lncreased circulating circular RNA_103516 is a novel biomarker for inflammatory bowel disease in adult patients
2019-11-21YuLanYeJuanYinTongHuLiPingZhangLongYunWuZhiPang
Yu-Lan Ye, Juan Yin, Tong Hu, Li-Ping Zhang, Long-Yun Wu, Zhi Pang
Abstract BACKGROUND Increasing evidence demonstrates that by acting as microRNA sponges modulating gene expression at the transcriptional or post-transcriptional level,circular RNAs (circRNAs) participate in the pathogenesis of a variety of diseases and are considered ideal biomarkers of human disease.AIM To examine the expression of circRNA_103516 in inflammatory bowel disease(IBD) and its associations with clinical phenotypes and inflammatory cytokines.METHODS Peripheral blood mononuclear cells (PBMCs) were obtained from patients with IBD, healthy controls (HCs), and patient controls (PCs). Expression of circRNA_103516 and hsa-miR-19b-1-5p was assessed by quantitative reverse transcription-polymerase chain reaction. Crohn's disease activity index (CDAI),Mayo score, C-reactive protein (CRP) level, and erythrocyte sedimentation rate(ESR) were measured. To assess the inflammatory cytokines tumour necrosis factor α (TNF-α), interferon-γ (IFN-γ), and interleukin-10 (IL-10), blood samples were analysed by flow cytometry.RESULTS Ninety Crohn’s disease (CD) and 90 ulcerative colitis (UC) patients, 80 HCs, and 35 PCs were included in the study. CircRNA_103516 was upregulated in CD and UC patients compared with HCs and PCs (P < 0.05). The area under the curve of circRNA_103516 for diagnosing CD and UC was 0.790 and 0.687, respectively. In addition, circRNA_103516 levels were increased in active CD and UC compared with remittent groups (P = 0.027, P = 0.045). Furthermore, in CD,circRNA_103516 correlated positively with CDAI (P < 0.001), CRP (P < 0.001),ESR (P < 0.001), TNFα (P < 0.001), and IFN-γ (P < 0.001) and negatively correlated with IL-10 (P = 0.006). In UC patients, circRNA_103516 correlated with Mayo score (P < 0.001), CRP (P < 0.001), ESR (P < 0.001), TNFα (P < 0.001), IFN-γ (P=0.011), and IL-10 (P = 0.002). Additionally, circRNA_103516 correlated positively with stricturing (P = 0.018) and penetrating (P = 0.031) behaviour. Moreover, hsamiR-19b-1-5p correlated negatively with circRNA_103516 in CD.CONCLUSION CircRNA_103516 levels in PBMCs can be considered an ideal candidate biomarker for diagnosing IBD. Dysregulation of circRNA_103516 may participate in the molecular mechanism of IBD through hsa-miR-19b-1-5p sponging.
Key words: Circular RNA; Circular RNA_103516; Inflammatory bowel diseases;Biomarker
INTRODUCTION
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD), comprises chronic inflammatory disorders of the gastrointestinal tract.IBD pathogenesis is believed to involve a complex interplay among immunology,genetic predisposition, and environmental risk factors[1-3]. Due to the characteristic of repeated recurrence, the disease activity of IBD must be assessed and monitored repeatedly. However, as most conventional detection methods are invasive, current detection methods are not suitable for repeated clinical applications. To overcome this limitation, serological biomarkers may constitute an optimal alternative choice for evaluating and screening disease activity in IBD.
Circular RNAs (circRNAs) are covalently closed continuous single-stranded RNA molecules that have advantageous properties because their circular structure enables rolling circle RNA replication and producing multiple genomic copies once a single initiation event occurs[4,5]. However, the characteristics of circRNAs are much less clear than those of microRNAs (miRNAs) and long noncoding RNAs (lncRNAs).Nonetheless, research on their functions has recently emerged, and increasing evidence demonstrates that circRNAs can modulate gene expression at the transcriptional or post-transcriptional level by sponging miRNAs or by interacting with other molecules[6]. Furthermore, circRNAs are evolutionally conserved, and their expression is relatively stable in the cytoplasm; these features indicate that circRNAs may be ideal biomarkers in human disease[7]. Although much remains to be revealed regarding circRNA biology and gene regulatory mechanisms, studies have elucidated their function in a variety of cancers[8], cardiovascular disease[9], autoimmune disease[10], and nervous system disorders[11], among others.
To date, little is known about the relationships between circRNAs and IBD. Our previous research based on microarray analysis identified 155 upregulated circRNAs and 229 downregulated circRNAs in peripheral blood mononuclear cells (PBMCs)from CD patients compared with healthy controls (HCs). Moreover, some aberrantly expressed circRNAs were chosen for evaluation of their potential use in the diagnosis of CD[12].
In this study, we focused on circRNA_103516, which is located at chr3: 171969049-172028671 and spliced fromFNDC3B. It was reported thatFNDC3Bmight play a role in the epithelial-to-mesenchymal transition and activates several cancer pathways,including phosphoinositide 3-kinase/Akt, retinoblastoma 1, and transforming growth factor (TGF) β signalling[13]. Our bioinformatics analysis showed that hsa_circRNA_103516 is predicted to harbour hsa-miR-147b, hsa-miR-19b-1-5p, hsamiR-134-3p, hsa-miR-576-5p, and hsa-miR-493-5p. Among them, miR-19b was found to be decreased in the serum and intestinal tissue of IBD patients[14]. Thus, in the present study, we explored the link between circRNA_103516 and hsa-miR-19b-1-5p in PBMCs from IBD patients and determined its possible correlations with the clinical phenotypes of CD and UC.
MATERIALS AND METHODS
Patient samples
Between January 2018 and December 2018, 180 IBD patients (90 with CD and 90 with UC) were prospectively recruited from the Department of Gastroenterology of the North District of the Affiliated Suzhou Hospital of Nanjing Medical University(Jiangsu, China). Eighty HCs and 35 patient controls (PCs) were also included. The age and sex of all groups were matched. The inclusion criteria were: (1) A diagnosis of IBD established based on clinical manifestations, radiological findings, and endoscopic and histological criteria; (2) Age from 17 to 75 years old; and (3)Demographic and clinical information collected by experienced clinicians reviewing and completing medical questionnaires. Patients with irritable bowel syndrome were used as the PCs. The exclusion criteria were as follows: (1) Isolated upper digestive tract involvement; (2) Other coexisting autoimmune diseases, including systemic lupus erythematosus, rheumatoid arthritis, and asthma; and (3) A history of malignant tumour or severe infection (Figure 1). Disease activity was identified according to the CD activity index (CDAI) for CD and the Mayo score for UC[15,16].Active IBD was defined as CDAI above 150 points or Mayo clinical score above 2. The sites and behaviour of the disease were defined according to the Montreal classification[17]. For assessing circRNA_103516, hsa-miR-19b-1-5p, C-reactive protein(CRP), erythrocyte sedimentation rate (ESR), TNF-α, interferon-γ (IFN-γ), and interleukin-10 (IL-10), blood samples were collected into ethylenediamine tetraacetic acid tubes for testing within one week before or after endoscopy.
Ethics statement
The present study was approved by the Ethics Committees of the Affiliated Suzhou Hospital of Nanjing Medical University (Jiangsu, China). All IBD patients and control subjects signed an informed consent form, in accordance with the relevant guidelines and regulations.
Extraction of total RNA from PBMCs
PBMCs were immediately separated after blood sample collection from each donor according to the manufacturer’s protocol (GE Healthcare, Uppsala, Sweden). Two millilitres of blood diluted in 2 mL of saline solution was layered onto 4 mL of Ficoll-Paque PLUS. After centrifugation for 30 min at 400gat room temperature, the interlayer was collected by washing twice with the same volume of saline solution.The precipitate was gathered by centrifuging for 15 min at 90gat room temperature.PBMCs were then frozen at -80 °C. TRIzol reagent (Invitrogen, Carlsbad CA, United States) was utilized for total RNA extraction from the PBMCs.
Quantitative reverse transcription-polymerase chain reaction (qRT-PCR)
determination of circRNA_103516 levels
Total RNA was reverse transcribed using a PrimerScript Realtime Reagent Kit (Takara Bio Inc., TaKaRa, Shiga, Japan), and expression of circRNA_103516 was quantitated with TB Green™ Premix Ex Taq™ II (Tli RNaseH Plus; TaKaRa, Shiga, Japan) and a LightCycler 480II real-time PCR system (Roche, Rotkreuz, Switzerland). The 2-ΔΔCt method was employed to analyse the data. β-actin was used as an internal reference.The primer sequences are presented in Table 1. In total, the cycling parameters for PCR were 30 s for 95 °C, followed by 40 cycles of denaturation at 95 °C for 5 s and annealing and extension at 60 °C for 30 s.
TNF-α, IFN-γ, and IL-10 measurements by flow cytometry
According to the manufacturer’s instructions, TNFα, IFN-γ, and IL-10 levels in plasma samples from IBD patients were measured using flow cytometry (FCM) kits(Hangzhou Cellgene Biotechco, LTD, China).

Figure 1 Flow chart of patient selection in the study and main study procedures. CD: Crohn’s disease; UC:Ulcerative colitis; IBS: Irritable bowel syndrome; CRP: C reactive protein; ESR: Erythrocyte sedimentation rate; TNF-α: Tumor necrosis factor α; INF-γ: Interferon γ; IL-10: Interleukin-10; PPV: Positive predictive value; NPV: Negative predictive value.
Annotation of circRNA/miRNA interaction
TargetScan (http://www.targetscan.org/) and miRanda (http://www.microrna.org/) were used to predict circRNA/miRNA interactions. Differential expression of circRNA_103516, as identified by qRT-PCR, was annotated in detail with the circRNA/miRNA interactions. Additionally, the sequences of MREs and predicted miRNA targets were examined.
Hsa-miR-19b-1-5p determination by qPCR
Expression of miR-19b-1-5p (predicted from annotations) in PBMCs from the 90 patients with CD and 90 patients with UC was detected using a Hairpin-itTMqRT-PCR miRNA Kit (GenePharma, LTD, China). U6 was used as an internal reference. The primer sequences used for hsa-miR-19b-1-5p are: 5’-UGUGCAAAUCCA UGCAAAACUG-3’ (forward) and 5’-GCTCACTGCAACCTCCTCCTCC-3’ (reverse).The primer sequences used for U6 are 5’-GCTTCGGCAGCACATA-TACTAAAAT-3’(forward) and 5’-CGCT-TCACGAATTTGCGTGTCAT-3’ (reverse). The PCR conditions included predenaturation at 95 °C for 3 min, followed by 40 cycles of denaturation at 95 °C for 12 s and annealing and elongation at 62 °C for 40 s. The 2-ΔΔCt method was used to analyse the data.
Statistical analysis
The results are reported as the mean ± standard deviation or median (25%75%);assays were performed in triplicate. The unpairedt-test or Mann-Whitney U-test was applied to compare continuous variables for two groups. Multiple comparisons were assessed by one-way analysis of variance or theχ2test. Spearman’s analysis was performed to determine linear correlation in different groups. Receiver operating characteristic curve analysis was employed to evaluate the clinical diagnostic value of
candidate circRNAs. Logistic regression was used to identify risk factors. APvalue <0.05 was considered statistically significant. The statistical analyses were performed using the package SPSS 19.0 (SPSS Inc., IBM, United States) for windows and GraphPad Prism 7.04 (GraphPad Software, San Diego, CA, United States).
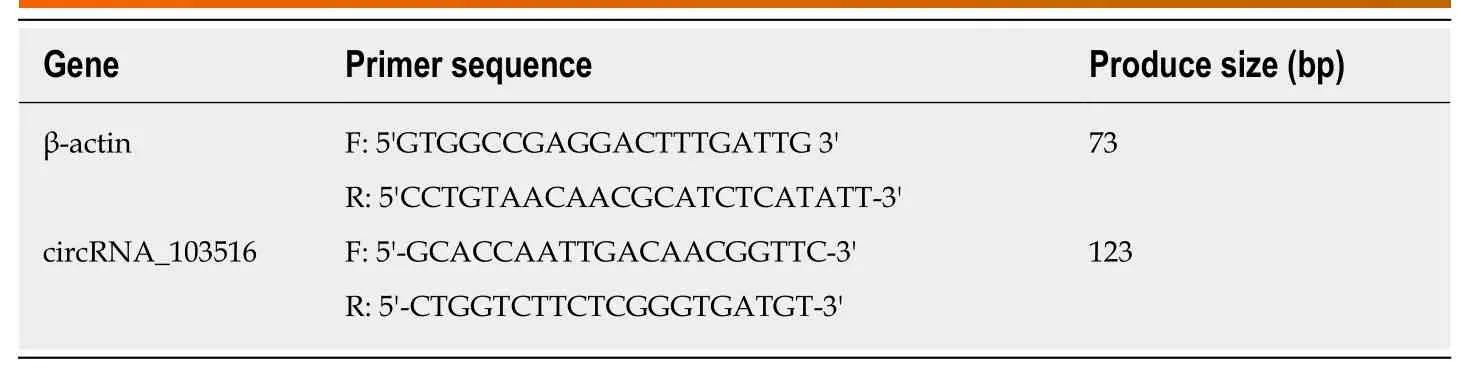
Table 1 Sequences of primers used for quantitative reverse transcription-polymerase chain reaction
RESULTS
Characteristics
The demographic and clinical data of the IBD patients and health controls and PCs are listed in Table 2. There were 90 CD patients [48 males (53.3%), mean age 39.94 years],90 UC patients [38 males (42.2%), mean age 41.69 years], 80 HCs [46 males (57.5%),mean age 37.64 years], and 35 PCs [19 males (54.3%), mean age 42.40 years]. Age and sex were not significantly different among the four groups (P> 0.05). CD and UC activity was classified as remission, mild, moderate, or severe according to CDAI and the Mayo score. Laboratory test results (CRP, ESR, TNF-α, INF-γ, and IL-10) and disease activity are shown in Table 3.
CircRNA_103516 expression in PBMCs from IBD patients and controls
Expression of circRNA_103516 in PBMCs was increased in CD patients [2.085(1.1953.510)] compared with that in UC patients [1.385 (0.9252.599),P= 0.003], HCs[0.901 (0.7241.376),P< 0.001], and PCs [0.901 (0.7421.375),P< 0.001]. The expression level of circRNA_103516 was higher in PBMCs from the UC group compared with those of the HC (P= 0.004) and PC (P= 0.025) groups. However, there was no significant difference between the HC and PC groups (P= 0.998) (Figure 2).
The diagnostic value of circRNA_103516 in differentiating the CD group from the HC group [area under the curve (AUC) = 0.790, 95% confidence interval (CI): 0.722-0.857] and the UC group (AUC = 0.631, 95%CI: 0.550-0.712) was also examined (Figure 3A and C, Table 4). Overall, circRNA_103516 may be considered a predictive factor in differentiating UC from HC (AUC = 0.687, 95%CI: 0.608-0.767) (Figure 3B, Table 4).The level of circRNA_103516 was considered positive at a cutoff value > 1.412 for CD and > 1.151 for UC (Table 4).
Correlations of circRNA_103516 expression with disease activity in IBD
The expression level of circRNA_103516 was markedly increased, with values 2.614-fold and 1.953-fold higher in PBMCs from active CD and active UC, respectively (P<0.001 andP< 0.001, respectively). However, expression was only 1.639-fold and 1.319-fold higher in CD and UC patients who were in remission, respectively (P< 0.001 andP= 0.024, respectively) (Figure 4A), and circRNA_103516 levels in active CD and UC were higher than those in remittent CD and UC (P= 0.027,P= 0.045) (Figure 4A and B).
Additionally, circRNA_103516 levels exhibited a positive correlation with disease activity and laboratory tests. In CD patients, circRNA_103516 correlated positively with CDAI (r= 0.554,P< 0.001), CRP (r= 0.470,P< 0.001) and ESR (r= 0.466,P<0.001) (Figure 5A-C); in UC patients, circRNA_103516 correlated with the Mayo score(r= 0.460,P< 0.001), CRP (r= 0.424,P< 0.001), and ESR (r= 0.407,P< 0.001) (Figure 5D and F).
Correlations of circRNA_103516 expression with inflammatory cytokines in IBD
CircRNA_103516 levels showed a positive correlation with TNFα and IFN-γ, though negative correlations were found for circRNA_103516 with IL-10.
In CD patients, circRNA_103516 correlated positively with TNFα (r= 0.637,P<0.001) and IFN-γ (r= 0.595,P< 0.001) and negatively with IL-10 (r= -0.287,P= 0.006)(Figure 6A-C). Similarly, we observed a correlation of circRNA_103516 with TNFα (r= 0.412,P< 0.001), IFN-γ (r= 0.267,P= 0.011), and IL-10 (r= -0.330,P= 0.002) in UC patients (Figure 6E and F).
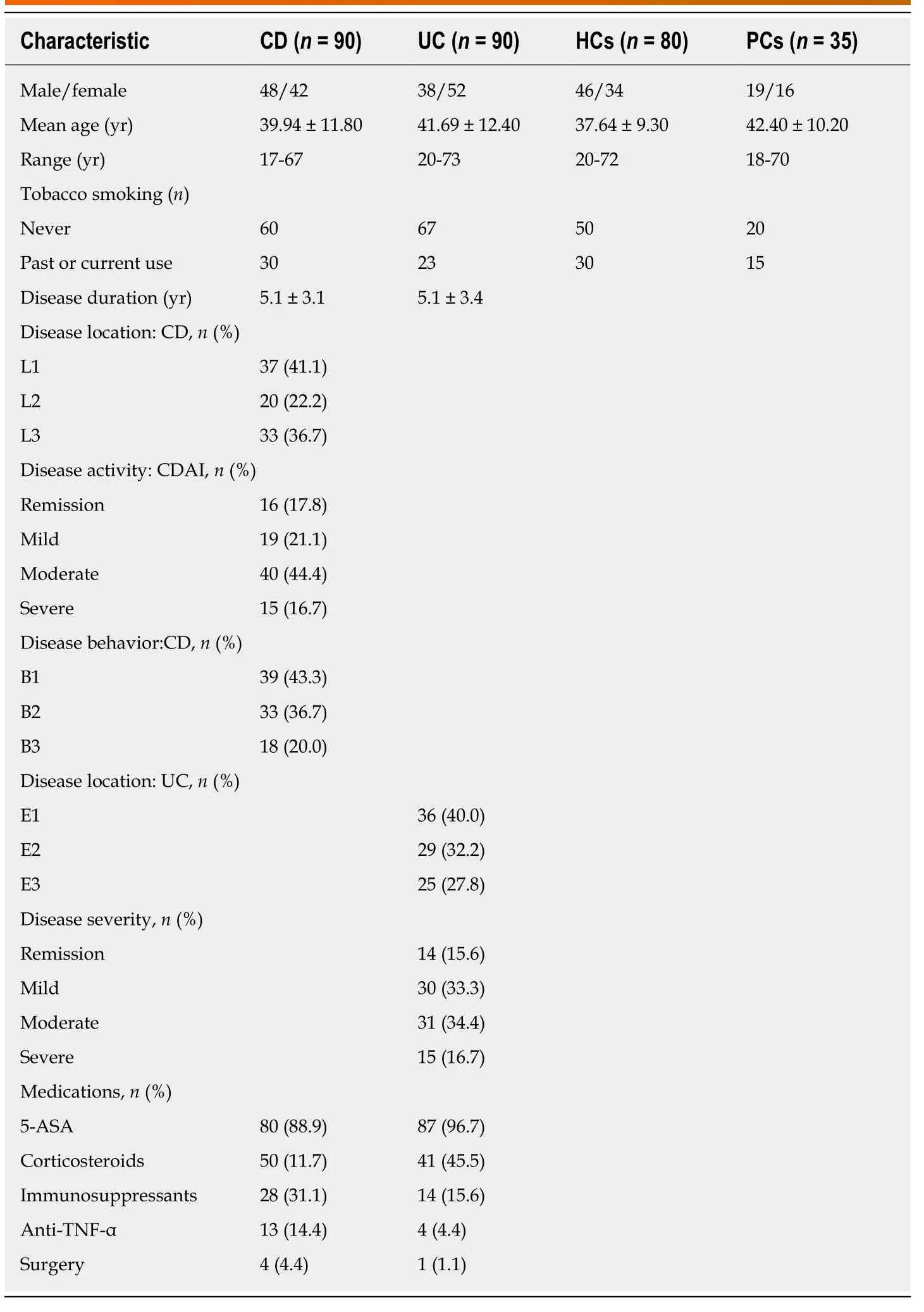
Table 2 Clinical characteristics of patients and controls
Correlations of circRNA_103516 status with subgroups of IBD
The disease phenotypes of CD compared with the corresponding circRNA_103516 status are listed in Table 5. The prevalence of circRNA_103516 positivity was higher in patients with moderate and severe CD than in patients with mild disease (82.5%,80.0%vs47.4%,P= 0.008,P= 0.025). After adjustment for sex, age, and smoking,bivariate logistic analysis showed that positive circRNA_103516 was independently associated with an increased risk of disease activity [moderate: odds ratio (OR) =4.886, 95%CI: 1.383-17.251,P= 0.014; severe: OR = 4.416, 95%CI: 0.084-22.054,P=0.043]. Additionally, circRNA_103516 positivity was more frequently detected in patients with complicated CD (B2/B3) compared with those with the simple phenotype (B1) (78.8%, 77.8%vs48.7%,P= 0.011,P= 0.045). After adjusting for clinical factors, logistic analysis also identified that circRNA_103516 correlated independently with an increased risk of stricturing (OR = 3.641, 95%CI: 1.245-10.650,P= 0.018) and penetrating (OR = 4.375, 95%CI: 1.147-16.690,P= 0.031) behaviour. In contrast, circRNA_103516 showed no correlation with disease location or medications.
In UC, circRNA_103516 positivity was associated with an increased risk of more severe disease behaviour (OR = 10.803, 95%CI: 1.171-94.687) (Table 6), though statistical power was not high due to the small number of patients with severe UC. No correlation of circRNA_103516 positivity with any other variable in UC was observed.
Interaction between circRNA_103516 and miRNAs
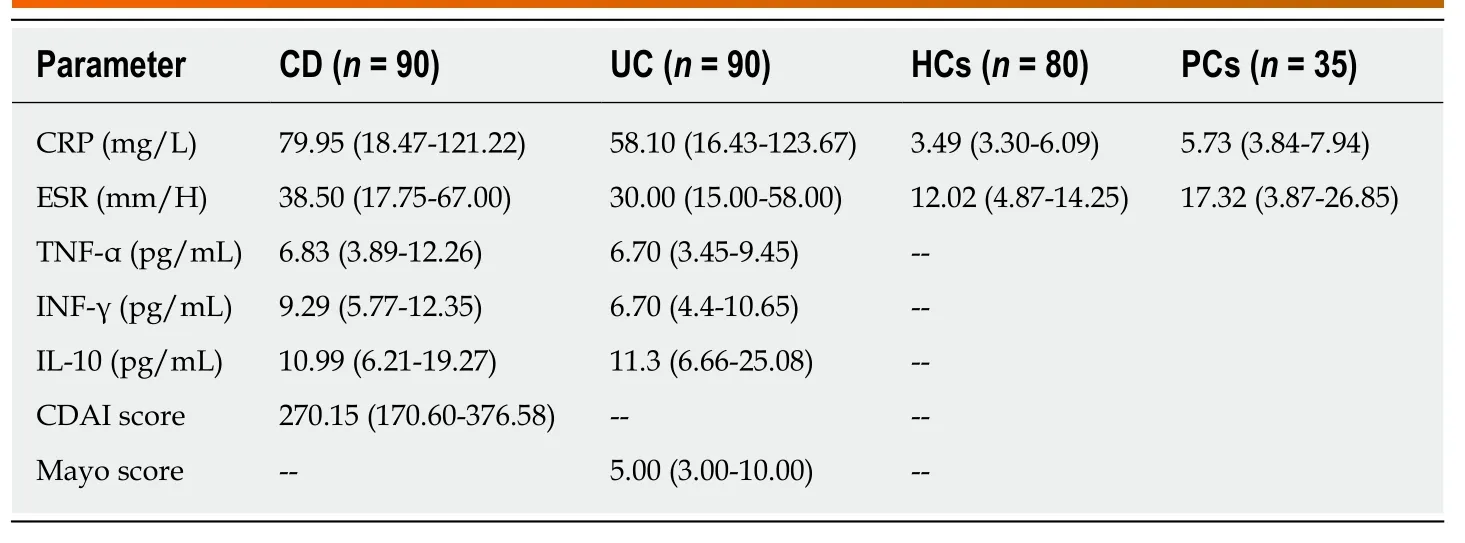
Table 3 Laboratory measures and disease activity scores of inflammatory bowel disease patients and control groups
Using miRNA target prediction software targetScan and miRanda, we investigated the top five predicted miRNA targets for circRNA_103516. The candidate hsa_circRNA_103516 is predicted to harbour sites for hsa-miR-147b, hsa-miR-19b-1-5p, hsa-miR-134-3p, hsa-miR-576-5p, and hsa-miR-493-5p, with different seed region types (i.e., 8mer, 7mer-m8, offset 6mer, and imperfect, respectively). We chose hsamiR-19b-1-5p for detailed investigation of a correlation with circRNA_103516.
Correlation of circRNA_103516 expression with hsa-miR-19b-1-5p in IBD
The expression level of circRNA_103516 correlated negatively with hsa-miR-19b-1-5p.In CD patients, circRNA_103516 showed a negative correlation with hsa-miR-19b-1-5p (r= -0.395,P< 0.001) (Figure 7A). In contrast, there was no significant correlation between circRNA_103516 and hsa-miR-19b-1-5p in patients with UC (r= -0.167,P=0.116) (Figure 7B).
DISUSSION
The diagnosis and therapy of IBD involve enormous challenges that can only be addressed by obtaining a better understanding of the molecular mechanisms of IBD.Currently, owing to the advent of high-density microarrays, numerous noncoding RNAs are being considered as novel and potent regulators of gene expression.Noncoding RNAs comprise miRNAs, lncRNAs, circular RNAs, ribosomal RNAs, and snRNPs as well as a variety of regulatory RNAs[18]. Among them, circRNAs are ideal diagnostic and therapeutic candidates due to their stability and conservation[19]. The most profound studies between circRNAs and diseases are with regard to tumours[20].For example, circEXOC6B and circN4BP2L2 are considered novel prognostic biomarkers in epithelial ovarian cancer[21]. Circ_0001451 was found to be downregulated in clear cell renal cell carcinoma and a potential biomarker for treatment of the disease[22]. Furthermore, sponging of miR-200a by circular RNA 101368 regulates the migration of hepatocellular carcinoma cellsviathe HMGB1/RAGE pathway[23].
Hundreds of miRNAs and lncRNAs have been reported to participate in IBD pathogenesis and can be considered as biomarkers for these patients[24,25].Nevertheless, the roles of circRNA in IBD have only begun to be elucidated.
Our previous research investigated circRNA microarray profiles in peripheral blood from adults with CD, revealing 384 differential circRNAs in CDvsHCs, with 155 increased circRNAs and 229 decreased circRNAs; thus, these molecules have great potential for investigating the pathogenesis of CD. In the present study, we focused on circRNA_103516 and validated it by real-time PCR in a larger IBD cohort. First,circRNA_103516 exhibited strong clinical diagnostic value for CD and UC, suggesting that circRNA_103516 may be considered a novel biomarker for IBD. Second,circRNA_103516 was significantly more upregulated in the active stage than in the remission stage of both CD and UC, with positive correlations with disease activity(CDAI, Mayo, CRP, and ESR). Third, circRNA_103516 correlated positively with proinflammatory cytokines (TNF-α and INF-γ) in CD and UC patients and negatively with anti-inflammatory cytokines (IL-10). Fourth, logistic regression analysis revealed that circRNA_103516 was independently associated with an increased risk of disease activity in CD and UC. These data indicate that circRNA_103516 may have a proinflammatory role.
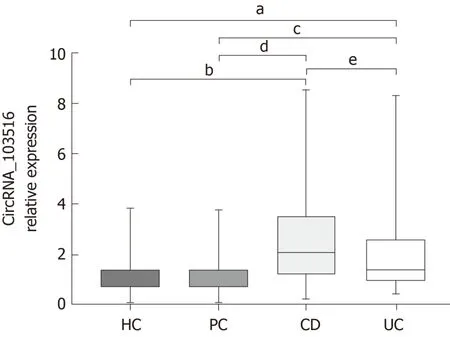
Figure 2 Circular RNA_103516 relative expression in patients with Crohn’s disease, patients with ulcerative colitis, healthy controls, and patient controls. Circular RNA (circRNA)_103516 was increased in Crohn’s disease(CD) and ulcerative colitis (UC) patients compared with healthy controls (HC) and patient controls (PC). A significant difference in circRNA_103516 was detected between CD and UC groups. Comparing the relative circRNA levelsbetween two groups was performed by the Mann Whitney U-test. aP < 0.05 vs HC and bP < 0.001 vs HC; cP < 0.05 vs PC; dP < 0.001 vs PC; eP < 0.05 vs UC. P < 0.05 was considered statistically significant. CD: Crohn’s disease, UC:Ulcerative colitis, HC: Healthy controls, PC: Patient controls; CircRNA: Circular RNA.
Given the roles of circRNAs as miRNA sponges and gene regulators[6,26], we investigated the top five predicted miRNA targets for circRNAs and identified that circRNA_103516 may target hsa-miR-147b, hsa-miR-19b-1-5p, hsa-miR-134-3p, hsamiR-576-5p, and hsa-miR-493-5p, competitively restraining miRNA activity. We chose hsa-miR-19b-1-5p to further evaluate the correlation with circRNA_103516 in detail.The current study showed that circRNA_103516 correlated negatively with hsa-miR-19b-1-5p in CD patients.
Interestingly, previous studies have identified that miR-19b levels are decreased in the serum and intestinal tissue of IBD patients[14,27], which is consistent with our study.Research has also shown that miR-19b may participate in abnormal inflammatory reactions by inhibiting suppressor of cytokine signalling 3 to regulate chemokine production in intestinal epithelial cells[27]. Furthermore, miR-19 and its family members modulate the chronic inflammatory process by activating NF-κB signalling in rheumatoid arthritis[28]. The NF-κB signalling pathway plays a vital role in autoimmune diseases by regulating T cell and macrophage development and function, ultimately participating in the inflammatory process and immune regulation[29]. Moreover, miRNA19b modulates Th17 cell development by targeting thymic stromal lymphopoietin[30]and has a vital function by suppressing the IL-10 level in peripheral dendritic cells[31]. Thus, we suggest that circRNA_103516 acts as a proinflammatory gene by sponging miRNA19b and is involved in the pathogenesis of IBD by mediating inflammation and immune-related signalling pathways.
Previous studies have shown that serum levels of miR-19 correlated negatively with stricturing CD[14]. The groups of Zhao and Zou attempted to explain these results by uncovering a new mechanism in which miR-19b depresses fibrogenesis by targeting TGF-beta receptor 2 in biliary atresia-related fibrosis[32]and myocardial fibrosis[33]. However, our study identified that circRNA_103516 positivity may be an independent risk factor for CD stricture and penetrating behaviour. Indeed, a higher prevalence of circRNA_103516 positivity was found in patients with complicated CD(stricturing and penetrating). These results further suggest that circRNA_103516 may play a significant role in the development and progression of CD by acting as a microRNA19b sponge. Nevertheless, elucidation of the precise function of miRNA-circRNA interactions in CD pathogenesis requires further research.
To the best of our knowledge, this is the first study to identify the relationship between circRNA_103516 expression in PBMCs and disease activity and the risk of IBD and inflammatory cytokines. Nonetheless, certain limitations in our study should not be neglected. First, the number of subjects was not large, which might have affected the results. In addition, a more diverse disease control group is needed for a more applicable conclusion. Second, we identified miRNA-circRNA interactions only by functional analysis and not by experimental verification. Thus, further research is needed.
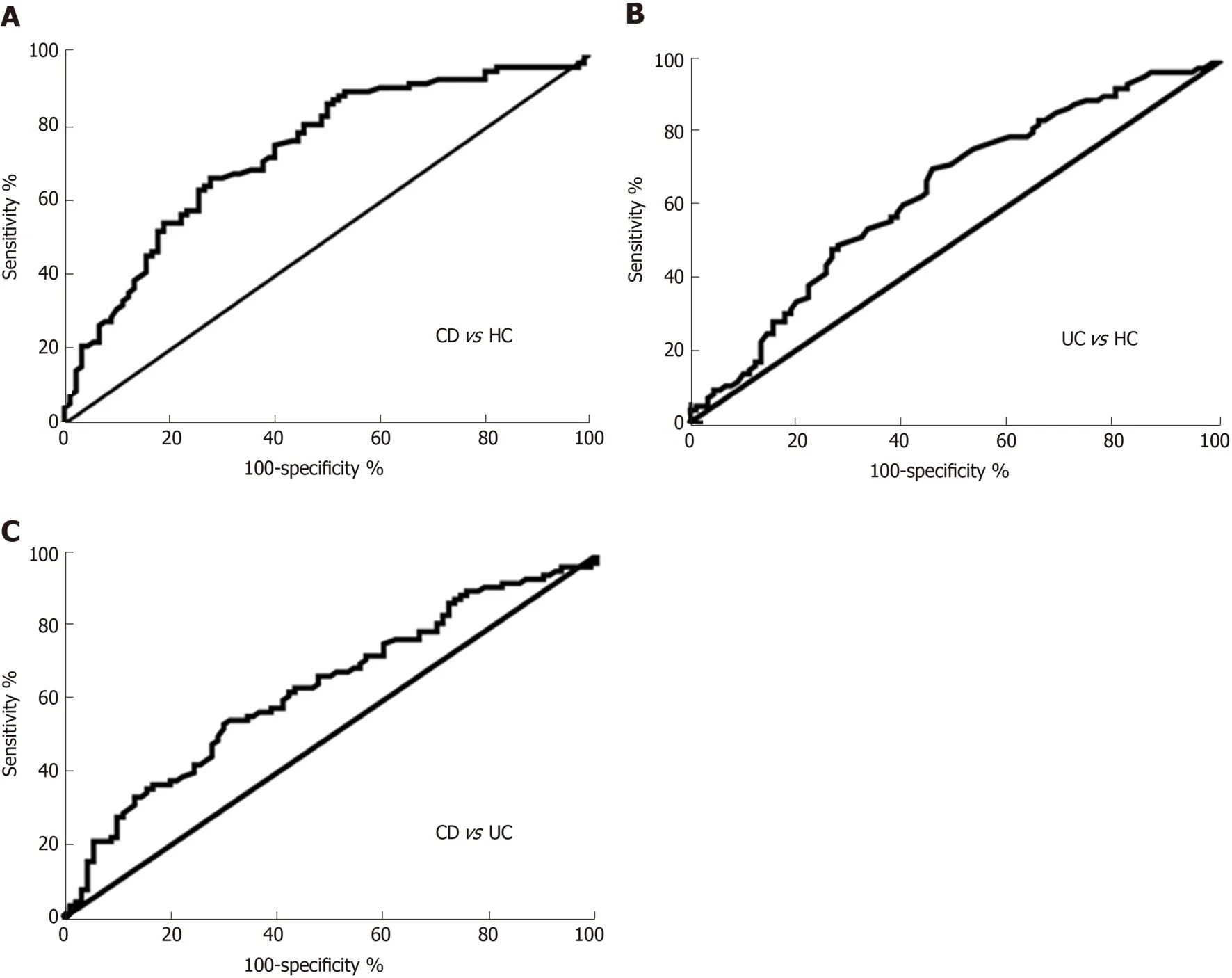
Figure 3 Receiver operating characteristic analysis of circular RNA_103516 in peripheral blood mononuclear cells from patients with Crohn’s disease and ulcerative colitis. A: Circular RNA (circRNA)_103516 was able to differentiate CD from HC; B: CircRNA_103516 could differentiate UC from HCs; C:CircRNA_103516 was able to differentiate CD from UC. CD: Crohn’s disease; UC: Ulcerative colitis; HCs: Healthy controls.
In conclusion, we verified that increased circRNA_103516 levels are a prospective candidate marker for IBD diagnosis and correlate positively with disease activity and behaviour in CD patients. Moreover, circRNA_103516 may participate in the molecular mechanism of CD by sponging miR-19b. The precise molecular mechanisms underlying circRNA functions in CD require further investigation.
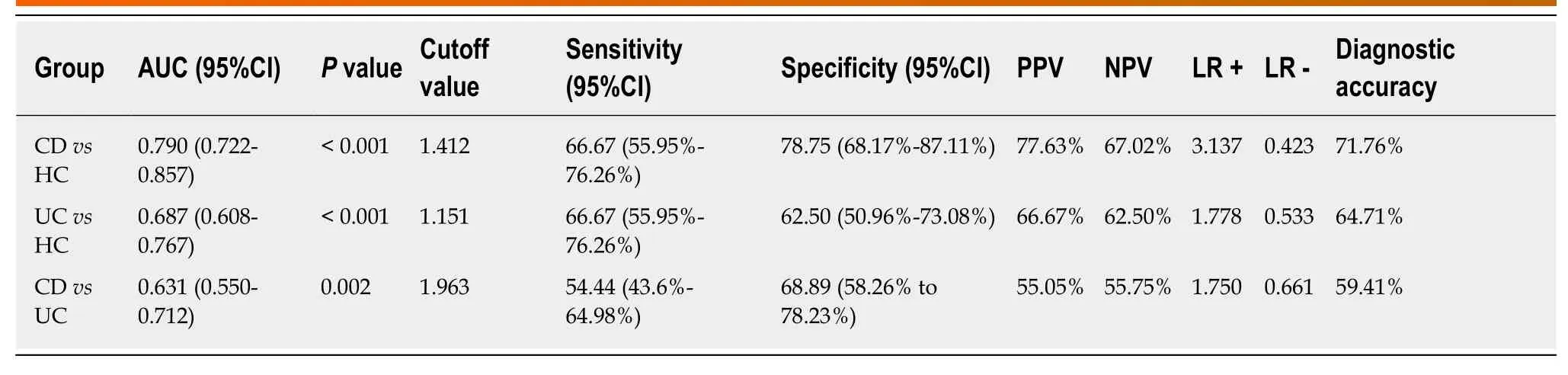
Table 4 Receiver-operating characteristic analysis of circular RNA_103516 in peripheral blood mononuclear cells from inflammatory bowel disease
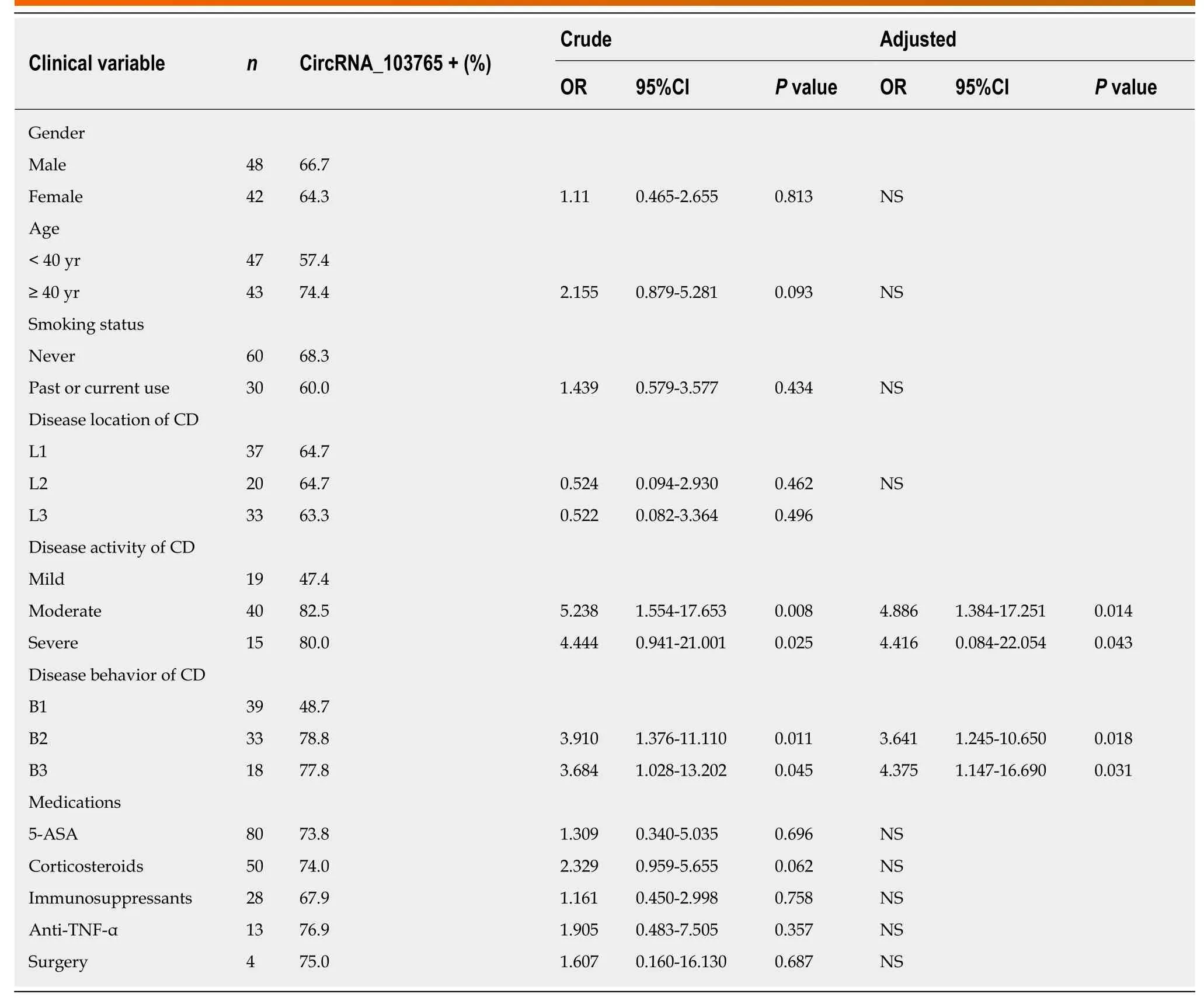
Table 5 Univariate logistic regression analysis showing the disease phenotypes of Crohn’s disease in correlation to circular RNA_103516 status as dependent variable
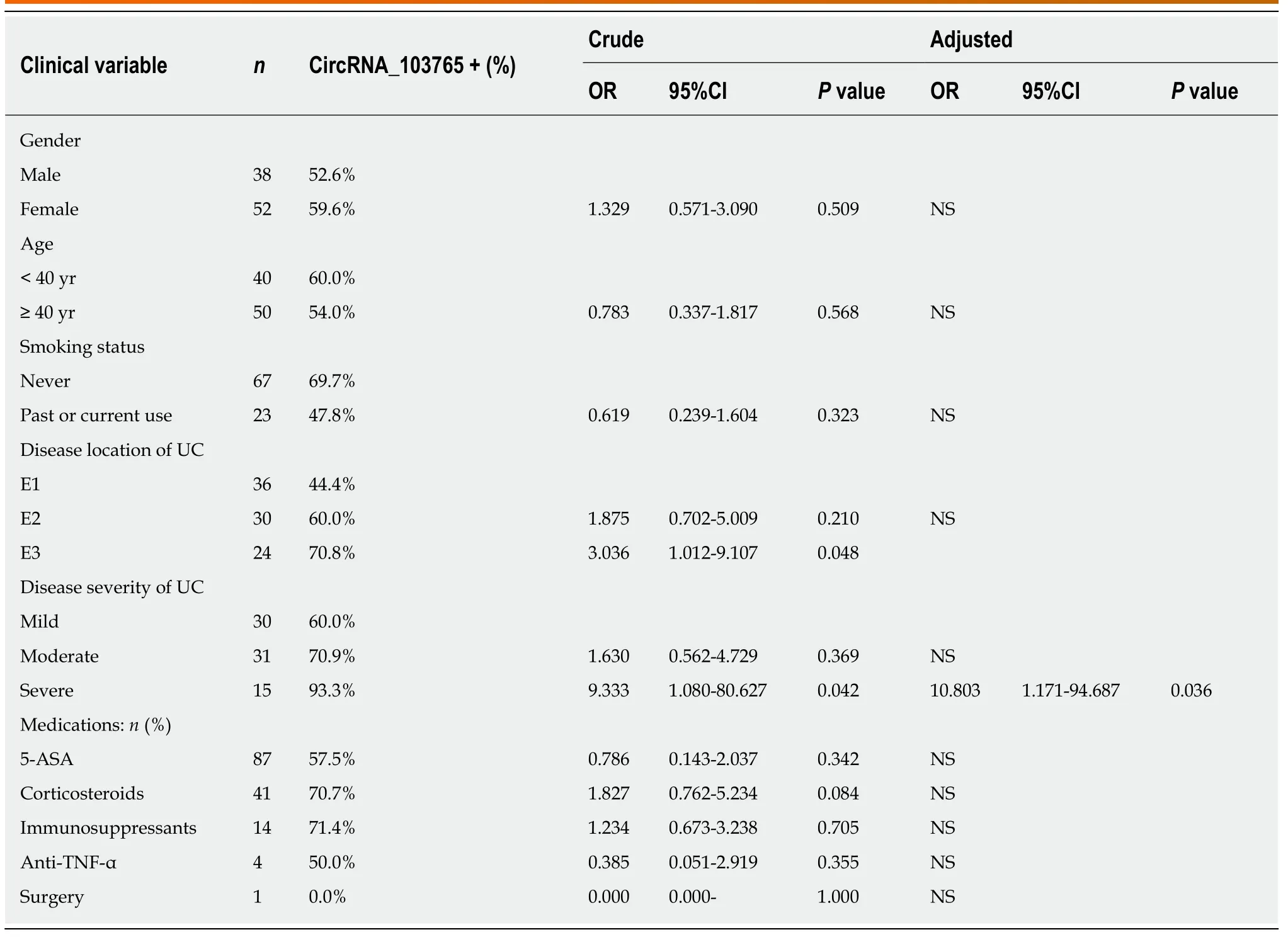
Table 6 Univariate logistic regression analysis showing the disease phenotypes of ulcerative colitis in correlation to circular RNA_103516 status as dependent variable
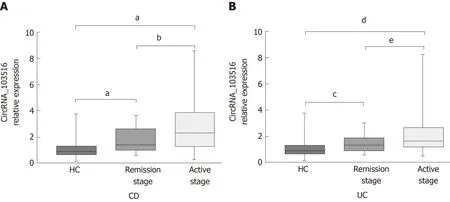
Figure 4 Expression of circular RNA_103516 in peripheral blood mononuclear cells from inflammatory bowel disease patients at different stages. A:Circular RNA (circRNA)_103516 in CD patients at different stages. aP < 0.001 vs HCs; bP < 0.05, remission stage vs active stage. B: CircRNA_103516 in UC patients at different stage. cP < 0.05 vs HCs; dP < 0.001 vs HCs; eP < 0.05, remission stage vs active stage. P < 0.05 was considered statistically significant. CD: Crohn’s disease; UC: Ulcerative colitis; CircRNA: Circular RNA.
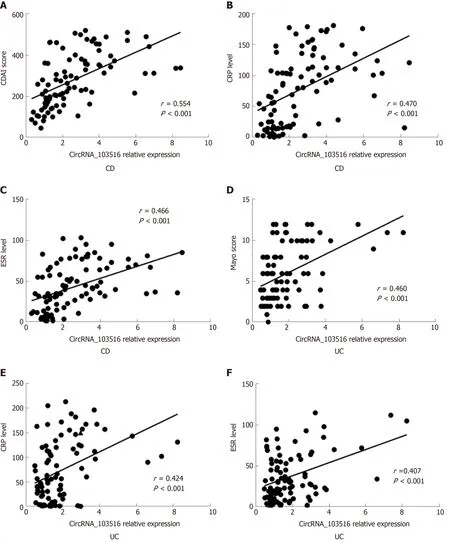
Figure 5 Correlations of circular RNA_103516 expression with Crohn's disease activity index, Mayo score, C reactive protein, and erythrocyte sedimentation rate in inflammatory bowel disease patients. Spearman’s analysis was applied to test the correlation of circular RNA (circRNA)_103516 expression with disease activity. A-C: Correlations of circRNA_103516 expression with disease activity in patients with CD; D-F: Correlations of circRNA_103516 expression with disease activity in patients with UC. P < 0.05 was considered statistically significant. CD: Crohn’s disease; UC: Ulcerative colitis; CDAI: Crohn's disease activity index;CRP: C reactive protein; ESR: Erythrocyte sedimentation rate; CircRNA: Circular RNA.
Figure 6 Correlations of circular RNA_103516 expression with inflammatory cytokines in inflammatory bowel disease. A-C: Correlations of circular RNA(circRNA)_103516 expression with TNFα, IFN-γ, and IL-10 in CD; D-F: Correlations of circRNA_103516 expression with TNFα, IFN-γ, and IL-10 in UC. P < 0.05 was considered statistically significant. CD: Crohn’s disease; UC: Ulcerative colitis; TNF-α: Tumor necrosis factor α; INF-γ: Interferon γ; IL-10: Interleukin-10; CircRNA:Circular RNA.
ARTICLE HIGHLIGHTS
Research background
Inflammatory bowel disease (IBD), including ulcerative colitis (UC) and Crohn’s disease (CD),comprises chronic gastrointestinal tract inflammatory disorders. Due to the characteristic of repeated recurrence, the disease activity of IBD must be assessed and monitored repeatedly.Accordingly, non-invasive serological biomarkers may constitute an optimal alternative choice for evaluating and screening disease activity in IBD. Increasing evidence demonstrates that circular RNAs (circRNAs) participate in the pathogenesis of a variety of diseases by modulating gene expression at the transcriptional or post-transcriptional level and are considered ideal biomarkers in human disease.
Research motivation
To date, little is known about the relationships between circRNAs and IBD. Our previous research identified 155 upregulated circRNAs and 229 downregulated circRNAs by microarray analysis of peripheral blood mononuclear cells (PBMCs) from CD patients compared with healthy controls (HCs). Moreover, bioinformatics analysis predicted that hsa_circRNA_103516 might participate in the pathogenesis of IBD by sponging hsa-miR-19b-1-5p.
Research objectives
The aim of this study was to identify expression of circRNA_103516 in IBD and its association with clinical phenotypes and inflammatory cytokines.
Research methods
We performed an observational study. PBMCs were obtained from patients with IBD, HCs, and patient controls. Expression of circRNA_103516 and hsa-miR-19b-1-5p was assessed by quantitative reverse transcription-polymerase chain reaction. Crohn's disease activity index(CDAI), Mayo score, C-reactive protein (CRP) level, and erythrocyte sedimentation rate (ESR)were measured. Flow cytometry was used to examine blood samples for the measurement of the inflammatory cytokines tumour necrosis factor-α, interferon-γ (IFN-γ), and interleukin-10 (IL-10). Spearman correlation analysis was performed to determine linear correlations for different groups. Receiver operating characteristic curve analysis was used to assess the clinical diagnostic value of candidate circRNAs. Logistic regression analysis was used to identify risk factors.
Research results
CircRNA_103516 was upregulated in CD and UC. Furthermore, circRNA_103516 correlated positively with CDAI, Mayo score, CRP, ESR, TNFα, and IFN-γ and negatively with IL-10 in IBD. Additionally, circRNA_103516 correlated positively with stricturing and penetrating behaviour. The predicted hsa-miR-19b-1-5p correlated negatively with circRNA_103516 in CD.
Research conclusions
CircRNA_103516 in PBMCs can be considered an ideal candidate for the diagnosis of IBD.Dysregulation of circRNA_103516 may participate in the molecular mechanism of IBD through hsa-miR-19b-1-5p sponging.
Research perspectives
More large prospective multicentre clinical studies need to be performed for a more applicable conclusion. In addition, miRNA-circRNA interactions were conducted by functional analysis and not by experimental verification. It is imperative to further explore their respective molecular mechanisms and genetic changes to achieve better diagnostic and treatment strategies in the future.
杂志排行
World Journal of Gastroenterology的其它文章
- Blood parameters score predicts long-term outcomes in stage II-III gastric cancer patients
- Tumor-infiltrating platelets predict postoperative recurrence and survival in resectable pancreatic neuroendocrine tumor
- Bacterobilia in pancreatic surgery-conclusions for perioperative antibiotic prophylaxis
- MiR-32-5p aggravates intestinal epithelial cell injury in pediatric enteritis induced by Helicobacter pylori
- Yinchenhao decoction attenuates obstructive jaundice-induced liver injury and hepatocyte apoptosis by suppressing protein kinase RNA-like endoplasmic reticulum kinase-induced pathway
- Therapeutic potential of menstrual blood stem cells in treating acute liver failure