Effect of routine iron supplementation on copper level and oxidative stress status in pregnant women
2020-04-08DerouicheSamirDoudiDalalAtiaNoura
Derouiche Samir, Doudi Dalal, Atia Noura
1Department of Cellular and Molecular Biology, Faculty of the Sciences of Nature and Life, El Oued University, El Oued 39000, El Oued, Algeria
2Laboratory of Biodiversity and Application of Biotechnology in the Agricultural Field, Faculty of the Sciences of Nature and Life, University of El Oued, El-Oued 39000, Algeria
ABSTRACT Objective: To determine the effects of routine iron supplementation on oxidative stress markers in pregnant women.Methods: This study enrolled 122 pregnant women aged between 20-38 years throughout three stages of pregnancy: beginning with pregnancy, until the twentieth week and up to the thirtieth week. They were divided into two groups: 61 pregnant women not supplemented with iron (the control group), and 61 pregnant women supplemented with iron (the iron group). Blood samples were collected and protein, iron, uric acid, total bilirubin level and oxidative stress status were estimated using molecular spectrophotometric method. Copper levels were estimated by using atomic absorption spectroscopy method.Results: Iron, protein and copper concentrations were significantly increased (P<0.05) at 20 and 30 weeks of pregnancy and hemoglobin level was significantly increased (P<0.05) at the beginning of pregnancy and until 20 weeks in the iron group compared to the control group. In addition, levels of serum uric acid, serum total bilirubin and malondialdehyde in serum and erythrocytes were significantly increased at 20 and 30 weeks of pregnancy whereas the reduced glutathione level was significantly decreased in serum (30 weeks of pregnancy) and erythrocytes (20 and 30 weeks of pregnancy) in the iron group as compared to the control group. Serum oxygen radical absorbance capacity was not significantly changed. There was a significant positive correlation between serum iron level and serum copper, malondialdehyde level in serum and erythrocytes in pregnant women supplemented with iron.Conclusions: Iron supplement at 20 and 30 weeks of pregnancy plays a role in the development of oxidative stress which is the origin of several maternal-fetal complications.
KEYWORDS: Pregnancy; Iron; Copper; Oxidative stress; Women
1. Introduction
Pregnancy is characterized by physiological changes related to fetal development and growth[1]. This event is associated with serious health risks for women[2]. In the light of growth and human development, iron and copper are indispensable elements for the life of a pregnant woman. Iron is a micronutrient essential to any form of life because it is involved in many biological activities[3].Hemoglobin integration in red blood cells allows the transport of oxygen to tissues and cells[4] and the heme of cytochromes involves in the respiratory chains[5]. During pregnancy, the iron requirements are even higher as it is necessary for fetal growth, for the elevation of the erythrocyte mass, and for the placental functioning[6]. On the other hand, copper is an essential trace element and is a cofactor of several intermediate metabolism enzymes, mainly oxidases and it is essential for the synthesis of hemoglobin (by mobilization of ferrous iron)[7]. In addition, the iron is oxidized by enzymatic intervention in the interstitial and cellular space but the copper as soon as they are absorbed undergoes a spontaneous oxidation[8].Iron and copper in free form are the particular promoters of radical damage[9] because they act mainly by the formation of highly reactive hydroxyl radicals, which leads to lesions of cell membranes, proteins, mitochondria and DNA[10]. These free radicals can generate oxidative stress[11]. Indeed, pregnancy exposes many complications that may be related to an alteration of oxidative stress that is also associated with the appearance of several pathologies during pregnancy which is considered a very important risk factor[12]. The aim of the present study was to evaluate the effect of systematic supplementation of iron in different periods of pregnancy on copper levels, hemoglobin and oxidative stress status in El Oued (Algerian) women.
2. Materials and methods
2.1. Study design
We randomly enrolled 122 volunteer pregnant women aged between 20-38 years who visited the gynecology service of Hospital Bachir Bennaceur El Oued from April 10, 2018 until February 18, 2019.These women reported to the clinical study service (NCT00000109)at 3 time points (mean±SD) for measurements (According to the official dates approved by the gynecology service): beginning/first trimester [(12±2) week, visit 1], second trimester [(20±2) week,visit 2], third trimester [(30±2) week, visit 3)]. At the initial stage, a total of 122 pregnant women consented and were randomly assigned who had been receiving iron supplementation since the first trimester of pregnancy (n=61) or who had not receiving iron supplemented(n=61). Contact information was received for 349 women initially interested in participating in the study (Figure 1). After we lost contact with each other (52 cases) and others not interested to participate (36 women) or did not complete medical visits for some of them (139 women), the number reached 122 women who were enrolled in the study, 41% completed the intervention through visit 2 (50 women), and 26.2% were retained until the final visit (32 women), equally divided between the iron and control groups (n=16/group) (Figure 1). All the volunteers (the control and iron groups)in this study lived and resided in the El Oued region located in the southeast of Algeria.
2.2. Study population
We assessed the eligibility of all pregnant women admitted to gynecology service of Bachir Bennaceur Hospital. We included women who had clinical diagnosis and laboratory findings of pregnancy, lived in the El Oued (Algeria) region in this study. Some of the women included to this study did not take iron supplement,while among the women who had been taking iron supplementation at a dose between 25-30 mg/d since the first trimester of pregnancy,we selected a sample of them who accepted to participate in the study. We excluded the participants with diabetics, anemia and other chronic diseases from the iron and control groups. A representative in the gynecology service approached families to ask if they would be willing to have a research coordinator speak to them about the study. If yes, the coordinator spoke with the family, described the study (risks/benefits, voluntary participation, procedures). Families were given adequate time to reflect on the information, had any questions answered and gave free and voluntary consent.
2.3. Study interventions
Fasting blood samples were collected and placed into containing tubes. Blood was transferred into ethylene diamine tetra acetate(EDTA) tubes for oxidative stress markers and the serums were obtained. After centrifugation at 1 008×gfor 5 min, serum was removed and retained for assay of protein, iron, copper and oxidative stress parameters. Serum samples were stored at -20 ℃ until analysis. Blood EDTA tubes contents were centrifuged at 448×gfor 10 min and the plasma was removed. The cap of EDTA tube was lysis with 50 mL of Tris buffer solution (TBS) (EDTA 2.92M; Tris 1.21M; pH=7) and incubated 30 min in freezer. After incubation centrifuged at 700×gfor 10 min, and the obtained supernatant(erythrocytes) was used for the determination of oxidative stress markers. After separation of erythrocyte, the rest of EDTA tube contents were centrifuged at 448×gfor 10 min and the plasma was removed. The pellet was washed with lysis buffer and then kept in freezer for 30 min. After that, it was centrifuged at 700×gfor 10 min until the red blood cells pairing and then was collected into other tubes to make the dosage of oxidative stress tests[13].
2.4. Measurement of serum biochemical markers
Serum protein, acid uric, bilirubin and iron concentration were measured by using commercial kits (Spinreact) (ref: protein-001291, iron - MD1001247, uric acid - MD41001 and bilirubin-1001046). Serum copper was determined after 10-fold dilution using Atomic absorption spectrophotometry (Schimatzu, AA 6200).Copper calibration range solutions were prepared from a stock solution of copper nitrate at 1 mg/mL. All solutions were soaked in HNO3(10% v/v)[14]. Malondialdehyde (MDA) and reduced glutathione (GSH) were determined in red blood cells (erythrocytes)by Ohkawa method[15] and Ellman’s reagent[16], respectively. The total antioxidant power of the serum, that was to say its capacity to absorb oxygen free radicals [oxygen radical absorbance capacity(ORAC)] was estimated by the method of Blache and Prost[17].
2.5. Sample size
The sample size in the present study was calculated by the following formula equation[18] and the sample size was chosen to obtain the estimated prevalence of iron supplementation with a 95%confidence interval. The expected prevalence of systematic iron supplement to be used was about 35%. The calculated sample size(n) satisfied the relation given above.

The reliability coefficient (Zα/2) = 1.96
Estimated prevalence of systematic iron supplementation during pregnancy (P) = 0.65
Estimated prevalence of non-systematic iron supplement during pregnancy (1-P) = 0.35
The margin of error (e) = 0.05
n=(1.96)2×(0.35)×(0.65)/(0.05)2=349 pregnant women
After filtration of women abounded in this study, we estimated that a total of 122 pregnant women would be needed to detect a difference between groups.

Figure 1. Flowchart of subject recruitment, enrollment, and retention from early pregnancy to 30 weeks of pregnancy.
2.6. Statistical analysis
All data were presented as mean±standard deviation (mean±SD).The software SPSS V20.0 was used for all the statistical analyses.Data was first tested for normality using Kolmogorov-Smirnov test.Student’st-test was used to compare between means of different groups. Pearson’s correlation analysis were performed to assess the connection of different indexes.α= 0.05 was considered as statistically significant level.
2.7. Ethical statement
The ethical approach was requested and validated by the Ethics Committee referenced (79 EC/CMB/FNSL/EU2017) of the Department of Cellular and Molecular Biology, Faculty of Natural Sciences and Life, University of El Oued, Algeria.
3. Results
3.1. Description of study population
Characteristics of the study population were shown in Table 1.After obtained consent from all the participants in this study,there were 61 controls and 61 pregnant women supplemented by iron. There was no significant difference concerning mean age, body weight, height, body mass index and number of children in the iron group as compared with the control group (Table 1).
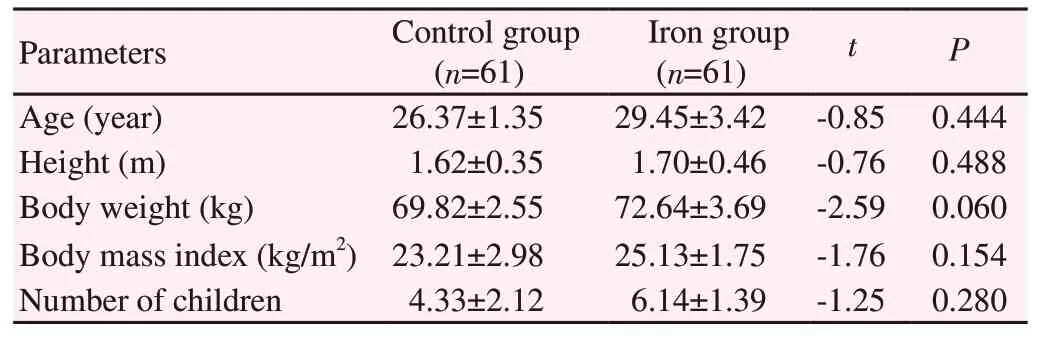
Table 1. Socio-demographic description of the control and iron groups.
3.2. Biochemical markers
The results obtained presented in Table 2 showed that the serum protein and iron concentrations were significantly increased(P<0.05) in the iron group at the 20th and 30th week of gestation.Serum copper was also significantly increased (P<0.05) in women supplemented with iron at the 20th and 30th week of gestation compared with the control group in the same period of pregnancy.But none of these parameters showed significant differences between two groups at beginning of study.
3.3. Serum oxidative stress markers
As shown in Table 3, there was a highly significant (P<0.01)decrease in serum GSH level in women of iron group at the 30th week of gestation and a significant (P<0.05) increase in serum MDA,uric acid and total bilirubin. But there was no significant change in total antioxidant activity at the 20th and 30th week of gestation between the two groups. All parameters did not differ significantly between the two groups in the beginning period of pregnancy except that for the bilirubin concentration where a significant elevation(P<0.05) was found in the iron group compared to the control group.
3.4. Hemoglobin and red blood cells oxidative stress markers
Table 4 showed that the hemoglobin concentrations were significantly increased (P<0.05) in women of iron group at the beginning of study and at the 20th week of gestation but the difference was not significant at the 30th week of gestation. On the other hand, the results showed that there was a significant increase(P<0.05) in erythrocytic MDA level and a significant decrease(P<0.05) in erythrocytic GSH of women supplemented with iron during the 20th and 30th week of pregnancy compared to women in the control group but the difference was not significant at the beginning of study.
3.5. Correlations between analyzed parameters
Figure 2 showed the results of correlation between serum iron level and oxidative stress markers in pregnant women supplemented with iron. Pearson’s correlation analysis showed that there was a significant positive correlation (P<0.05) between serum iron concentration and serum copper (r=0.73;P<0.05), serum MDA(r=0.72;P<0.05), and erythrocytic MDA (r=0.92;P<0.01)level. Also, a non-significant correlation (P>0.05) was observed between serum iron and serum ORAC and GSH level in serum and erythrocytes.

Table 3. Reduced glutathione, malondialdehyde, total antioxidant activity, uric acid and total bilirubin concentration in the control and iron groups.

Table 4. Hemoglobin and erythrocytic MDA and GSH level in the control and iron groups.

Figure 2. Scatter plots of serum iron and oxidative stress parameters in pregnancy women with iron supplement. MDA: malondialdehyde.
4. Discussion
Pregnancy is a physiological condition in women that is accompanied by physiological and organic changes from fertilization to delivery. The result of blood metal analysis showed that the serum iron concentration is significantly decreased in the third trimester of pregnancy but this level is significantly increased after iron supplementation in 20th and 30th week of gestation as compared to the control. These results are in agreement with the study of Razaet alwhich showed a significant decrease in serum iron from the 1st to the 3rd trimester of pregnancy[19].The observed decrease in serum iron concentration was due to increased need during pregnancy. About 1 000 mg of iron is needed to cover the needs of the pregnant woman[20] because of elevated erythrocyte mass, fetal growth, placental function and metabolic and physiological losses[21]. An iron supplement causes an increase in serum iron during the 20th and 30th week of gestation, which explains the need of iron supplementation to replace deficiency during pregnancy. Serum copper results showed an increase during last two trimesters of pregnancy and following iron supplementation with a significant correlation between copper and iron. Several studies are in agreement with our study, among which Fatemeh and Firouz who observed a high level of serum copper concentration in the second and third trimesters of pregnancy[22]. This can be attributed to increased levels of estrogen, which contributes to the synthesis and release of ceruloplasmin[23].
In addition, other studies have shown that excess iron has an antagonistic action for copper in the body by an unknown mechanism, or maybe excess iron inhibits the absorption of copper at the level of the intestinal lumen[24]. The obtained results also show that the hemoglobin level is gradually decreased during the three trimesters of pregnancy. Our results are in agreement with the research of Rayiset al[25]. This result may be associated with progressive hemodilution, which is a physiological change in all pregnant women to compensate for the needs of the fetus and its environment[26]. On the other hand, it has been reported in our results that iron supplementation increases hemoglobin levels. An iron supplement accelerates the synthesis of hemoglobin and the production of red blood cells by erythropoiesis which meets the iron requirements during pregnancy. The physiological mechanism for covering additional iron requirements is to release iron from the body stores[27]. Our results show that the pregnancy is associated with disturbances of oxidative/antioxidant status. They have a high level of serum and erythrocyte lipid peroxidation markers, serum uric acid and total bilirubin level, associated with a reduction in serum and erythrocyte GSH antioxidant defense, especially in the third trimester of pregnancy. Our results are consistent with several published researches[28-30] that show a decrease in antioxidative defense capacity in pregnant women especially in the third trimester of pregnancy. According to Debier[30], pregnancy is often associated with oxidative stress that reduces antioxidant vitamins and sometimes leads to premature births. The obtained results show also that an iron supplement especially in the two last trimesters of pregnancy in women causes oxidative stress characterized by elevation of MDA and decrease of GSH level in serum and erythrocyte with a high correlation with serum iron level. Iron becomes a toxic element if its level and/or distribution are not properly regulated[30]. Ferrous toxicity is developed by the production of reactive oxygen species that are formed during normal cellular metabolism[31]. H2O2is generated from transformation of the superoxide anion enzymatically (superoxide dismutase) and non-enzymatically. The most important reaction of H2O2with free or poorly ligated Fe (Ⅱ) is the Fenton reaction, generating highly reactive hydroxyl ions[32]. Fe (Ⅱ) by reacting with unsaturated fatty acids in the presence of H2O2can initiate lipid peroxidation in biological membranes and lipoproteins producing HO• leading cellular dysfunction[33]. However, any small amount of “free iron”following high levels of supplemented iron or specific mechanisms that function during the deficiency or dysregulation of iron homeostasis may increase the risk that high level of iron induces oxidative stress[34].
In conclusion, our results clearly show the role of an iron supplement in 20th and 30th week of pregnancy on the development of oxidative stress which is the origin of several maternal-fetal complications such as pre-eclampsia, miscarriage and abortion.This draws attention to the routine supplementation of iron without real control of the pregnant woman’s needs in different periods of pregnancy.
Conflict of interest statement
All authors have approved the manuscript with no conflict of interest.
Funding
This work was supported by the research project funded by the ministry of higher education, Algeria and by Directorate general for Scientific Research and Technological Development (Grant No.D01N01UN390120190001).
Author’s contributions
The conception of the study, drafting the article and interpretation of data was done by the first author Derouiche Samir; the other authors Doudi Dalal and Atia Noura were responsible for the acquisition of data and analysis.
杂志排行

Asian Pacific Journal of Reproduction的其它文章
- Erectile dysfunction and statins: The assorted view of preponderance
- Effect of short-term gavage of ethanolic extract of cogon grass (Imperata cylindrica L)root on the ovarian activity and estrus behavior of female mice
- Effect of aqueous seed extract of Mucuna pruriens on arsenic-induced testicular toxicity in mice
- Effects of ciprofloxacin on testicular tissue and sperm quality in rabbits
- Influence of N-acetylcysteine on pituitary-gonadal axis hormones and protamine expression level in streptozotocin-induced diabetic male rats
- Influence of butylated hydroxytoluene addition to cryodiluents on freezability and DNA integrity of Boer and Zaraibi buck spermatozoa