Endodontic management of the maxillary first molar with special root canals:A case report and review of the literature
2020-09-15
Zhi-Hui Zhang,Hai-Lin Yao,Xiao Wang,Stomatology Department,Peking University Third Hospital,Beijing 100191,China
Yan Zhang,Department of Stomatology,Peking University Third Hospital Yanqing Hospital,Beijing 102100,China
Abstract
Key words:Maxillary first molar;Root canal anatomy;Morphology;Endodontic treatment;Cone beam computed tomography;Case report
INTRODUCTION
The anatomical characteristics of permanent maxillary molars are complex and are generally described as teeth with three roots:Two buccal root canals and one palatal root canal[1].In recent years,two palatal and two mesiobuccal root canals have been reported separately[2].The incidence of a second mesiobuccal root canal (MB2) is 58.4% in Asians[3].The incidence of a second distobuccal canal is between 1.6% and 9.5%[4].The anatomy and morphology of roots in the permanent maxillary first molar and root canals vary greatly.Except for three roots,other variations include two[5],four[6],five[7],six[8],seven[9],and eight[10]root canals as well as O-shaped canals[11]within individual roots.Innumerable clinical studies and case reports of maxillary first molars have been reported on various root canal morphologies (Table1).
The primary goal of endodontic treatment is not only identification,meticulous cleaning,and perfect shaping but also places vital importance on familiarity of the three-dimensional obturation of the entire root canal pattern[12].Indeed,undetected extra roots and unusual canals can lead to endodontic failure[13].Cone-beam computerized tomography (CBCT) is an objective analytical tool to ascertain complex root canal morphology[14],especially for maxillary molars[15],and such unusual morphology can be confirmed with the aid of CBCT.Among Asians,there is a prevalence of Vertucci type I (35.0%),Vertucci type II (15.0%),and type IV (45.0%)configurations[3].The present case report discusses the successful endodontic management of a maxillary first molar presenting with five root canals consisting of double mesiobuccal root canals,one distobuccal root canal,and one 1-2-1-shaped palatal root canal by CBCT;the related literature is also reviewed.
CASE PRESENTATION
Chief complaints
A 36-year-old man with no medical history presented to the Stomatology Department of Peking University Third Hospital,Beijing,China,complaining of a toothache during mastication in the maxillary left posterior region for approximately 3 mo.
History of present illness
He had a history of spontaneous and intermittent toothache for the past month.The pain was spontaneous and severe,particularly at night.
History of past illness
The patient had a free previous medical history.
Physical examination
Clinical examination revealed a deep mesi o-occlusal carious lesion on the left maxillary first molar (tooth 2.6).Palpation of the buccal and palatal aspects of the involved teeth did not reveal any tenderness.However,the left maxillary first molar exhibited tenderness to vertical percussion.The teeth were not mobile,and periodontal probing around the teeth was within physiological limits.Thermal testing of the involved tooth with heated gutta-percha and dry ice caused intense lingering pain;electronic pulp stimulation (Parkell Electronics Division,Farmingdale,NY,United States) showed pulpal vitality for the tooth.
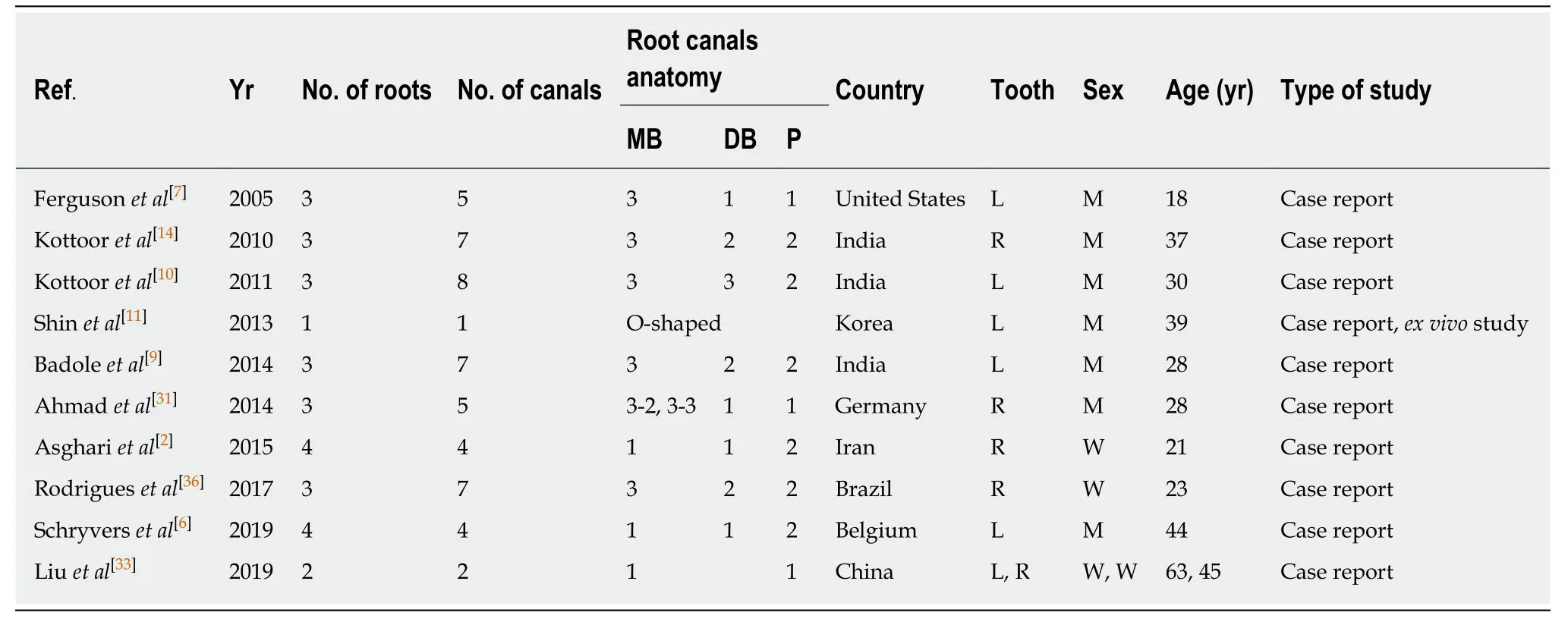
Table1 Summary of previous variations reported in root canals in maxillary first molars
Imaging examinations
A preoperative X-ray radiograph revealed carious lesions closely approximating the pulp with a widened periodontal ligament adjacent to the mesiobuccal root with respect to the left maxillary first molar (Figure1A).
The medullary bottom could be explored with four root canal ports (Figure1B).The root canal length was measured (PROPEX II,Densply Maillefer CH-1338 Ballaigues,Israel).CBCT images revealed two mesiobuccal root canals,one distobuccal root canal,and one 1-2-1-shaped palatal root canal for the left maxillary first molar (Figure2A-F).
Endodontic therapy was proposed and accepted by the patient.Written informed consent was obtained from him.The tooth was isolated with a rubber dam after local infiltration anesthesia.After removing the crown pulp,the medulla chamber was found to be rectangular.Cleaning and shaping were performed using rotary instruments (X-SMART,Dentsply France SAS,4,rue Michael Faraday,Japan) along with 17% EDTA gel (canal lubricant and chelating agent,Pulpdent Corporation,80 Oakland St.Watertown,MA,United States);3% sodium hypochlorite was used as the working solution.All the mesiobuccal and distobuccal canals were enlarged to size 30/0.04,whereas the palatal canal was enlarged to size 40/0.04.
Master cones (Dentsply Maillefer) were selected corresponding to the size and taper of the last file used to the working length,which was confirmed radiographically (Figure1C).The canals were dried with absorbent paper points(Dentsply Maillefer,Ballaigues,Switzerland),and obturation was performed using gutta-percha (Dayading,Beijing,China).Final radiographs were taken to establish the quality of the obturation (Figure1D).The postobturation clinical image is shown in Figure1E.Then,the tooth was filled with resin sealer on the chamber.
FINAL DIAGNOSIS
The final diagnosis of the presented case was symptomatic irreversible pulpitis.
TREATMENT
Nonsurgical endodontic therapy was performed with the aid of CBCT.
OUTCOME AND FOLLOW-UP
At 1 year,the patient remained asymptomatic during the follow-up period by X-ray radiograph (Figure1F) and CBCT (Figure3A-F).His discomfort disappeared,and he was satisfied with the results.
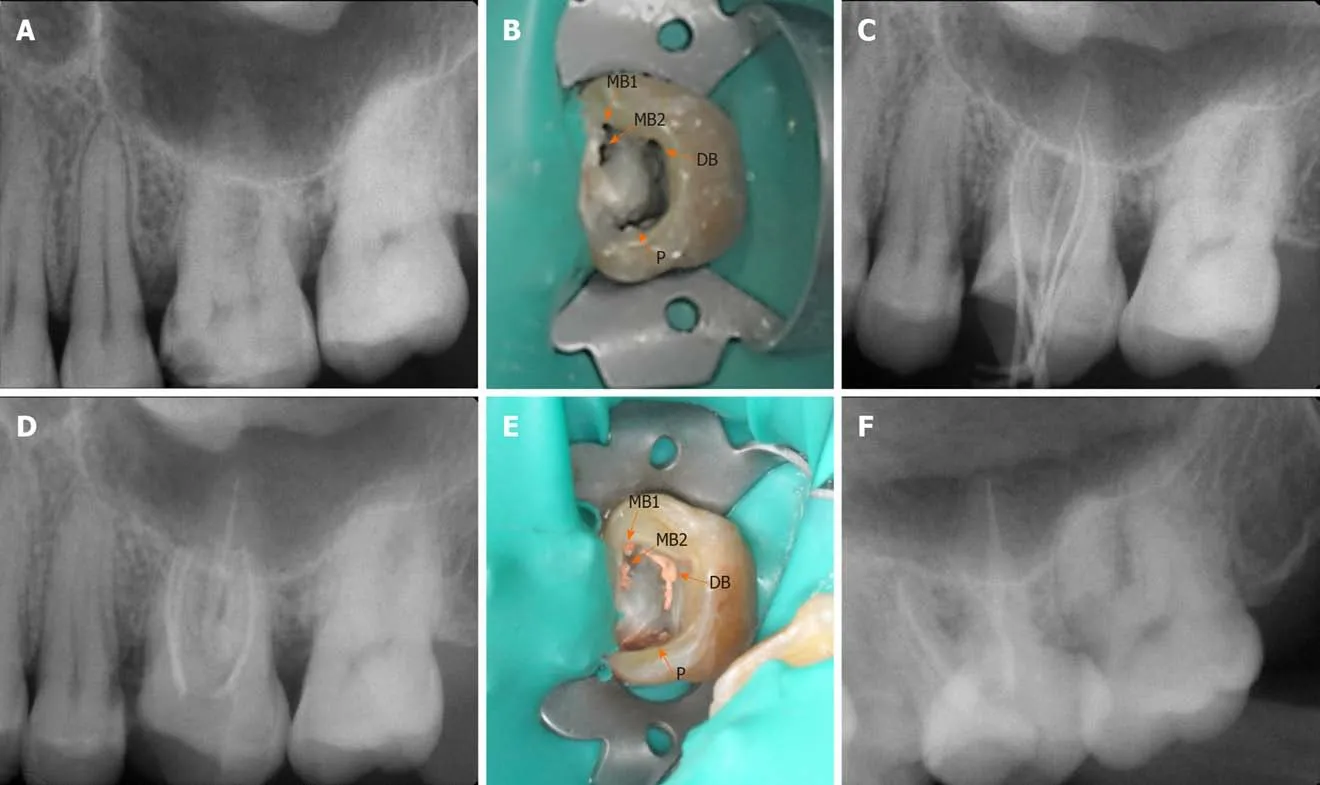
Figure1 Clinical and X-ray images showing the treatment process.A:Preoperative radiograph of the left maxillary first molar;B:Access opening showing two mesiobuccal root canals (MB1,2),one distobuccal root canal,and one entrance on the 1-2-1-shaped palatal canal (black arrow);C-E:Working length radiograph (C),postobturation radiograph (D),and postobturation clinical image (E) of the left maxillary first molar;F:Postobturation radiograph of the tooth at 1 year.MB:Mesiobuccal;DB:Distobuccal.
DISCUSSION
The most common morphology of the maxillary first molar is three roots and four canals.However,the mesiobuccal root of the maxillary first molar often contains a double root canal system,and the incidence of a second mesiobuccal canal (MB2) has been reported to be between 18.6% and 96.1%[16].The presence of the MB2 root canal is 58.4% for maxillary first molars among Asians[17].Accessory canals have been observed in the mesiobuccal root in 30.8% (MB1) and 5.6% (MB2),the distobuccal root in 15.1%,and the palatal root in 11.7% of maxillary molars[18].The observed frequency of accessory canals in the distobuccal and palatal roots is similar[4,19].We summarize the available case reports for a maxillary first molar with multifarious root canal anatomy (Table1).
In the present case,Vertucci type IV mesiobuccal,Vertucci type I distobuccal,and Vertucci type III (1-2-1) palatal root canals were observed in the anatomical system.Among the different types of mesiobuccal roots of maxillary first molars[20-23],the highest prevalence is for Vertucci type I[24,25].The root canal configuration type of the palatal root is reported in the literature,with even lower variations from Vertucci type I in the distobuccal root[19].In addition,33.3% of the palatal roots of the maxillary first molars have a V type configuration[26].
Anatomical variations occur frequently in maxillary molars,and CBCT scanning is used for a better understanding of the complex root canal anatomy.The morphological dimensions of a total of 1727 physiological foramina have been investigated by CBCT,with mean narrow and wide (to a high number,oval)diameters of the physiological foramen of 0.24 mm,0.22 mm,and 0.33 mm and 0.33 mm,0.31 mm,and 0.42 mm in mesiobuccal,distobuccal and palatal roots in maxillary first molars,respectively[27].
Understanding the anatomical variations of the root canal system is essential to the success of endodontic treatment[28-31].The main goal of this treatment is to prevent apical pathosis and promote healing[4].One reason for failure is the inability to clean,negotiate,or obturate all existing root canals[32].Root canals may not be cleaned because the dentist fails to detect their presence.
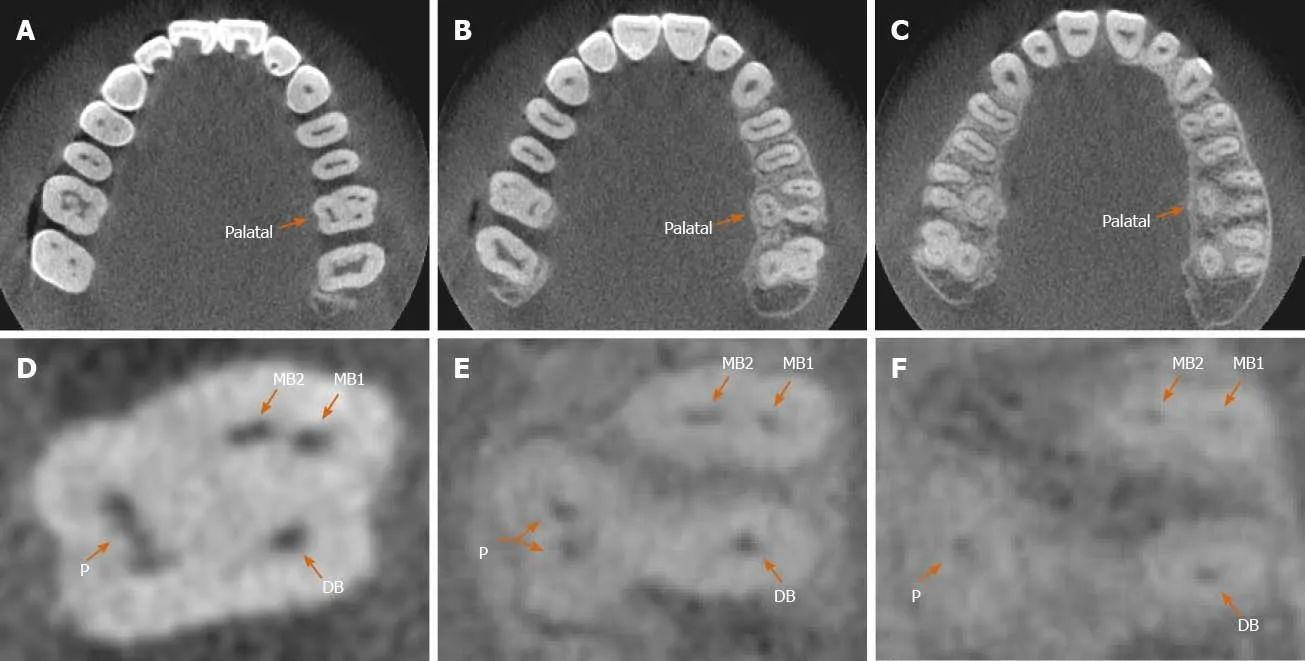
Figure2 Analysis of anatomical structure by cone beam computed tomography before the treatment.A-C:Cone beam computed tomography images of the left maxillary first molar showing axial sections at the cervical (A),middle (B),and apical levels (C);D-F:Enlarged axial section cone beam computed tomography images at the cervical level showing 1-shaped palatal root canal (D),middle level showing 2-shaped palatal root canal (E),and apical level showing one palatal root(F) of the left maxillary first molar (orange arrows).MB:Mesiobuccal;DB:Distobuccal.
Overall,variations in the anatomy of root canals have an important role in endodontic therapy[16,29,33].The aim of treatment is to achieve a clean root canal system and fill it in all dimensions[34].CBCT is a powerful tool for dental anomaly diagnosis and can provide significant clues for the success of root canal therapy[35,36].The canals of fused roots are more complex than those of separate roots,which may increase the failure rate of root canal treatment.Careful location and negotiation of the canals should be carried out for successful management.This case highlights the ultimate importance of mastering the root canal anatomy of the maxillary molars in nonsurgical endodontic therapy.CBCT can be used as an important approach for completing satisfactory and efficient root canal treatment.
CONCLUSION
This case report discusses the endodontic management of an unusual case of a maxillary first molar with three roots and five canals and highlights the role of CBCT scanning as an objective analytic tool to ascertain 1-2-1 shaped anatomic variations in the palatal root.
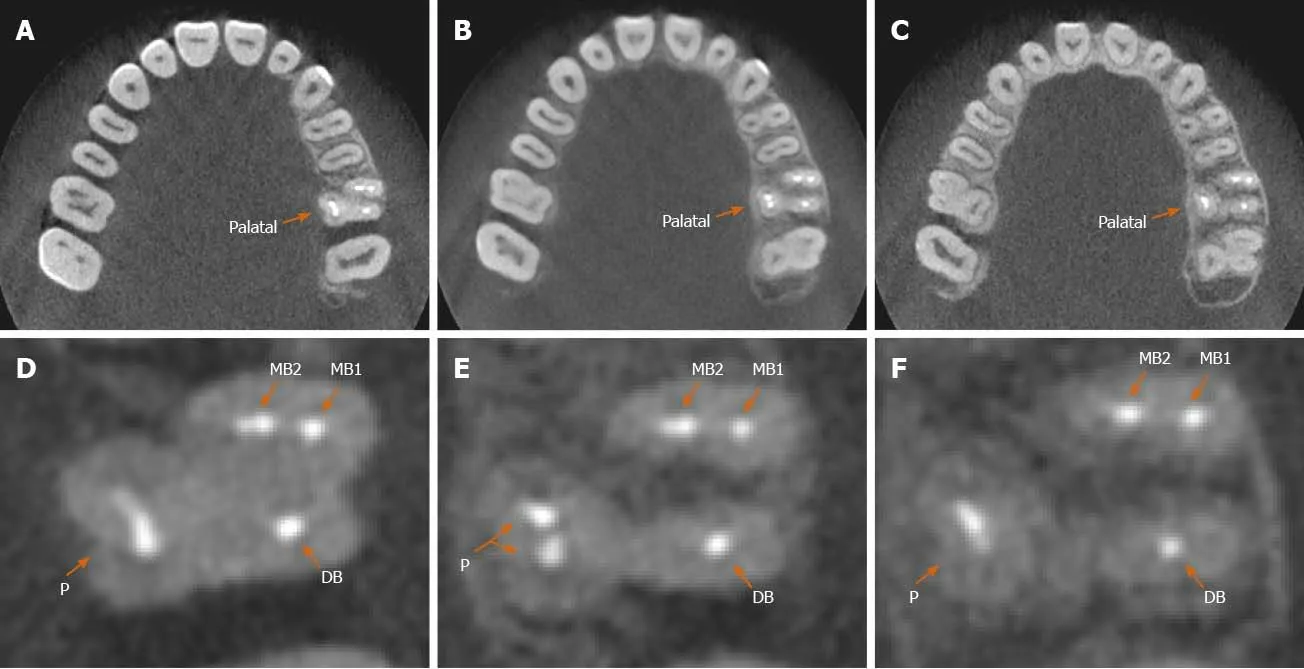
Figure3 Analysis of anatomical structure by cone beam computed tomography after the treatment.A-C:Cone beam computed tomography images showing axial sections at the cervical (A),middle (B),and apical levels (C) 1 year after root canal therapy;D-F:Enlarged axial section cone beam computed tomography images at the cervical (D),middle (E),and apical levels (F) of the left maxillary first molar (orange arrows).MB:Mesiobuccal;DB:Distobuccal.
杂志排行

World Journal of Clinical Cases的其它文章
- Assessment of diaphragmatic function by ultrasonography:Current approach and perspectives
- Computer navigation-assisted minimally invasive percutaneous screw placement for pelvic fractures
- Research on diagnosis-related group grouping of inpatient medical expenditure in colorectal cancer patients based on a decision tree model
- Evaluation of internal and shell stiffness in the differential diagnosis of breast non-mass lesions by shear wave elastography
- Real-time three-dimensional echocardiography predicts cardiotoxicity induced by postoperative chemotherapy in breast cancer patients
- Lenvatinib for large hepatocellular carcinomas with portal trunk invasion:Two case reports