Increased Q-Factor increases frontal-plane knee joint loading in stationary cycling
2020-06-10TannerThorsenKelleyStrohackerJoshuaWeinhandlSongningZhang
Tanner Thorsen,Kelley Strohacker,Joshua T.Weinhandl,Songning Zhang
Department of Kinesiology,Recreation and Sport Studies,The University of Tennessee,Knoxville,TN 37996,USA
Abstract Background:Q-Factor(QF),or the inter-pedal width,in cycling is similar to step-width in gait.Although increased step-width has been shown to reduce peak knee abduction moment(KAbM),no studies have examined the biomechanical effects of increased QF in cycling at different workrates in healthy participants.Methods:A total of 16 healthy participants(8 males,8 females,age:22.4±2.6 years,body mass index:22.78±1.43 kg/m2,mean±SD)participated.A motion capture system and customized instrumented pedals were used to collect 3-dimensional kinematic(240 Hz)and pedal reaction force(PRF)(1200 Hz)data in 12 testing conditions:4 QF conditions—Q1(15.0 cm),Q2(19.2 cm),Q3(23.4 cm),and Q4(27.6 cm)—under 3 workrate conditions—80 watts(W),120 W,and 160 W.A 3×4(QF×workrate)repeated measures of analysis of variance were performed to analyze differences among conditions(p <0.05).Results:Increased QF increased peak KAbM by 47%,56%,and 56%from Q1 to Q4 at each respective workrate.Mediolateral PRF increased from Q1 to Q4 at each respective workrate.Frontal-plane knee angle and range of motion decreased with increased QF.No changes were observed for peak vertical PRF,knee extension moment,sagittal plane peak knee joint angles,or range of motion.Conclusion:Increased QF increased peak KAbM,suggesting increased medial compartment loading of the knee.QF modulation may influence frontal-plane joint loading when using stationary cycling for exercise or rehabilitation purposes.2095-2546/©2020 Published by Elsevier B.V.on behalf of Shanghai University of Sport.This is an open access article under the CC BY-NC-ND license.(http://creativecommons.org/licenses/by-nc-nd/4.0/).
Keywords:Cycling biomechanics;Inter-pedal distance;Knee abduction moment;Knee adduction moment;Q-Factor
1.Introduction
Cycling is a common form of sport,transportation,and recreation that encourages many health benefits.1Compared to walking or jogging,cycling promotes cardiorespiratory fitness and muscle strength with reduced loading demands on the knee joint.2-4Peak knee contact force,for example,has been shown to reach between 0.5 and 1.5 body weight in cycling compared to nearly 2.5 times body weight in walking and greater than 6 times body weight in jogging.3,5,6
Sagittal plane biomechanics of the knee during cycling have been studied extensively.2,7-10With respect to performance,injury prevention,and rehabilitation,it is important to understand not only sagittal plane joint kinetics,which dictate overall knee joint loading,but also frontal-plane joint kinetics,reflected by the internal knee abduction moment(KAbM).Cycling-overuse injuries resulting in medial knee pain as well as pathologies such as knee osteoarthritis(OA)may be influenced by the magnitude of KAbM.11,12Although the overall joint loading in cycling is reduced compared to walking or jogging,understanding how KAbM is influenced during cyclic repetitive exercise may be of particular interest for people with knee pathologies and for cyclists and clinicians.
KAbM has been used as a surrogate variable for medial compartment knee loading during walking13-15and cycling.4,11,16In gait-modification research,increased step width has been shown to reduce KAbM in level walking,17stair ascent,18and stair descent.15Recent cycling research has investigated frontal-plane biomechanics with respect to foot progression angles,12lateral shoe wedges,11cadence and workrate manipulation,16and lower limb alignment.4Results of these studies indicate that for healthy participants,manipulation of foot progression angle,12differences in lower limb alignment(varus,valgus,and neutral),4and cycling cadence16had no significant effect on peak KAbM.Implementation of a 10˚lateral shoe wedge decreased KAbM,11while increasing workrate increased KAbM.16
Q-Factor(QF)refers to the horizontal distance between bike pedals.19It is typically measured from the outside face of 1 crank arm to the other crank arm(Fig.1A).19QF in cycling is similar to step-width in gait.Preferred step-width has been reported to be between 7 and 12 cm in normal walking,20-2213 and 17 cm in stair ascent,13-15and 15 and 17 cm in stair descent.14,15Generally,QFs range from approximately 15 cm on a road bike to approximately 18 cm on a mountain bike,with no mass-produced bicycle having a QF lower than 13.5 cm.19
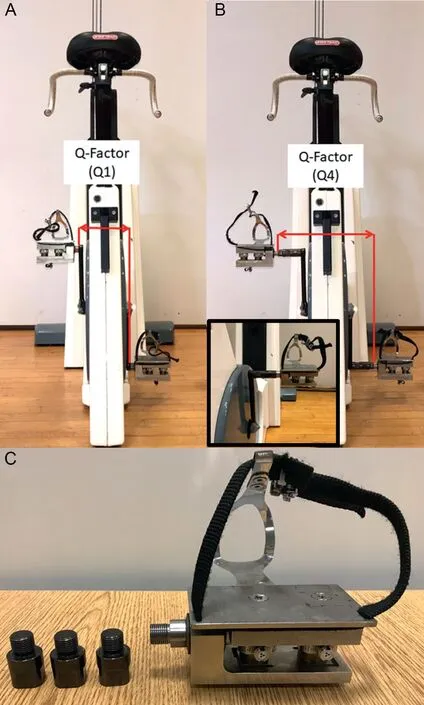
Fig.1.(A)Instrumented bicycle pedals with Q-Factor set at Q1;(B)with Q-Factor set at Q4 with a close-up view of the pedal with the 3 extenders in the lower left corner;(C)right-instrumented bicycle pedal with 3 individual QF extenders.
To our knowledge,there have been no cycling studies examining the effects of increased QF on knee joint biomechanics.Manipulation of QF has been examined in 2 studies investigating mechanical and metabolic efficiency among trained and recreational cyclists.19,23Smaller QF resulted in greater gross mechanical efficiency,23with no effect on the level and timing of selected lower extremity muscle activations for trained cyclists.19QF modulation,as a frontal-plane modification,may have greater potential to influence KAbM than sagittal plane adjustments because many commonly accepted bike-fit practices focus primarily on adjustments in the sagittal plane,such as saddle height,24handlebar fore/aft position,25and saddle fore/aft position.25Furthermore,the effect of increased QF as workrate increases is unclear.Recently,Fang et al.16demonstrated that increased workrate, but not cadence, increased KAbM. If increased step-width during gait decreases KAbM,but increased workrate increases KAbM in cycling,it is plausible that increasing QF may,to some degree,mediate the effect of workrate on KAbM.The purpose of this study,therefore,was to examine effects of standard and increased QFs at different workrates on the knee biomechanics of healthy,untrained participants during stationary cycling.It was hypothesized that as QF increases,peak KAbM would decrease,and as QF increases further,the frontalplane knee moment would become an adduction moment.Furthermore,it was hypothesized that with increased workrate,the frontal-plane knee moment would increase,and peak knee extension moment would not change significantly.
2.Methods
2.1.Participants
A total of 16 recreationally active young adults(8 males,8 females,age:22.4±2.6 years,height:1.74±0.11 m,body mass index:22.78±1.43 kg/m2,mean±SD)participated.Being recreationally active was defined as engaging in moderate-to-vigorous activity 3 days or more per week for a total of ≥150 min/week,26with less than 3 h/week of cycling.All participants were free from lower extremity injury within the past 6 months.An a priori power analysis for a repeated measures analysis of variance,using KAbM and knee extension moment from previous research,16indicated that a sample size of 16 was needed for an α of 0.05 and a β of 0.80 with a conservative effect size of 0.25(G*Power 3.1;Heinrich Heine University Dusseldorf,Dusseldorf,Germany).All participants signed a written informed consent document approved by the University of Tennessee,Knoxville,institutional review board.
2.2.Instrumentation
A 12-camera motion analysis system (240 Hz; Vicon Motion Analysis Inc.,Oxford,UK)was used for 3-dimensional(3D)kinematic data collection.Participants wore tightfitting spandex shorts,a t-shirt,and neutral running shoes(Pegasus,Nike,Beaverton,OR,USA).Retroreflective anatomic markers were placed bilaterally on the acromion process,iliac crest, greater trochanter, medial and lateral epicondyles,medial and lateral malleoli,head of the 5th metatarsal,head of the 1st metatarsal,and the 2nd toe.A semirigid thermoplastic shell with 4 retroreflective tracking markers was placed on the shanks,thighs,pelvis,and trunk.Four individual retroreflective tracking markers were affixed to the heel counter of each shoe.
Participants cycled on a Lode cycle ergometer(Excalibur Sport,Lode,Groningen,Netherlands).Saddle height was set at a height with 25˚to 30˚knee flexion,measured with a hand-held goniometer when the pedal was placed at the bottom,dead center.27The saddle fore/aft position was also adjusted such that the participant’s knee was in line with the pedal spindle when the crank was in the forward horizontal(90˚)position.4The handlebar position was set such that the angle between the participant’s trunk and thigh was 90˚,measured by a handheld goniometer when the crank was at 90˚.4
Two customized instrumented bike pedals were used to collect pedal reaction forces(PRF)on the Lode cycle ergometer.Each pedal assembly contained two 3D force sensors(Type 9027C;Winterthur,Kistler,Switzerland),and each force sensor was coupled with an industrial charge amplifier(Type 5073A,Kistler).4A custom jig was built to secure the bike to a floor-mounted force platform to align it with the laboratory’s global coordinate system.16Prior to using the pedal assemblies,extensive calibration testing was done to ensure that the pedal reaction force and center pressure measurements were accurate.11
QF was measured from the outside face of 1 crank arm to the outside face of the opposite crank arm for Q1(Fig.1A),which was 15.0 cm,and the original QF of the stationary cycle ergometer.QF was increased using 3 pairs of pedal extenders for the 3 extended QFs,which were 19.2 cm(Q2,with 1 pair of extenders),23.4 cm(Q3,with 2 pairs of extenders),and 27.6 cm(Q4,with 3 pairs of extenders).The QFs for each of these 3 extended QFs was measured from the location where the pedal inserted into the crank arm with the added pedal extenders to the location where the opposite pedal inserted into the opposite crank arm with the added pedal extenders(Sunlite;Brooklyn,NY,USA)(Fig.1B and 1C).Each single pedal extender increased the QF by 2.1 cm,and a pair(1 on each pedal)increased the QF by a total of 4.2 cm.
2.3.Experimental procedures
Participants performed a 2-min warm-up on the cycle ergometer.Each participant then completed a total of 12 testing conditions,pedaling at cadence of 80 rotations/min28for 2 min at workrates of 80 watts(W),120 W,and 160 W,in each of 4 QFs.All conditions were randomized first by QF,followed by workrate within each QF.Cadence was determined and monitored by the visual display on the cycle ergometer.Simultaneous recordings of kinematic(240 Hz)and kinetic(1200 Hz)data were collected for a minimum of 5 consecutive pedal cycles beginning in the last 30 s of each test condition.4Following the conclusion of each QF condition,a 2-min rest period was given to all participants,during which they provided their rating of perceived exertion(RPE)using the Borg scale,29as well as comfort and knee pain via numeric visual analog scales with a range of 1-10,with greater numbers indicating greater discomfort and knee pain.
The data were exported,and 3D joint kinematics and kinetics were analyzed in Visual3D biomechanical analysis suite(Version 6.0,C-Motion;Germantown,MD,USA).Angular computations were completed using a Cardan rotational sequence(X-Y-Z)based on the right-hand rule to define angular kinematic and kinetic variable conventions.Kinematic and pedal reaction-force data were filtered using a 0 lag and fourth-order Butterworth low-pass filter at 6 Hz.11Joint moments were computed as internal moments.30Peak kinematic and kinetic variables were determined during the power phase(0-180˚)of the crank cycle.The force and moment variables were not normalized to body weight or mass because in cycling the majority of the body weight is supported by the saddle and handlebars.4
A 3×4(workrate×QF)repeated measures analysis of variance(ANOVA)was used to detect differences between workrate and QF conditions(Version 25.0;SPSS,IBM,Armonk,NY,USA).When an interaction was present,a pairwise t test was performed in the post hoc analysis with Bonferroni adjustments to determine the location of the statistical differences between QF and workrate.An α level of 0.05 was set a priori and adjusted for post hoc comparisons such that workrate α <0.017,QF α <0.008,and interaction α <0.008.Effect size for all significant main effects and interactions was reported using partial eta squared(η2).
3.Results
Workrate influenced RPE(F(2,14)=40.285,p <0.001,η2=0.852)(Table 1),and post hoc comparisons showed an increase of RPE between 80 W and 120 W,80 W and 160 W,and 120 W and 160 W(p ≤0.001 for all comparisons).
There was an interaction effect between workrate and QF for peak KAbM(F(6,10)=4.370,p=0.020,η2=0.724)(Table 2).Post hoc comparisons showed increased KAbM between Q1 and Q3 and between Q1 and Q4,and Q2 and Q4 at 80 W(p ≤0.001 for all comparisons).At 120 W,increases were shown for all comparisons from Q1 to Q4(p ≤0.007 for all conditions).Finally,at 160 W,increases were shown between Q1 and Q2,Q1 and Q3,and Q1 and Q4,as well as between Q2 and Q4(p ≤0.003 for all comparisons).Ensemble curves of KAbM and knee extension moment are provided in Fig.2.There was a main effect of QF on frontal-plane knee angle(F(3,13)=6.532,p=0.006,η2=0.601).Post hoc comparison showed that an increase of knee-abduction angle existed only between Q1 and Q4 at all workrates(p ≤0.002).Finally,a main effect of QF was found for peak knee abduction range of motion(ROM)(F(3,12)=3.042,p=0.022,η2=0.540).Increased ROM existed between Q1 and Q4 and between Q2 and Q4(p ≤0.005 for all comparisons).There was a main effect of QF on knee extension ROM(F(3,13)=15.065,p <0.001,η2=0.777).Post hoc comparison showed that increased knee extension ROM existed between Q1 and Q2,Q1 and Q3,Q1 and Q4,as well as between Q2 and Q3 and Q2 and Q4 and between Q3 and Q4(p ≤0.002 for all comparisons).There was a main effect of workrate on peak knee extension moment(F(2,14)=42.459,p <0.001,η2=0.858).Workrate increased between 80 W and 120 W,80 W and 160 W,and 120 W and 160 W(p ≤0.003 for all comparisons).
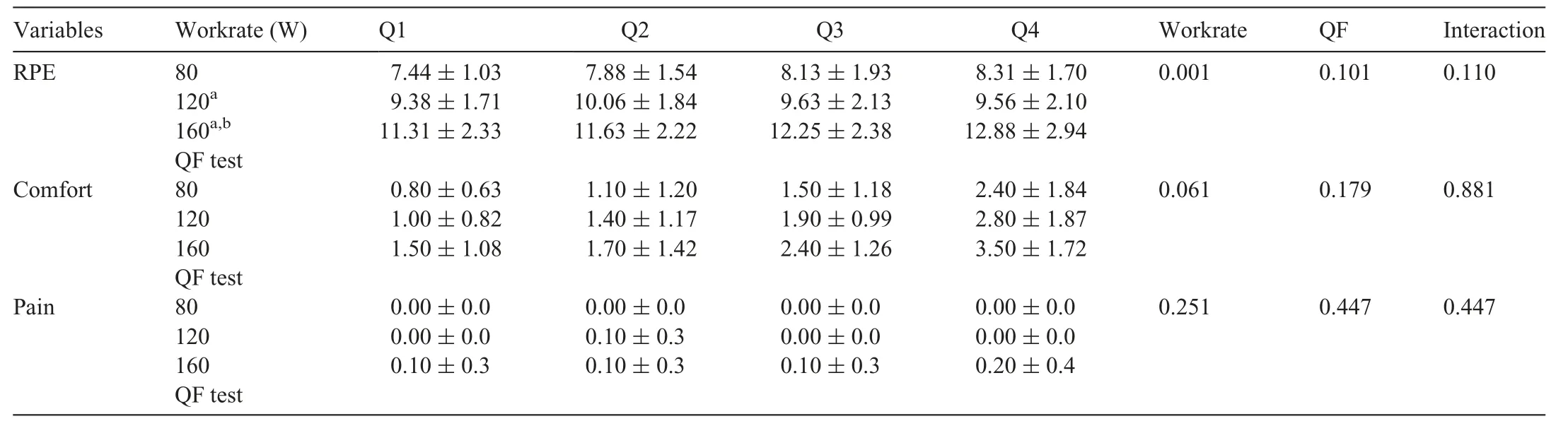
Table 1 Group mean rating of perceived exertion,comfort,and knee pain scores.
There was a main effect of workrate for peak vertical PRF(F(2,14)=267.183,p <0.001,η2=0.974)(Table 3),and post hoc comparisons showed increases between 80 W and 120 W,80 W and 160 W,as well as 120 W and 160 W(p ≤0.001 for all comparisons).There was an interaction effect between workrate and QF for peak medial PRF (F (6,10)=4.724, p=0.016, η2=0.739). Post hoc comparisons showed increases of medial PRF between Q1 and Q3,Q1 and Q4,and Q2 and Q4(p ≤0.001 for all comparisons)at 80 W.At 120 W,increases were shown between Q1 and Q2,Q1 and Q3, Q1 and Q4, and Q2 and Q4 (p ≤ 0.001 for allcomparisons). Finally, increases were shown at 160 W between Q1 and Q2,Q1 and Q3,Q1 and Q4,and Q2 and Q4(p ≤0.001 for all comparisons).
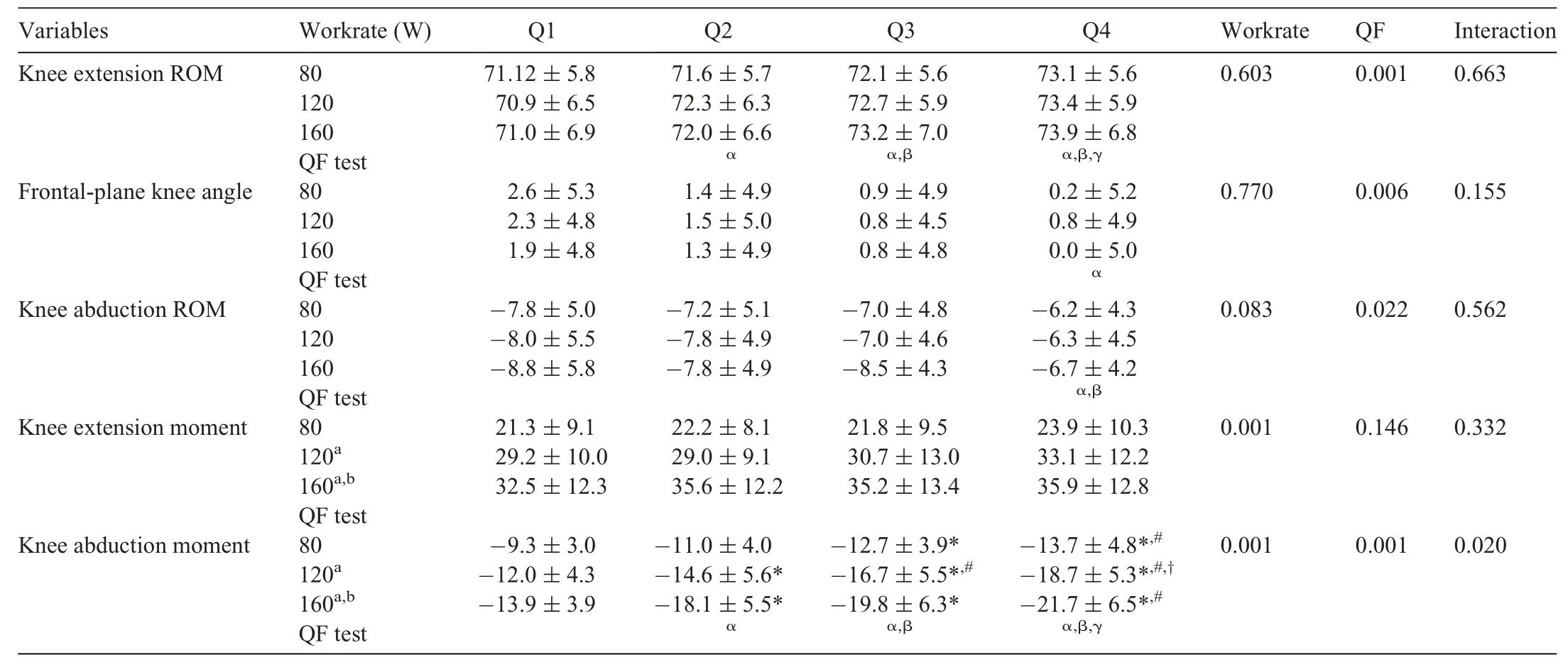
Table 2 Peak power phase knee joint angles(˚),ROM(˚),and moments(N⋅m).
4.Discussion
The purpose of this study was to examine the effects of standard and increased QFs at different workrates on knee biomechanics of healthy participants during stationary cycling.It was hypothesized that as QF increased,peak KAbM would decrease,and as QF increased further,the frontal-plane knee moment would become a knee adduction moment. The hypothesis was not supported because the changes in KAbM were in the opposite direction from those hypothesized,and KAbMs increased with increased workrate.
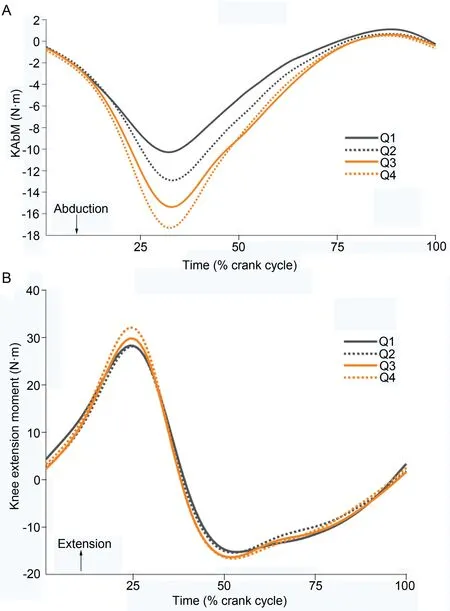
Fig.2.Ensemble curves of(A)knee abduction moment(KAbM)while cycling at 120 W at each Q-Factor(QF).(B)knee extension moment while cycling at 120 W at each increasing QF.
Peak KAbM increased 47%,56%,and 56%as QF increased from Q1 to Q4 at the 3 workrates,respectively(Table 2).These results showed the opposite trend compared to step-width modifications in gait.With increased step-width,KAbM decreases in level walking,15,17,31stair ascent,13,15and stair descent.14In other studies,mean wide step-widths have been reported as 0.32 m13and 0.30 m,15which are similar to Q2 in the current study.QF in cycling studies is measured from crank arm to crank arm,19,23whereas step-width in walking studies is commonly measured as the distance from left to right foot center of mass(COM).13,15,32The actual horizontal distance between the centers of the 2 pedals(a closer approximation of foot COM)was estimated to be about 0.32 m for Q2(19.2 cm+additional 13 cm,the combined distance from the center of the pedal to the crank arm),which is comparable to the wide step-width in gait. In other studies of walking, KAbM was reduced by 19.4%13and by 5.1%15at wider step-widths in healthy adults.In our cycling study,as QF increased from Q1(similar to the preferred step-width)to Q2(similar to the wider step-width),KAbM increased by 18%,22%,and 30%,respectively,at each workrate.KAbM continued to increase as QF widened to Q3 and Q4,with increases in peak KAbM of 13%and 10%,respectively.At Q4,peak KAbM was,on average,54%greater than at Q1 across all workrates.One explanation for the reduction of peak KAbM in walking is a reduction in frontal-plane moment arm of frontal-plane resultant ground reaction force(GRF)to knee joint.14,33Step-width modification research suggests that during weight acceptance,whole-body COM shifts laterally closer to the support leg to establish balance and shifts the GRF vector from the medial side of the knee closer to the knee joint,thus decreasing the frontal-plane GRF moment arm and KAbM.14,33Previous gait-modification research has observed a decrease in frontal-plane knee joint loading as mediolateral trunk lean has increased from neutral up to 12˚.34,35In cycling,whole-body COM does not shift significantly relative to the knee joint due to constraint from the seat and,thus,marginally influences the frontal-plane PRF moment arm.In this study,the average mediolateral trunk sway was between 2.7˚and 4.5˚ across all test conditions.Increased QF and a stationary COM increased the frontal-plane PRF moment arm,thus increasing KAbM.Furthermore,linear regression models indicated thatQFs were strongly correlated with KAbMs and predicted KAbMs well,with R2values of 0.99,0.99,and 0.95 at 80 W,120 W,and 160 W,respectively.

Table 3 Peak power phase pedal reaction forces.
Increased medial PRF may also contribute to increased KAbM because a QF main effect of medial PRF was present in all conditions.An interaction for peak medial PRF showed greater increases at higher workrates(Table 3).KAbM is observed when the knee joint is in the adducted position.14Increasing QF increases the frontal-plane moment arm of the PRF.Additionally,an increased frontal-plane PRF vector,a result of the increased medial PRF,also increased the moment arm.The combination of these 2 results,without the compensation of whole-body COM,may have contributed to the increased KAbMs.As QF increases,the lower limb is moved farther away from the saddle,thus pushing more laterally during the power phase and,thereby,increasing medial PRF.It is worth noting that the medial PRF increased significantly with increased QF and that changes in the medial PRF seem to parallel closely those of KAbM.
The hypothesis that as workrate increases,the increase in the frontal-plane knee moment will become greater was supported by our data.A QF×workrate interaction was observed for KAbM. In general, the magnitude change of KAbM increased with wider QFs and at higher workrates.At 80 W,KAbM increased by 4.4 N⋅m from Q1 to Q4,whereas at 160 W KAbM increased by 7.8 N⋅m.QF manipulation,in conjunction with workrate manipulation,may allow for the modulation frontal-plane knee joint loading,enhancing protocols used in exercise prescription and rehabilitation for knee OA or populations with total knee replacements.Recent studies of knee OA examining level walking,15stair ascent,13and stair descent14have reported normalized KAbM of-0.52,-0.36,and-0.77 N⋅m/kg,respectively,at preferred step-width.In those same studies, but at wide step-widths, normalized KAbM was reported to be between-0.29 and-0.73 N⋅m/kg.In the present study,normalized KAbM was-0.13 N⋅m/kg at Q1(similar to preferred step-width)and-0.20 N⋅m/kg at Q4(analogous to wide step-width)at 80 W.Although cycling may elicit decreased frontal-plane loading compared to different forms of walking,patients with medial knee compartment OA may want to avoid cycling at higher workrates on ergometers with larger QFs or gradually increase combinations of QF and workrate to promote joint strength,mobility,and cardiovascular fitness.
Our final hypothesis, stating that peak knee extension moment will not change significantly with increased QF,was supported by our data because peak knee extension moment was not significantly influenced by widened QFs.Similarly,peak vertical PRFs were not affected by increased QFs.Given the length of lower-extremity segments,the relatively small increase in medial PRF(5.1 N,8.3 N,and 9.8 N at each workrate,respectively)might have not been large enough to change the resultant PRFs(Table 3).Furthermore,as discussed previously,as QF increases,the lower limb is moved farther away from the saddle and pushes more laterally during the power phase,thus does not significantly change the vertical PRF.These results demonstrate that the overall knee joint loading is not changed with manipulation of QF.In conjunction with the lack of effect of QF on RPE,comfort,or knee pain,this may provide added benefits to those affected by overuse injury or knee OA.One such benefit is that QF manipulation may be a safe and effective tool in rehabilitation protocols and exercises,allowing for specific targeting of medial compartment joint loading.
One limitation of this study is that due to the construction of the instrumented force pedals,we were constrained in the mechanism to increase QF.In gait modification literature,step-width is often measured as a percent increase of leg length.13-15,18,32Disley and Li19,23used a “floating pedal”to move the foot freely about the mediolateral axis of a lengthened pedal spindle.Given the location of the instrumented force sensors within the pedal body,we were able to increase QF only with spacers at the crank arm site,which constrained the QF increase to the 4.2 cm in each increment(Fig.1B and 1C).Although Q1 and Q2 were similar in absolute width to the preferred and wide step-widths reported previously,determining custom QFs from anthropometric measurements may be necessary to provide more tailored rehabilitation programs. A second limitation of this study was the use of healthy young participants.Although our study is,to our knowledge,the first to examine the effects of increased QF on knee joint biomechanics during cycling, these findings may not be directly applied to clinical populations affected by frontalplane knee joint loading (e.g., knee OA or total knee replacement).Further research is necessary to examine the efficacy of QF manipulation in clinical populations.
5.Conclusion
The findings of this study indicate that as the QF of a stationary cycle is increased,peak KAbM will increase as well,suggesting increased medial compartment loading of the knee.Increasing the QF did not change the knee extension moment or sagittal plane loading patterns of the knee.Modulating frontal-plane knee joint loading by adjusting QF may be beneficial for exercise prescription,rehabilitation protocols,and bike fitting.Future studies should examine the effects of QF modulation on populations diagnosed with or predisposed to OA,as well as the biomechanical effects of QF self-selection for recreational cyclists and clinical populations.
Authors’contributions
TT was involved in the conception and design of the study,data collection,data processing,statistical analysis,data interpretation,and drafting of the manuscript;SZ was involved in the conception and design of the study,data collection,data processing,statistical analysis,data interpretation,and drafting of the manuscript;KS and JTW participated in the design of the study and drafting of the original manuscript.All authors have read and approved the final version of the manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interest.
杂志排行

Journal of Sport and Health Science的其它文章
- Impacts of exercise intervention on various diseases in rats
- Reply to“Is physical performance(in mice)increased by Veillonella atypica or decreased by Lactobacillus bulgaricus?”
- Muscle strength cut-offs for the detection of metabolic syndrome in a nonrepresentative sample of collegiate students from Colombia
- Land-walking vs.water-walking interventions in older adults:Effects on aerobic fitness
- Longitudinal associations of physical activity and pubertal development with academic achievement in adolescents
- Transition to forefoot strike reduces load rates more effectively than altered cadence