Muscle strength cut-offs for the detection of metabolic syndrome in a nonrepresentative sample of collegiate students from Colombia
2020-06-10AntonioGariaHrmosoAljanraTorillaSanrsJorgEnriquCorraBautistaMarkPtrsonMiklIzquiroAuraCristinaQuinovilaCarolinaSanovalCullarKathrinGonzlzRuRoinsonRamrzlz
Antonio Garia-Hrmoso ,Aljanra Torilla-Sanrs ,Jorg Enriqu Corra-Bautista ,Mark D.Ptrson ,Mikl Izquiro ,Aura Cristina Quino-Ávila ,Carolina Sanoval-Cullar ,Kathrin Gonzálz-Ruíz ,Roinson Ramírz-Vélz
a Physical Activity,Sport and Health Sciences Laboratory,University of Santiago de Chile,Santiago de Chile 7500618,Chile
b Center of Studies in Physical Activity Measurements,School of Medicine and Health Sciences,Universidad del Rosario,Bogotá 111221,Colombia
c Department of Physical Medicine and Rehabilitation,University of Michigan,Ann Arbor,Michigan 48109,USA
d Department of Health Sciences,Public University of Navarre,CIBERFES(CB16/10/00315),Navarre 31009,Spain
e CORPS Group,Faculty of Health Sciences,University of Boyacá,Boyacá,Tunja 153610,Colombia
f Physical Exercise and Sports Research Group,Manuela Beltrán University,Bogotá 111221,Colombia
Abstract Background:Evidence shows an association between grip strength and health;however,grip strength cut-offs for the detection of metabolic syndrome(MetS)in Latin American populations are scarce.The purpose of this study was to determine cut-offs of normalized grip strength(NGS)for the detection of MetS in a large nonrepresentative sample of a collegiate student population from Colombia.Methods:A total of 1795 volunteers(61.4%female;age=20.68±3.10 years,mean±SD),ranging between 18 and 30 years of age participated in the study.Strength was estimated using a handheld dynamometer and normalized to body mass(handgrip strength(kg)/body mass(kg)).Anthropometrics,serum lipids indices,blood pressure,and fasting plasma glucose were measured.Body composition was measured by bioelectrical impedance analysis.MetS was defined as including ≥3 of the 5 metabolic abnormalities according to the International Diabetes Federation definition.A metabolic risk score was computed from the following components:waist circumference,triglycerides,high-density lipoprotein cholesterol,glucose,and systolic and diastolic blood pressure.Results:Receiver operating curve analysis showed significant discriminatory accuracy of NGS in identifying the thresholds and risk categories.Lower strength was associated with increased prevalence of MetS.In males,weak,intermediate,and strong NGS values at these points were<0.466,0.466-0.615,>0.615,respectively.In females,these cut-off points were <0.332,0.332-0.437,>0.437,respectively.Conclusion:Our sex-specific cut-offs of NGS could be incorporated into a clinical setting for identifying college students at cardiometabolic disease risk.2095-2546/©2020 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords:Cardiometabolic risk;Muscular fitness;Receiver operating characteristic curve;Thresholds
1.Introduction
Muscular weakness,as determined with the use of a handgrip dynamometer,is recognized as a marker of health risk,similar to that observed for conventional risk factors.1-3López-Martínez et al.3demonstrated that muscle strength is negatively associated with metabolic syndrome(MetS)in young adults.Additionally,in a prospective study(follow-up in young adulthood for 20 years),Fraser et al.4showed that those in the lowest third tertile of strength were independently associated with adult MetS.Similarly,our group5,6and other investigators7-9have shown an independent and inverse association between low strength and cardiometabolic risk clustering among adolescents and adults. The contribution of muscular weakness to the progression of sedentary behavior with aging and/or cardiometabolic risk factors(e.g.,obesity,MetS,insulin resistance)is equally unequivocal,and recent national efforts to identify cut-offs or thresholds for clinically relevant weakness among young people10will help clinicians screen individuals at greatest risk.11,12
Senechal et al.11determined low muscle strength cut-offs for the prediction of MetS among middle-aged and older males using a composite score of normalized strength from chest press and leg press from a sample of 5685 men aged <50 years and 1541 men aged ≥50 years.However,at this time,thresholds derived from handgrip muscle strength,a clinically relevant strength measure, among Latin-American college students remains to be determined.Moreover,even though there is scientific evidence regarding the role of muscle strength preservation for prevention against cardiometabolic risk in several populations,no studies have established the minimum strength capacity associated with the risk of MetS among Latin-American college students.Clinically relevant handgrip strength cut-offs for detecting MetS have been established for youths,6adults,11and older adults.7,8
However,Leong et al.13reported considerable heterogeneity in median handgrip strength among 125,462 healthy adults aged 35-70 years from 21 countries in the Prospective Urban Rural Epidemiology study.This finding is important because it has been reported that handgrip strength is predictive of mortality and cardiovascular disease(CVD)independently of country income.14Therefore,from a public health perspective,the inclusion of handgrip strength measures in health surveillance systems is clearly justifiable.For example,moderate weight gain from early to middle adulthood is associated with significantly increased risk of major chronic diseases and mortality.2Therefore,young adults may also be a good population for monitoring fitness,identifying risk factors,and offering interventions among those at high cardiometabolic risk.For that,cut-offs to determine young adults at caridiometabolic risk are required and to be used later to promote muscular strength and to lower CVD risk in later life.
Thus,our study aimed to determine cut-offs of grip strength for the detection of MetS in a large collegiate student population from Colombia.Such evidence could serve as proof of a concept for the development of broad normative reference test standards for clinical,academic,and community settings.
2.Methods
2.1.Participants and study design
Data were from a cross-sectional component of the FUPRECOL(in Spanish,Asociación de la Fuerza Prensil con Manifestaciones Tempranas de Riesgo Cardiovascular en Adultos Colombianos) study conducted during the 2014-2017 academic years.We recently published a complete description of the FUPRECOL study design,methods,and primary outcomes for our current cohort.9A convenience sample comprised 1795 volunteers(61.4%female;age=20.68±3.10 years,mean±SD)between ages 18 and 30 years of low to middle socioeconomic status,which was evaluated in accordance with the following Colombian government classification: Stratum 1-2=low, Stratum 3-4=middle,and Stratum 5-6=high).The sample comprised students enrolled in public or private universities from 3 distinct areas of Colombia:the capital district of Bogota(Cundinamarca),Tunja(Boyacá),and Santiago de Cali(Valle del Cauca).
Exclusion criteria included medical or clinical diagnosis of a major systemic disease,including malignant conditions such as cancer,type 1 or 2 diabetes,high blood pressure,and hypothyroidism or hyperthyroidism;a history of drug or alcohol abuse;regular use of multivitamins;chronic inflammatory conditions including rheumatoid arthritis, systemic lupus erythematosus,and multiple sclerosis;infectious conditions;or a body mass index(BMI)≥35 kg/m2.Volunteers were not compensated for their participation.Informed consent was obtained from each participant. All participants provided written consent,and each study was approved by the local authorized institutional review boards(Bogotá UMB Code N˚ 01-1802-2013, UR Code N˚CEI-ABN026-000010; Cali UNIAJC Code N˚111-02.01.48/16;Tunja Code N˚RECT 60)and complied with the Declaration of Helsinki(World Medical Association for Human Subjects).The students who agreed to participate and who had signed the informed consent form were given appointments for the procedures described in the following.
2.2.Physical examination
Subjects were screened for inclusion in the study via personal interviews.Interview questions included queries about health status,medical history,CVD risk factors,and lifestyle.After completing another general information questionnaire,participants were instructed to wear shorts and t-shirts to the physical examination.They were also required to remove all jewelry and metal objects.Once the subjects were barefoot and in their underwear,their body weight(kg)was measured using an electric scale(Tanita Model BC-418;Tanita Corp.,Tokyo,Japan)with a range of 0-200 kg and with an accuracy within 100 g.Height was measured with a portable stadiometer with a precision of 0.10 mm and a range of 0-2.50 m(Seca 274;Vogel and Halke,Hamburg,Germany).BMI was calculated by using the following formula:body mass(kg)/height(m)2.BMI status was evaluated according to the World Health Organization criteria.15The waist circumference(WC)was measured in cm as the narrowest point between the lower costal border and the iliac crest.When this point was not evident,it was measured at the midpoint between the last rib and the iliac crest,using a metal tape measure(Lufkin W606PM;Cooper Tools,Parsippany,NJ,USA).The evaluation process was carried out by a team of professionals(4 physical therapy professors)with extensive experience in anthropometric measurement.Measurements for 2%of the sample was carried out twice to ensure quality of measures.The technical error of measurement(TEM)values were <2%for all anthropometric variables.
Body fat percentage(BF%)and fat mass index(FMI)were determined for bioelectrical impedance analysis(BIA)by a tetrapolar whole-body impedance (Tanita Model BC-418;Tanita Corp.).For the calculation of intra-and inter-observer TEM,at least 50 subjects needed to be measured(30 males,20 females,aged 22.3±2.1 years).The Tanita Model BC-418 is a reliable system that has good agreement with laboratorybased methods of assessment(hydrostatic weighing:r=0.81,p <0.05;error of 1.68 BF%or Dual-energy X-ray absorptiometry(DXA):r=0.87,p <0.001).16,17The corresponding intraobserver technical error(%reliability)of the measurements was 95%.A detailed description of the BIA technique can be found elsewhere.18Before testing,participants were required to adhere to the BIA manufacturer’s instructions(http://www.tanita.com/es/bc-418/),including not to(i)eat or drink within 4 h of the test;(ii)consume caffeine or alcohol within 12 h of the test;(iii)take diuretics within 7 days of the test;(iv)do physical exercise within 12 h of the test,and(v)urinate within 30 min of the test.FMI was calculated by dividing each subject’s fat mass(kg)by the square of his or her height(m)2,as described previously.19
2.3.Muscular strength
Handgrip strength was assessed using an adjustable digital handgrip dynamometer(T-18 TKK SMEDLY III;Takei Scientific Instruments Co.,Ltd.,Niigata,Japan).Participants watched a brief demonstration of the technique and were given verbal instructions on how to perform the test.The dynamometer was adjusted according to the subjects’hand size based on a predetermined protocol.20The best score for each hand was recorded in kg.The handgrip strength was calculated as the average of the left and right hand.Because there is substantial covariance between strength capacity and body mass,and because the link between strength and both physical function and chronic health is directly mediated by the proportion of strength relative to body mass,handgrip strength was a normalized grip strength(NGS)per body mass—for instance,handgrip strength(kg)/body mass(kg).The reproducibility of our data was R=0.96.Intra-rater reliability was assessed by determining the intra-class correlation coefficient (0.98, 95% confidence interval (CI):0.97-0.99,n=20,median age=22.88±1.41 years,median weight=66.2±5.41 kg,median height=1.75±0.10 m,median BMI=24.91±3.12 kg/m2).
2.4.MetS diagnosis
After the subjects had fasted for 10-12 h,blood samples were obtained from capillary sampling from 6:00-10:00 a.m.Participants were asked not to engage in prolonged exercise in the 24 h prior to testing.The biochemical profile included the following:(i)high-density lipoprotein cholesterol(HDL-C),(ii)triglycerides (TG), (iii) low-density lipoprotein cholesterol(LDL-C),(iv)total cholesterol,and(v)glucose fasting by enzymatic colorimetric methods.Inter-assay reproducibility(coefficient of variation)was determined from 80 replicate analyses of 8 plasma pools over a period of 15 days.The percentages obtained were 2.6% (TG), 2.0% (total cholesterol), 3.2%(HDL-C),3.6%(LDL-C),and 1.5%(fasting glucose).
Blood pressure was taken on the left arm at the heart level with the automatic device Omron M6 Comfort (Omron Healthcare Europe B.V.,Hoofddorp,The Netherlands)while the participants were sitting still.The blood pressure monitor cuff was placed 2-3 finger-widths above the bend of the arm,and a 2-min pause was allowed between the first and the second measurement with a standard cuff for an arm circumference of 22-32 cm.The mean arterial pressure(MAP)was calculated using the following formula:MAP=(systolic blood pressure+(2×diastolic blood pressure))/3.
Participants were considered to have diagnoses of the MetS if they had ≥three of the following:(i)abdominal obesity(WC ≥80 cm in females and WC ≥90 cm in males),(ii)hypertriglyceridemia(≥150 g/dL),(iii)low HDL-C(<50 mg/dL in females and <40 mg/dL in males),(iv)high blood pressure(systolic blood pressure ≥130 mmHg or diastolic blood pressure ≥85 mmHg)or MAP ≥100 mmHg,and(v)high fasting glucose(≥100 mg/dL).MetS was defined in accordance with the updated harmonized criteria of the International Diabetes Federation(IDF).21
We calculated a composite MetS score that reflects a continuous score of the 5 MetS risk factors.The MetS score was calculated from the individual subjects’data,based on the IDF,21and the SDs were calculated using data from the entire subject cohort at baseline. The equation used was MetS score=((HDL-C:male ≤40 mg/dL or female ≤50 mg/dL)/(SD:female=1.04 or male=-0.19))+((TG:150 mg/dL)/(SD: female=0.99 or male=97))+((fasting glucose: 100 mg/dL)/(SD: female=0.98 or male=1.02))+((WC: male≥94 cm or female ≥80 cm)/(SD: female=0.99 or male=0.94))+((MAP:100 mmHg)/(SD:female=0.88 or male=1.07)).The mean of this continuously distributed MetS score was therefore 0 by definition.
2.5.Lifestyle covariates
A standardized questionnaire,the“FANTASTIC”lifestyle(family,physical activity(PA),nutrition,tobacco toxins,alcohol,sleep/stress,personality type,insight,and career),was used to collect comprehensive information about substance use via a personal interview with participants.Alcohol consumption and smoking status were defined as subjects who had consumed any alcoholic beverage ≥1 time per week and those who had smoked ≥10 cigarettes per week for at least 6 months,respectively,as previously described by Ramírez-Vélez et al.22Participants who exercised ≥3 times a week for>30 min were categorized as“physically active”,and those who exercised <3 times a week were considered“physically inactive”.22
2.6.Statistical analysis

3.Results
The 1795 volunteers included 1103 females(61.4%).Their mean age was 20.68±3.10 years.Overall,males had greater body weight,WC,blood pressure,high TG,and PA levels than females(p ≤0.001),whereas females had lower handgrip and NGS(p <0.001).The prevalence of overweight and obesity was 21.31% and 5.53% in females, respectively(p <0.001)(Table 1).In males,the prevalence of overweight and obesity was 20.81%and 4.77%,respectively(p <0.001).It was observed that 40.75%of males had high blood pressure.Total cholesterol,and LDL-C levels were significantly higher in females than in males(p <0.05).
Table 2 depicts ROC curve analysis for the diagnostic performance NGS in identifying weak,intermediate,and strong risk of MetS.Since multiple levels of risk were desired,the selection of the resulting cut-off values was based on multiple combinations of sensitivity and specificity.In males,NGS values for weak,intermediate, and strong were <0.466, 0.466-0.615, and>0.615,respectively.In females,these cut-offs were <0.332,0.332-0.437,and >0.437,respectively(Table 2).
Mean differences in anthropometrics,cardiometabolic risk,and muscle strength parameters according to NGS categories are shown in Table 3.In males and females,analysis of variance adjusted for age,tobacco,alcohol,and PA levels showed that there were differences in body weight,FMI,and muscle strength(all p <0.05).
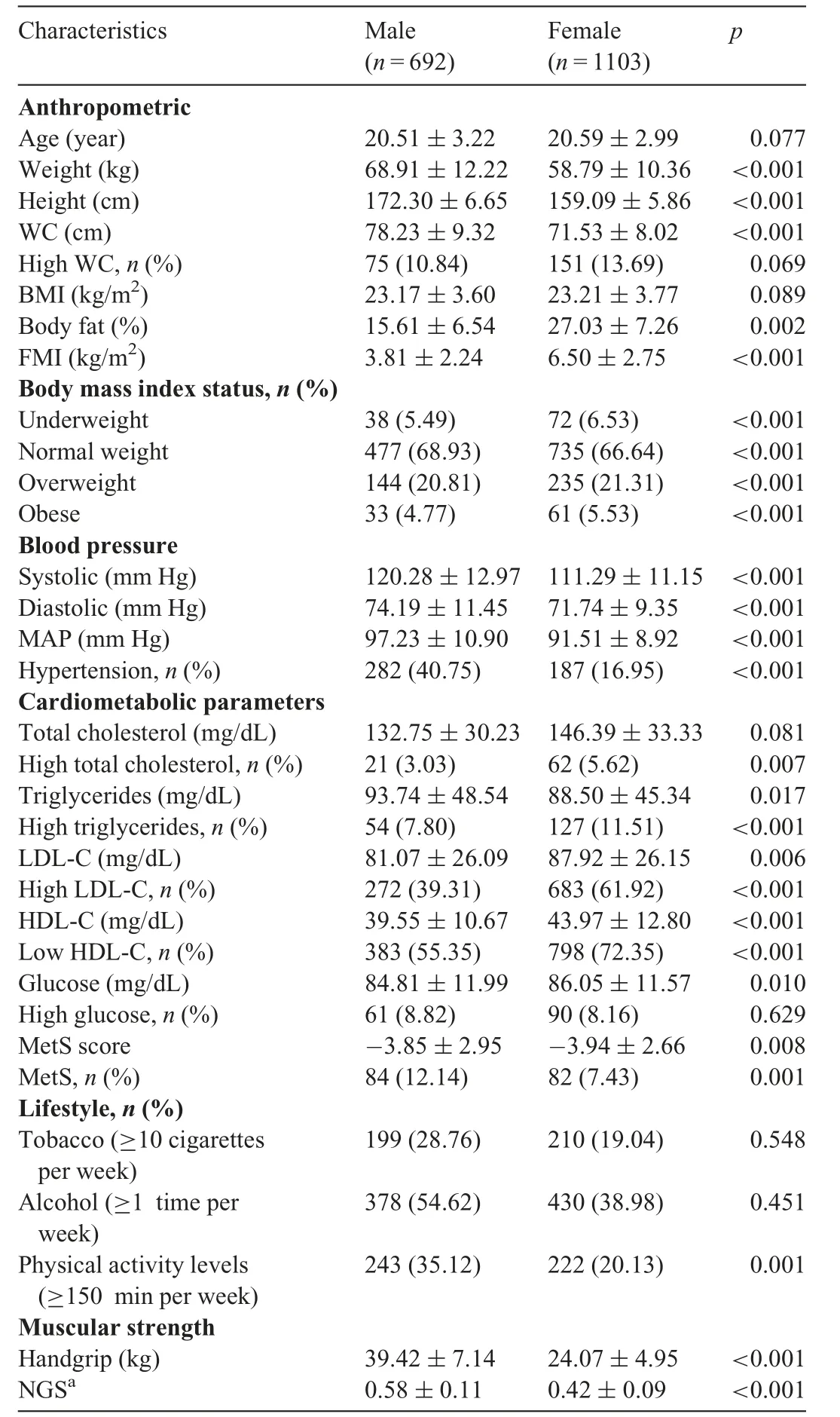
Table 1 Characteristics among a sample of college students from Colombia(n=1795).
Conditional inference trees predicting probability of the high-risk cardiometabolic phenotype(MetS according to the IDF criteria) confirmed different low strength thresholds between males and females.Fig.1 provides results for the primary definition.The first cut-off point identified in males was based on having NGS <0.466 vs.≥0.466.Within the group of subjects with NGS ≥0.466,a second cut-off point was identified as an NGS ≤0.615.Among the weakest males(NGS<0.466),34.6%had MetS,as compared with 10.7%amongmales with intermediate NGS(0.466-0.615),and only 4.9%among males with the highest NGS(>0.615).Among females,the first identified cut-off was based on having an NGS ≤0.437 vs.>0.437.Within the group of subjects with an NGS≤0.437,a second cut-off point was identified as an NGS≥0.332.Among the weakest females(NGS <0.332),18.0%had MetS,as compared with 7.9%among females with intermediate NGS(0.332-0.437)and only 2.4%among females with the highest NGS(>0.437).

Table 2 Parameters of the ROC curves analysis for the diagnostic performance of NGS inidentifying weak,intermediate,and strong risk of MetS according to the IDF criteria in males and females.
Fig. 2 provides plots of the association between NGS and MetS score for males and females.Inspection of the locally weighted scatterplot smoothing curves provides evidence of a well-defined threshold effect of low strength on the MetS score as a continuous outcome.
4.Discussion
This is one of the first studies to identify sex-specific cutoffs for NGS to detect a high-risk cardiometabolic phenotype among a large population of college students.The role of muscular strength has been increasingly recognized in the prevention of chronic disease in adult populations.1-3Evidence suggests that muscle mass and strength decrease progressively after the age of 20 years,24whereas in old age,some grip strength and hip strength declines by an average of 1.10 kg per year and 1.31 kg per year,respectively.25Therefore,young adulthood seems to be crucial time frame for monitoring and intervening to reduce the risk of weakness and cardiometabolic disease.
Few studies have proposed cut-offs for low muscular strength among adults for screening cardiometabolic risk;however,this has yet to receive adequate attention in young adult populations,and information is scarce.Most studies have analyzed the older adult population.For example,Lee et al.26demonstrated that cardiometabolic risk was 54%lower for individuals with relative handgrip strength(absolute handgrip strength divided by BMI)in the 75th percentile compared with the 25th percentile.In addition,Duchowny et al.27established cut-off points for muscle weakness assessed as handgrip strength in a nationally representative sample by race and sex among older American adults.Senechal et al.11determined low muscle strength cut-off points for the prediction MetS using a composite score of normalized strength from the chest press and leg press.Among middle-aged adults,Strand et al.28revealed an association between handgrip strength and allcause mortality and cardiovascular mortality,confirming the role of handgrip strength as a mortality predictor.29Finally,among young adults,Wilkerson et al.30investigated 62 collegiate football players(mean age 19.9 years)and found that low leg muscle strength was associated with an increased likelihood of MetS.
In line with studies mentioned earlier,our study revealed cut-offs for NGS by sex and identified 3 cardiometabolic risk categories (“high”, “intermediate”, and “low”). The ROC curves generated for this study showed acceptable AUCs and 95%CI limits,suggesting that the resultant cutoffs were not owing to chance(both AUC ≥0.72).Specifically,among males in the highest strength category,only 4.9%had the MetS phenotype,as compared with 10.7%among males with intermediate strength and 34.6%among males with low strength.Among the females in the highest strength category,only 2.4%had the MetS phenotype,as compared with 7.9% among females with intermediate strength and 18.0%among those with low strength.The identification of the 3 categories of cardiometabolic risk coincides with the findings of Peterson et al.,31who determined by sex the distribution of high cardiometabolic risk according to the cut-off points: weak, intermediate, and strong.These cut-off points were obtained from a similar size sample but not related to the age range.The cut-off points are lower than those identified in our study.
However, the AUCs observed for this threshold were 0.72-0.74 for males and 0.72 for females,whereas in the study performed by Senechal et al.,11the AUCs were 0.65 for males and 0.81 for females.The lower sensitivity and specificity reported in our study might be related to differences in age(20-50 years vs.18-30 years),sample size of the populations studied(1795 vs.5685),and the methods used to assess muscle strength(handgrip vs.leg and bench press),as well as the use of a composite measure of MetS.Thus,our findings reinforce the concept that muscle strength may be an important modifiable lifestyle factor for CVD risk assessment in the same way that physical inactivity,body composition,and healthy dietary patterns are important.
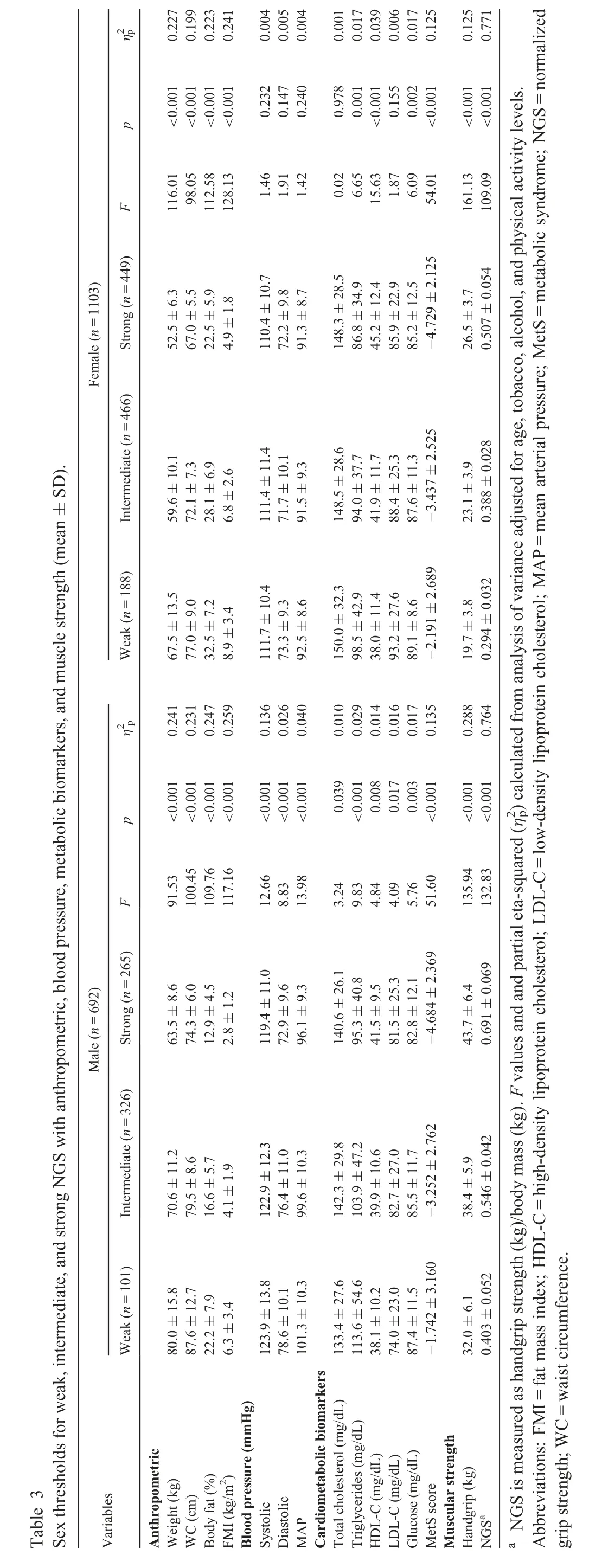
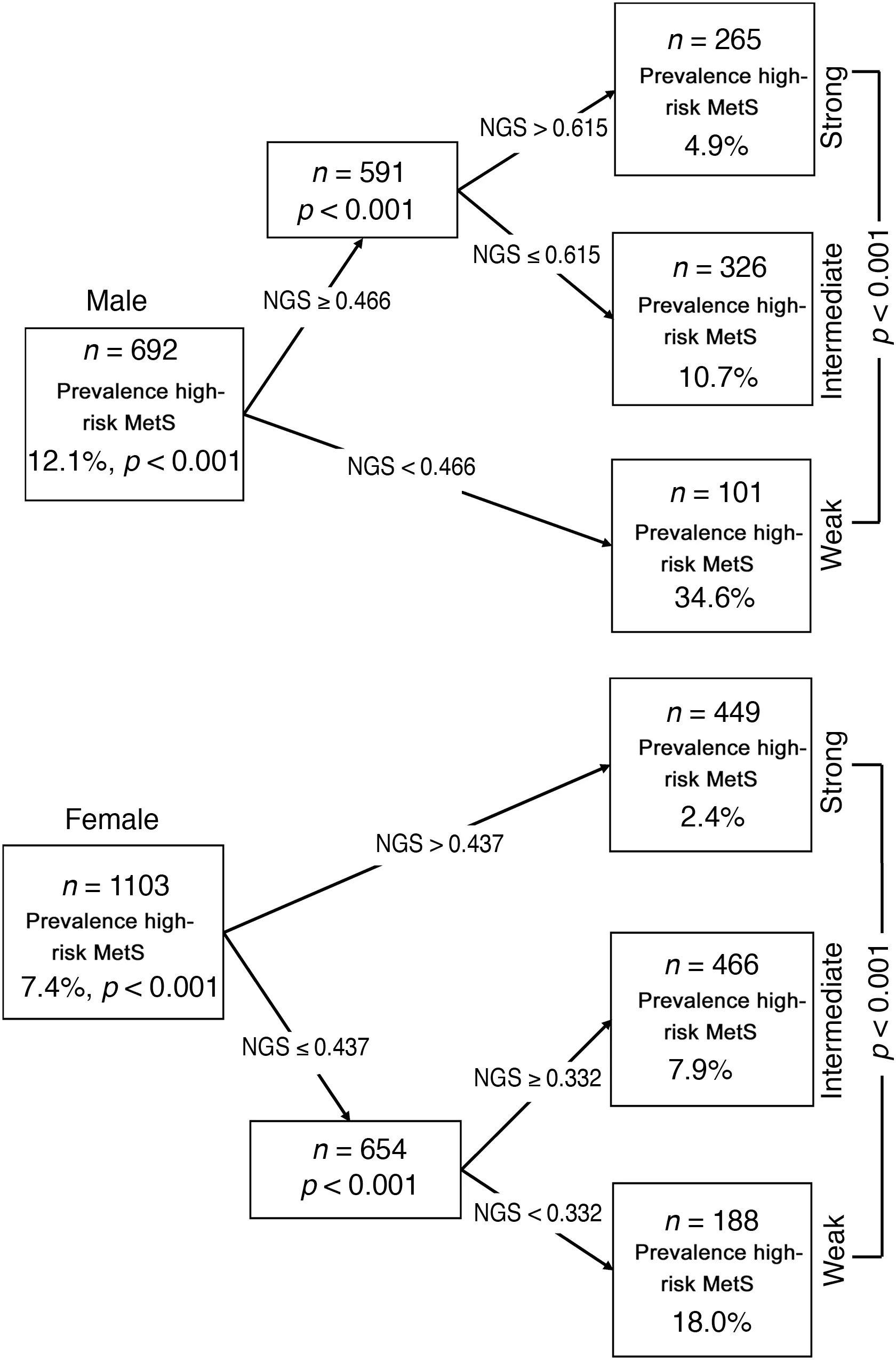
Fig. 1.Conditional inference trees for NGS,as predictors in identifying risk of MetS according to the IDF criteria in males and females.NGS is measured as grip strength(kg)/body mass(kg).IDF=International Diabetes Federation;MetS=metabolic syndrome;NGS=normalized grip strength.
Our findings therefore support previous results demonstrating that low muscle strength is associated with MetS.These findings coincide with Sasaki et al.,32in which for each 5-kg increase in grip strength,the number of deaths caused by heart disease and stroke diminishes significantly.A plausible explanation for the role of muscle strength in MetS prevalence may be through the metabolic and structural changes that improve muscle insulin sensitivity and glycemic control.33As demonstrated by Wu et al.34in a recent meta-analysis,there is a 63%higher risk of premature mortality owing to CVD among adults with low handgrip muscle strength.

Fig.2.Scatterplots with overlaid locally weighted scatterplot smoothing curves to depict the shape of the association between the NGS and MetS score by sex.NGS is measured as grip strength(kg)/body mass(kg).MetS=metabolic syndrome;NGS=normalized grip strength.
The strengths of this study include the large sample size and a commonly used and feasible test for assessing muscle strength.However,there are some limitations that need to be highlighted. First, owing to the cross-sectional nature of the study design,we were unable to draw causal relationships.Thus,we were unable to deduce whether low NGS leads to increased risk of MetS,or conversely whether poor cardiometabolic profiles lead to declines in muscle strength.Future longitudinal studies are needed to better understand how declines in muscle strength contribute to health risks in college-aged adults.Second,the ROC curve analysis does not enable adjustments for potential confounders within the model,and data were not adjusted prior to ROC curve analysis.Finally,we only analyzed relatively healthy individuals;therefore,the generalization of our results is limited to healthy younger adults.Our study suggests that NGS could be used as a complementary tool that may help clinicians and practitioners screen for high cardiometabolic risk.
5.Conclusion
In summary,our sex-specific NGS cut-offs could be incorporated into a clinical setting for identifying college students at high cardiometabolic disease risk and used as a target for strength training programs designed to reduce the risk of MetS. Longitudinal studies are necessary to determine if increasing handgrip strength reduces the likelihood of MetS.
Acknowledgments
The authors gratefully acknowledge the contributions of Elisa Andrea Cobo, Boyacá University, that assisted the authors in obtaining data. We also acknowledge Monica Ojeda,Boyacá University,for assistance with data analysis.Both of their contributions were without compensation.This study was part of the project entitled Body Adiposity Index and Biomarkers of Endothelial and Cardiovascular Health in Adults,which was funded by the Centre for Studies on Measurement of Physical Activity,School of Medicine and Health Sciences, Universidad del Rosario (Code N˚FIUR DNBG001)and Universidad de Boyacá(Code N˚RECT 60).The funder had no role in the study design,data collection,data analysis and interpretation,preparation of the manuscript,or decision to publish.
Authors’contributions
RRV,KGR,and JECB conceived the study,designed it,and analyzed the data;AGH,ATS,MDP,MI,ACQA,and CSC analyzed the data and wrote the article.All authors have read and approved the final manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
杂志排行

Journal of Sport and Health Science的其它文章
- Impacts of exercise intervention on various diseases in rats
- Reply to“Is physical performance(in mice)increased by Veillonella atypica or decreased by Lactobacillus bulgaricus?”
- Land-walking vs.water-walking interventions in older adults:Effects on aerobic fitness
- Longitudinal associations of physical activity and pubertal development with academic achievement in adolescents
- Increased Q-Factor increases frontal-plane knee joint loading in stationary cycling
- Transition to forefoot strike reduces load rates more effectively than altered cadence