Tibial tubercle osteotomy in revision total knee arthroplasty: A systematic review
2020-07-23
Byron Chalidis,Dimitrios Kitridis,Panagiotis Givissis,1st Orthopaedic Department,Aristotle University of Thessaloniki,George Papanikolaou Hospital,Thessaloniki 55210,Greece
Abstract
Key words: Tibial tubercle osteotomy; Knee flexion; Extension lag; Union; Revision total knee arthroplasty; Stiff knee
INTRODUCTION
Tibial tubercle osteotomy (TTO) is a useful and well-established technique to deal with a tight extensor mechanism and stiffness in revision total knee arthroplasty(RTKA).It provides excellent exposure and visualization of the knee joint as it allows unforceful eversion or lateral subluxation of the patella and unimpeded access to the lateral gutter and lateral component-bone interface[1,2].The osteotomized bone fragment should be of sufficient size to facilitate secure hardware fixation with wires and screws and provide an appropriate contact area for bone consolidation.Furthermore,preservation of the musculature sleeve is of primary importance for bone segment viability and stability and a good result can be achieved even after a previously performed TTO[2].
The osteotomy can be safely extended into the intramedullary tibial canal to utilize removal of the tibial stem and retained cement[3,4].Although the intramedullary extension of the osteotomy may prolong union time due to the relatively small boneto-bone contact area at the site of the TTO,good healing capacity has been reported[2].In addition,re-alignment of the extensor mechanism for optimal balance and simultaneous correction of patellar height by proximalization of the tibial tubercle can be safely applied at the time of osteotomy fixation[2,3].
On the other hand,several reports have described potential osteotomy-related complications such as extensor lag,tibia fracture,nonunion,tibial tubercle migration,metalware irritation,and wire breakage.In the majority of cases,the aforementioned problems were largely attributed to surgical technique and adversely affected the functional outcome[5,6].
The current review aims to investigate the literature and estimate the efficiency of TTO in RTKA in terms of osteotomy union rate,knee range of motion (ROM),and incidence of complications.
MATERIAL AND METHODS
The authors followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) recommendations[7].
Literature search
MEDLINE,Scopus,and the Cochrane Central Register of Controlled Trials were searched for entries from inception to February 2020.The search strategy for Medline was “(tibial tubercle osteotomy) AND (total knee)” and was adjusted to each database and no filters or language restrictions were used.The reference lists from the included articles were also manually screened for additional studies.Two authors (Kitridis D and Chalidis B) independently searched for studies and reviewed all titles and abstracts.Subsequently,the full texts were screened for eligible studies that met all identified inclusion criteria.
Eligibility criteria
Clinical studies relevant to TTO in RTKA,which enrolled more than 10 patients over 18 years old,were included in the review.Trials with incomplete clinical data and articles reporting mixed results with primary total knee arthroplasty were excluded.
Data extraction
Two authors (Kitridis D and Chalidis B) performed the data extraction process from the selected articles in a blinded manner.Studies and patients' characteristics (i.e.,study type,year,country and size,as well as patients' demographics),kind of surgical interventions,clinical results and complications,and the follow-up observations were gathered and analyzed.Any disagreement was resolved by review from a third author (Givissis P).
When there were insufficient data,these were requested from the corresponding author of each article.
Quality assessment
Two investigators (Kitridis D and Chalidis B) independently performed the quality appraisal.Case series studies were assessed using the tool developed by Mogaet al[8],which consists of 18 entries; studies achieving a score of 13 or greater are considered of high quality,7-12 of moderate,and 0-6 of low quality.Comparative trials were evaluated using the Coleman Methodology Score[9],which relies to ten methodological criteria; a score of 100% is considered the optimal high quality score.
Outcomes
The main outcome of the review was the TTO union.Secondary outcomes were the improvement of ROM and the incidence of TTO-related and RTKA complications.
Statistical analysis
Pooled-data analysis was performed using weights according to each study's sample size.Categorical outcomes were expressed as percentages.The longest follow-up measurements of each study were used.Microsoft Excel version 16 and IBM Statistical Package for Social Sciences software version 24 were utilized for data analysis.
RESULTS
The literature search yielded 395 articles,of which 183 were duplicates and 139 were excluded from the titles and abstracts.Finally,29 clinical studies did not fulfill the selection criteria and 15 clinical studies were considered for review (Figure1).
Characteristics of the included studies
Ten retrospective case series studies[1,2,4,6,10-15],three retrospective non-randomized comparative studies[3,16,17],one prospective non-randomized comparative trial[18],and one prospective randomized clinical trial[19]enrolled 780 patients.Data were extracted from a total of 545 patients,who underwent 593 TTOs.Of them,296 were performed in aseptic RTKAs and 297 in septic RTKAs.Of note,eight studies included two-stage revisions for infected RTKAs[2-4,6,10,11,13,19].All the cited articles were published from 1998 to 2019.Eight studies originated from Europe[1,6,12-16,19],five from North America[2,4,10,11,17],and two from Asia[3,18].Tables 1 and 2 present details about studies and surgical interventions,respectively.
Quality assessment
Ten studies were level IV evidence[1,2,4,6,10-15],four were level III[3,16-18],and one was level II[19].Nine case series were found to be of high quality[2,4,6,10-15],and one of low quality[1].The effect of the particular low-quality study was evaluated as a potential confounding factor; the stratified analysis of outcomes was repeated after excluding the study,and no substantial differences were noted (P= 0.83).Therefore,the study was finally included in the review.The comparative trials were rated with a mean Coleman Methodology Score[3,16-19]of 73.6% (range 54-92%).
Synthesis of the results
Eleven non-unions out of 593 TTOs were reported (union rate 98.1%,Figure2).There were three intraoperative tibial tubercle (TT) fractures (0.5%),10 proximal avulsion fractures (1.7%),and five metaphyseal tibial fractures (0.8%).Proximal migration of the TT was observed in 41 cases (6.9%).Anterior knee pain was reported in 38 cases(6.4%),13 of which required hardware removal (2.2%).All TTO-related complications are reported in Table3.
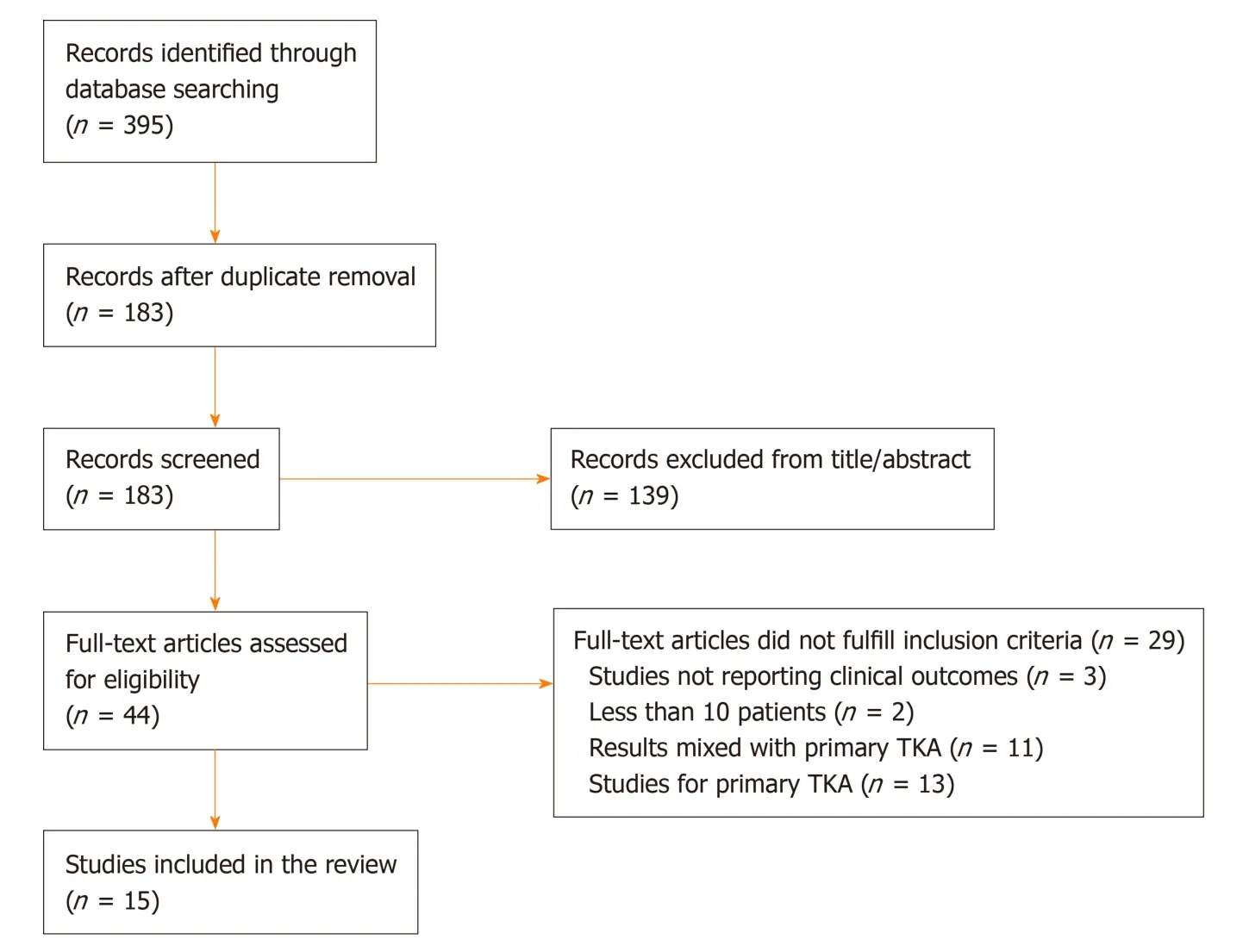
Figure1 Flow chart diagram for inclusion and exclusion article process.TKA: Total knee arthroplasty.
Total ROM improved from 73.4° preoperatively to 97° postoperatively and knee flexion increased from 82.9° before surgery to 100.1° after surgery.Data in detail are reported in Table4.
Stiffness requiring manipulation under anesthesia was evident in 27 cases (4.6%).From all RTKAs that performed due to periprosthetic joint infection via TTO,29 knees(9.8%) showed recurrence of infection.None of the studies reported any major complications.Specifically,all non-TTO related complications are documented in Table5.
DISCUSSION
The present systematic review advocates the use of TTO in RTKA.Knee flexion and ROM were improved from 82.9° and 73.4° preoperatively to 100.1° and 97°postoperatively,respectively.Furthermore,TTO permits early rehabilitation and restoration of quadriceps excursion and strength minimizing the incidence of extension lag[4].Bruniet al[19]compared the utilization of TTO and Rectus Snip techniques at the time of reimplantation during two-stage RTKA for prosthetic joint infection.Patients in the TTO group had a higher mean Knee Society Score than the Rectus Snip group (88vs70,respectively).Mean maximum knee flexion was greater in the TTO group (113°vs94°) with a lower incidence of extension lag (45%vs13%).However,the risk of joint arthrofibrosis and stiffness even after utilization of TTO isn't insignificant.We found that 4.6% of cases underwent postoperative closed manipulation under anesthesia to improve knee ROM.
Non-union of osteotomy is rare as 98.1% of bone healing was obtained.Even in case of tibial tubercle distalization or/and medialization for achieving proper tension and tracking of the patella and the extensor mechanism,excellent healing capacity should be expected[2,16].Similarly,repeat osteotomy as well as intramedullary extension of osteotomy was associated with high union rates.Chalidis and Ries noticed that the median union time for the primary TTO was 15 wk (range 6 to 47 wk)and for the repeat TTO was 21 wk (range 7 to 27 wk)[2].In addition,intramedullary TTO had a longer healing time (median 21 wk,range 7 to 38 wk) when compared to extramedullary osteotomy (median 12 wk,range 6 to 47 wk).
Proximal migration of TT and anterior knee pain were the most common complications of TTO with an incidence of 6.9% and 6.4%,respectively.Proximal stepcut osteotomy might prevent superior displacement of the osteotomized tibialfragment,although this was not necessarily associated with extensor mechanism dysfunction[2,14].Anterior knee pain was mainly related to metalware prominence and irritation and it was apparent regardless the type of fixation with wires and screws[10,11].However,we found that only 2.2% of cases required hardware removal.Suture repair may reduce even further the incidence of anterior knee pain but the technique relies on the integrity of the lateral periosteal sleeve and therefore risks migration of TTO[15,20].

Table1 Summary of studies characteristics
Recurrence of periprosthetic knee joint infection was identified in 9.8% of RTKA cases.The overall risk appears to be a complex and multifactorial issue involving patient and surgical factors.Tibial tubercle osteotomy should be considered a safe extensile procedure as so far there is no evidence that the technique may adversely affect the possibility of reinfection.When TTO was compared to rectus snip regarding re-infections after two-stage revisions in infected RTKA,Bruniet al[19]reported that the results were similar in both groups (7% in the snip group and 5% in the TTO group,P= 0.84).Furthermore,Sunet al[3]in another comparative study found that the incidence of reinfection in two-stage RTKAs was 4.8% in the TTO group and 7.4% in the snip group.Nevertheless,this difference failed to reach statistical significance (P=0.71).
The main limitation of the current study was the fact that it was not feasible to conduct a meta-analysis with direct comparisons between interventions.This occurred because the majority of the included studies did not include a control group.Moreover,the case series studies were of low level of evidence.Another limitation was that the study by Zonnenberget al[15]had a borderline moderate quality Coleman methodology score of 54%,and the study by Hockinget al[1]was of low quality according to the Moga score.After accounting for the risk of bias introduced in the review by the latter study with a stratified analysis,no significant changes of the results were noted compared to the primary analysis.Therefore,both studies were included to increase the sample size and improve the power of the review.Also,13 out of 15 studies were retrospective,which might create data collection or patient selection bias.All these reflect the need for high-quality trials comparing different interventions.
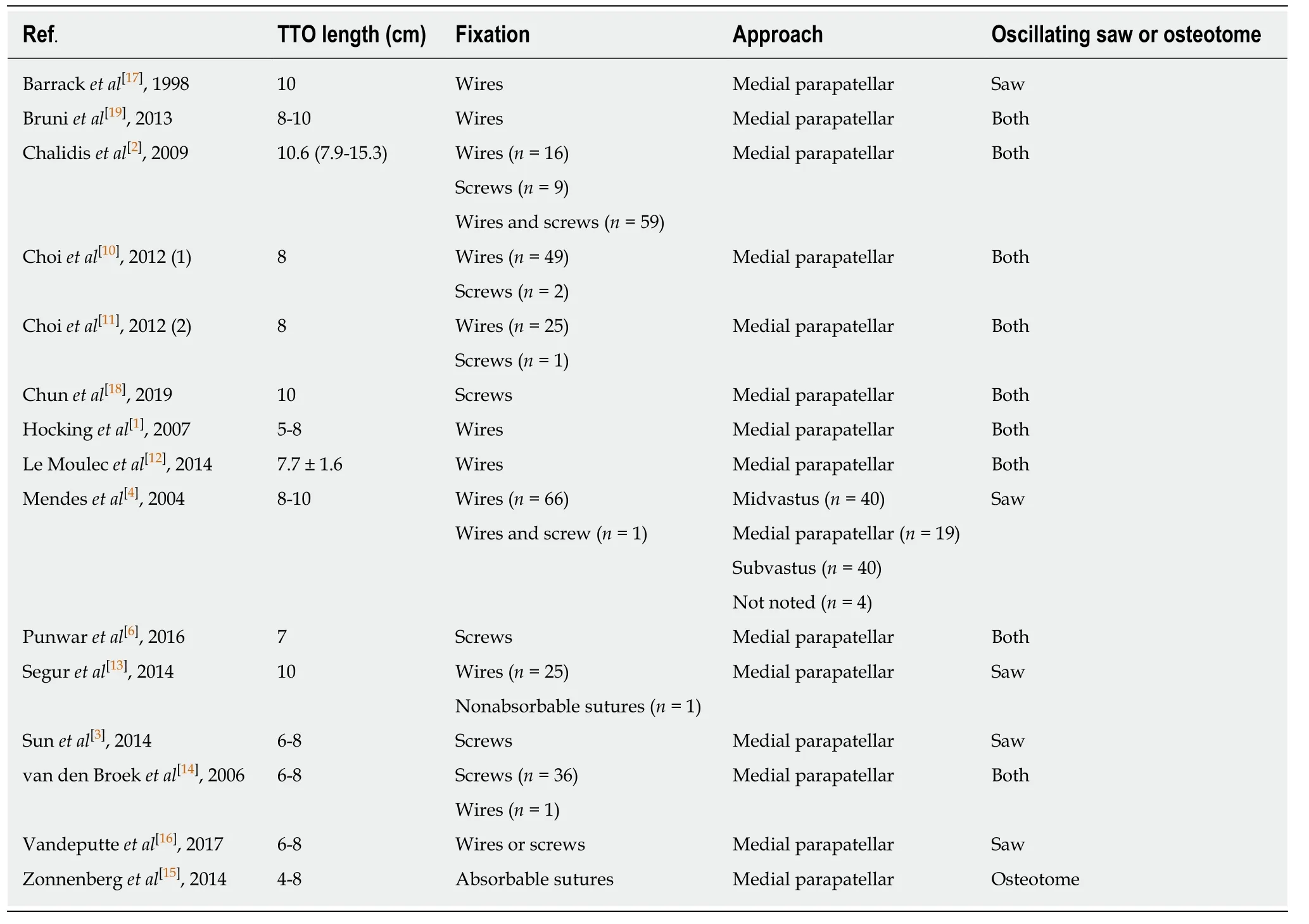
Table2 Surgery parameters
CONCLUSION
In conclusion,TTO shows great clinical safety and efficacy in RTKA.Non-union is rare,and the most reported TTO-related complications are proximal migration and anterior knee pain.However,in the vast majority of cases they aren't associated with secondary procedures of osteotomy refixation or metalware removal.
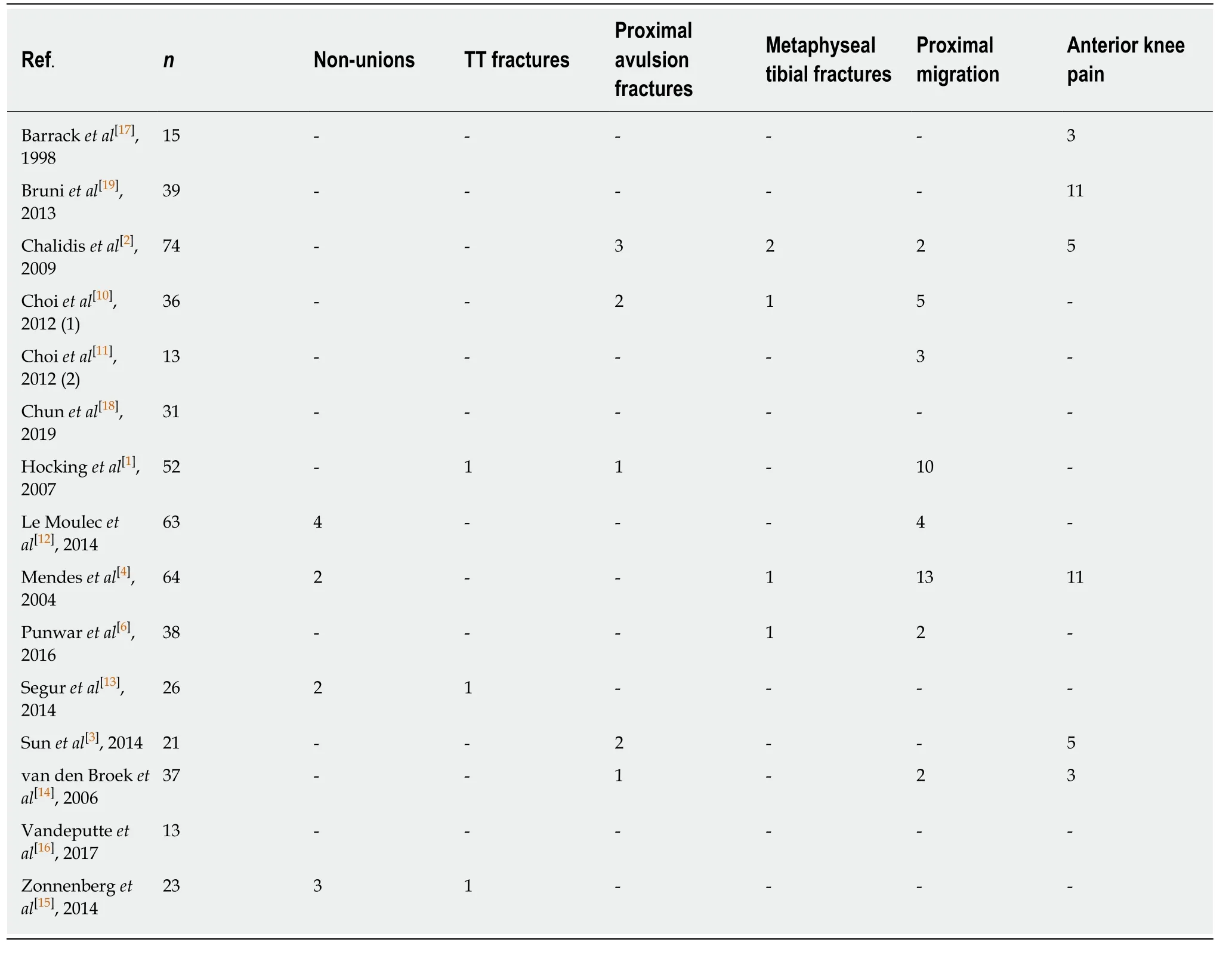
Table3 Tibial tubercle osteotomy-related complications
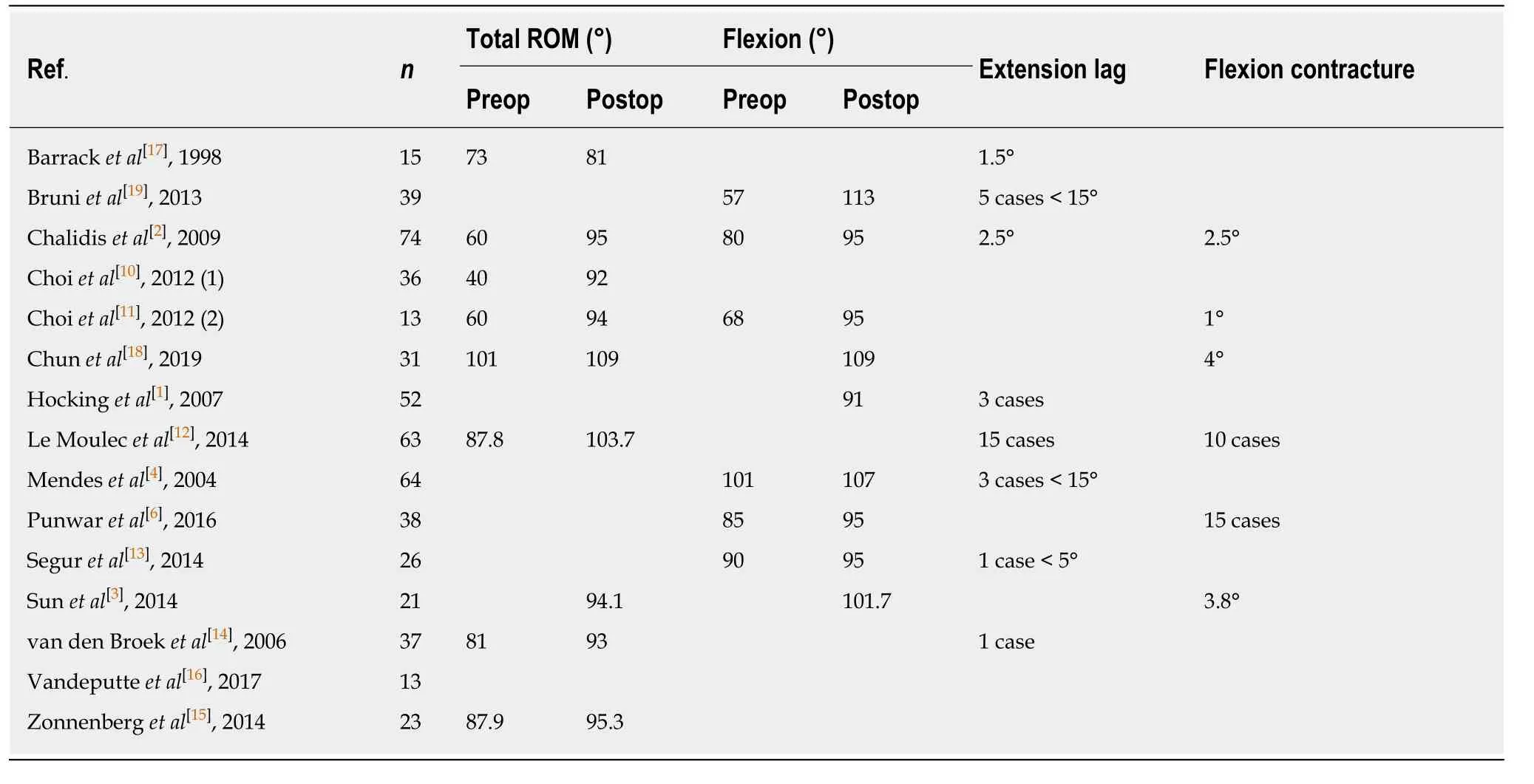
Table4 Mean range of motion,flexion,extension lag and flexion contracture values

Table5 Non-tibial tubercle osteotomy related complications
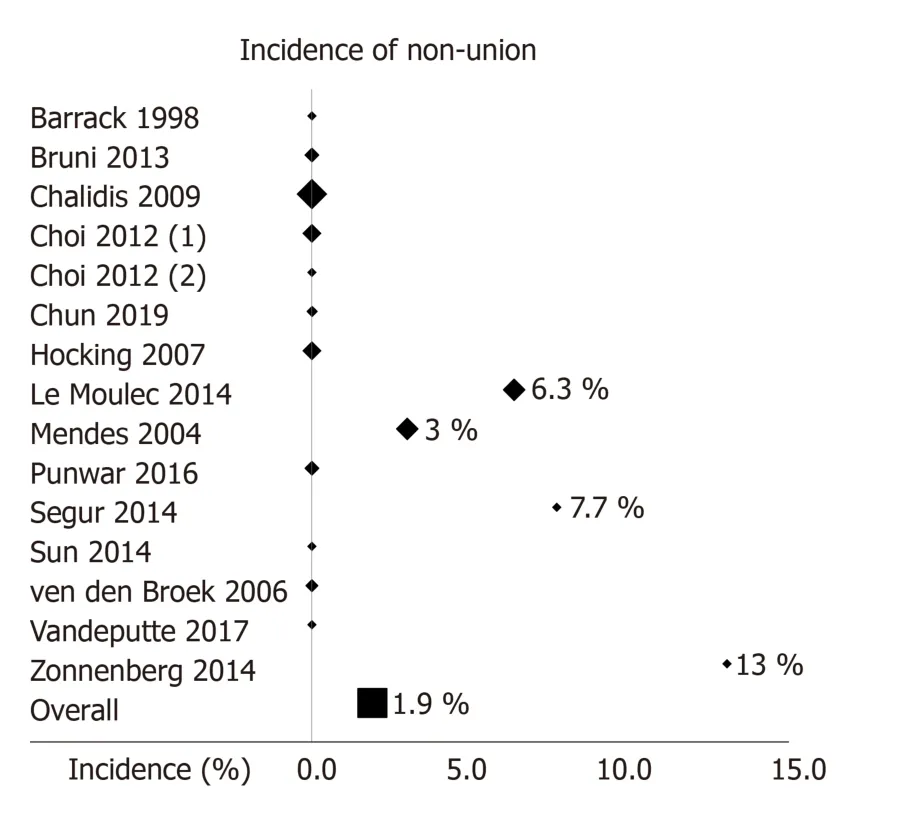
Figure2 Forest plot of the incidence of non-union of the tibial tubercle osteotomy.The markers are weighted according to the number of the cases of each study.
ARTICLE HIGHLIGHTS
Research background
Tibial tubercle osteotomy (TTO) is a useful technique to deal with a stiff knee in revision total knee arthroplasty (RTKA).It provides excellent exposure and visualization of the knee joint as it allows unforceful eversion or lateral subluxation of the patella.Complications such as nonunion,tibial tubercle migration and fragmentation,and metalware related pain have been reported.
Research motivation
Although TTO is widely utilized in RTKA,several reports have reported potential osteotomyrelated complications.There is currently a lack of synthesis of the evidence about TTO in RTKA.
Research objectives
The present review aims to evaluate the availabl e literature and estimate the efficiency of TTO in RTKA in terms of osteotomy union,knee mobility,and complications.
Research methods
Medline,Scopus,and the Cochrane Central Register of Controlled Trials were systematically screened for studies from inception to February 2020.The main outcome was the incidence of union of the osteotomy.Secondary outcomes were the knee range of motion as well as the TTOrelated and overall procedure complication rate.The systematic review was conducted following the PRISMA recommendations.
Research results
Fifteen clinical studies were included in the systematic review.Eleven non-unions out of 593 TTOs were reported (union rate 98.1%).Proximal migration of the TT was observed in 41 cases(6.9%).Anterior knee pain was reported in 38 cases (6.4%),13 of which required hardware removal (2.2%).Total knee range of motion improved from 73.4° preoperatively to 97°postoperatively and knee flexion increased from 82.9° before surgery to 100.1° after surgery.Stiffness requiring manipulation under anesthesia was evident in 27 cases (4.6%).
Research conclusions
TTO shows great clinical safety and efficacy in RTKA.Non-union is rare,and the most reported TTO-related complications are proximal migration and anterior knee pain.However,in the vast majority of cases they aren't associated with secondary procedures.
Research perspectives
Further clinical studies are encouraged to determine the optimal extensile approach in RTKA.High quality randomized studies comparing different techniques using standardized protocols will need to be performed.