Blood parameters score predicts long-term outcomes in stage II-III gastric cancer patients
2019-11-21JianXianLinYiHuiTangJiaBinWangJunLuQiYueChenLongLongCaoMiLinRuHongTuChangMingHuangPingLiChaoHuiZhengJianWeiXie
Jian-Xian Lin, Yi-Hui Tang, Jia-Bin Wang, Jun Lu, Qi-Yue Chen, Long-Long Cao, Mi Lin, Ru-Hong Tu,Chang-Ming Huang, Ping Li, Chao-Hui Zheng, Jian-Wei Xie
Abstract BACKGROUND Increasing numbers of laboratory blood parameters (BPM) have been reported to greatly affect the long-term outcomes of gastric cancer (GC) patients. However,the existing prognostic models do not comprehensively analyze these predictors.AIM To construct a new prognostic tool, based on all the prognostic BPM, to achieve more accurate prognosis prediction for GC.METHODS We retrospectively assessed 850 consecutive patients who underwent curative resection for stage II-III GC from January 2010 to April 2013. The patients were classified into developing (n = 567) and validation (n = 283) cohorts using computer-generated random numbers. A scoring system, namely BPM score, was then constructed using least absolute shrinkage and selection operator (LASSO)Cox regression model in the developing cohort, and validated in the validation cohort. A nomogram consisting of BPM score and tumor-lymph node-metastasis(TNM) stage was further created. The discrimination and calibration of the nomogram were evaluated via Harrell’s C-statistic and the Hosmer-Lemeshow test.RESULTS Using the LASSO model, we established the BPM score based on five BPM:Albumin, lymphocyte-to-monocyte ratio, neutrophil-to-lymphocyte ratio,carcinoembryonic antigen, and carbohydrate antigen 19-9. The BPM scores were divided into high- and low-BPM groups based on a cut-off value of -0.93. High-BPM patients were significantly older and had more advanced, larger tumors. In the developing cohort, significant differences were found in 5-year overall survival (OS) and 5-year disease-specific survival between the high-BPM and low-BPM patients. Similar results were found in the validation group.Multivariable analysis showed that the BPM score was an independent predictor of OS. High-BPM patients had a poorer 5-year OS for each subgroup.Furthermore, a nomogram that combined the BPM score and TNM stage had significantly better prognostic value compared with TNM stage alone.CONCLUSION The BPM score provides more accurate prognosis prediction in stage II-III GC patients and is an effective complement to the TNM staging system.
Key words: Blood parameters score; Gastric cancer; Long-term survival; Nomogram;Discrimination and calibration
INTRODUCTION
Gastric cancer (GC) remains an important malignancy worldwide; there were over 1000000 new cases of GC and an estimated 783000 deaths caused by GC (equating to 1 in every 12 deaths globally) in 2018, making it the fifth most frequently diagnosed cancer and the third leading cause of cancer death[1]. The tumor-lymph nodemetastasis (TNM) staging system is the most commonly used criteria to predict GC patients’ long-term outcomes[2]. However, clinical outcomes can vary in patients with GC who have the same TNM stage and similar treatment regimens[3-5], indicating that this anatomy-based system provides incomplete prognostic information. Hence, the identification of potential predictors of risk stratification and treatment selection has become a hot topic in recent years.
There is growing evidence that the patient’s immune and nutritional statuses are closely related to long-term survival in patients with various malignancies[5-14]. Over the past decades, the lymphocyte count and serum albumin have been the most widely used biomarkers for defining the immune and nutritional statuses. As a result,several scoring systems, including the prognostic nutritional index (PNI), the modified Glasgow prognostic score (mGPS), and the controlling nutritional status(CONUT) score, have been constructed and commonly used to predict the outcomes in patients with GC[9-11]. However, these scores contain limited blood parameters(BPM) and may provide inadequate prognostic information[11,15-16]. Ongoing work is seeking other prognostic biomarkers. To date, several ratios based on circulating blood cell counts, such as the neutrophil-to-lymphocyte ratio (NLR), lymphocyte-tomonocyte ratio (LMR), and platelet-to-lymphocyte ratio (PLR), have been developed to predict the outcome of GC[12-14]. In addition, tumor markers, including carcinoembryonic antigen (CEA) and carbohydrate antigen (CA) 19-9, are routinely applied in the early detection and postoperative follow-up of GC. Some studies have proved their prognostic value in GC[17-18]. Therefore, we hypothesized that a new scoring system, based on all available laboratory BPM, would provide more accurate prognostic information in patients with GC.
In the present study, we used the least absolute shrinkage and selection operator(LASSO) Cox regression model to select the optimal combination of BPM and to establish a novel prognostic classifier, namely, the BPM score, in order to predict outcomes in patients with stage II-III GC.
MATERIALS AND METHODS
Study population
We retrospectively assessed patients undergoing curative resection for GC at the Fujian Medical University Union Hospital (FMUUH) between January 2010 and April 2013. Patients who met the following criteria were included: (1) Aged ≥ 18 years; (2)Stage II-III gastric adenocarcinoma confirmed by histopathology; and (3) No preoperative chemoradiotherapy. The following patients were excluded: (1) Distant metastasis; (2) Malignant disease of other organs; (3) R1 resection; (4) Acute infections or other inflammatory conditions within 7 days before surgery; and (5) Incomplete medical records or follow-up data. Finally, 850 patients were enrolled in this study.All surviving patients had a follow-up period of at least 5 years. The patients were classified into developing (n= 567) and validation (n= 283) cohorts using computergenerated random numbers. All surgical procedures, including lymph node dissection, were performed according to the guidelines of the Japanese Research Society for the Study of GC[19], while staging was performed according to the TNM classification (AJCC, 8th edition). All patients were routinely recommend to receive 5-fluorouracil (5-FU) based adjuvant chemotherapy after surgery[4].
Data collection
Data on patient demographics and pathological results were obtained from a largescale prospective database. Routine blood tests were carried out during 1 wk before surgery, including hemoglobin, serum albumin, total cholesterol level, total peripheral neutrophils, lymphocyte count, monocyte count, platelet count, CEA, CA 19-9, and fibrinogen. LMR was calculated by dividing lymphocyte count by monocyte count. NLR was calculated by dividing neutrophil count by lymphocyte count. PLR was calculated by dividing platelet count by lymphocyte count. We used widely accepted thresholds to define the dichotomous forms of these BPM: hemoglobin(males 120 g/L; females 110 g/L), albumin (35 g/L), cholesterol (4.6 mmol/L or 180 mg/dL), CEA (5 ng/mL), CA 19-9 (37 U/mL), and fibrinogen (400 mg/dL)[8,17,21-22].According to the X-tile program (3.6.1 software 20, http://medicine.yale.edu/lab/rimm/research/software.aspx), NLR, LMR, and PLR cut-off values for overall survival (OS) were 3.9, 3.2, and 161, respectively[23]. The utility of clinical data was approved by the FMUUH Institutional Review Board.
Follow-up investigation
All patients were followed postoperatively by physical examination and laboratory tests (including CEA, CA 19-9, and CA 72-4), every 3 mo for 2 years, every 6 mo during years 2-5, and annually thereafter. In addition, examinations, including chest radiography, abdominal computed tomography, and endoscopy, were performed at least once per year. The follow-up period was completed in April 2018 or to the date of death of patients. OS was defined as the time interval from surgery to death from any cause or to the last follow-up. Disease-specific survival (DSS) was defined as the time interval from surgery to death from GC or to the follow-up.
Model development
As assays may vary between hospitals, all the BPM are expressed as ratio of lower limit of normal (including hemoglobin, albumin, and cholesterol), upper limit of normal (including fibrinogen, CEA, and CA 19-9), or cut-off values (including NLR,LMR, and PLR). The relation between the BPM (as continuous variables) and OS was investigated in univariate Cox models with restricted cubic splines (RCS)[24].Additional variable transformation was performed if strong nonlinear effects were shown. Next, we calculated the Akaike information criterion (AIC) scores of the continuous form and the dichotomous form of each blood parameter to determine the form in which the blood parameter was analyzed[25]. Finally, we used the LASSO Cox regression model to select the most useful predictors among the candidate BPM in the developing cohort[26,27]. A risk score based on multiple BPM, the BPM score, was then constructed to predict the prognosis of GC. Details of methods are described in the Supplementary Materials.
Statistical methods
Continuous variables were compared using the Student’st-test, and categorical variables were assessed using theχ2test or the Fisher exact test. The Kaplan-Meier method was used to analyze OS and DSS, and the differences were assessed by logrank tests. The time-dependent receiver operating characteristic (ROC) curve was generated to assess the discriminatory power of indicators for time-dependent disease outcomes[28]. Univariate and multivariate analyses were performed using the Cox proportional hazards model. A nomogram consisting of the BPM score and TNM stage was created to translate model parameter estimates into a visual scoring system to calculate the estimated survival probability. The discriminative power of the nomogram was assessedviaHarrell’s C-statistic[29]. The calibration of the nomogram was evaluated by the Hosmer-Lemeshow test to assess the goodness of fit[30]. Decision curve analysis was used to examine the usefulness and benefit of the nomogram[31].Two-tailedPvalues < 0.05 were considered statistically significant. All statistical analyses were conducted with SPSS software, version 18.0 (SPSS Inc., Chicago, IL,United States) and R software, version 3.1.2 (R Foundation for Statistical Computing,Vienna, Austria).
RESULTS
Patient characteristics
Overall, 850 patients were included in the study. There were 656 (77.2%) males and 194 (22.8%) females. The median age at the time of surgery was 62 years (range, 20-91 years). According to the TNM classification, 285 (33.5%) were classified as having stage II and 565 (66.5%) as having stage III, respectively. The majority of the patients(n= 645, 75.8%) received adjuvant chemotherapy. The median follow-up time was 61 mo (range, 1-102 mo). Patient characteristics in the developing and validation cohorts are detailed in Table 1.
Derivation of the BPM score
It was observed that the relationship between total cholesterol level and OS followed a U-shaped pattern, with a turning point approximately 1.5 × LLN. Therefore, the values for this variable were transformed by taking the absolute distance between cholesterol (in unit × LLN) and the turning point. Similarly, CEA and CA 19-9 were transformed to the form of ln CEA and ln CA 19-9. After transforming, no strong nonlinear effect was observed in all BPM (Supplementary Figure 1). Then, we calculated AIC scores and Harrell’s C-statistics of 9 BPM as continuous variables(Supplementary Table 1) and as dichotomous variables. It was found that only hemoglobin, albumin, ln CEA, and fibrinogen had smaller AIC scores as well as significantly higher Harrell’s C-statistics in their continuous forms(Supplementary Table 2). So, they were further analyzed as continuous variables, with the others analyzed as dichotomous variables.
Using LASSO Cox regression analysis, we identified five out of the nine BPM in the developing cohort: Albumin, LMR, NLR, CEA, and CA 19-9, and derived a formula to calculate the BPM score for each patient: BPM = -0.86259331 × Albumin (× LLN) +0.08074780 × Low_LMR + 0.06002645 × High_NLR + 0.05939068 × High_CA19-9 +0.04007563 × ln CEA (× ULN) (Figure 1A and B).
In this formula, LMR, NLR, and CA 19-9 were valued as 0 or 1; LMR ≤ 3.2, NLR ≥3.9, and CA 19-9 ≥ 37 U/mL were assigned a score of 1, and a value of 0 otherwise.The optimum cutoff value for BPM score was selected on the basis of the association with the patients’ OS by using X-tile plots (-0.93). We then assigned patients to a high-(BPM score ≥ -0.93) or low-BPM (BPM score < -0.93) group by this value.
Correlations between clinicopathological findings and BPM score
Table 1 shows the relationship between clinicopathological factors and the BPM score.In both the developing and validation cohorts, high-BPM status was related to older age (P< 0.001 for both), higher tumor stage (P< 0.001 andP= 0.004, respectively),and larger tumor size (P< 0.001 andP= 0.014, respectively), compared with low-BPM status. In addition, although the high-BPM patients had a smaller body mass index(BMI) (P= 0.038) than the low-BPM patients in the developing cohort, it did not reach statistical significance in the validation cohort (P= 0.285).
Prognostic value of BPM score
In the developing cohort, the 5-year OS rates in the low-BPM and high-BPM groups were 70.0% and 41.6%, and the 5-year DSS rates were 72.4% and 46.4% (log-rankP<0.001, Figure 2A). We performed the same analyses in the validation cohort. The 5-year OS rates in the low-BPM and high-BPM groups were 67.3% and 39.7%, and the 5-year DSS rates were 70.1% and 41.9% (log-rankP< 0.001, Figure 2B). In the multivariate analysis, BPM score remained an independent prognostic factor for OS (P< 0.001 andP= 0.004, respectively) in both the developing and validation cohorts(Table 2).
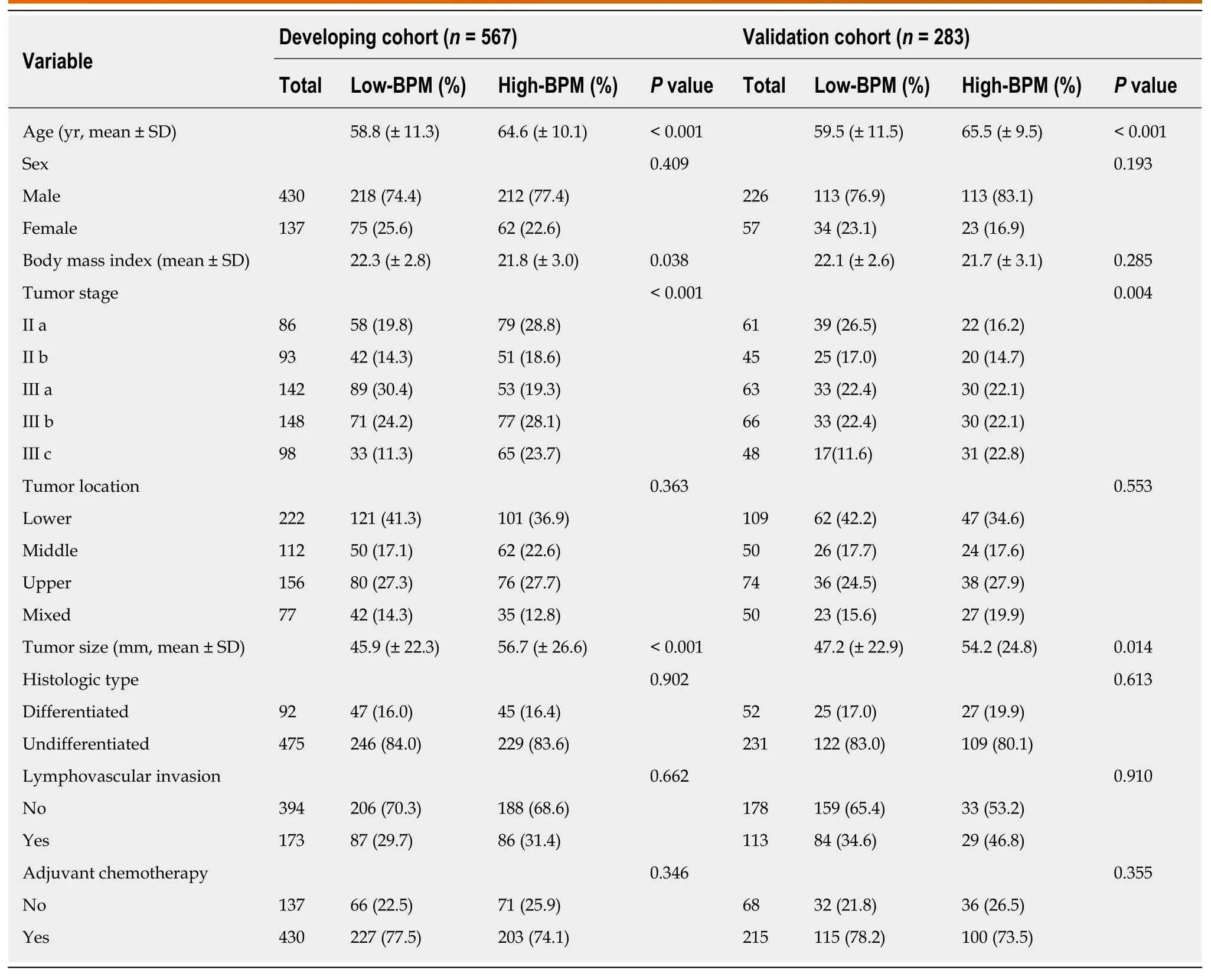
Table 1 Clinicopathological characteristics of patients according to the blood parameters score in the developing and validation cohorts
To confirm whether the BPM score has more benefits than using only one marker,we compared their areas under the curves (AUC) using ROC analysis in the entire cohort. The BPM score exhibited a higher prognostic accuracy (0.680) than each individual marker, including albumin (0.640,P< 0.001), LMR (0.580,P< 0.001), NLR(0.546,P< 0.001), CEA (0.578, P < 0.001), and CA 19-9 (0.565,P< 0.001). Furthermore,the time-dependent ROC curves calculated at different time points for BPM score (as a dichotomous variable) and other scoring systems [including PNI, CONUT score, and modified systemic inflammation score (mSIS)[32]] clearly showed that the BPM score was continuously superior to the other scoring systems at each time point (Figure 2C).
Next, we used multivariate Cox models by means of RCS to further analyze the relationship between BPM score and OS with adjustment for the clinicopathologic factors (including age, BMI, tumor stage, tumor size, lymphovascular invasion, and adjuvant chemotherapy, which reached statistical significance in the univariate analysis). A continuous linear association between BPM score and OS was observed in the analysis of the developing, validation, and entire cohorts (Supplementary Figure 2).
BPM score has stable prognostic value in different subgroups of patients
We performed stratified analyses of GC patients in the entire cohort. High-BPM patients with stages IIa, IIb, IIIa, IIIb, and IIIc disease had a shorter OS and DSS compared with low-BPM patients (log-rankP< 0.05 for all, Figure 3). A forest plot based on 5-year OS was further established, and the results confirmed that high-BPM patients had a poor prognosis among each subgroup (Figure 4). Furthermore, we assigned patients to an adjuvant chemotherapy (AC) or a non-AC group based on the receipt of postoperative adjuvant chemotherapy and then performed the Kaplan-Meier survival analysis. The results revealed that high-BPM patients had a poorer prognosis compared with low-BPM patients in both the AC and non-AC groups (logrankP< 0.001 for all, Supplementary Figure 3).
Prognostic value of TNM + BPM
To make individualized prediction of the survival probability in stages II and III GC patients, we established a nomogram that combined the BPM score and TNM stage in the entire cohort (Figure 5A). The Harrell’s C-statistic of this nomogram was significantly higher than that of TNM stage alone (0.727vs0.697,P< 0.001). The Hosmer-Lemeshow test showed that the model had good fit for 1-, 3-, and 5-year OS(P= 0.979,P= 0.853, andP= 0.655, respectively). The decision curve analysis revealed that TNM + BPM had better clinical utility than TNM stage alone at 1, 3, and 5 years(Figure 5B-D).
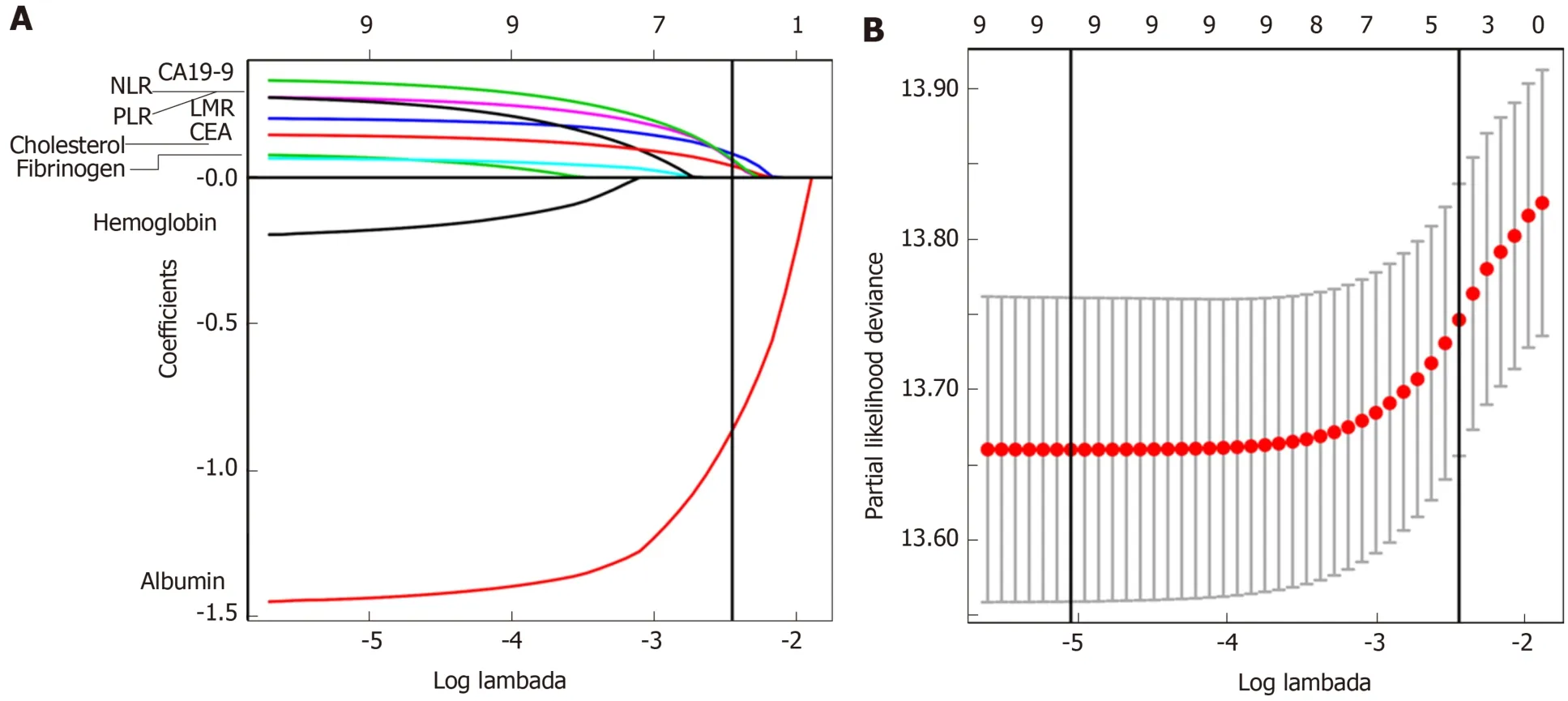
Figure 1 Construction of the blood parameters score, a classifier comprising five blood parameters. A: Least absolute shrinkage and selection operator(LASSO) coefficient profiles of the nine blood parameters. The vertical line indicates the value chosen by 10-fold cross-validation; B: Ten-fold cross-validation for tuning parameter selection in the LASSO Cox model. Solid vertical lines represent partial likelihood deviance ± standard error. We plotted the partial likelihood deviance vs log (λ), where λ is the tuning parameter. The vertical lines are drawn at the optimal values by minimum criteria and 1 - S.E. criteria.
DISCUSSION
A growing body of evidence has demonstrated the potential of some laboratory BPM as prognostic markers to predict the oncologic outcomes in human malignancies[5-14,17-18,21-22]. However, how to comprehensively use these predictors to predict the long-term prognosis of patients with GC remains unclear. So far, researchers have established PNI, mGPS, CONUT, and mSIS as scoring systems that reflect immunological and nutritional statuses to more accurately predict clinical outcomes and to administer individualized treatment[9-11,32]. However, the clinical usefulness of these scoring systems is still controversial. Liuet al[15]found that low PNI was marginally associated with 5-year OS in patients with stage III GC, but the prognostic value was not significant in stages I and II GC. A retrospective study of 416 patients reported that a high CONUT score was strongly associated with 5-year OS in both pStage I and pStage II patients but not in pStage III patients[11]. Similarly, previous studies showed that the utility of mGPS and mSIS in patients with GC was also controversial[16,32]. A possible explanation was that these scores did not include all valuable BPM for comprehensive analysis, resulting in their limited prognostic value.
In addition, in the pursuit of simplicity, some of the current scoring systems handle the BPM in a categorical manner when they are, in fact, generated as continuous variables. It was reported that dichotomisation of continuous variables in a multiple regression procedure may be associated with considerable loss of statistical power and introduction of bias[33,34]. However, we should acknowledge that considering an
indicator as a continuous variable does not necessarily improve the prediction accuracy. At the same time, it may not be easy to use in the clinical decision-making process[35]. Therefore, in the present study, we separately calculated and compared the AIC score and Harrell’s C-statistic of each blood parameter in the dichotomous and continuous forms to determine which form was better for this indicator. It was found that only the continuous form of hemoglobin, albumin, fibrinogen, and CEA had smaller AIC scores than their dichotomous form, with significantly stronger discriminative power. So, we further analyzed them as continuous variables, while the remaining indicators (including cholesterol, LMR, NLR, PLR, and CA 19-9) were valued as 0 or 1 according to their cut-off values.
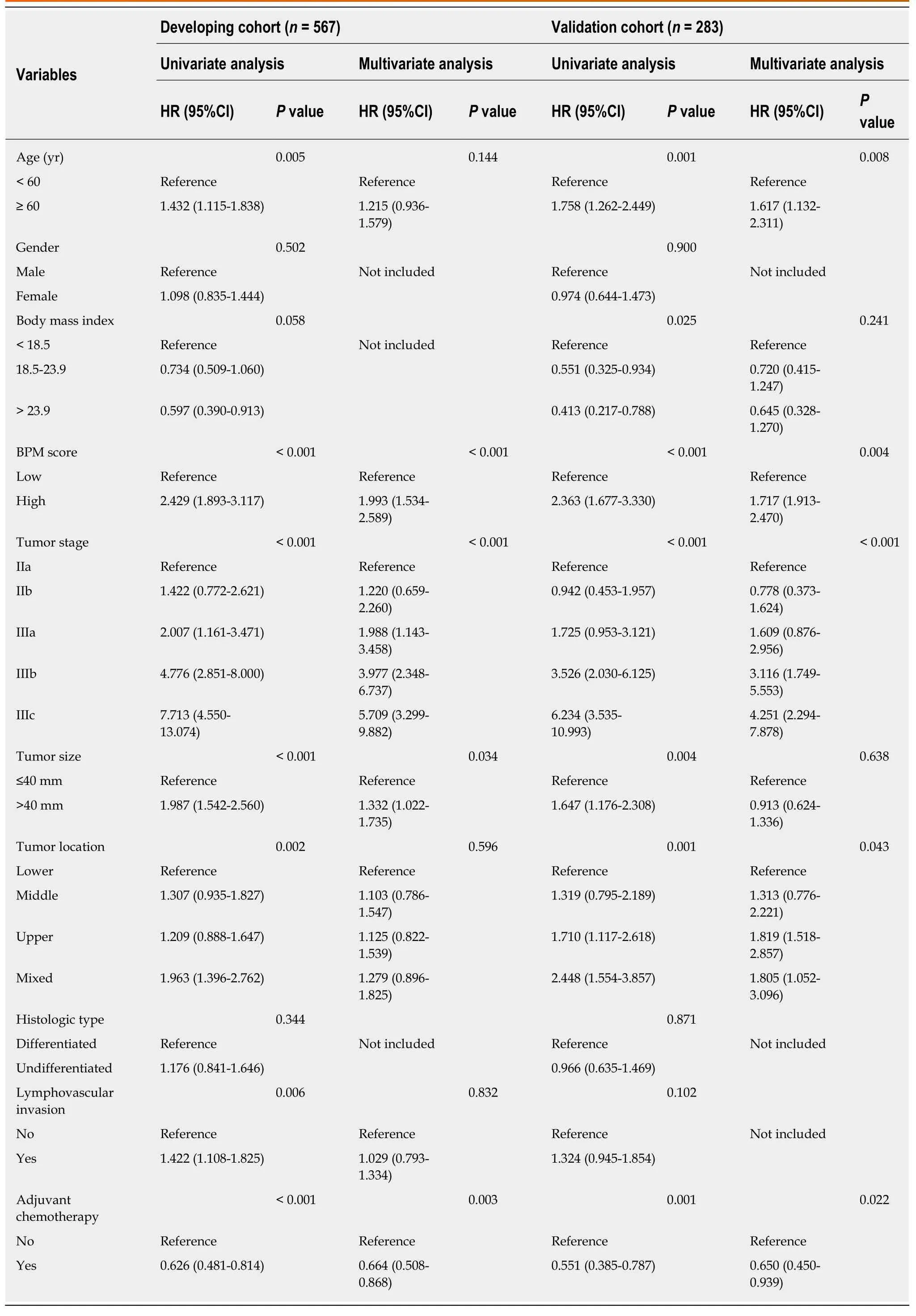
Table 2 Univariate and multivariate analyses for overall survival in the developing and validation cohorts
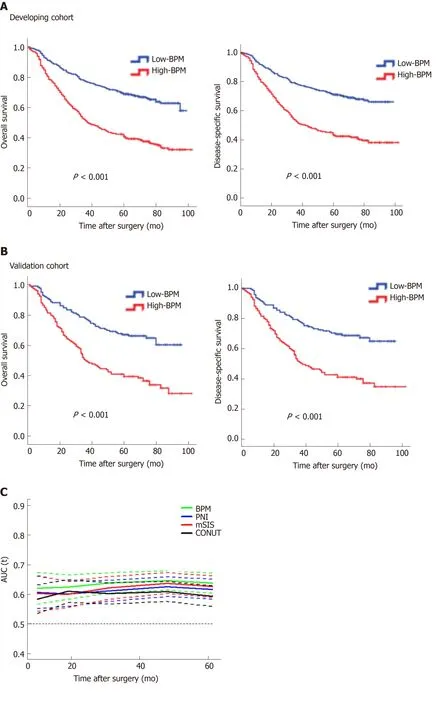
Figure 2 Survival impact of the blood parameters score measured by Kaplan-Meier survival. A: Survival impact of the blood parameters (BPM) score measured by Kaplan-Meier survival in the developing cohort; B: Survival impact of the BPM score measured by Kaplan-Meier survival in the validation cohort. We calculated P values using the log-rank test; C: Time-dependent receiver operating characteristic curves of BPM score, prognostic nutritional index (PNI), controlling nutritional status (CONUT), and modified systemic inflammation score (mSIS) for the prediction of overall survival. PNI indicates prognostic nutritional index calculated as follows: 10 × serum albumin (g/L) + 0.005 × lymphocyte count (/mm3). CONUT indicates controlling nutritional status, a scoring system calculated by summing the value of serum albumin, total cholesterol, and total lymphocyte count. mSIS indicates modified systemic inflammation score developed based on serum albumin and lymphocyte-monocyte ratio. PNI: Prognostic nutritional index; CONUT: Controlling nutritional status; mSIS: Modified systemic inflammation score; BPM: Blood parameters.

The prognostic influence of perioperative laboratory BPM may be difficult to discern in patients with stage I GC, who experience fewer cases of DSS, and in patients with stage IV GC, who experience extremely lower survival rates[5].Therefore, the present study enrolled stage II-III GC patients based on a prospectively collected database of a high-volume center in order to provide a novel prognostic model for these patients with resectable locally advanced GC. Using LASSO Cox regression analysis, we established the BPM score based on five objectively measured,easily obtained BPM covering inflammatory, nutritional, and tumor markers:Albumin, LMR, NLR, CEA, and CA 19-9. To our knowledge, the link of malnutrition and systemic inflammation with carcinogenesis, tumor growth, and cancer progression has been demonstrated in several cancers, including GC[5-16,36-39]. In addition, tumor markers, as circulating substances that can be measured quantitatively, have a causal relationship with malignant diseases and are currently applied in prognosis prediction of GC patients[17,18,40]. A comparison of the clinicopathological variables between high-BPM and low-BPM patients revealed that a high BPM score was associated with older age, higher tumor stage, and larger tumor size. Multivariate analysis showed that the BPM score was an independent risk factor,had a stable prognostic ability among patients in each subgroup, and had better predictive accuracy than the traditional scoring systems. More importantly, the BPM score proved to be a supplement to the TNM staging system. Therefore, we recommend the use of the TNM + BPM scoring system incorporating preoperative albumin, LMR, NLR, CEA, and CA 19-9 levels for multimodality treatment planning and risk stratification in prospective studies.
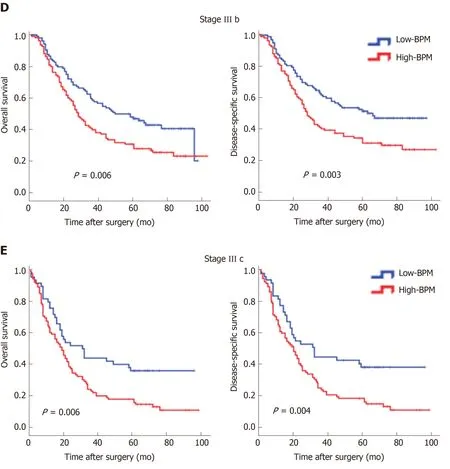
Figure 3 Kaplan-Meier curves for overall survival and disease-specific survival in the high-blood parameters or low-blood parameters groups for different stages. A: Stage IIa; B: Stage IIb; C: Stage IIIa; D: Stage IIIb; E: Stage IIIc. BPM: Blood parameters.
In this study, we found that the BPM score, a novel scoring system based on five BPM, was predictive of long-term outcomes in stage II-III GC patients. This tool may have important uses in prognostic stratification, therapeutic intervention, and postoperative surveillance strategies, especially after incorporating TNM stage. For example, patients with a high BPM score will be recommended to receive postoperative multimodality treatment, such as chemotherapy, immunotherapy, and targeted therapy. And more regular follow-up schedule will be offered to early detect recurrence, which may provide survival benefit[41]. A patient example of how the model can be used in clinical practice is provided in the Supplementary Materials.
This study has some limitations. First, as a retrospective, single-institution study, it may have been subject to selection bias. However, all data were derived from a prospectively collected database of a high-volume center, which can reduce this bias.Second, because C-reactive protein and prealbumin were not routinely tested before surgery in our institution, we did not include these potentially valuable biomarkers.Third, the validity and generalizability of the BPM score need to be established by testing it in other locations and groups of patients[42].
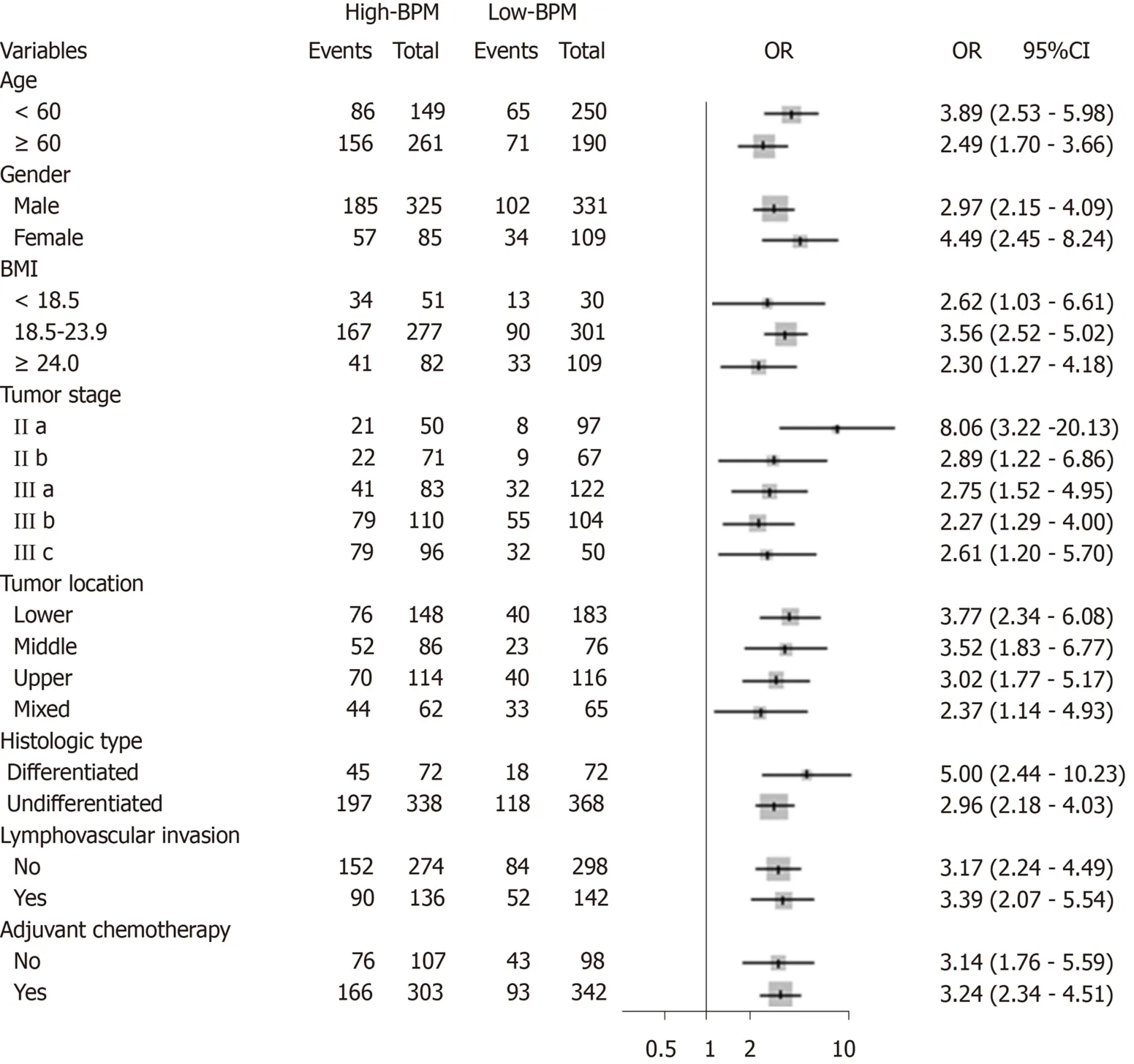
Figure 4 Forest plot showing the impact of blood parameters score on 5-year overall survival stratified by different clinicopathological factors. Odds ratios with 95% confidence intervals are shown for the high-blood parameters (BPM) group vs low-BPM group. CI: Confidence interval; OR: Odds ratios; BMI: Body mass index; BPM: Blood parameters.
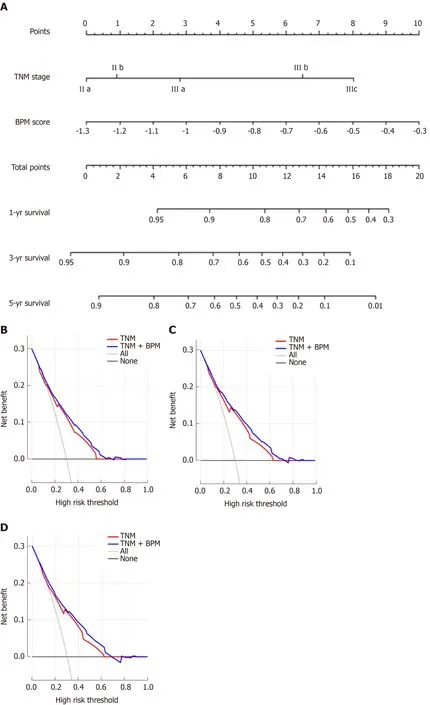
Figure 5 Prediction and analysis of 1-, 3-, and 5-year overall survival in patients. A: A nomogram combining blood parameters score and tumor-lymph nodemetastasis stage for predicting 1-, 3-, and 5-year overall survival (OS) in patients with stage II-III gastric cancer; B: Decision curve analysis of the nomogram for 1-year OS; C: Decision curve analysis of the nomogram for 3-year OS; D: Decision curve analysis of the nomogram for 5-year OS. TNM: Tumor-lymph node-metastasis;BPM: Blood parameters.
ARTICLE HIGHLIGHTS
Research background
Increasing numbers of laboratory blood parameters (BPM) have been reported to greatly affect the long-term outcomes of gastric cancer (GC) patients. However, the existing prognostic models, including the prognostic nutritional index, the modified Glasgow prognostic score, and the controlling nutritional status score, contain limited BPM and provide inadequate prognostic information.
Research motivation
We hypothesized that a new scoring system, based on all available BPM, would provide more accurate prognostic information in patients with GC.
Research objectives
The present study aimed to construct a new prognostic tool, based on all the prognostic BPM, to achieve more accurate prognosis prediction for GC.
Research methods
We retrospectively assessed 850 consecutive patients who underwent curative resection for stage II-III GC from January 2010 to April 2013. The patients were classified into developing (n= 567)and validation (n= 283) cohorts using computer-generated random numbers. A scoring system,namely BPM score, was then constructed using the least absolute shrinkage and selection operator (LASSO) Cox regression model. A nomogram consisting of the BPM score and tumorlymph node-metastasis (TNM) stage was created. The discrimination and calibration of the nomogram were evaluatedviaHarrell’s C-statistic and the Hosmer-Lemeshow test.
Research results
Using the LASSO model, we established the BPM score based on five BPM: Albumin,lymphocyte-to-monocyte ratio, neutrophil-to-lymphocyte ratio, carcinoembryonic antigen, and carbohydrate antigen 19-9. The BPM scores were divided into high-BPM and low-BPM groups based on a cut-off value of -0.93. High-BPM patients were significantly older and had more advanced, larger tumors. In the developing cohort, significant differences were found in 5-year overall survival (OS) and 5-year disease-specific survival between the high-BPM and low-BPM patients. Similar results were found in the validation group. Multivariable analysis showed that the BPM score was an independent predictor of OS. High-BPM patients had a poorer 5-year OS for each subgroup. Furthermore, a nomogram that combined the BPM score and TNM stage had significantly better prognostic value compared with TNM stage alone.
Research conclusions
The BPM score provides more accurate prognosis prediction in stage II-III GC patients and is an effective complement to the TNM staging system. Therefore, we recommend the use of the BPM score for multimodality treatment planning and risk stratification in the future clinical work.
Research perspectives
Although we confirmed that the BPM score can accurately predict the outcomes in stage II-III GC patients, the efficiency of this novel scoring system need to be investigated in a prospective multicenter trial.
杂志排行
World Journal of Gastroenterology的其它文章
- lncreased circulating circular RNA_103516 is a novel biomarker for inflammatory bowel disease in adult patients
- Tumor-infiltrating platelets predict postoperative recurrence and survival in resectable pancreatic neuroendocrine tumor
- Bacterobilia in pancreatic surgery-conclusions for perioperative antibiotic prophylaxis
- MiR-32-5p aggravates intestinal epithelial cell injury in pediatric enteritis induced by Helicobacter pylori
- Yinchenhao decoction attenuates obstructive jaundice-induced liver injury and hepatocyte apoptosis by suppressing protein kinase RNA-like endoplasmic reticulum kinase-induced pathway
- Therapeutic potential of menstrual blood stem cells in treating acute liver failure