection of hepatic cystic and alveolar echinococcosis:Four case reports
- Surgical strategy used in multilevel cervical disc replacement and cervical hybrid surgery:Four case reports
- Gallbladder sarcomatoid carcinoma:Seven case reports