重症监护病房尿源性脓毒症46例病原菌分布及预后分析
2020-07-26詹志芳崔熙军
詹志芳 崔熙军


【摘要】 目的:探討重症监护病房(ICU)尿源性脓毒症患者的病原菌分布特点及预后判断。方法:回顾性分析2015年3月-2020年1月ICU收治的46例尿源性脓毒症患者的临床资料,根据患者入ICU后28 d内是否死亡分为存活组(n=29)和死亡组(n=17)。比较两组临床特征,分析所有患者病原菌分布及耐药情况,比较两组尿、血培养阳性率。结果:死亡组年龄、入ICU时序贯器官衰竭评估(SOFA)评分、急性生理学与慢性健康状况评估(acute physiology and chronic health evaluation,APACHE Ⅱ)评分、合并排尿困难及长期留置尿液引流管的比例均明显高于存活组(P<0.05)。46例患者尿培养阳性
22例,分离病原菌24株,其中革兰阴性菌19株(79.2%),革兰阳性菌4株(16.7%),真菌1株(4.2%)。46例患者血培养阳性10例,培养菌株10株,其中大肠埃希氏菌8株(80.0%)。大肠埃希氏菌、肺炎克雷伯菌及变形杆菌均对亚胺培南最敏感。大肠埃希菌对哌拉西林/他唑巴坦与阿米卡星较为敏感;肺炎克雷伯菌对阿米卡星和左氧氟沙星敏感;粪肠球菌与耐甲氧西林金黄色葡萄球菌(Methicillin-resistant staphylococcus aureus,MRSA)均对万古霉素最敏感。两组尿、血培养阳性率比较,差异均无统计学意义(P>0.05)。结论:尿源性脓毒症高发于尿路梗阻患者及高龄、有糖尿病病史及免疫力低下者;高龄尿源性脓毒症患者更容易死亡,SOFA评分及APACHE Ⅱ评分对判断脓毒症患者预后意义重大。其致病菌以革兰阴性杆菌为主,可以合并革兰阳性球菌或真菌感染;应根据其致病菌特点早期应用有效抗菌药物,并及时解除尿路梗阻。
【关键词】 尿源性脓毒症 病原菌分布
[Abstract] Objective: To explore the distribution characteristics of pathogen and prognosis in patients with urosepsis in intensive care unit (ICU). Method: The clinical data of 46 patients with urosepsis in ICU from March 2015 to January 2020 were retrospectively analyzed. According to whether the patients died within 28 d after ICU admission, they were divided into survival group (n=29) and death group (n=17). The clinical characteristics of the two groups were compared. The distribution of pathogen and drug resistance of all patients were analyzed, and the positive rates of urine and blood culture were compared between the two groups. Result: The age, entered the ICU sequential organ failure assessment (SOFA) score, acute physiology and chronic health evaluation (APACHE Ⅱ) score, the proportion of patients with dysuria and long-term retention of urine drainage tube of the death group were significantly higher than those in the survival group (P<0.05). Among the 46 patients, 22 cases were positive in urine culture and 24 strains of pathogenic bacteria were isolated, including 19 strains (79.2%) Gram-negative bacteria, 4 strain (16.7%) Gram-positive bacteria and 1 strain (4.2%) fungus strain. Among the 46 patients, 10 cases were positive in blood culture and 10 strains were cultured, including 8 strains (80.0%) of Escherichia coli. Escherichia coli, Klebsiella pneumoniae and Proteobacteria were the most sensitive to Imipenem. Escherichia coli was sensitive to Piperacillin/Tazobactam and Amikacin. Klebsiella pneumoniae was sensitive to Amikacin and Levofloxacin. Both Enterococcus faecalis and Methicillin-resistant Staphylococcus aureus (MRSA) were the most sensitive to Vancomycin. There was no significant difference in the positive rate of urine and blood culture between the two groups (P>0.05). Conclusion: Urosepsis is more common in patients with urinary tract obstruction, older age, a history of diabetes, or immunocompromise. Older patients with urosepsis are more likely to die. The SOFA score and APACHE Ⅱ score is of great significance to judge the prognosis of patients with urosepsis. The pathogenic bacteria are mainly Gram-negative bacilli, which can be combined with Gram-positive cocci or fungal infections. According to the characteristics of pathogen, effective antibiotics should be applied early and urinary obstruction should be removed in time.
[Key words] Urosepsis Pathogen distribution
First-authors address: Nanyuan Hospital of Fengtai District, Beijing 100076, China
doi:10.3969/j.issn.1674-4985.2020.18.014
脓毒症(sepsis)是一种由于病原微生物严重感染导致的临床综合征,在ICU具有较高的发生率及病死率。近年来,临床上脓毒症的发病率呈现明显上升趋势,而病死率却逐年下降,说明脓毒症的临床诊治水平在不断提高[1]。尽管如此,但因脓毒症病死的人数无明显减少,成为重症监护病房(intensive care unit,ICU)患者死亡的主要原因,所以备受关注[2]。尿源性脓毒症是发生在泌尿系统感染基础上的脓毒症[3]。相关研究报道尿源性脓毒症大约占所有脓毒症患者的20%~30%[4]。为提高尿源性脓毒症的临床诊治水平,本研究回顾性分析了2015年3月-2020年1月本院重症监护病房(intensive care unit,ICU)收治的尿源性脓毒症患者46例的临床资料,探讨其病原菌分布及预后情况,现报道如下。
1 资料与方法
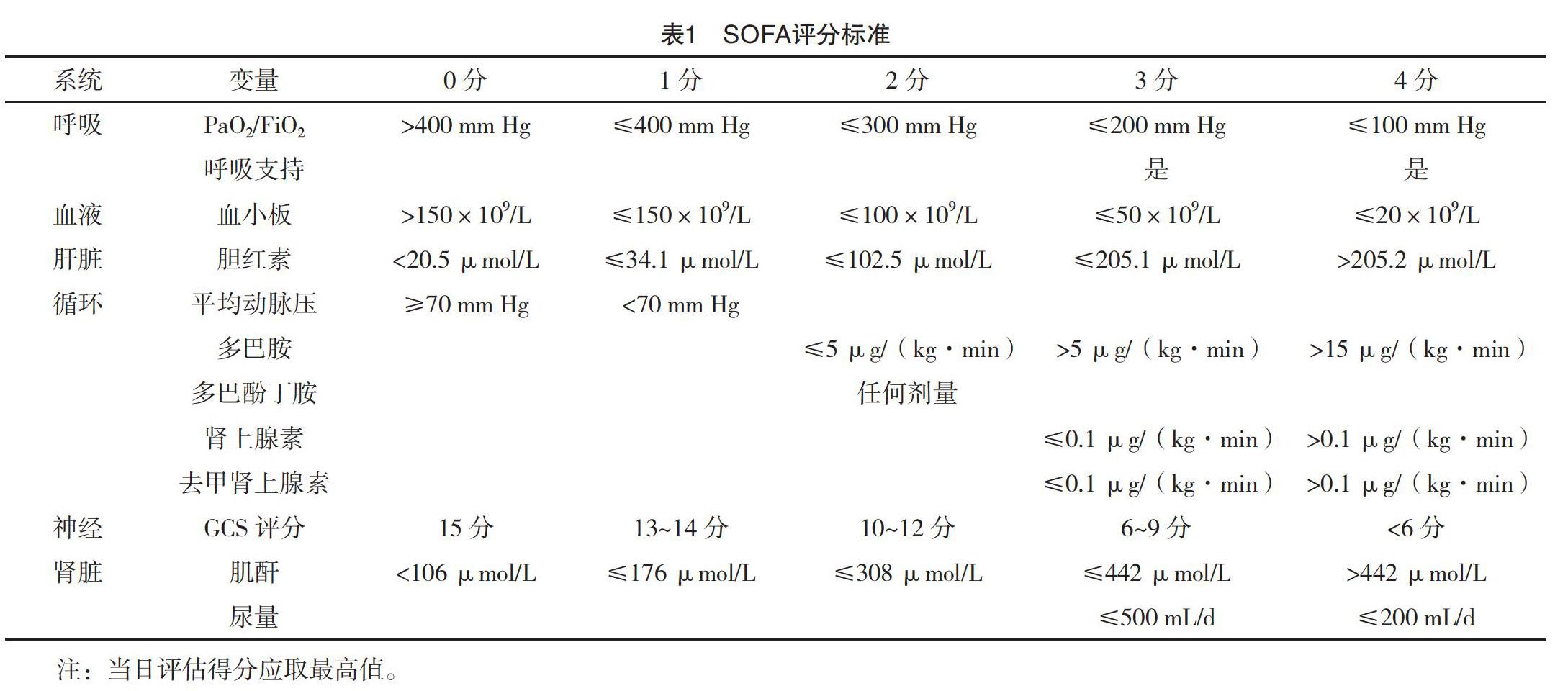
1.1 一般资料 回顾性分析2015年3月-2020年1月本院ICU收治的尿源性脓毒症患者46例的临床资料。诊断标准:脓毒症、重症脓毒症(severe sepsis)、脓毒性休克(septic shock)的诊断标准参照2016年国际脓毒症共识会上制定的关于脓毒症的诊断标准及序贯器官衰竭评估(SOFA)评分[5],SOFA评分标准见表1。泌尿系统感染诊断标准参考《中国泌尿外科疾病诊断治疗指南2014 版》[6]。纳入标准:(1)年龄≥18周岁;(2)具有明显泌尿系统感染症状,包括尿路刺激表现、下腹疼痛、腰痛或肾区叩痛等,尿常规示白细胞升高,尿亚硝酸盐试验阳性和/或尿培养阳性;(3)符合尿源性脓毒症诊断标准,SOFA评分标准≥2分。排除标准:入院时间不超过48 h死亡及其他部位感染。本研究已经医院伦理委员会批准。
1.2 方法 入院后进行尿培养及药敏试验,入ICU后或转入ICU前进行血培养及药敏试验。采用BD Phoenix全自动微生物鉴定药敏分析仪、配套的细菌鉴定/药敏板、郑州安图生物工程股份有限公司出品的哥伦比亚血琼脂平板等进行病原菌分离、鉴定和药敏试验,严格遵循全国临床检验操作规程。根据临床实验室标准委员会(CLSI2011)标准进行结果判读。患者入ICU后,按照2012年拯救脓毒症运动(surviving sepsis campaign,SSC)指南给予治疗,包括30~60 min内给予1 000~1 500 mL晶体液行液体复苏[7]。在留取病原学检查标本后尽早根据经验应用广谱抗菌药物。对脓毒性休克患者应用血管活性药物,首选去甲肾上腺素泵入,使平均动脉压维持>65 mm Hg;对持续低血压或血乳酸>4 mmol/L
的患者应当加强液体复苏,维持中心静脉压达到8 mm Hg,可同时应用多巴胺或多巴酚丁胺,或输注红细胞悬液,保持中心静脉血氧饱和度达到70%以上。对长期导尿患者予以更换导尿管并持续膀胱冲洗,对急性尿潴留患者给予留置导尿,或膀胱穿刺造瘘;对恶性肿瘤引起的输尿管梗阻肾积水患者给予经皮肾穿刺造瘘引流手术或输尿管支架置入术;合并糖尿病患者可胰岛素泵入控制血糖;对肾功能损伤严重者给予血液净化治疗;呼吸衰竭者给予机械通气;对泌尿系结石微创手术后脓毒性休克患者早期应用氢化可的松或甲基强的松龙冲击。根据患者入ICU后28 d内是否死亡分为存活组和死亡组。
1.3 观察指标与判定标准 (1)比较两组临床特征。包括性别、年龄、患者入ICU当日SOFA评分、急性生理学与慢性健康状况评估(acute physiology and chronic health evaluation,APACHE Ⅱ)评分及基础疾病(高血压、慢性阻塞性肺疾病、心脏病、糖尿病、慢性肾病、恶性肿瘤)。APACHE Ⅱ评分包括三部分,即急性生理评分、年龄评分及慢性健康评分,最高分为71分,通过电脑软件完成评分。
(2)比较两组尿、血培养阳性率。
1.4 统计学处理 采用SPSS 23.0軟件对所得数据进行统计分析,计量资料用(x±s)表示,比较采用t检验及Fisher精确检验;计数资料以率(%)表示,比较采用字2检验、连续矫正字2检验及Fisher精确检验。以P<0.05为差异有统计学意义。
2 结果
2.1 所有患者治疗情况 46例患者中因寒战、高热症状由急诊收入ICU 19例,由内科病房转入ICU 23例,因泌尿系结石微创手术后由泌尿外科病房转入ICU者4例。所有患者ICU住院时间4~65 d,其中28 d内病死17例,病死率达37.0%,均在ICU住院期间死亡。存活组29例,死亡组17例。
2.2 两组临床特征比较 死亡组年龄、入ICU时SOFA评分、APACHE Ⅱ评分、合并排尿困难及长期留置尿液引流管的比例均明显高于存活组,差异均有统计学意义(P<0.05),见表2。
2.3 所有患者病原菌分布及耐药情况 入院后尿培养中阳性22例;分离菌株24株,其中单一菌株感染者20例,两种病原菌感染2例;混合病原菌感染者为长期留置导尿管患者。24株病原菌中,培养革兰阴性菌19株(79.2%),其中大肠埃希氏菌16株(84.2%)、肺炎克雷伯菌2株(10.53%)、变形杆菌1株(5.26%);革兰阳性菌4株(16.7%),其中粪肠球菌2株(50.0%),耐甲氧西林金黄色葡萄球菌(Methicillin-resistant Staphylococcus aureus,MRSA)
综上所述,尿源性脓毒症高发于尿路梗阻及高龄、有糖尿病病史及免疫力低下者;高龄患者更易死亡,SOFA评分及APACHE Ⅱ评分的高低对判断脓毒症患者预后意义重大,血、尿培养阳性不能作为判断患者预后差的指标。其致病菌以革兰阴性杆菌为主,可以合并革兰阳性球菌或真菌感染;应根据其致病菌特点早期应用有效抗菌药物。及时解除尿路梗阻对缓解病情至关重要;对明确合并感染的上尿路结石梗阻患者,先期引流解除梗阻有利于预防术后脓毒性休克的发生。希望本研究能为提高尿源性脓毒症的临床诊疗水平有所帮助。
参考文献
[1] Paoli C J,Reynolds M A,Sinha M,et al.Epidemiology and costs of sepsis in the United States-An analysis based on timing of diagnosis and severity level[J].Crit Care Med,2018,46(12):1889-1897.
[2]纪明锁.严重脓毒症的治疗进展[J].岭南急诊医学杂志,2016,21(1):91-92.
[3]李为兵.尿源性脓毒症的新定义及诊治进展[J].现代医药卫生,2018,34(5):650-656.
[4] Bonkat G,Cai T,Veeratterapillay R,et al.Management of urosepsis in 2018[J].Eur Urol Focus,2019,5(1):5-9.
[5] Singer M,Deutschman C S,Seymour C W,et al.The ThirdInternational Consensus Definitions for Sepsis and Septic Shock(Sepsis-3)[J].JAMA,2016,315(8):801-810.
[6]那彦群,叶章群,孙颖浩,等.中国泌尿外科疾病诊断治疗指南2014版[M].北京:人民卫生出版社,2014:424-434.
[7] Dellinger R P,Levy M M,Rhodes A,et al.Surviving Sepsis Campaign:international guidelines for management of severe sepsis and septic shock:2012[J].Intensive Care Med,2013,39(2):165-228.
[8] Levy M M,Fink M P,Marshall J C,et al.2001SCCM/ESICM/AC-CP/ATS/SIS International Sepsis Definitions Conference[J].Crit Care Med,2003,31(4):1250-1256.
[9]中国医学会.重症医学-2016[M].北京:人民卫生出版社,2016:162-165.
[10] Adfie C,Alberlic C,Chaix-Couturier C,et al.Epidemiology and economic evaluation of severe sepsis in France:age,severity,infection site,and place of acquisition(community,hospital,or intensive care unit)as determinants of workload and cost[J].J Crit Care,2005,20(1):46-58.
[11] Scotland K B,Lange D.Prevention and management of urosepsis triggered by ureteroscopy[J].Res Rep Urol,2018,10:43-49.
[12]喬允,陆晓晔,徐欣晖,等.急诊科尿源性脓毒症的临床回顾性研究[J].现代生物医学进展,2019,19(2):253-257.
[13]马序竹,郑波,王逸群,等.113例成年尿源性脓毒症患者的病原学分布及耐药性分析[J].中国临床药理学杂志,2019,35(1):36-38,51.
[14]吕其军,史太阳,周芳,等.16S rRNA基因检测在脓毒症早期诊断中的研究进展[J].中华医院感染学杂志,2016,26(10):2395-2397.
[15]梁霞,邹望远.尿源性脓毒症的研究进展[J].中南大学学报(医学版),2019,44(4):455-460.
[16]张贤芝.尿液不同检测方法对泌尿系统感染的诊断价值[J].中华实用诊断与治疗杂志,2011,25(3):265-266.
[17]王松岚.尿路感染的诊断与治疗[J].中国临床医生,2013,41(4):1-3.
[18] Zahar J R,Timsit J F,Garrouste-Orgeas,et al.Outcomes in severe sepsis and patients with septic shock:Pathogen species and infection sites are not associated with mortality[J].Critical Care Medicine,2011,39(8):1886-1895.
[19] Hofmann W.Urosepsis and uroseptic shock[J].Z Urol Nephrol,1990,83(6):317-324.
[20] McAleer I M,Kaplan G W,Bradley J S,et al.Endotoxin content in renal calculi[J].J Urol,2003,169(5):1813-1814.
[21] Wagenlehner F M,Weidner W,Naber K G.Optimal management of urosepsis from the urological perspective[J].International Journal of Antimicrobial Agents,2007,30(5):390-397.
(收稿日期:2020-04-21) (本文编辑:田婧)
