Role of the Ilizarov non-free bone plasty in the management of long bone defects and nonunion: Problems solved and unsolved
2020-07-23
Dmitry Y Borzunov,Department of Traumatology and Orthopedics,Ural State Medical University,Ekaterinburg 620109,Russia
Sergei N Kolchin,Orthopaedic Department 4,Ilizarov National Medical Research Centre for Traumatology and Orthopaedics,Kurgan 640014,Russia
Tatiana A Malkova,Department for Medical Information and Analysis,Ilizarov National Medical Research Centre for Traumatology and Orthopaedics,Kurgan 640014,Russia
Abstract
Key words: Bone defect; Ilizarov method; Distraction osteogenesis; Bone transport; Bone nonunion; Free vascularized grafts; Induced membrane technique complication
INTRODUCTION
Segmental long bone defects resulting from acute trauma,post-traumatic sequelae,resection due to tumor or bone infection,nonunion or congenital deficiencies lead to significant negative consequences or disability if not managed properly with surgical interventions involving the use of bone grafting and fixation systems[1,2].The universally acknowledged surgical techniques such as autogenous bone grafts for small defects (< 5 cm),free vascularized grafts (FVG),distraction osteogenesis (DO)and induced membrane technique (IMT) for larger defects are contemporary strategies of reconstruction[1-3].These techniques are based on autogenous grafting,either free or non-free,as long as the autogenous bone possesses osteoinductive,osteoconductive and osteogenic properties to induce bone healing.Moreover,the techniques which preserve the vascularity of the graft with the surrounding tissues or generate new vessels would be most effective in promoting bone remodeling.Therefore,FVG,DO and IMT have become the main methods in bone defect management.
DO was developed by G.A.Ilizarov for a number of orthopedic diseases and injuries and was initially realized with the author's external apparatus[4-6].Nowadays,the regeneration philosophy of the Ilizarov method is a cornerstone of contemporary bone lengthening and reconstruction surgery and is implemented with a number of designed devices[6].The author of bone fragment transport for segmental long-bone defect management first reported on the technique in 1969[5,7].Since the 1990s,it has become a vital method for compensation of bone loss and infected nonunion across the world,and has been named the Ilizarov non-free bone plasty[8].Bone nonunion and defects still remain the conditions for which the Ilizarov method has gained most popularity[5].
Vascularized free grafting and the IMT were reported by their authors in 1975 and 2000,respectively[9,10].The first had been used for the reconstruction of many types of bone defects until Ilizarov bone transport (IBT) became popular in the 1990s and IMT later demonstrated successful outcomes in long bone defect management[1,2,10-13].
Management of segmental long bone defects is one of the challenges of contemporary orthopedics due to the severity of high-energy trauma,traffic accidents and military activities that are so characteristic of life in the modern world[2].It is dictated by the defect size,patient comorbidities,soft-tissue condition,local vascularity,nonunion type and possible infection in the defect.Choosing between the three major options for large-scale defects depends on clinical factors,orthopedic surgeon training and preferences,as well as on the availability of the instrumentation needed for successful implementation of the methods[12,13].
We aimed to study the recent available literature on the role of Ilizarov non-free bone plasty in the management of bone defects,the problems to solve and future prospective trends which would enable better treatment outcomes.
MATERIALS AND METHODS
Three databases (PubMed,Scopus,and Web of Science) were screened for recent literature on long bone defect and nonunion treatment within a five-year period(2015-2019) using the key words: Bone defect,large bone defect,nonunion,Ilizarov bone transport (BT),Masquelet (induced membrane) technique,FVG,and free vascularized fibular graft (FVFG).The titles and abstracts were reviewed while screening,potentially relevant articles were retrieved and assessed for inclusion.Table1 presents the findings of search engines in the databases indicated above.In total,232 articles were assessed for eligibility according to the abstracts.The selected 65 full-text clinical articles and reviews available in English were based on the inclusion and exclusion criteria.
Inclusion criteria for literature sources in the study
Full-text articles in English: (1) Reviews on the management of segmental long bone defects and nonunion; (2) Clinical studies stating that patients with segmental bone defects and nonunion were treated using DO,IMT or FVFG.Clinical articles were chosen if they contained treatment results,complications after treatment and described large patient samples (not less than ten cases for congenital,post-tumor resection cases or rare conditions such as subtotal defects,and more than 20 cases for the remainder).Major adverse events were considered problems if they involved operative procedures to correct the treatment failure or its sequelae; and (3) Original articles that compared DO with the methods of IMT or FVFG used for long bone defect management and contained quantitative data on the evaluation of the methods.
Exclusion criteria for literature sources in the study
Exclusion criteria: (1) Case reports,pilot and preliminary studies; and (2) Duplicate studies.
RESULTS
The search showed that there are numerous studies on long bone defect and nonunion management with DO and IMT published in the period under survey while the use of FVFG is less reported (Table1).Reports on FVFG and DO were mainly clinical studies,while there were a number of technical descriptions,reviews and experimental research on the impact of IMT due to the fact that the technique is relatively new.IMT was described technically and reviewed in 18 articles while DO and FVFG were described only in seven and five reviews,respectively.IMT was investigated experimentally in 24 studies while DO was investigated in three and FVFG in none.The full texts of a total of 65 articles using these three techniques were reviewed,including 35 clinical reports on the use of DO or its comparison with two other methods,which described large series of patients and were published in the recent five-year period (2015-2019) (Table1).Merits,shortcoming and problems of the Ilizarov non-free bone plasty,IMT and FVFG are summarized in Table2.The summary shows that the main severe adverse events in the management of bone defects that impede the success of these treatment methods are common: Failure to achieve union and graft incompleteness.
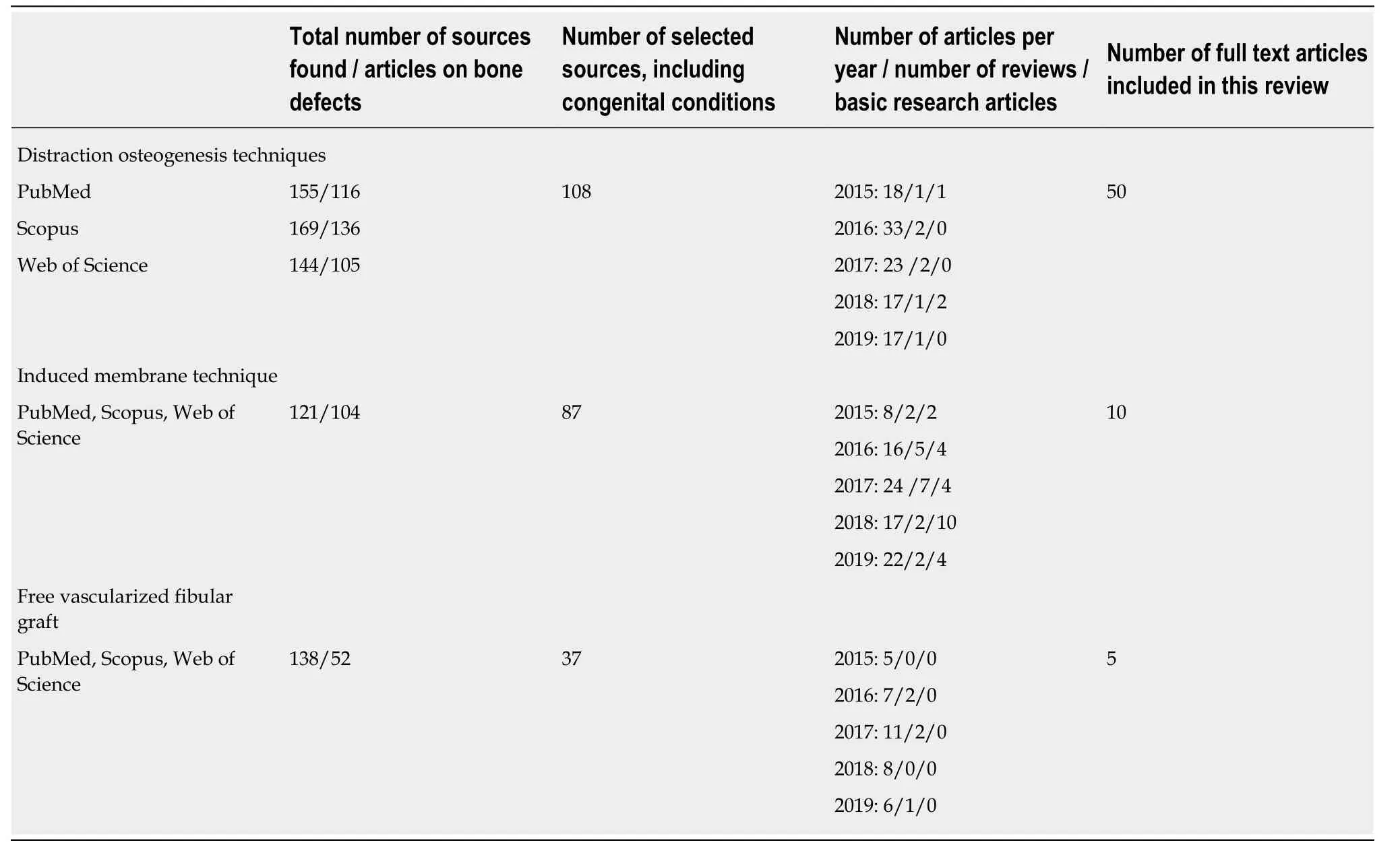
Table1 Number of five-year literature sources found and studied
Out of the total number of articles on DO found,only nine were devoted to bone defects in the upper extremity while infected and aseptic post-traumatic defects of the lower limbs were reported in more than 70% of the articles (Table3),infected tibia being the most frequent pathology (Table4).The clinical studies using DO to treat segmental long bone defects that included the largest series of patients and the problems of their treatment are presented in Table4.Most patient series were retrospective and used the ASAMI scoring system for assessment of bone and functional results and Paley's classification of complications.High rates of successful outcomes were reported by the authors that ranged from 77% to 100% and depended on the pathology and the type of Ilizarov method protocols used.It was not possible to demonstrate quantitatively the outcome success rates of all the studies included due to their heterogeneity and ambiguity.Therefore,primary and secondary treatment failures reported in the studies are presented in Table4.Table4 also indicates the country the authors belong to in order to show where the DO method was used as the samples of patients are numerous.Several comparative studies of the methods used in bone defect and nonunion management were identified by the search and their conclusions are presented in Table5.
DISCUSSION
The Ilizarov method which involves the use of a circular external fixator is one of the most widely used techniques of bone reconstruction in bone nonunion and defects due to physiological bone growth induced by distraction,tension stress and axial forces enabling adequate new bone tissue distribution providing bone gap bridging and union[14-45].Four Ilizarov protocols are used for bone nonunion and defect management[20].Two physical phenomena can be executed for bone fragments,compression and distraction,for either: (1) Approximation of fragments for union by compression and subsequent distraction through osteotomy if required; or (2) BT of an osteotomized fragment for gap filling with new bone and compression at the docking site to achieve bone union[20,38].The bone tissue thus regenerated for lengthening and bone gap coverage can be charged as almost a perfect type of grafting as a vascularized bone callus is formed inside the surrounding soft tissues which remodels into mature bone tissue over time[8].The Ilizarov techniques for bone nonunion and defects stabilize the limb,lead to bone union and at the same time address malalignment,leg length discrepancy and soft-tissue problems[15].They yieldsatisfactory outcomes using limited resources for both aseptic and infected bone defects and nonunion,but should be implemented in medical centers with trained personnel[46].

Table2 Summary of merits and problems of the methods used for nonunion and bone defect management
Moreover,bone distraction and compression may be produced with a number of external and internal devices that have been developed for this purpose and are currently available on the market[5,13].Therefore,the DO procedure has been universally accepted by the orthopedic community throughout the world.However,the shortcomings and problems of the method still remain the issues which restrict its overall use (Table2).Poor regeneration that may occur due to different causes,infection and poor condition of soft tissues in the defect area may result in various stages to fill in the defect,especially if it is massive,or has previously failed[14,17].There is a controversial view on regular bone grafting at the docking site if BT is implemented.Most authors currently recommend routine docking site revisionsduring BT and use supportive bone grafting[47].The authors of the clinical studies conclude that BT is a safe option for treatment of aseptic and infected nonunion of the tibia and femur despite the complications encountered.The average bone and functional scores significantly improve within two years after the end of treatment[47].The authors underline that it is essential to explain the complications to the patients and their relatives before the application of external fixators to increase their compliance with a long and highly emotional course of treatment due to severe pain,mental,and physical stress[47,48].
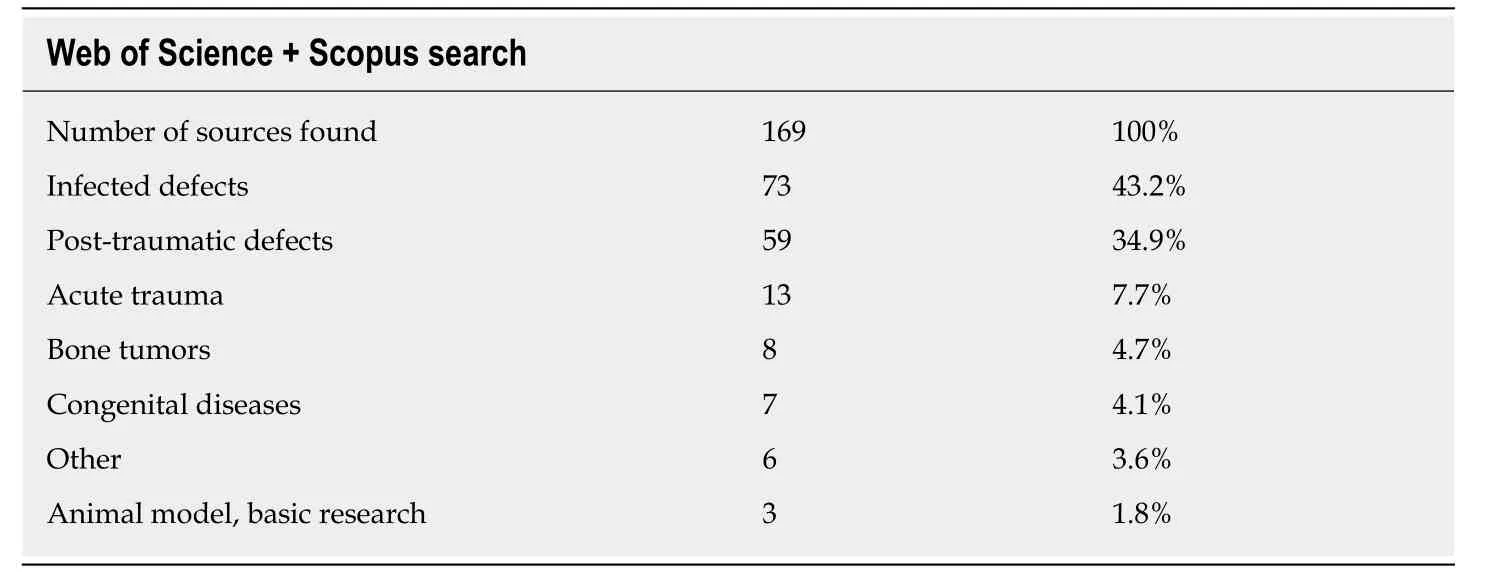
Table3 Web of Science + Scopus search results for the period 2015-2019 (key words: Ilizarov method,bone defects)
Table4 shows that DO is a solution for segmental long bone defects and nonunion in a number of conditions caused by acute injuries,trauma sequelae,bone infection and bone tumor resection in the tibia and femur,but infected tibia is the segment in which DO and the Ilizarov apparatus have been used extensively.According to the studies,the Ilizarov BT and acute shortening and then lengthening techniques remain reliable methods to repair bone defects[16,18,29].The following are some of the main conclusions and recommendations the authors focus on: (1) DO is a good method that can treat the triad of problems simultaneously (bone loss,soft-tissue loss and infection) without the need for major plastic surgery[21]; (2) The Ilizarov fixator is better suited for infected nonunion of the tibia because it can provide a stable mechanical environment,BT,correction of deformities,and enables weight bearing[19].The current findings suggest that the Ilizarov methods in the treatment of infected nonunion of the tibia and femur result in satisfactory outcomes.Radical debridement is the key step to control bone infection[42]; (3) The use of a ring fixator is recommended in patients with an infected tibial bone gap of more than 6 cm.Patients with a bone gap up to 6 cm can be managed with either a ring or rail fixator[24,30]; (4)Antibiotic-impregnated spacers were used in open tibial trauma and reduced the external fixation index considerably[25,28]; (5) Patients treated with combined fixation spent less time in the external fixator.The frequency of adverse events and ability to restore limb length was not different to the group treated with the external fixator only[26]; (6) Acute shortening followed by distraction histogenesis is a safe method for acute treatment of open tibial fractures with bone and soft-tissue loss[29].The technique is limited by the defect size and the condition of the surrounding soft tissues.The technique of acute shortening and re-lengthening was not recommended in postgunshot defects[30]; and (7) DO is a method an orthopedic surgeon with limited conditions can use,though it has a long treatment period[29,35].
Tables 2 and 4 reveal that docking site nonunion and after-frame regenerate fracture or deformity are the major causes of DO failures[14].Therefore,orthopedic surgeons and researchers search for the ways to improve the DO procedure for segmental bone defect and nonunion management.They report on a number of solutions to overcome the problems and gain better results.The following is a summary of these solutions according to the literature under our investigation.
Solutions to the shortcomings and problems within the DO method or combining it with other methods as offered in the studies reviewed
The following are solutions to the shortcomings and problems within the DO method or combining it with other methods as offered in the studies reviewed: (1) Accurate study of the regenerate with radiographic methods and clinical tests to exclude premature removal of the external fixator and potential treatment failure[8]; (2) The accordion technique combined with minimally invasive percutaneous decortications to stimulate regeneration[49]; (3) Compaction of the problematic regenerate to rescue DO and achieve union[50]; (4) Bifocal or multifocal BT to reduce BT time,time in the frame,and total treatment time in one stage[8,17,19,23,50,51]; (5) Acute shortening and
subsequent DO in the management of open tibial fractures with bone and soft-tissue loss to avoid the need for a soft-tissue flap to cover the wound or post-traumatic defects if soft tissues allow it[16,18]; (6) Antibiotic cement spacers for infected nonunion with bone defect to reduce infection recurrence[27,28]; (7) Use of monolateral external fixators and rail fixators,especially in the femur,which provide effective stability,BT and improve patients' compliance and quality of life[19,33,37-39,42,44]; (8) BT with a hexapod external fixator[52]and combined Ilizarov and Taylor spatial frames versus a conventional circular frame to achieve union[23]; (9) Gradual transport of a fibular fragment with the Ilizarov external fixator for subtotal and total tibial defects to salvage the limb[8,34,35]; (10) BT over an intramedullary nail using cable and pulleys or BT and then nailing to combine internal and external fixation to decrease time in the frame and patient's quality of life[14,53]; (11) Hydroxyapatite coated pins with external fixators to exclude loosening and infection[54,55]; (12) Intraosseous injection of bonemarrow derived autologous mesenchymal stem cells as an add-on therapy to the DO procedure improvement[56]; and (13) Teriparatide treatment during the consolidation phase to stimulate bone formation[57].
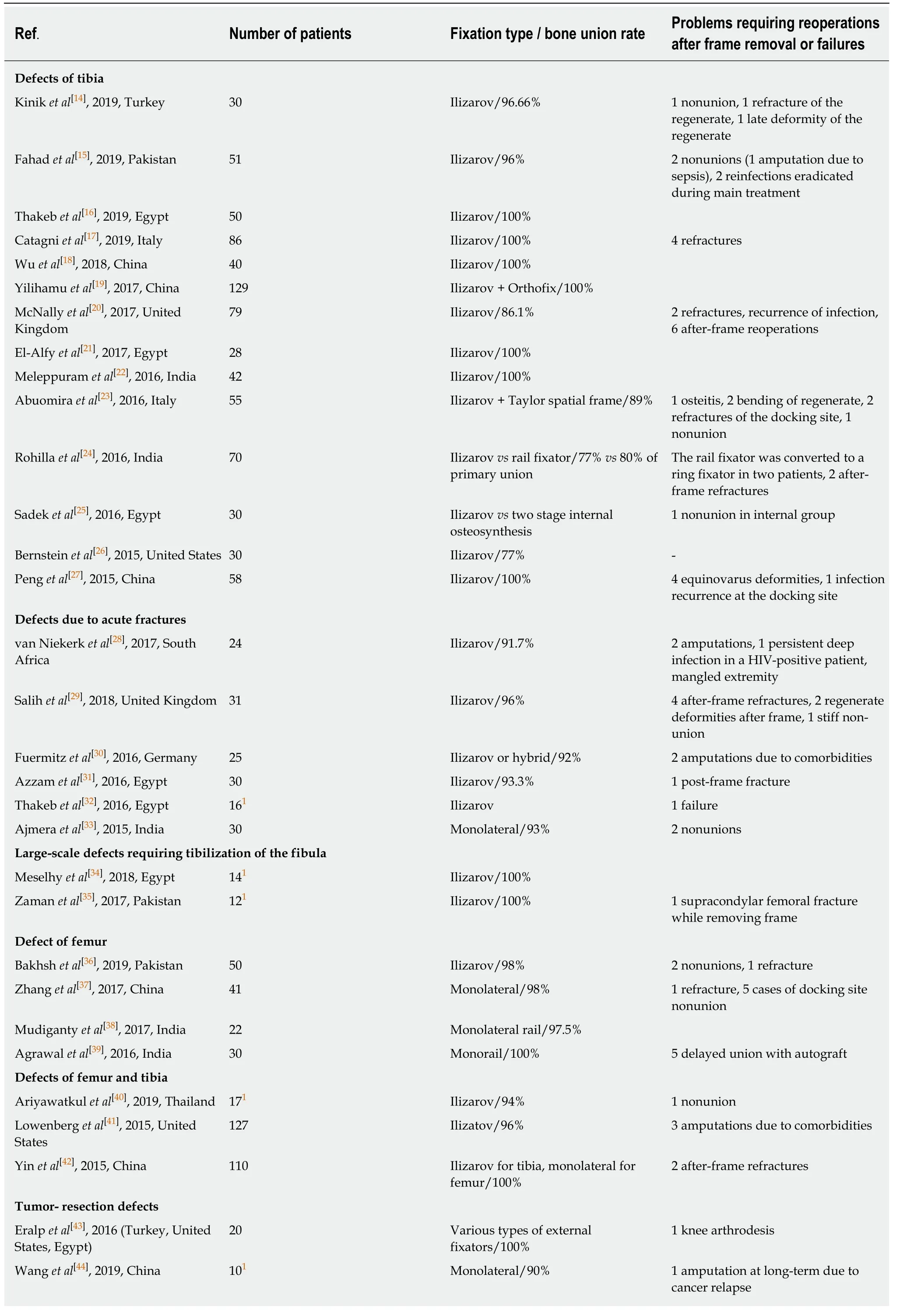
Table4 Largest clinical studies published in 2015-2019 and their outcomes with distraction osteogenesis techniques
Current clinical tendencies in segmental bone defects management with the method of DO
It is evident that significant advancements such as internal cable transport,multifocal transport,and combined techniques with internal fixation have helped increase the effectiveness of the ring fixator by minimizing many of its drawbacks.However,the main problems in the management of bone defects and nonunion (failure to achieve docking site union and bone graft incompleteness) impede the DO success irrespective of the fixator used and need to be solved with osteogenesis stimulation and perfection of bone fixators.
Advances in bone fixation techniques
We have come to a conclusion that it is the combination of external and internal technologies that is the main clinical tendency in the use of DO for long bone defects in the tibia and monolateral fixation in the femur[14,24-26,30,42].It seems to be logical as it solves some of the external-fixator associated shortcomings,mainly the long-term wearing of ring external devices that worsen patients' quality of life and a long rehabilitation time[47].Thus,the combined techniques of BT over nail (BT over nail and BT and then nailing have recently been used for reconstruction of post-traumatic and post-resection defects in the lower limbs,including the infected nonunion and defects once the latter have been debrided thoroughly[26].Their main merits are: (1) Reduction of external fixation time; (2) Less knee stiffness and opportunity to do more exercise therapy for joints after frame removal; (3) Comfort after frame removal; (4) Alignment of the regenerate on the nail; and (5) Exclusion of regenerate deformities and fractures.However,the regeneration features and complication rates were similar and not statistically different[26].Closed intramedullary nailing (IMN) was found to be an effective and easy solution for cases without pin-tract infection to manage the nonunion problem of the docking site[58].However,the risks of pin-tract and deep infection as well as pain due to stretching and nail breaking risks remain[59].Moreover,combined external and internal fixation was found to have a greater risk of infection recurrence in the treatment of infected tibial nonunion and chronic osteomyelitis[59,60].
Some more options of a combined technique have been reported,such as a lengthening nail for transport and a locking plate for docking and a carbon-fiber IMN,including an antibiotic-coated carbon fiber IMN nail,specifically designed for femurs[61,62].The latter allows for artifact-free visualization on magnetic resonance imaging,which is important for monitoring the treatment response.However,besides its high cost,it was found clinically that the nail performs poorly in long-bone surgery and cannot be added to external fixation instead of a titanium nail even for combination.
Nevertheless,Ilizarov's fundamental principles must still be followed even with internal devices.Internal telescopic lengthening nails show similar bone results and significantly improve patients' quality of life,as well as exclude pin-tract infection problems.It is evident that IMN fixation alone would be much more comfortable than the combined techniques[63].Recently,new IMNs have been investigated to provide a one-stage alternative to external fixators for reliable DO in defect management.Lately,some reports on their designs supplied with clinical cases involving the tibia and femur have been made by German researchers[64].The system is called a cylindricalcombitube segmental transport (MagicTube) module for combination with a commercially available motorized lengthening nail.This MagicTube module enables a
completely internal segmental BT and optional lengthening if needed.However,its application for segmental bone defect still poses questions such as docking site problems,device functioning failure and high costs.

Table5 Comparative studies of the methods in the period 2015-2019
Osteogenesis stimulation advances
Cell-based additives,such as bone marrow aspirate concentrate (BMAC),growth factors,bone morphogenic proteins (BMPs) and platelet-rich plasma,to accelerate the DO process,bone repair and to reduce the problems related to prolonged external fixation have been extensively experimented and discussed[56,65-68].Our search for clinical trials and studies on their use did not yield many examples of their application.There are studies reporting the clinical use of BMAC in nonunion and fracture healing and complications related to the use of BMAC.Despite the findings demonstrating the clinical effectiveness of adjunct application of commercially available BMPs (rhBMP-7 or -2) in nonunion treatment there is no clinical evidence of their use in the DO procedure[69].It has also be referred to in the clinical literature on the real benefit of platelet-rich plasma to treat fractures and nonunion.Mixed results have been described in terms of efficacy and adverse events.
Also,nanostructured scaffolds made of materials including polymers,ceramics,composites and metals that can be enriched with osteogenic agents to promote bone formation are under investigation but have not been used clinically yet due to unanswered concerns regarding clinical safety of the long-term effect of nanomaterials on human health.Tissue engineering and cell-based therapies have not found their place in long bone defect management yet as was expected by previous reviews[1,2].The issue necessitates much advancement in stem cell biology,novel biomaterials,and 3D bioprinting.Therefore,the comprehension of the merits,shortcomings and adverse events of the established methods of DO,IMT and FVFG as well as proper understanding of the recent practice in the reconstruction of large segmental bone defects may guide the clinician towards the right choice (Table2).
Our search for recent literature confirmed an increasing popularly,larger series of patients treated with IMT and more reports on its results in segmental bone defects[3,70-76].Recently,IMT has been widely used for septic,traumatic,neoplastic or congenital bone defects in adults and children[3,10,70-73].The pearls and tricks of the technique were explained by its author and followers in an illustrative way[3].Although some authors find this type of reconstruction rapid and safe,gross problems are not excluded either (Table2).Others point out that although it is a simple and straight-forward procedure,the total time required for growth and maturation of the graft is similar to DO and FVFG[74].The polymethylmethacrylate spacer used to induce membrane is not degradable and needs to be removed surgically with a rigorous technique during cement sleeving followed by grafting and stabilization of the defect to prevent nonunion with the bone fixation means available.The main complications are stabilization loosening and resorption of the graft which need reoperations that are gross procedures.It was proposed that a circular Ilizarovlike external fixator that is able to apply compressive stresses and prevents shear stresses is more favorable for IMT reconstruction than a monolateral external fixator[70].Both Ilizarov BT and IMT lead to satisfactory bone results in the treatment of segmental lower extremity bone defects but several authors revealed better functional results with IMT,especially in femoral cases and periarticular bone defects,and conclude that BT should be preferred in cases of limb deformity[75].In pediatrics,BT and IMT may both be also used for post-tumor reconstructions but there are constraints related to chemotherapy and tumor recurrence[44,70].Better rates of success are expected in aseptic and septic nonunions with the use of this technique and diamond concept[76].
The reconstruction procedure with IMT first induces a membrane and then promotes osteointegration and remodeling of the graft as well as osteogenesis that was proven on animal models and a human induced membrane study[77].It is apparent that the role of the induced membrane in promoting bone formation has recently been thoroughly investigated to explain the phenomena[77,78].It was revealed that the induced membrane matured between the 4thand the 6thweek and secreted growth factors to promote osteogenesis.It was discovered that the mature induced membrane and periosteum had similar structures and abilities to promote osteogenesis of mesenchymal stem cells but the induced membrane was found to be thicker than the periosteum and characterized by maturing vascularized fibrous tissue,which secretes several growth factors,including the vascular endothelial growth factor,BMP-2 and transforming growth factor-β1.This membrane on the spacer was called a “neoperiosteum” in the other basic research study[78].Its inner layer is structured with low-differentiated connective tissue cells manifesting the signs of osteogenic differentiation confirmed by expression of osteopontin.Therefore,it was proposed to combine the two biological effects,those of DO and IMT,for treating congenital pseudarthrosis of the tibia,as both methods promote vascularized new bone formation.Congenital anomalies,including congenital pseudarthrosis of the tibia,treated using IMT have promising results[70,78].
Vascularized free grafting has been the workhorse for reconstruction of many kinds of bone defects,including massive post-resection and infected defects[9,79-81].Being blood supplied,these grafts have high success rates in bone reconstruction and accelerate the repair process at the injury site.However,FVFG in the lower limbs and mainly in the tibia should be well protected with internal or external fixation and bracing during the first year to undergo remodeling.External fixator frames are advocated for this purpose nowadays to provide load-sharing and mechanical alignment to exclude a stress fracture.Best results were achieved in the management of upper extremity defects where the vascularized grafts unite with the recipient bone in the period which is close to the average fracture consolidation terms in upper extremity and where the DO procedure would be very complex[80].However,the FVFG procedure is technically difficult,involves microsurgical equipment and skilled microsurgeons.
The application of the three techniques was thoroughly reviewed in numerous literature and clinical reports (Table1).Several authors demonstrated sufficient literature verification of the merits and shortcomings of the methods in their reviews[1-3,60,81].Moreover,there were clinical studies that compared the contemporary techniques of segmental bone defect management (Table5)[3,75,78,82].However,due to few systemic reviews and comparative studies between different surgical methods,the orthopedist should choose the appropriate treatment according to particular situations,types of bone nonunion or defect,being guided by his/her skills and economic issues.
Main conclusions of the literature review
DO with circular frames (Ilizarov techniques) remains particularly useful for complex problems in the tibia while monolateral external fixators are preferably applied in the femur.Free vascularized fibular grafts have recently been used mainly in the upper limb and post-tumor cases.The IMT has become an important method for the treatment of bone nonunion with large bone defects.
We performed this study to identify whether the role of the Ilizarov method has changed in the recent five-year period due to the emergence of new trends and methods of long bone defect treatment.The search revealed that its important role has not diminished.At present,ring fixation continues to provide the most effective means of treatment for large bone defects in many clinic situations while DO is the leading technique that is used with a number of available external fixators.The use of the IMT has expanded in recent years and also offers valid solutions.
In conclusion,DO techniques provide the most widespread means for the treatment of segmental bone defects and infected nonunion of the lower extremity in many clinical conditions,especially in complex lower limb problems.Management of tibial defects mostly utilizes the Ilizarov ring fixator.The role of the Ilizarov non-free bone plasty has not lost its significance in the treatment of segmental bone defects and nonunion despite its shortcomings and unsolved problems.
ARTICLE HIGHLIGHTS
Research background
Segmental long bone defects are one of the challenges in contemporary orthopedic practice due to severity of high-energy trauma,traffic accidents and military activities.Current strategies for their reconstruction [distraction osteogenesis (DO),free vascularized grafting (FVG),and induced membrane technique (IMT)] are based on autogenous type of grafting,either free or non-free,which is their main merit.However,the shortcomings and problems of these methods still remain the issues which restrict their overall use.The Ilizarov non-free bone plasty is a method of DO used with the Ilizarov apparatus which originated in Russia and has been used in other countries since 1990s.
Research motivation
Being experienced in the Ilizarov method of limb reconstruction,we studied the most recent available literature on these three methods for long bone defect and nonunion management to determine the present role of the Ilizarov techniques in this orthopedic field and to investigate the solutions proposed by the authors to the problems they encounter for improving treatment outcomes.
Research objectives
The main objectives were to find scientific material in the databases of orthopedic medical journals and to select suitable articles on the management of segmental long bone defects using current methods that show treatment results,merits,shortcomings,ways to overcome failures and prospective trends for future research in this field.In addition,we searched for original articles that compared the Ilizarov techniques with the methods of IMT or FVG and contained quantitative data on the evaluation of these methods.
Research methods
Three databases (PubMed,Scopus,and Web of Science) were screened for recent studies in long bone defect and nonunion treatment within a five-year period (2015-2019).Sixty-five full-text clinical articles and reviews in English were selected for data analysis.Clinical studies were included if they described large patient samples (not less than ten cases for congenital,posttumor resection cases or rare conditions,and more than 20 cases for the remainder) and contained treatment results and complications.Major adverse events involving operative procedures to correct the treatment failure,or its sequelae were of particular interest.Merits,shortcomings and problems of the Ilizarov non-free bone plasty,IMT and free vascularized fibular graft were summarized.Out of a total of 50 articles on DO found,only nine were devoted to bone defects in the upper extremity while infected and aseptic post-traumatic defects of the lower limbs were reported in more than 70% of the articles,infected tibia being the most frequent location.
Research results
The search showed that there are numerous studies on long bone defect and nonunion management with DO and IMT.The use of free vascularized fibular graft has been less reported.Full texts of a total of 65 articles using these three techniques including 35 clinical reports on the use of DO or its comparison with two other methods were reviewed for outcome measures.It was found that DO techniques provide solutions to many complex problems as it addresses the triad of problems simultaneously (bone loss,soft-tissue loss and infection).Management of tibial defects mostly utilizes the Ilizarov circular fixator.Monolateral rail fixators are preferable in the femur.The use of a ring fixator is recommended in patients with an infected tibial bone gap of more than 6 cm.High rates of successful treatment were reported by the authors that ranged from 77% to 100% and depended on the pathology and the type of the Ilizarov technique used.Unfortunately,the outcome success rates were heterogeneous and lacked definite statistical findings.Docking site nonunion and after-frame regenerate fracture or deformity were the major causes of failures.One of the solutions to these problems is the application of hybrid external and internal fixation.Most authors currently recommend docking site revisions during bone transport and use supportive bone grafting.Effective technical solutions and add-on therapies to improve quality and control over osteogenesis have been developed.
Research conclusions
The main solutions to the problems of DO that are recommended by the authors focus on the following developments: (1) Mechanical stimulation of regeneration; (2) Multifocal bone transport to reduce total treatment time; (3) Acute shortening followed by distraction histogenesis; (4) Gradual transport of a fibular fragment in subtotal and total tibial defects; (5)Bone transport over an intramedullary nail; (6) Hydroxyapatite coated pins; and (7) Intraosseous injection of bone-marrow derived autologous mesenchymal stem cells.There are few comparative clinical studies that evaluate outcomes of the three methods used for long bone defects and nonunion.
Research perspectives
The combination of the biological effects of DO and IMT for treating congenital pseudarthrosis of the tibia has been proposed,as both methods promote vascularized new bone formation.New internal telescopic nails have been investigated to provide a one-stage alternative to external or hybrid fixation for reliable DO as they show similar bone formation results,exclude pin-tract infection problems and significantly improve patients' quality of life.The issues of DO stimulation with cell-based additives and the use of nanostructured materials still require further investigation.