Sleep quality of patients with postoperative glioma at home
2020-04-08YangHuangZiJuanJiangJuanDengYuJuanQi
Yang Huang, Zi-Juan Jiang, Juan Deng, Yu-Juan Qi
Yang Huang, Zi-Juan Jiang, Juan Deng, Yu-Juan Qi, Department of Neurosurgery, The Affiliated Brain Hospital of Nanjing Medical University, Nanjing 210029, Jiangsu Province, China
Abstract BACKGROUND The sleep quality of patients with postoperative glioma at home has not been reported worldwide. In this study, the sleep quality of postoperative glioma patients at home was explored through telephone interviews.AIM To investigate the sleep quality of patients with postoperative glioma.METHODS Glioma patients who were treated and operated on at Nanjing Brain Hospital from May 2012 to August 2019 were selected as participants via convenience sampling. A total of 549 patients were recruited by telephone, and 358 of those patients responded to the Pittsburgh Sleep Quality Index (PSQI).RESULTS The total PSQI score was 5.19 ± 3.39 in all patients with postoperative glioma,which was higher than that of the normal group. There were 135 patients with poor sleep quality (PSQI > 7), which accounted for 37.7% of all respondents. The scores of the seven dimensions of the PSQI were sleep latency (1.22 ± 1.05), sleep disturbance (1.12 ± 0.98), subjective sleep quality (1.03 ± 0.92), habitual sleep efficiency (1.02 ± 0.91), daytime dysfunction (0.95 ± 0.43), sleep persistence (0.83 ±0.76), and use of sleeping medication (0.25 ± 0.24). The results showed that the subjective sleep quality of the patients who underwent an operation 1-2 years ago was worse than that of the patients who underwent an operation more than 2 years ago (P < 0.05). Older patients had worse sleep latency and sleep duration scores than younger patients (P < 0.05). Sleep disturbance and daytime dysfunction were worse in patients who received postoperative radiotherapy/chemotherapy (P < 0.05).CONCLUSION The sleep quality of patients with postoperative glioma at home is worse than that of normal adults. Moreover, difficulty falling asleep and sleep disorders are common complications among these patients, and age, postoperative duration,and postoperative chemoradiotherapy could affect sleep quality.
Key Words: Sleep quality; Postoperative; Glioma patients; Radiotherapy; Chemotherapy;Outcome
INTRODUCTION
Glioma is a very common primary intracranial malignant tumor, with an incidence ranging from 5 to 8 out of 100000 individuals. The 5-year mortality of glioma is the third highest among all systemic tumors (behind pancreatic cancer and lung cancer)and thus, it poses a substantial threat to human health[1]. Some factors, such as discharge from the hospital, prolonged postoperative time, environment, and physical pain, may affect patients’ sleep quality. However, the sleep quality of patients with postoperative glioma at home has not been reported worldwide. In this study, the sleep quality of postoperative glioma patients at home was explored through telephone interviews to provide some evidence regarding interventions for patients'sleep quality.
MATERIALS AND METHODS
Study design and patients
Convenient sampling was used to recruit patients with postoperative glioma who were admitted to The Affiliated Brain Hospital of Nanjing Medical University from May 2012 to August 2019. This hospital is a tertiary hospital with a specialized neurosurgical unit. The inclusion criteria were as follows: (1) Patients were at least 18 years old and possessed certain language communication skills; (2) Glioma surgery occurred more than 3 mo before the survey; and (3) Patients volunteered to participate in this study. The exclusion criteria were as follows: (1) Patients with mental disorders;and (2) Patients who could not communicate properly. In this study, 358 valid questionnaires were answered through telephone interviews. The age of patients ranged from 19-71 (44.64 ± 11.07) years old. A total of 47.9% of the patients had a junior high school education or above, 24.2% were still working, and 190 (95%)patients were married. The minimum postoperative time was 3 mo, the longest was 7 years, and the mean postoperative time was 4.41 ± 2.57 years.
Measurement tool
The Pittsburgh Sleep Quality Index (PSQI) was developed by Buysseet al[2]at the University of Pittsburgh in 1989 to evaluate the sleep quality of respondents in the past month. The scale has good internal consistency (Cronbach's α = 0.83) and test-retest reliability (r= 0.85), suggesting that it is suitable for clinical and sleep quality evaluations in China. By assessing both the quality and quantity of sleep, we could not only evaluate the sleep behavior and habits of the general population but also comprehensively evaluate the sleep quality of clinical patients. This index includes 19 self-assessment items and five other review items. The self-assessment items include 18 items that are scored, including items assessing subjective sleep quality, sleep latency, sleep continuity, habitual sleep efficiency, sleep disorder (disorder), the use of sleep medication, and daytime dysfunction. Scores for each factor range from 0-3 points. The sum of the scores of the above seven factors is the total score of the PSQI.Higher scores indicate worse sleep quality[2]. The total PSQI score could be used to diagnose sleep quality, and 5 points is often used as the diagnostic threshold in foreign countries[2]. Using the PSQI, Liuet al[3]measured sleep quality in a Chinese population and found that the scale had a high sensitivity (98.3%) and specificity (90.2%) when the threshold was set at 7. Thus, in this study, 7 points were used as the threshold. PSQI scores > 7 indicated poor sleep quality, and scores ≤ 7 indicated good sleep quality.
Investigation methods
This study was reviewed and approved by the hospital ethics committee, and the data were collected by nurses from the clinical research group. The nurses performed telephone interviews, administered the questionnaire in the standardized language,and investigated the patients. For undereducated patients who could not complete the questionnaire independently, the phased information was used to collect data by the inquiry method. The interviewers asked questions and recorded the responses to each item in a uniform way; when the interviewees could not understand the question, the nurses rephrased the question in common and easy-to-understand language.
Statistical analysis
Epidata 5.0 (Solvusoft Inc., Chicago, IL, United States) was used to input data, and SPSS 18.0 software (SPSS Inc., Chicago, IL, United States) was used to analyze the data.Categorical data are described as frequencies and percentages. The quantitative data that were normally distributed are described as the mean ± SD and were compared using independent-samplest-tests. For nonnormally distributed data, the nonparametric tests were used for between-group comparisons.P< 0.05 was considered statistically significant.
RESULTS
Total sleep quality score and scores for each factor
The total PSQI score and the scores of each of the seven factors are shown in Table 1.The scores for each of the seven factors of the PSQI ranged from high to low in the following order: Sleep latency, sleep disturbance (disorder), subjective sleep quality,habitual sleep efficiency, daytime dysfunction, sleep persistence, and use of sleeping medication. There were 132 (37%) patients with PSQI scores > 5 and 135 (37.7%) with PSQI scores > 7. The mean total PSQI score of the patients studied herein was compared with that of 112 normal adults measured by Liuet al[3](3.88 ± 2.52); the results showed that the mean PSQI score of the patients studied herein was significantly higher than that of the normal group (Z = -8.387,P= 0.011), as shown in Table 1.
Specific sleep conditions
In this survey, 75 (21%) patients felt that their sleep quality was poor or quite poor in the past month. A total of 100 (29.2%) patients took more than 30 min to fall asleep each night, and 36 (10.0%) took more than 60 min to fall asleep. On average, 94 (26.3%)patients were unable to fall asleep within 30 min at least 2-3 nights per week. The average bedtime of the patients was 8.84 ± 2.56 h, but the actual sleep time was only 7.09 ± 1.35 h, and the sleep efficiency (actual sleep time/bedtime) of the 107 (30.0%)patients was less than 85% because they could not fall asleep quickly after bed. A total of 39 (11%) patients had used medication to help them fall asleep within the last month. The sleep disorders of glioma patients are shown in Table 2.
Comparison of sleep quality in glioma patients by different pathophysiological factors and clinical treatment factors
Because sleep is directly affected by some pathophysiological factors, the patients were divided into groups according to postoperative duration, age, radiotherapy, and chemotherapy. The differences in the total PSQI score and the differences in the scorefor each factor between the different groups were tested byt-test or analysis of variance, and the results are shown in Table 3. The results showed that there was a significant difference in subjective sleep quality between patients with a postoperative period of 1-2 years and those with a postoperative period of more than 2 years (t= -5.361,P= 0.028, 95%CI: 0.10565-0.85785). There were statistically significant differences in sleep latency (t =-3.661,P= 0.029, 95%CI: 0.41759-1.02441) and sleep duration [t =-3.306,P= 0.001, 95%CI: -1.14466-(-0.20334)] between the different age groups, with older respondents having higher scores. Patients receiving postoperative chemoradiotherapy had a higher level of sleep disturbance (t =1.677,P= 0.037, 95%CI:-0.3658-0.3134) and daytime dysfunction (t =4.976,P= 0.017, 95%CI: 0.24866-0.61834)than those who did not.
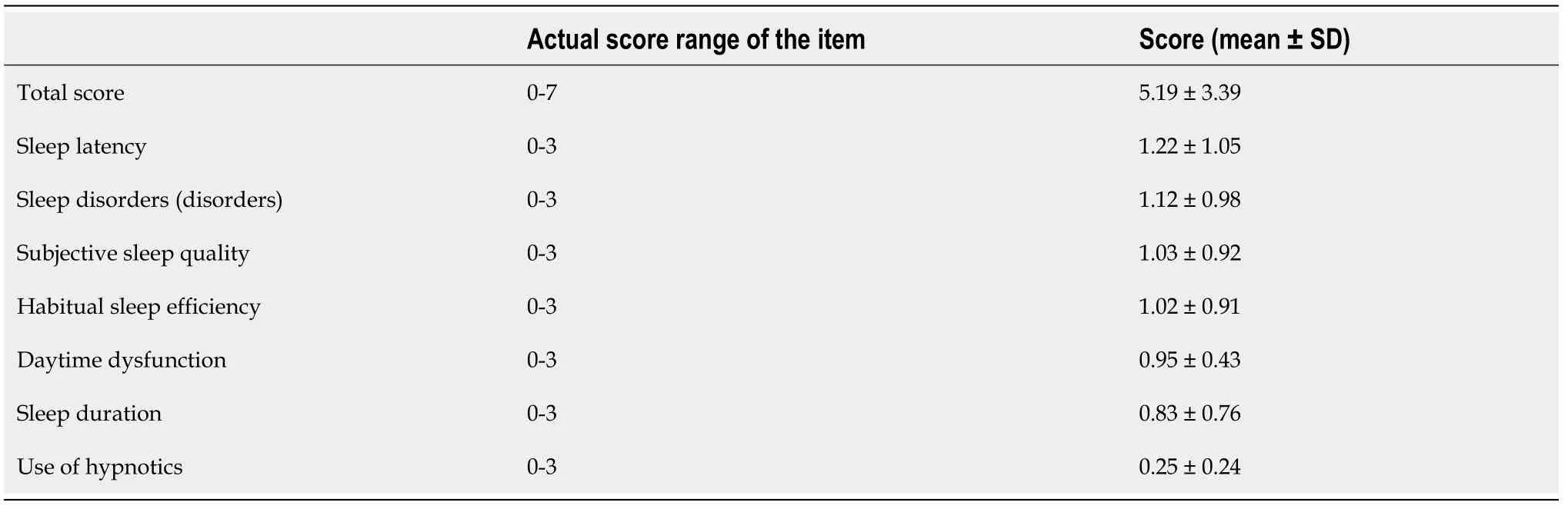
Table 1 Total Pittsburgh Sleep Quality Index score and scores for each factor in glioma patients
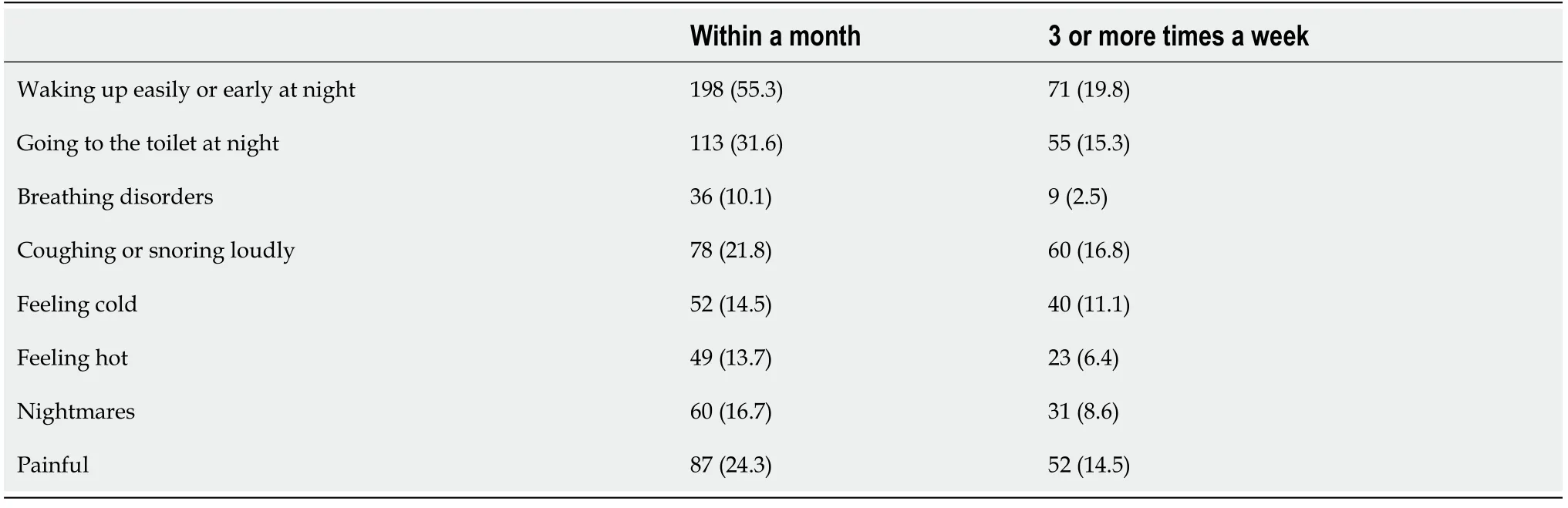
Table 2 Postoperative sleep disorders in patients with glioma, n (%)
DISCUSSION
In this study, our data indicated that patients with glioma after surgery had relatively good sleep quality within 1-2 years after being discharged from the hospital. After 2 years, patients began to worry about recurrence, and those worries were accompanied by anxiety and pain, which often led to sleep disorders. The sleep quality of such patients was lower than that of normal adults, which is similar to the results of foreign academic research. Jeonet al[4]searched the literature from 1990 to 2015, focusing on studies of adults with primary or nonprimary sleep disorders and patients with secondary sleep disorders after intracranial tumor surgery. Sleep disorders and sleepiness are often reported as the most severe symptoms in the overall health-related and quality of life of the disease. Mental and psychological factors are also important factors that affect sleep quality, and the occurrence of somatic diseases will further aggravate the occurrence of adverse emotions[5]. The common clinical symptoms of glioma patients are headache, vomiting, visual impairment, dizziness, and epilepsy;glioma is also often accompanied by helplessness, expectation, anxiety, fear, and other emotions, which seriously affect the function of the nervous, endocrine, andcirculatory systems. Domestic and foreign researchers have found that patients with severe anxiety often experience sleep disorders[6]. Postoperative glioma patients generally have low sleep quality. It is suggested that medical staff and family members of patients should quickly and accurately evaluate the postoperative sleep status of patients, regardless of whether they are in the hospital or discharged. When a patient frequently shows a decline in daily activity, fatigue, and other performance issues, the patients’ sleep quality should be assessed as early as possible. Advice and help should be given to the patient according to his/her sleep problems, and the patient should be encouraged to seek help from the doctor if necessary.
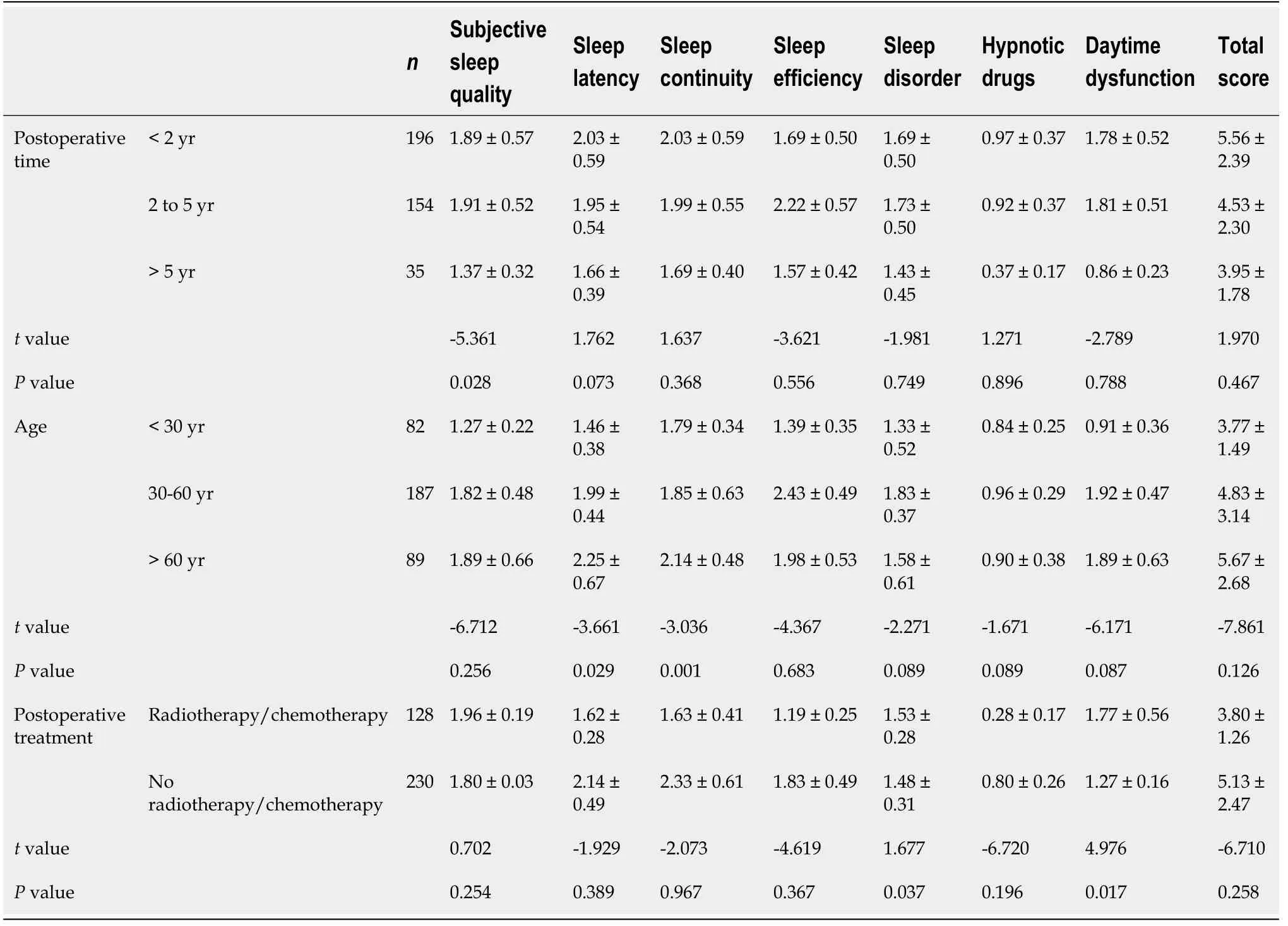
Table 3 Comparison of Pittsburgh Sleep Quality Index scores among different groups based on psychosocial factors and clinical factors in glioma patients (score, mean ± SD)
Sleep disorder is a common body dysfunction that manifests as various functional disorders during the sleep-wake process[7]. The occurrence of postoperative sleep disturbance in glioma patients is related to neurological function and sensory disturbance, resulting in adverse effects on patients' daily activities. The present study demonstrated that 73% of patients had sleep disorders after undergoing a glioma operation. The risk factors for sleep disorders in glioma patients[8]include the tumor itself (such as a tumor resulting in abnormal hormone secretion or tumor infiltration that causes pain, dyspnea, nausea, itching,etc.), treatment, medication (such as radiation therapy, chemotherapy drugs, hormone drugs, sympathetic nerve medicine,and sedative hypnotics), environmental factors inside the bedroom (such as extreme temperature and strong light or noise), and psychological barriers (such as having depression, anxiety, or tension). There are many causes for sleep disorders, the most common of which is pain. Therefore, it is particularly important to explain to the patients and their families the necessity of treatment and the possible side effects in the treatment process. It is also important to tell patients that a decline in sleep quality will make them feel that the disease is serious and aggravate their anxiety symptoms, thus affecting their postoperative recovery[9,10].
In addition, nightmares, coughing, and snoring are also common causes of sleep disorders. Therefore, patients should avoid drinking more water before bed to reduce nocturnal urination, and other family members should help to maintain a quiet sleeping environment. If the patient has some sleep disorders, such as increased nocturnal urination and excessive frequency of coughing and snoring, it is necessary to pay attention to whether the patient has urinary tract infection or respiratory diseases.If these problems exist, they should be treated actively to avoid sleep disorders caused by urinary and respiratory diseases[11].
Moreover, our study showed that older patients are less likely than younger patients to sleep longer and to sleep more efficiently. This suggests that there are some differences in sleep quality among patients of different ages. In China, 45.5% of the population have sleep problems[12]. This may be related to some physiological changes in human sleep patterns with age. It has been reported[13]that as many as 80% of elderly people have varying degrees of sleep problems, and the incidence of sleep disorders among this population ranges from 25% to 60%. The quality of sleep is affected by human diseases and mental conditions, and the quality of sleep in elderly patients with glioma is worse than that in normal elderly patients.
Finally, radiotherapy and chemotherapy were confirmed to affect the postoperative sleep quality of glioma patients. Our results showed that patients who received postoperative chemoradiotherapy had worse sleep disturbance (disorder) and daytime dysfunction than patients who did not. The 3- to 5-year disease-free survival rate(event_free sun, ival, ESF) was < 20% for glioma patients before the combined treatment of surgery and radiotherapy/chemotherapy[14]. At present, the conventional treatment for glioma is still comprehensive treatment combining radiotherapy,chemotherapy, and chemoradiotherapy on the basis of maximizing surgical resection of tumor lesions[15]. During radiotherapy and chemotherapy, gastrointestinal discomfort, bone marrow suppression, epilepsy, and other adverse events (hair loss,muscle numbness and pain, constipation, and limb movement disorder) occur more frequently, which seriously affects the patients’ diet, daily life, and sleep quality. Most of the patients showed low energy during the day, felt sleepy in the day, had difficulty falling asleep at night, had anxiety, and experienced pain.
The limitation of this study is that it did not investigate whether the patient had previous related diseases, such as sleep disorders, and whether there was a history of related drugs that affect sleep. In addition, this study only discussed the relationship between age, gradual time, and gradual radiotherapy and chemotherapy and the quality of sleep of patients. Subsequent research work can further explore the relationship between patients' sleep quality and the impact of family and social support and constantly explore feasible nursing intervention methods to ensure that patients receive comprehensive and effective alternative nursing services. A more systematic examination of sleep disturbance is warranted to guide the development of better symptom management programs in this population.
CONCLUSION
In conclusion, the results of this study showed that sleep disturbance is an important factor affecting the outcome and quality of life of patients. Sufficient attention should be paid to such patients. However, we did not find any literature reports that continuously tracked and evaluated sleep status of glioma patients after discharge,and many of the extant studies focus on the postoperative recurrence and survival time of glioma patients[16,17]. Owing to the complexity of the disease, its high mortality rate, complicated medication regimen, and other factors, there are still many challenges in the study of glioma patients, especially regarding the follow-up process,the complexity of influencing factors, and so on. It is recommended that future research on sleep disorders among postoperative glioma patients should choose specific assessment tools and coping strategies to improve patients' sleep according to their specific situation.
ARTICLE HIGHLIGHTS
Research background
Glioma is a very common primary intracranial malignant tumor with an incidence rate ranging from 5/100000 to 8/100000. The 5-year mortality rate is the third highest among systemic tumors after pancreatic cancer and lung cancer. Thus, glioma poses a substantial threat to human health. However, as the patient returns home and the postoperative time increases, environmental factors and physical pain will change, and the patient's sleep quality may also change accordingly.
Research motivation
Since there has not been any relevant research on the sleep quality of postoperative glioma patients, the results of this study can provide guidance for interventions to improve the sleep quality of postoperative glioma patients.
Research objectives
The purpose of this study was to understand the sleep quality of postoperative glioma patients at home.
Research methods
In this study, postoperative glioma patients were investigated, and follow-up calls were conducted by telephone to conduct a questionnaire survey. The questionnaire used was the Pittsburgh Sleep Quality Index (PSQI), and nurses used standardized guidance language while conducting the survey. For those with a low education level and other factors that led them to be unable to complete the survey independently, the inquiry survey method was used to collect the data, and the nurse recorded each item in a unified manner. Questions that the interviewee did not understand were answered without suggestion.
Research results
The mean total PSQI score of postoperative glioma patients was 5.19 ± 3.39, which was higher than that of the normal group. The results also showed that the subjective sleep quality of patients with a postoperative time of 1-2 years was worse than that of the group with a postoperative time of more than 2 years (P <0.05). Older patients had worse sleep latency and sleep duration than younger patients (P <0.05). Patients who received postoperative radiotherapy/chemotherapy had worse sleep disturbance and daytime dysfunction than patients without postoperative radiotherapy/chemotherapy(P <0.05).
Research conclusions
The sleep quality of postoperative glioma patients at home is worse than that of normal adults. These patients find it difficult to fall asleep and have sleep disturbances. The sleep quality of patients differs depending on age, the length of postoperative time, and the use of postoperative radiotherapy/chemotherapy.
Research perspectives
This study is a telephone follow-up survey and a statistical analysis of the sleep quality of postoperative glioma patients. Future studies should examine sleep disorders in glioma patients from multiple angles, reduce the impact of radiotherapy and chemotherapy on patients' sleep, and assist patients in taking measures that are beneficial to sleep. Future research should also explore the relationship between the patient's sleep quality and family and social support and continue to explore feasible nursing-based intervention methods to ensure that patients receive comprehensive,effective, and high-quality nursing services. With joint efforts, the sleep quality of postoperative glioma patients can be improved.
杂志排行
World Journal of Clinical Cases的其它文章
- Relationship between non-alcoholic fatty liver disease and coronary heart disease
- Remission of hepatotoxicity in chronic pulmonary aspergillosis patients after lowering trough concentration of voriconazole
- Endoscopic submucosal dissection as alternative to surgery for complicated gastric heterotopic pancreas
- Observation of the effects of three methods for reducing perineal swelling in children with developmental hip dislocation
- Predictive value of serum cystatin C for risk of mortality in severe and critically ill patients with COVID-19
- Early complications of preoperative external traction fixation in the staged treatment of tibial fractures: A series of 402 cases