Rapid spontaneous resolution of lumbar ganglion cysts: A case report
2020-01-16VitoChiarellaAlessandroRamieriMarcoGiuglianoMaurizioDomenicucci
Vito Chiarella, Alessandro Ramieri, Marco Giugliano, Maurizio Domenicucci
Vito Chiarella, Marco Giugliano, Maurizio Domenicucci, Department of Neurological and Psychiatric, Sapienza University of Rome, Rome 00185, Italy
Alessandro Ramieri, Orthopaedic Division, Don Gnocchi Foundation, Milan 20148, Italy
Abstract
Key words: Lumbar ganglion cyst; Spontaneous resolution; Conservative treatment;Radiological disappearance; Case report
INTRODUCTION
Spinal articular cysts are more frequently found in the lumbar spine and often they are treated by surgical cystectomy, with or without spinal instrumentation. Recently,the term “ganglion” was proposed to identify the pathological entity, together with an original morphological classification to define possible localizations[1]. Remission of this type of cyst after conservative treatment was not so frequently reported in literature[2]. We report a case of clinical and radiological resolution of a symptomatic lumbar ganglion cyst (LGC) after conservative treatment, discussing mechanisms that could have led to its disappearance.
CASE PRESENTATION
Chief complaints
A 51-year-old man presented to our observation with complaints of low back and right leg pain with a L5 dermatomeric distribution.
History of past illness
His disorders persisted from 10 d.
Personal and family history
Personal and family history were negative for medical or surgical diseases.
Laboratory examinations
Lasègue test was highly positive, without neurological deficits. Tendon reflexes were normal. Laboratory tests were normal.
Imaging examinations
Lumbar MRI showed a cystic lesion in the L4-L5 spinal canal, medial and adjacent to the right internal facet joint, iso-hypointense in T1 and hyperintense in T2-weighted images, compatible with a ganglion cyst.
FINAL DIAGNOSIS
Final diagnosis was: A symptomatic right L4-L5 LGC.
TREATMENT
After discussion on treatment options, the patient was referred to medical therapy,based on NSAID, SAID for 10 d and lumbar bracing. Clinical follow-up was instituted after 4 wk, advising the patient to call us in case of neurological worsening.Surprisingly, 4 wk later, the patient showed complete resolution of the symptoms. We scheduled a new lumbar MRI after 2 d, in order to evaluate the evolution of the lesion.T1 and T2 sequences demonstrated the complete resolution of the LGC as well as compression of the right L5 nerve root (Figure 1).
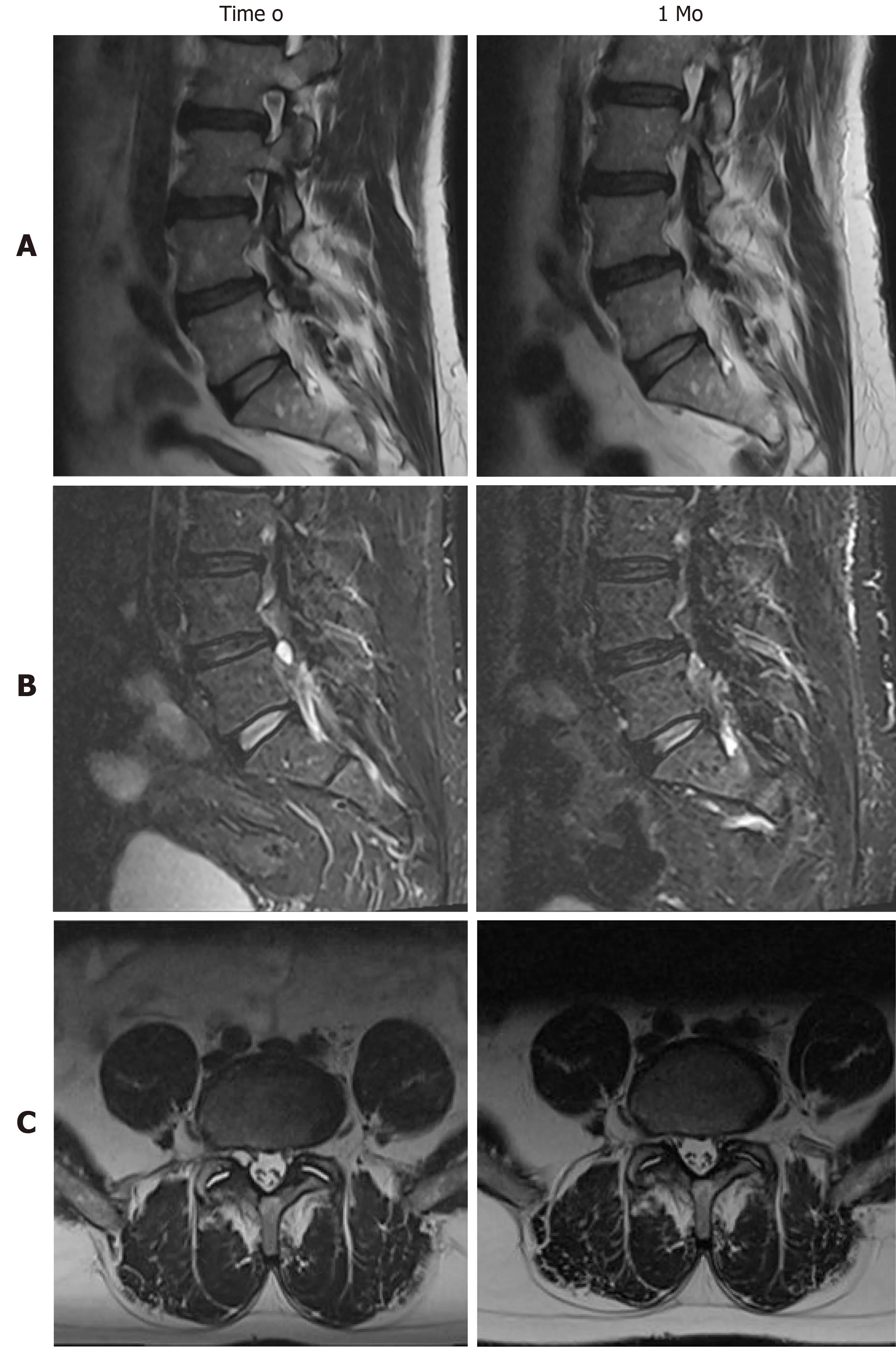
Figure 1 Radiological detection of the spontaneous disappearance of our right L4-L5 ganglion cyst,comparison of magnetic resonance imaging findings at observation (time 0) and follow-up (1 mo).
We conducted a PubMed research on literature published until October 2018. The search was undertaken using the keywords ‘‘lumbar cyst”, “ganglion cyst’’, ‘‘synovial cyst’’, “juxtafacet cyst”, “facet joint cyst”, and “resolution”. References from the retrieved reports were checked to identify other possible results. We enrolled cases with radiological documented remission of LGC and/or clinical improvement after conservative treatment based on rest, lumbar bracing, drugs and/or kinesiotherapy,excluding all those treated by surgery or deep percutaneous procedures (e.g.radiofrequency, epidural injectionetc). For every case collected, we analyzed age, sex,symptoms, neurological deficits and treatment received. When radiological data were available, we classified the localization of the LGC following our previous original classification[1]and we searched for the presence of instability signs, even in the follow-up images. Outcome clinical data were classified in 4 categories: (1) Excellent;(2) Good; (3) Fair; or (4) Poor, according to Macnab[3](Table 1).
OUTCOME AND FOLLOW-UP
Demographic, clinical and radiological data were summarized in Table 2. The total number of cases, including ours, was 26. Male: Female ratio was 1.6 (16 males and 10 females) and the mean age was 56 (range 15-75). Most of localizations were in L4-L5(17; 65%), followed by L5-S1 (6; 23%) and L3-L4 (3; 12%). In 1 case LGCs werebilateral. All classified LGCs (21; 81%) were in the spinal canal and medium: Mediumexternal in 9 cases (33%), medium-internal in 4 (15%), purely medium in 7 (26%); 1 case (4 %) was purely external (intra-foraminal); in 6 cases (22%) there were no data available to classify the LGC. In all papers the radiological diagnosis was made by MRI, except for 2 cases published before year 2000 in which diagnosis was made by CT scans. Associated spondylolisthesis was detected in 5 (19%) cases, while increased interfacet fluid in 9 (33%). Clinical presentation was constantly characterized by single or double radiculopathy due to irritation of exiting and/or traversing nerve roots.Low back pain accompanied radicular pain 11 times (42%), while pure low back pain was the only symptom in 2 cases (8%). Sensory radicular deficits were identified in 4 cases (15%). There were no cases of motor deficits. Before observation, the mean duration of symptoms was 6.8 mo (range 5 d - 36 mo). When reported (18 cases; 70%),among conservative treatments, a lumbar brace was used in 5 cases (28%),nonsteroidal anti-inflammatory drugs in 13 (72%), corticosteroids in 2 (11%) as well as gabapentin. Rest was recommended in 10 cases (55%), while kinesiotherapy(especially unloading exercises) in 8 (44%). Chiropractic manipulation was performed on 4 patients (22%). Radiological reduction or resolution of the lesion were evaluated by CT or MRI in 21 cases (81%), but in 4 cases images were not available in papers.The mean time for radiological resolution was 11 mo (range 2 d - 48 mo). Signs of instability remained unchanged, except in 2 cases (13%) for reduction of interfacet fluid amount. The mean time for clinical improvement was 7 mo (range 2 d - 24 mo).Final clinical condition was good or excellent in all cases.

Table 1 Macnab[3] criteria used for measuring outcome
DISCUSSION
The number of reported synovial cysts of the lumbar spine have been increasing probably due to the availability of magnetic resonance imaging technique. Recently,the term “ganglion” and a new morphological classification were introduced to identify the pathological entity and its localization[1].
LGCs are usually associated with osteoarthritis of the adjacent facet joint,degenerative spondylosis and/or spondylolisthesis, particularly in middle aged or elderly patients. The majority of such cysts require surgical resection due to persistent radicular symptoms and/or occasional paresis[4], that could be associated to fusion if pre-operative instability is detected[1]. While ganglion cysts elsewhere (e.g. the wrist)spontaneously resolve in 40% of patients, the spontaneous resolution of root compression with radiological disappearance of LGC were rarely reported in literature.
这与家长对孩子的客观认识有密切关系。曾有心理学家做过实验,婴儿刚出生时,很多家长都对孩子抱有极高的期待,婴儿期的快速发展也常常超家长的预期。但当孩子不断长大,有了自己的个性,也与其他孩子有了区别时,家长往往会进入一个比较的阶段,期望自己的孩子超过别人。这也是幼儿园和小学阶段,家长特别焦虑的根源之一。而到了初中、高中,孩子的能力差异、学习差异逐渐确定,家长们的焦虑也随之减轻。
We collected 24 cases from the literature[2,4,5]that affected the adult lumbar spine in adults and one more in the adolescent spine (Table 2)[6-22]. All ganglia, detected by CT or MRI and classified according to Domenicucciet al[1], were in the spinal canal and in medium position (95% of cases), except one reported by Tepeet al[15]that was purely external. Most were associated to indirect signs of segmental hypermobility (e.g.increase of synovial fluid) or proper instability. They were able to give, exiting and/or transiting nerve roots, irritation and compression, with prevalently single radiculopathy but without significant neurological deficits. Their resolution,demonstrated by radiological follow-up in 17 cases (68%), was always associated to substantial clinical improvement or full recovery. Indirect radiological signs of segmental instability remained unchanged after resolution, except in one case[10]in which occurred the reduction of interfacet synovial fluid amount, similar to our MRI follow-up findings.
Explaining the spontaneous resolution of LGC is complicated, in part because of the high prevalence of surgical removal. Some authors have supported the thesis that progressive degenerative changes of the facet joint lead to fixation of the previously hypermobile facets, so that intra-articular pressure decreases and the cyst shrinks[6].The cyst may also undergo degenerative changes, losing connection with the facetjoint and resolving because of a lack of supply[9]. Other possible causes for resolution include rupture, as seen in other different articular districts of the human body, with the extrusion of its contents, followed by reabsorption of the cystic wall[7]; or reduction of the local intra-articular forces that contributed to synovial herniation through the facet joint capsule. The last hypothesis could be supplied by the antigravitary lumbar bracing or unloading exercises usage in most cases described, including ours (11/19;58%). Also chiropractic manipulations seemed clinically effective[14,18], though only one paper[8]showed the radiological resolution of the cyst. So, in our patient, who underwent treatment with NSAIDs, corticosteroids and lumbo-sacral bracing, LGC probably resolved because of the association between decreased inflammatory fluid production and microtraumatic loads.

Table 2 Regression of lumbar ganglion cyst: Our case and 25 from literature

1Domenicucci et al[1];2Macnab[3]; SPL: Spondylolisthesis; IFF: Interfacet fluid; LBP: Low back pain; Rad: Radiculopathy; S: Sensory deficits; NSAID: Nonsteroidal antiinflammatory drug; SAID: Steroidal anti-inflammatory drug; KT: Kinesiotherapy; NR: Not reported; NA: Not available data; med: Medial; int: Internal; ext:External; MRI: Magnetic resonance; CT: Computed tomography;aIncrease;bDecrease.
An early clinical and radiological remission as ours is referred in only 2 cases[20,22].Two fast clinical resolutions were previously reported, but without radiological confirmation of the cyst reabsorption[6,18]. Other two early clinical improvement were described, but radiological resolution was achieved after over one year[16,19]. Generally,clinical improvement and radiological remission occurred on average respectively in 7 and 11 mo.
CONCLUSION
The natural history of spinal ganglion cysts is unknown and there is scant literature involving their non-surgical therapy. In the lumbar spine, different degrees of biomechanical impairment seem to play a fundamental role in their pathogenesis, but LGCs should be considered as dynamic entities. In other words, formation and resolution appear strictly influenced by event and regression of inflammatory and mechanical phenomena.
Although rarely, the symptoms related to LGC, essentially represented by low back and/or radicular pain, could regress spontaneously, if cystic evolution (enlargement,hemorrhage, worsening of spondylolisthesis) with associated worsening of neurological status does not occur.
Our case is the twenty-sixth in literature. Based on our experience and reviewing data, we can suggest that in case of absence of neurological deficits and in selected compliant patients, percutaneous procedures or surgery should be considered when conservative treatment, consisting of rest, pharmacological therapy, kinesiotherapy and/or lumbar bracing, prolonged at least for 6 mo, fails to produce symptoms control. We recommend, anti-inflammatory drugs and light unloading exercises to control pain and reduce intra-cystic fluid, but also rest and lumbar bracing to achieve the decrease of loads on arthritic facets. We also recommend MRI confirmation of cyst resolution, which can be helpful to understand mechanisms responsible of resolution.
猜你喜欢
杂志排行
World Journal of Orthopedics的其它文章
- Patents and intellectual property in orthopaedics and arthroplasty
- Use of three-dimensional printing in preoperative planning in orthopaedic trauma surgery: A systematic review and meta-analysis
- Effect of deep transverse friction massage vs stretching on football players’ performance
- Good accuracy of the alpha-defensin lateral flow test for hip periprosthetic joint infection: A pilot study in a retrospective cohort of 52 patients
- Corrections in alpha angle following two different operative approaches for CAM-type femoral acetabular impingement - Ganz surgical hip dislocation vs anterior mini-open
- National trends in total hip arthroplasty for traumatic hip fractures:An analysis of a nationwide all-payer database