Allicin as add-on therapy for Helicobacter pylori infection: A systematic review and meta-analysis
2019-10-30XiaoBeiSiXuMinZhangShuaiWangYuLanShuoZhangLinYuHuo
Xiao-Bei Si, Xu-Min Zhang, Shuai Wang, Yu Lan, Shuo Zhang, Lin-Yu Huo
Abstract BACKGROUND Allicin (2-propene-1-sulfinothioic acid S-2-propenyl ester, diallyl thiosulfinate)extracted from garlic, has proven activity against Helicobacter pylori (H. Pylori)infection. In recent years, clinical trials have explored its utility as an add-on therapy with variable outcomes reported.AIM To perform a systemic review of allicin as an add-on treatment for H. Pylori infection and assess its efficacy in randomized controlled trials (RCTs).METHODS Electronic databases including MEDLINE, EMBASE, the Web of Science, the Cochrane Database, the China National Knowledge Infrastructure Database,Chinese VIP Information Databases, Chinese Medical Databases, and the Wan-Fang Database were searched for keywords including “allicin”, “Helicobacter pylori”, “randomized clinical trials”, and their synonyms. A meta-analysis was performed using the fixed-effects model for low heterogeneity and the randomeffects model for high heterogeneity with sensitivity analysis. Bias was evaluated using Egger’s tests. Trial sequential analysis (TSA) was used to evaluate information size and treatment benefits. The Grading of Recommendations Assessment, Development and Evaluation (GRADE) was used to assess the level of quality, and studies were classed as “high quality”, “moderate quality”, “low quality”, and “very low quality”.RESULTS A total of eight RCTs consisting of 867 participants (435 from the allicin group and 432 from the control group) were included. Eradication rate in the allicin group (93.33%, 406/435) was significantly higher than that of the control group(83.56%, 361/432) [I2 = 0%, odds ratio (OR) = 2.75, 95% confidence interval (CI):1.74-4.35, P < 0.001]. The healing rate of ulcers following H. pylori therapy in the allicin group (86.17%, 349/405) was significantly higher than that of the control group (75.87%, 305/402) [I2 = 0%, OR = 2.05, 95%CI: 1.39-3.03, P < 0.001]. The total remission rate of peptic ulcers across all allicin groups was 97.16%, which was significantly higher than that of controls [96.05% (389/405) vs 86.55%(360/402), I2 = 0, OR = 3.04, 95%CI: 1.51-6.12, P = 0.015]. No significant differences in side effects were observed. TSA suggested that the trials were of sufficient standard to draw reliable conclusions. The quality of outcomes including eradication rates and side effects was graded as “very low” due to downgrades for “risk of bias” and “indirectness”. Other outcomes such as ulcer healing rates and total ulcer remission rates were graded as "low" due to downgrades for “risk of bias”.CONCLUSION Allicin as an add-on therapy improves H. pylori eradication, healing of ulcers, and remission of symptoms. These results are suggested to be treated with caution due to limited quality.
Key words: Allicin; Helicobacter pylori; Randomized controlled trials; Add-on therapy;Systematic review; Meta-analysis
INTRODUCTION
Helicobacter pylori (H. pylori)is a Gram-negative microaerophilic bacterium that colonizes the gastric mucosa[1]. Globally, ≥ 50% of individuals are infected, and the prevalence is higher in developing countries[2]. H. pylori is a major cause of gastritis and peptic ulcers, as well as atrophy, intestinal metaplasia, intraepithelial neoplasia,and mucosa-associated lymphoid tissue lymphoma (MALT)[1,2].
Proton pump inhibitors (PPIs) in combination with antibiotics have been used to treat H. pylori infection. PPI triple therapy (PTT), consisting of PPI and two antibiotics such as amoxicillin and clarithromycin, is the recommended front-line treatment[2]but its eradication rates have decreased to ~70% or lower[2]. Antibiotic resistance,particularly towards clarithromycin and metronidazole, is the major cause of this decline[3]. Bismuth containing quadruple therapy (BCQT) is now recommended as the main empirical therapy in regions with high clarithromycin and metronidazole resistance (> 15%)[1]. However, eradication rates using BCQT range from 70% to 94%,questioning its effectiveness as a therapeutic strategy[1,2,4]. Therefore, new strategies to treat H. pylori infection are needed.
Choosing new alternatives with high efficiency and less side effects is one of the possible desirable options in the treatment of H. pylori infection[5]. In recent years, a series of studies were performed to explore the anti-H. pylori activities and clinical application of various agents as alternative therapies, such as plants[6,7], probiotics[8],and gastric mucin[9]. However, most of them were done in vitro[5]. In vivo studies as well as clinical trials are needed.
Garlic (Allium sativum L.) is one of the most widely grown vegetable crops in Asia,and is a known medical plant worldwide. Garlic contains 33 sulfur compounds including allicin, alliin, ajoene, diallyl trisulfide (DATS) and others[10]. Previous in vitro studies have shown that garlic inhibits bacterial growth and colonization including H.pylori[11]. Several clinical trials using garlic oil and fresh oral garlic failed to show improvements in H. pylori infection[12,13].
Allicin (2-propene-1-sulfinothioic acid S-2-propenyl ester, diallyl thiosulfinate) is an active anti-H. pylori component of garlic[11]. Due to developments in pharmaceutical technology, commercial allicin tablets are available. Allicin in addition to PTT and BCQT has been trialed as an anti-H. pylori therapy, with variable results[14-23]. Based on these studies, we performed this meta-analysis to systemically review the efficacy and safety of allicin as an add-on therapy to PTT/BCQT for H. pylori infection.
MATERIALS AND METHODS
Protocol
Preplanned protocols were established with protocols.io (https:// www.protocols.io)under the title “Allicin as a Complementary Medicine of Triple/Quadruple Therapy for Helicobacter pylori; A Systemic review and Meta-analysis of Randomized Controlled Trials (protocol)”. (https://dx.doi.org/10.17504/protocols.io.4ybgxsn)
Information sources and search strategy
We performed a systemic literature search in MEDLINE, EMBASE, the Web of Science, the Cochrane Database, the China National Knowledge Infrastructure Database, Chinese VIP Information Databases, Chinese Medical Databases, and the Wan-Fang Database from inception to June 1, 2019. Academic journals, dissertations,and conference proceedings were included irrespective of gray literature status. The search terms included “Helicobacter pylori”, “allicin”, “randomized clinical trials”, and their synonyms. The search strategy is listed in Appendix 1, with PubMed as an example. Reference lists were searched for potentially relevant titles. Literature searches and analysis were preplanned prior to the systemic review.
Inclusion and exclusion criteria
The following criteria were used for literature selection: (1) The subjects enrolled were adults with H. pylori infection with/without H. pylori-related disease including gastritis and ulcers. The diagnosis of H. pylori infection was based on positive histology, rapid urease tests (RUT), or urease breath tests (UBT); (2) Subjects in the treatment group underwent interventions using allicin plus PTT or BCQT. The control group received PTT/BCQT alone; (3) PTT/BCQT regimens in both groups were identified; (4) The main outcome was the eradication rate. Secondary outcomes were side effects, the relief of digestive symptoms, and ulcer healing (healing rate and total effectiveness rate); and (5) The study design consisted of randomized controlled trials(RCTs).
Studies that met the following criteria were excluded: (1) Duplicate articles or evaluation of the same samples; (2) Articles published as reviews, meta-analysis, or protocols; (8) Studies recruiting children; and (9) In vitro studies.
Study selection and data collection
All retrieved trials were independently screened by two reviewers (Xiao-Bei Si and Shuo Zhang). Titles and abstracts were screened for all relevant articles. Full texts were screened for further assessments according to the inclusion and exclusion criteria. Disagreements were resolved by discussion or through consultation with a second specialist.
Two reviewers (Xiao-Bei Si and Shuai Wang) independently extracted data from the included RCTs. Authors, publication year, sample size, interventions, eradication rate, and secondary outcomes (remission of digestive symptoms, healing rate of peptic ulcers, and side effects) were included. Eradication rate was defined as H. pylori negativity following eradication therapy[1]. Peptic ulcers were classed as healed,effective, or ineffective following endoscopic examination before and after eradication therapy. The healing of peptic ulcers was defined as the disappearance of ulcer lesions and surrounding inflammation. Effectiveness was defined as a reduction in ulcer lesions to ≤ 50% of the original size, whilst non-effectiveness was deemed as ≥ 50% of the lesion remaining. Healing rate was defined as the number of cured cases divided by the total number of cases. Total effectiveness rate was defined as the percentage of patients whose peptic ulcers were classed as healing and/or effectiveness [Total effectiveness rate = (total number - non-effectiveness number)/total number ×100%][24]. The remission of abdominal pain was defined as a disappearance of abdominal pain after treatment. Disappearing abdominal pain was defined as the time from the initiation of H. pylori treatment to the disappearance of abdominal pain.Side effect rate was defined as the percentage of patients with at least one side effect[24].
Risk of bias assessment
We evaluated the risk of bias of the included articles using the Cochrane handbook[25].Methodological quality was assessed with regard to random sequence generation,allocation concealment, the blinding of participants and personnel, the blinding of outcome assessments, incomplete outcome data, selective reporting, and other bias.Risks of bias were categorized as “low”, “high”, or “unclear”.
Statistical analysis
Meta-analysis was performed using Comprehensive Meta-analysis software (version 2.2.064; Biostat Inc, Englewood, United States). Sensitivity analysis was performed depending on the heterogeneity across the included studies. Statistical heterogeneity was assessed by I2statistics. The Chi-square test P < 0.10 or I2values ≥ 50% indicated heterogeneity. Trials showing either clinical heterogeneity or statistical heterogeneity were combined according to the random-effects model. The fixed-effects model was otherwise used. Publication bias was analyzed using an Egger's test. Funnel plots were performed if >10 studies were included.
Trial sequential analysis (TSA)
TSA was used to evaluate treatment benefits based on the sample sizes using TSA software (version 0.9.5.10 Beta; Copenhagen Trial Unit, Copenhagen, Denmark) with α = 5% and 1-β = 80%. The anticipated relative risk reduction was based on the pooled estimate of available trials. Boundaries were monitored to confirm the early termination of the trials when P-values were sufficiently small enough to confirm the anticipated effects. The chance of random errors increased due to insufficient comparisons and the repetitive testing of pooled data. When cumulative Z-curves crossed sequential monitoring boundaries, a sufficient level of evidence is obtained for the intervention. When Z-curves did not cross the boundaries, the conclusions for the intervention were not justified[26].
Evidence quality evaluation
The quality of the meta-analysis was evaluated using The Grading of Recommendations Assessment, Development and Evaluation (GRADE). As per GRADE criteria, certainty was rated as downwards to include risk of bias,inconsistency, indirectness, imprecision, and publication bias. Certainty was increased through large effects, dose-response relationships, and the adjustment of all plausible residual confounding effects. Evidence was summarized into four categories: “High quality”, “moderate quality”, “low quality”, and “very low quality”[27].
RESUTLS
Literature analysis and quality assessment
We identified 211 records using our established search strategy. Of these, 82 were excluded as duplicated records, 114 were non-clinical trials, 14 were unrelated articles, and one trial was excluded due to allicin plus non-PTT/BCQT regimens. In total, 10 clinical trials were retrieved for further full text screening. One trial[14]was excluded as the participants underwent non-standard triple therapy of amoxicillinbismuth-PPI. A single trial[23]was excluded as the triple therapies in the allicin and control groups differed. Thus, a total of eight RCTs with 867 participants (435 from the allicin group and 432 from the control group) were finally included. The sample population of each RCT ranged from 60 to 220. A flow chart of article screening and selection processes is shown in Figure 1. One study was performed in Turkey whilst the rest were performed in China. The characteristics of each included study are summarized in Table 1.
We used the Cochrane handbook tool to assess the quality of the included studies.No studies reported methods of randomization or concealment, despite claims of“randomized trials”. No studies implemented blindness, and one study[22]reported incomplete outcome data. No studies reported the existence of reporting bias. Table 2 shows the results of quality assessments. No included studies registered published protocols. An Egger’s test showed no publication bias (Intercept: -1.21506, P = 0.25).Funnel plots were not performed due to the insufficient study number (n < 10).
Eradication rates
We compared the eradication rates of H. pylori between allicin and control groups.
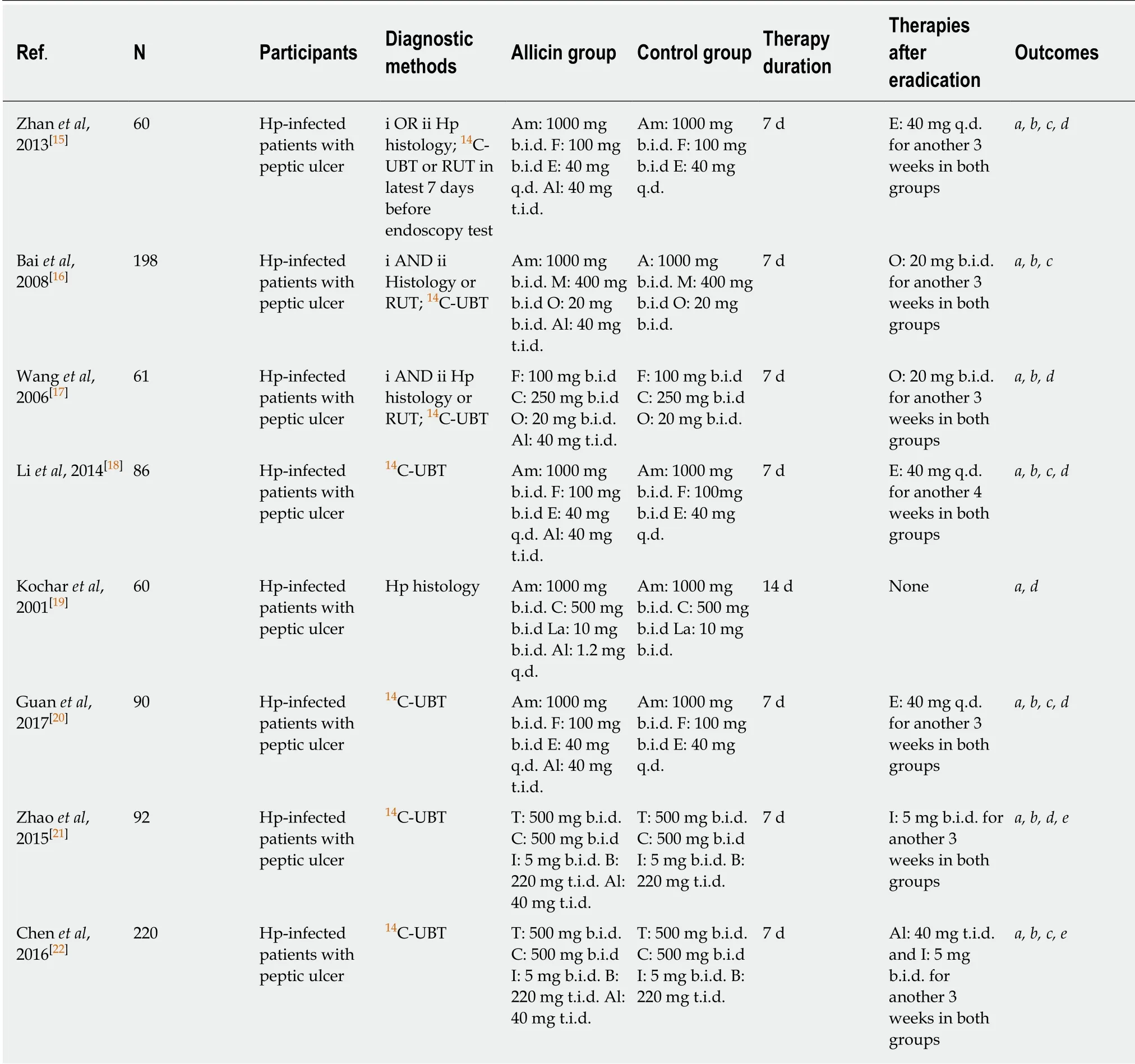
Table 1 Summary of included studies
The eradication rates of the allicin group (93.33%, 406/435) were significantly higher than those of the control group (83.56%, 361/432) for intent-to-treat (ITT) analysis [I2=0%, heterogeneity P = 0.993, odds ratio (OR) = 2.75, 95% confidence interval (CI): 1.74-4.35, P < 0.001] (Figure 2) and per-protocol (PP) analysis [93.55% (406/434) vs 83.76%(361/431), I2= 0%, heterogeneity P = 0.996, OR = 2.81, 95%CI: 1.77-4.47, P < 0.001][15-22].
Six studies[15-20]compared allicin plus PTT vs PTT alone. The eradication rates of the allicin group were significantly higher than those of the control group for both ITT analysis [92.47% (258/279) vs 82.61% (228/276), I2= 0%, OR = 2.87, 95%CI: 1.65-4.99, P< 0.001] and PP analysis [92.81% (258/278) vs 82.91% (228/275), I2= 0%, OR = 2.66,95%CI: 1.53-4.64, P = 0.001]. A further two studies[21,22]compared allicin combined with PPI-bismuth-tinidazole-clarithromycin therapy vs PPI-bismuth-tinidazoleclarithromycin therapy. The eradication rates in the allicin and control groups were 94.87% (148/156) and 85.25% (133/156), respectively, which significantly differed for ITT/PP analyses [I2= 0%, OR = 3.19, 95%CI: 1.38-7.38, P = 0.007]. Three studies[15,18,20]compared 7-day PPI-amoxicillin-furazolidone therapy with or without allicin and reported eradication rates of 92.46% (135/146) and 81.33% (122/150), respectively, for ITT/PP analyses [I2= 0%, OR = 2.38, 95%CI: 0.99-5.71, P = 0.053] (Table 3).
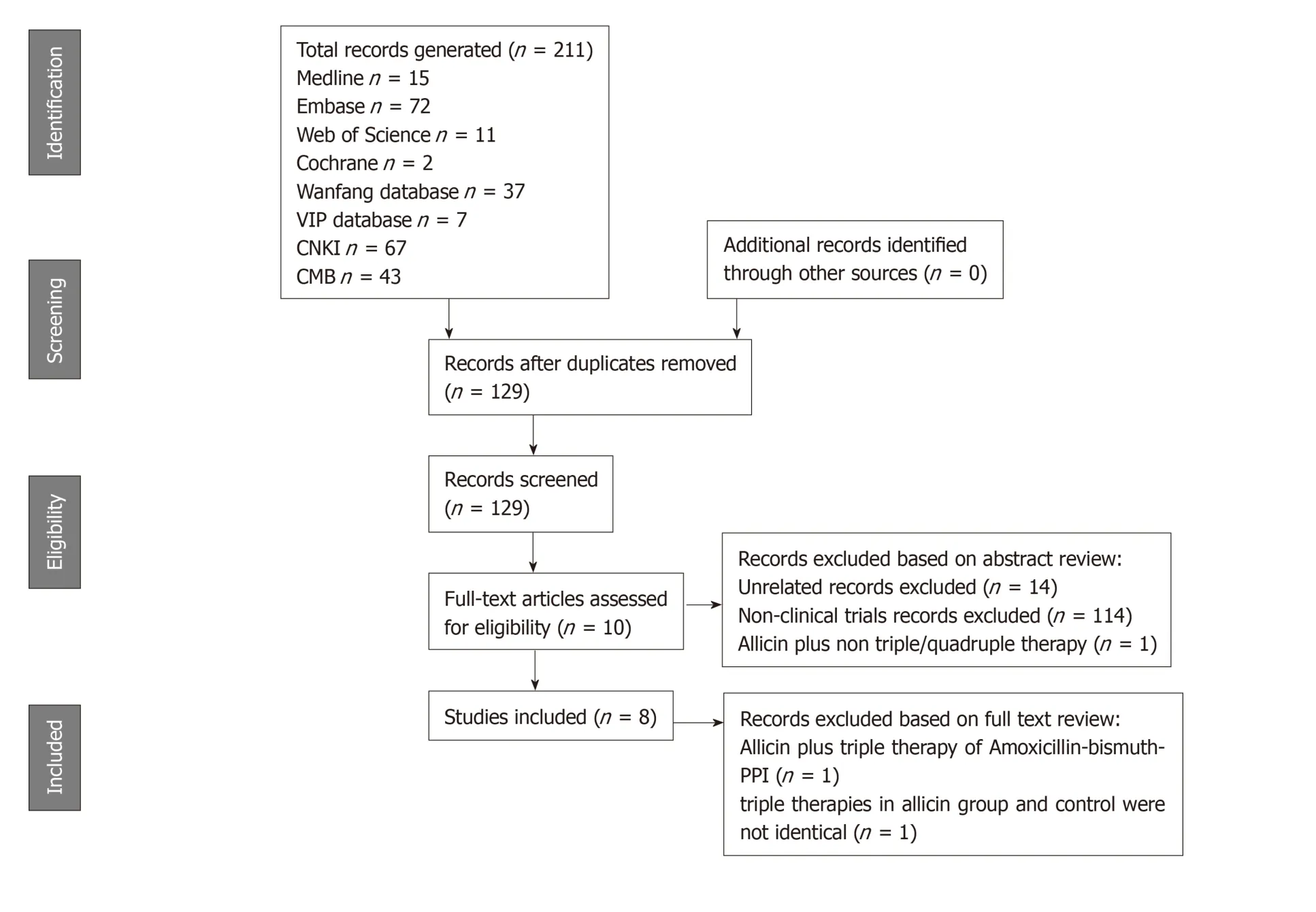
Figure 1 Flowchart showing the process of study selection for the systematic review.
Healing rates of peptic ulcers
Patients with H. pylori related peptic ulcers across seven studies were included. The healing rates of ulcers after H. pylori eradication therapy in the allicin group were significantly higher those of the control group for ITT analysis [86.17% (349/405) vs 75.87% (305/402), I2= 0%, heterogeneity P = 0.536, OR = 2.05, 95%CI: 1.39-3.03, P <0.001] (Figure 3) and PP analysis [86.39% (349/404) vs 76.06% (305/401), I2= 0%,heterogeneity P = 0.527, OR = 2.06, 95%CI: 1.40-3.05, P < 0.001][15-18,20-22].
Five studies[15-18,20]compared the healing rates following 7 days of allicin combined with PTT vs PTT alone. The allicin group showed significantly higher rates of healing rates compared to the control group for both ITT analysis [80.32% (200/249) vs 68.29%(168/246), I2= 0%, OR = 2.14, 95%CI: 1.39-3.29, P = 0.001] and PP analysis [80.65%(200/248) vs 68.57% (168/245), I2= 0%, OR = 1.93, 95%CI: 1.25-2.96, P = 0.003]. Upon comparison of allicin-PPI-bismuth-tinidazole-clarithromycin vs PPI-bismuthtinidazole-clarithromycin, significantly higher healing rates in the allicin group were observed for ITT/PP analyses [95.51% (149/156) vs 87.82% (137/156), I2= 22.924, OR =2.83, 95%CI: 1.13-7.10, P = 0.026][21,22]. Allicin plus PPI-amoxicillin-furazolidone showed significantly higher healing rates than the control group for ITT/PP analyses[83.62% (97/116) vs 65.00% (78/120), I2= 0%, OR = 1.90, 95%CI: 1.18-3.06][15,18,20](Table 4).
Total remission rates of peptic ulcers
Six studies[15,16,18,20-22]reported peptic ulcer remission rates. The total remission across allicin groups was significantly higher than that of controls for ITT/PP analyses[95.99% (359/374) vs 89.25% (332/372), I2= 0, heterogeneity P = 0.84, OR = 3.13,95%CI: 1.51-6.51, P = 0.004] (Figure 4).
Four studies[15,18,20,21]compared allicin combined with PTT vs PTT alone for total remission rates for ITT/PP analyses [93.57% (233/249) vs 80.83% (204/246), I2= 0, OR= 3.04, 95%CI: 1.51-6.13, P = 0.004]. Studies comparing BCQT plus allicin vs BCQT alone reported total remission rates of 100%[21,22]. Allicin plus PPI-amoxicillinfurazolidone showed higher total remission rates of 94.22% compared to 7-day PPIamoxicillin-furazolidone therapy for ITT/PP analyses [93.97% (109/116) vs 80.83%(97/120), I2= 0%, OR = 4.87, 95%CI: 1.36-17.50, P = 0.015][15,18,20](Table 5).
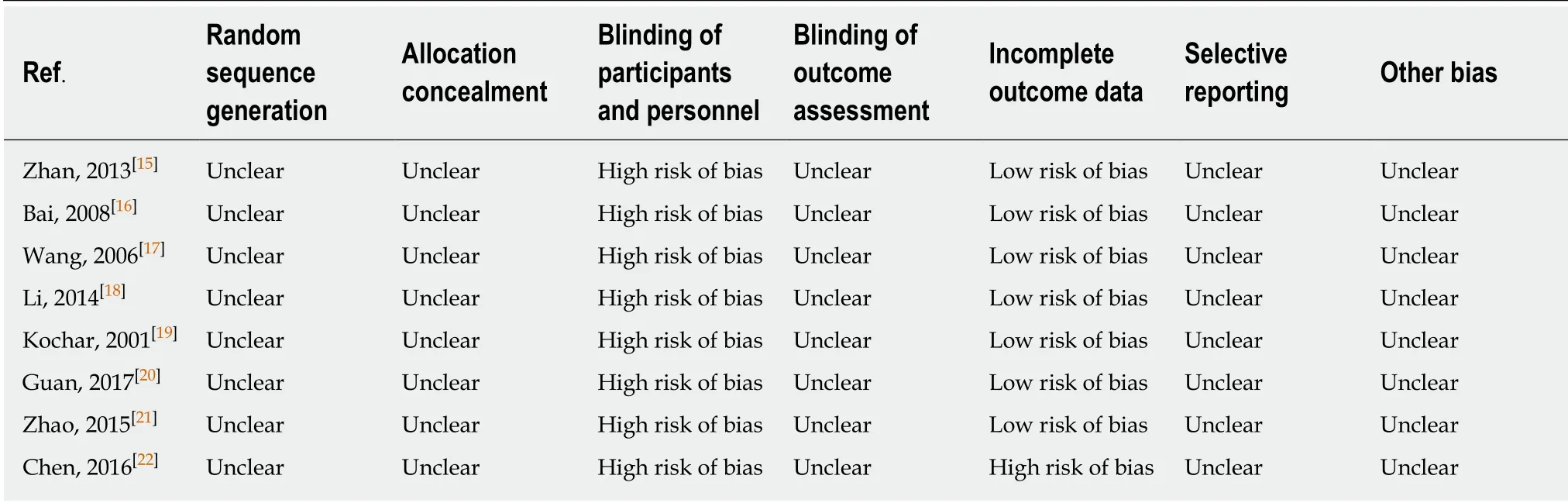
Table 2 Results of quality assessment
Side effects
Six studies[17-22]reported side effects in the allicin group and control group without statistical significance for ITT analysis [5.90% (18/305) vs 9.53% (29/304), I2= 0%,heterogeneity P = 0.591, OR = 0.61, 95%CI: 0.32-1.16, P = 0.133] (Figure 5) and PP analysis [5.92% (18/304) vs 9.57% (29/303), I2= 0%, heterogeneity P = 0.593, OR = 0.61,95%CI: 0.32-1.16, P = 0.132].
Four studies[17-20]compared allicin combined with PTT vs PTT alone for side effects.No significant differences were observed for ITT analysis [7.38% (11/149) vs 13.51%(20/148), OR = 0.52, 95%CI: 0.22-1.20, P = 0.125] and PP analysis [5.92% (18/304) vs 9.57% (29/303), OR = 0.61, 95%CI: 0.32-1.16, P = 0.132]. Two studies[18,20]compared allicin-PPI-amoxicillin-furazolidone therapy vs PPI-amoxicillin-furazolidone alone,which showed no significant differences between groups for ITT/PP analyses [2.27%(2/88) vs 7.95% (7/88), I2= 0%, OR = 0.27, 95%CI: 0.054-1.34, P = 0.110]. No significant differences were observed for allicin-PPI-bismuth-tinidazole-clarithromycin vs PPIbismuth-tinidazole-clarithromycin alone for ITT/PP analyses [4.49% (7/156) vs 5.77%(9/156), I2= 0%, OR = 0.77, 95%CI: 0.28-2.13, P = 0.612][21,22](Table 6).
Remission of abdominal pain
Two studies[21,22]reported the remission of abdominal pain in both groups. Chen et al[22]reported the subsidence of abdominal pain after 1.52 ± 0.5 d in the allicin group compared to 2.2 ± 1.2 d in control subjects. This significant difference was in contrast to that reported by Zhao et al[21](average times of 1.55 ± 0.5 d and 1.80 ± 0.6 d in the allicin and control groups, respectively). A further meta-analysis showed more rapid cessation of abdominal pain in the allicin group [standard mean difference (SMD) = -0.653, 95%CI: -0.88--0.43, P < 0.001] (Figure 6).
Sensitivity analysis
From the sensitivity analysis, the individual removal of studies had no statistical significance and the pooled OR was unchanged.
TSA
TSA of the eradication rates showed that the required information size (RIS) of 295 participants were required to calculate the eradication rates of our meta-synthesis,based on the following statistical indicators of I error probability (α = 5%): Type II error probability (β = 20%); relative risk reduction (RRR = -12.41%); and incidence in the control arm (Pc = 83.45%, derived from the meta-analysis data). Cumulative Zcurve crossed the trial sequential monitoring boundary, showing significant evidence of eradication rates. The cumulative values of the Z scores crossed conventional boundary values, trial sequential monitoring boundaries, and RIS line, suggesting that the trials were sufficient, and no alterations of the conclusions were likely (Figure 7).
A further TSA of the healing rates showed that RIS of 635 participants was required to calculate the healing rates based on the following statistical indicators of I error probability (α = 5%): β = 20%; RRR = -10.49%; and Pc = 79.14%. Cumulative Z-curves crossed the trial sequential monitoring boundary, which showed sufficient evidence of statistically significant healing rates. Z-curves crossed the conventional boundary values, and trial sequential monitoring boundaries reached the RIS line, suggesting that the trials sufficiently drew reliable conclusions (Figure 8).
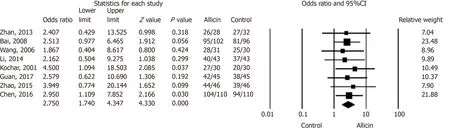
Figure 2 Eradication rates of Helicobacter pylori between allicin and control groups (intent-to-treat analysis).
Evidence quality evaluation
We downgraded by two levels for the “risk of bias” as the included studies did not state randomization methods, despite claiming to be randomized. In addition, the blinding of patients was not described in all included studies, which were therefore classed as non-blind. Studies were further downgraded due to “indirectness”. We assessed the efficacy of eradication rates as primary outcomes in patients with H.pylori infection. However, participants of the seven included studies (7/8, 87.50%) had H. pylori infection combined with peptic ulcers. These differences might lead to further bias. As a result, the overall certainty of the eradication rates was "very low"due to such downgrades. The outcomes of “healing rates of peptic ulcers” and “total remission rates of peptic ulcers” were “low” due to the “risk of bias” as all included studies did not state randomization and blinding methods despite claiming to be randomized. The outcome of “side effect rates” was graded as “very low” due to similar issues. GRADE evidence profiles are shown in Table 7.
DISCUSSION
H. pylori infection is one of the pathogenic factors of gastritis, peptic ulcers, and MALT[1]. H. pylori eradication plays an important role in the treatment of digestive disease and reduces the lifetime risk of gastric cancer[1]. In recent years, antibiotic resistance, particularly metronidazole and clarithromycin, have threatened H. pylori therapy[2]. Nearly 15% of H. pylori isolates develop multiple drug resistance (resistance to three or more antibiotics)[3,28]. As a result, the eradication rates of PTT have decreased to 70%-85%[1,29]. Accordingly, clarithromycin-based triple therapy is not recommended in areas of high resistance[3]. Compared to PTT, BCQT is an accepted strategy to increase eradication rates[1], particularly in areas of clarithromycin and metronidazole resistance[1]. According to the meta-analysis performed by Venerito et al[30], the eradication rates of bismuth-based quadruple therapy range from 68.8% to 91.0% (intention-to-treat analysis) with a total eradication rate of 77.6%. Both therapies failed to effectively control H. pylori. Considering increased antibiotic resistance rates and treatment failure rates, new H. pylori treatment strategies need to be developed. Accordingly, finding alternative non-antibiotic approaches is one of new strategies for H. pylori treatment.
Garlic is anti-bacterial and has been used to treat infectious diseases. In 1998,Chung et al[31]first reported that garlic components can suppress H. pylori growth.Diallyl sulfide (DAS) or diallyl disulfide (DADS) was shown to elicit bactericidal effects on H. pylori cultures. During that period, commercial garlic preparations containing either garlic powder (GP) or garlic oil (GO) were assessed. GP is a preparation of sliced, dried, and pulverized garlic cloves to which water is added. GO is produced by heating crushed garlic cloves to 100 °C, collecting the vapor as a distillate, and diluting the final product in vegetable oil[32]. Although O'Gara et al demonstrated the anti-H. pylori effects of GO and GP in vitro, determined through minimal inhibitory concentrations ranging from 8 to 32 mg/mL and 250 to 500 mg/mL, respectively, subsequent clinical studies failed to confirm this activity. Aydin et al[12]reported a prospective cohort of 20 H. pylori infected individuals treated with GO (275 mg three times per day combined with omeprazole) in whom no significant effects on H. pylori eradication were observed. A non-randomized crossover trial byGraham et al[13]treated H. pylori infected individuals with fresh oral garlic, with no beneficial effects reported. In 2001, McNulty et al[33]performed a clinical trial with GO therapy in which the subjects received one 4 mg GO capsule with their meals four times per day for 14 d. No evidence of either H. pylori eradication or the improvement of symptoms was observed. These negative results failed to prove the inhibitory effects of fresh garlic and GO on H. pylori. These failures can, however, be rationalized. First, although the levels of allicin in commercial products are roughly equivalent to those of fresh crushed garlic, the conversion of allicin to other garlic sulfides can occur during the production process[12]. Second, it is accepted that the anti-H. pylori effects of garlic are dose dependent but no consensus on acceptable garlic doses exists. Whether effective doses were used in these trials remains unclear.
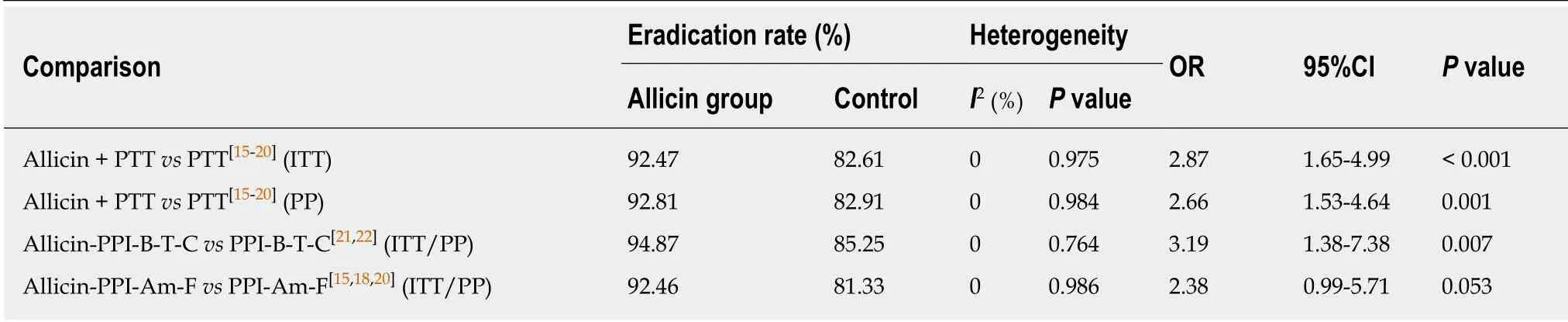
Table 3 Subgroup analyses of eradication rates
Allicin was first defined as an antimicrobial agent in 1944[34]and was subsequently shown to have anti-H. pylori effects[35], the mechanism(s) of which remain undefined[35]. H. pylori suppression may contribute to the anti-inflammatory effects of allicin, particularly the inhibition of IL-8 and TNF-α. H. pylori infection inhibits heat shock proteins (HSP) and promotes lipopolysaccharidase release[36]. In recent years,the artificial synthesis of allicin in commercial preparation (40 mg per tablet)improved allicin therapy. A series of clinical trials were performed in H. pylori infected individuals in whom allicin was administered as an add-on treatment to PTT/BCQT to treat H. pylori infection and H. pylori-related disease. Xue et al[37]performed a trial in which the eradication rate of allicin with ranitidine therapy were compared to that of ranitidine alone. Negative results were reported, suggesting that garlic products fail to eradicate H. pylori in the absence of antibiotics.
In this review, we analyzed trials that included allicin as an add-on treatment to PTT/BCQT for H. pylori infection. Allicin treated groups showed an eradication rate of ~93.81%. These results were graded as “good” (90%-95%) and highlight the benefits of allicin as an add-on treatment for H. pylori eradication[38]. Our meta-analysis also showed that allicin plus PTT/BCQT resulted in higher healing rates and total remission rates of peptic ulcers. Several mechanisms contribute to improved ulcer responses. First, inflammatory responses play a role in the development of peptic ulcers. Allicin inhibits the activation of NF-Kβ, which inhibits the production of TNFα, leading to anti-inflammatory effects[39]. Second, garlic extracts have protective effects and alleviate oxidative stress in gastric tissue. Such process contributes to mucosal injury and ulcer development[40]. Third, peptic ulcers result from a disturbance of aggressive and defensive factors in the stomach. Garlic extracts may enhance NO synthesis through increasing the activity of constitutive nitric oxide synthase (cNOS) and promoting the maintenance of endothelial function[41-42].
In recent years, several options such as phytotherapy[6,7]or traditional Chinese medicine[43], probiotics[8], and nutraceutical agents[44]have been proposed as alternative treatments for H. pylori infection. In addition to allicin, several other add-on treatments to PTT/BCQT have been investigated as well, with clinical evidence published. Berberine, extracted from Coptis chinensis Franch, was used to treat H. pylori infection through its combination with PTT. The eradication rate of berberine plus PTT was 85.89 % according to previous meta-analysis[45]. Probiotics have been used as an add-on treatment for H. pylori infection. Gong et al[29]performed a meta-analysis to evaluate the efficacy of probiotics plus PTT with an eradication rate of 80.74%reported. A further meta-analysis evaluated the effects of probiotics plus BQCT with an eradication rate of 90.76% observed[8]. Yin et al[42]also performed a meta-analysis that evaluated the traditional Chinese medicine Jinghua Weikang capsules plus PTT with an eradication rate of 85.47%. These therapeutic regimens did not achieve the effectiveness of allicin plus PTT therapy for the treatment of H. pylori infection.However, the role of alternative treatment remains controversial. Previous studies mostly demonstrated that the agents as alternative treatment exhibit antiinflammatory, immunomodulatory, and gastro-protective activities. Such activities contributed to improvement of peptic ulcer healing and remission of gastrointestinal tract symptoms. The anti-H. pylori activities were not well proved due to the lack of correlation between in vitro susceptibility and in vivo efficacy. What's more, no agent of alternative treatment was accepted to treat H. pylori infection as a monotherapy. In this regard, we speculate that anti-H. pylori activities of such agents, especially medical plants, exist while their active ingredients and effective dosages need to be further explored. The research and development process of allicin, i.e., identification of active ingredients followed by therapeutic dosage exploration, might be a typical case of clinical application of alternative medicine.
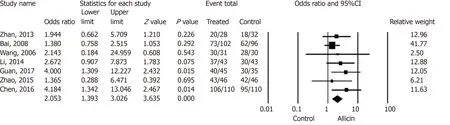
Figure 3 Healing rates of peptic ulcers between allicin and control groups (intent-to-treat analysis).
Two previous meta-analyses[46-47]showed comparable findings, but common insufficiencies limit the quality of their evidence. Both analyses[46-47]included studies of PPI-clarithromycin-bismuth ± allicin[14], whilst Hu et al[46]compared ranitidine plus allicin to allicin alone[37]. Both therapeutic regimens are not wildly accepted and may have caused an unneglected bias risk. The study by Hu et al[46]performed an adequate search strategy, but the H. pylori patients had duodenal ulcers, which narrowed the application of the evidence.
This is the first systematic review and meta-analysis of H. pylori treatment using allicin that was assessed using the GRADE system, although the quality of main outcome was graded as “very low” due to downgrades for the risk of bias and indirectness. What’s more, when considering this meta-analysis, potential limitations should be considered: (1) The included studies were of low quality, which limited the clinical evidence; (2) Although I2 statistics assessment showed no statistical heterogeneity, we considered existence of clinical heterogeneity of the included studies. First, seven included studies included the participants with H. pylori infection combined with H. pylori related ulcers while the rest one[19]included the participants with H. pylori infection alone. Second, the present review compared the efficacy of allicin plus PTT/BCQT vs PTT/BCQT alone. However, the PTT/BCQT regimens of included studies differed, especially components of antibiotics. Third, most of the included studies (7/8, 87.50%) were performed in China except for the study by Kochar et al[19]. Fourth, the eradication therapy period of the included studies ranged from 7 d to 14 d; and (3) Antibiotic resistance of the participants was not assessed, so the efficacy of allicin on antibiotic resistant H. pylori strains was not assessed.
In conclusion, this study provides evidence that allicin improves eradication rates,healing rates, the remission of peptic ulcers, and the remission of abdominal pain, but does not affect side effects when used as an add-on treatment for H. pylori infection and H. pylori related ulcers. However, the quality of this study was graded as “very low” for eradication and side effects rates and “low” for healing and total remission rates of peptic ulcers. These results should be treated with cautions due to limited quality of the included studies.
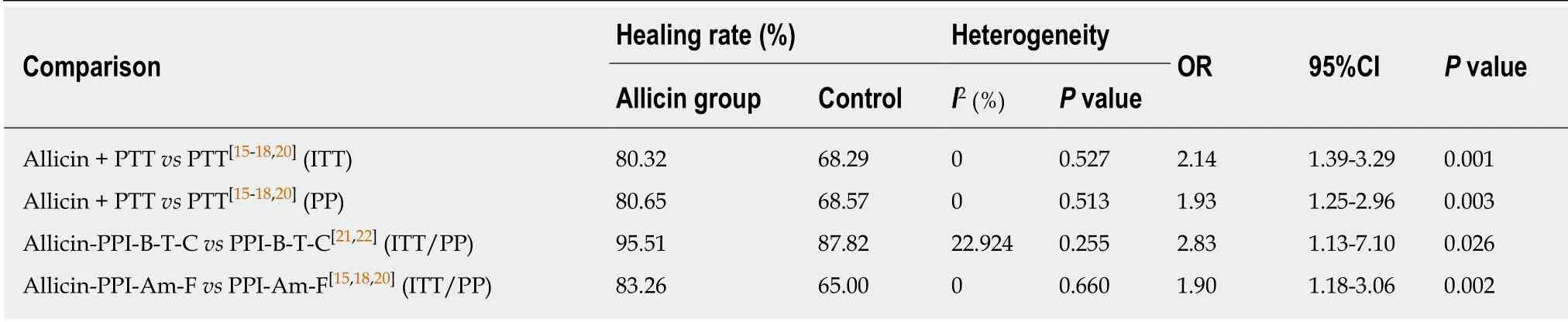
Table 4 Subgroup analyses of healing rates of peptic ulcers

Table 5 Subgroup analyses of total remission rates of peptic ulcers
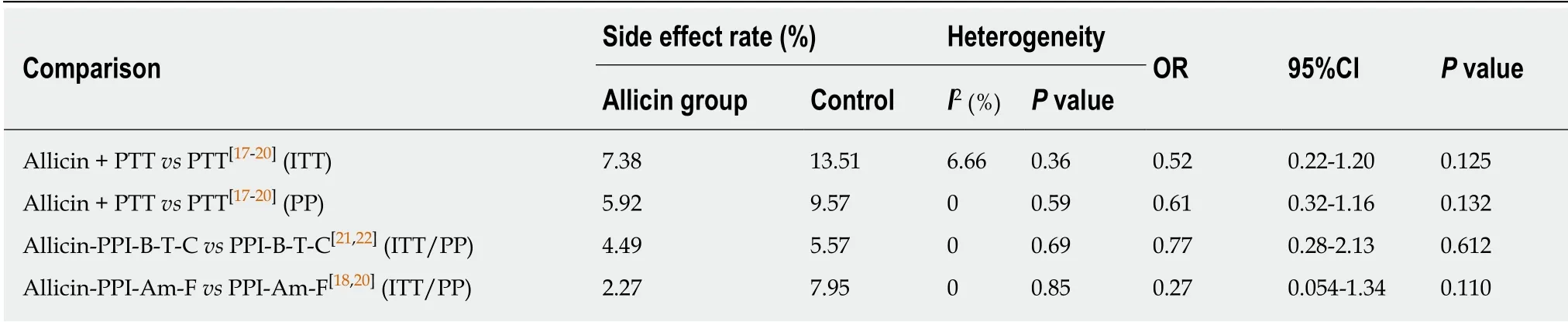
Table 6 Subgroup analyses of side effect rates
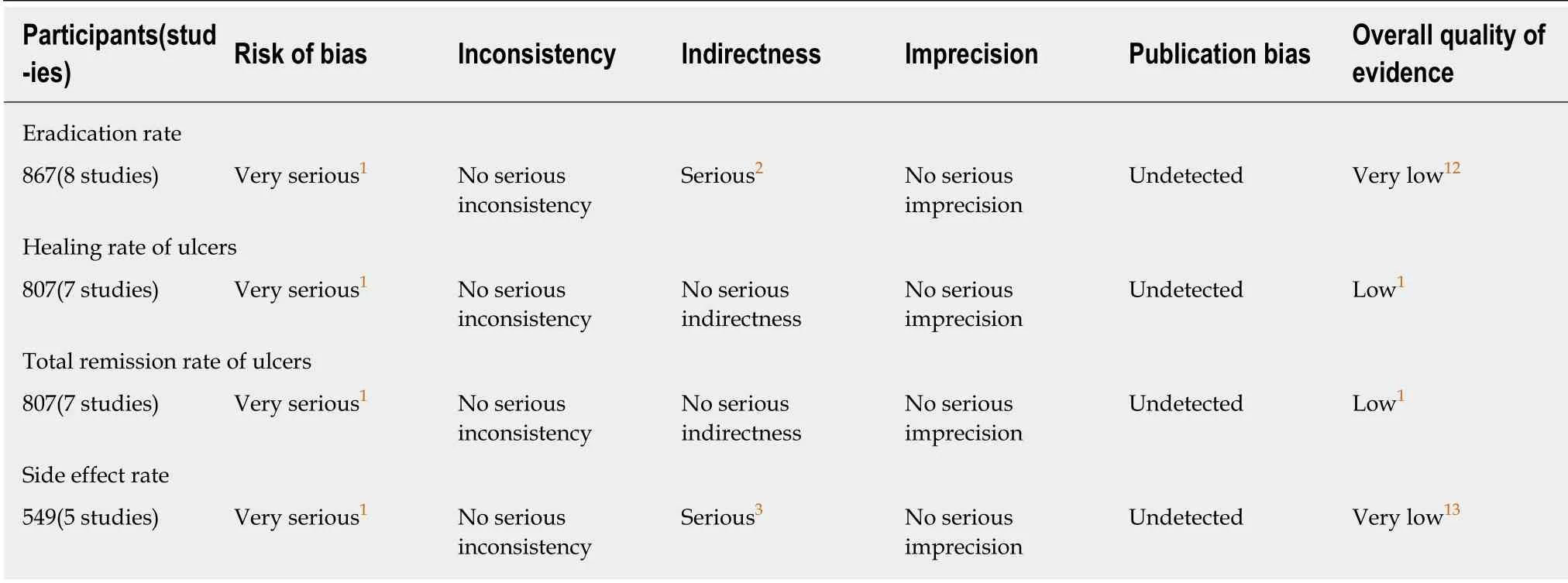
Table 7 Results of quality assessment
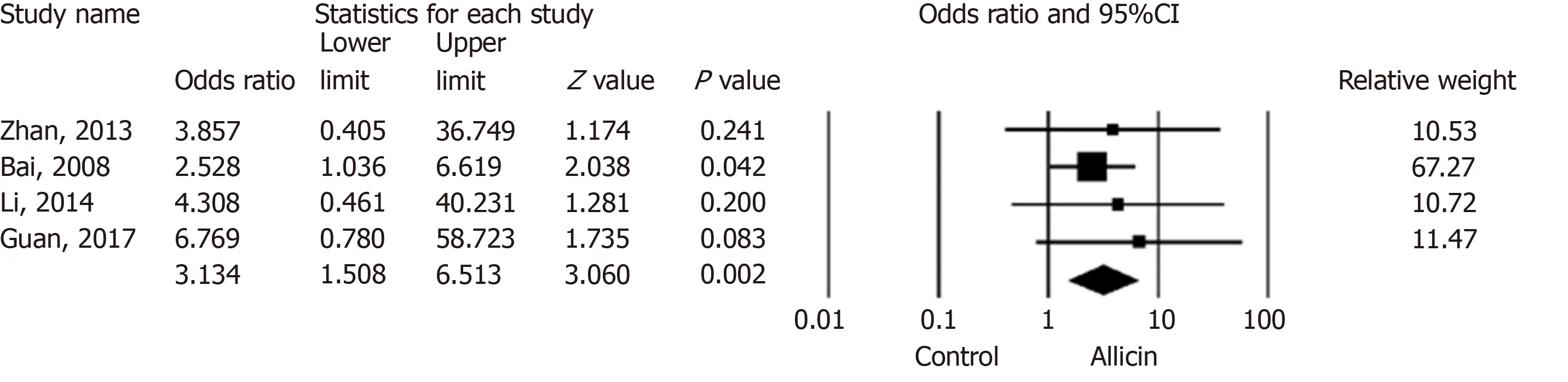
Figure 4 Total remission rates of peptic ulcers between allicin and control groups (intent-to-treat/per-protocol analysis).
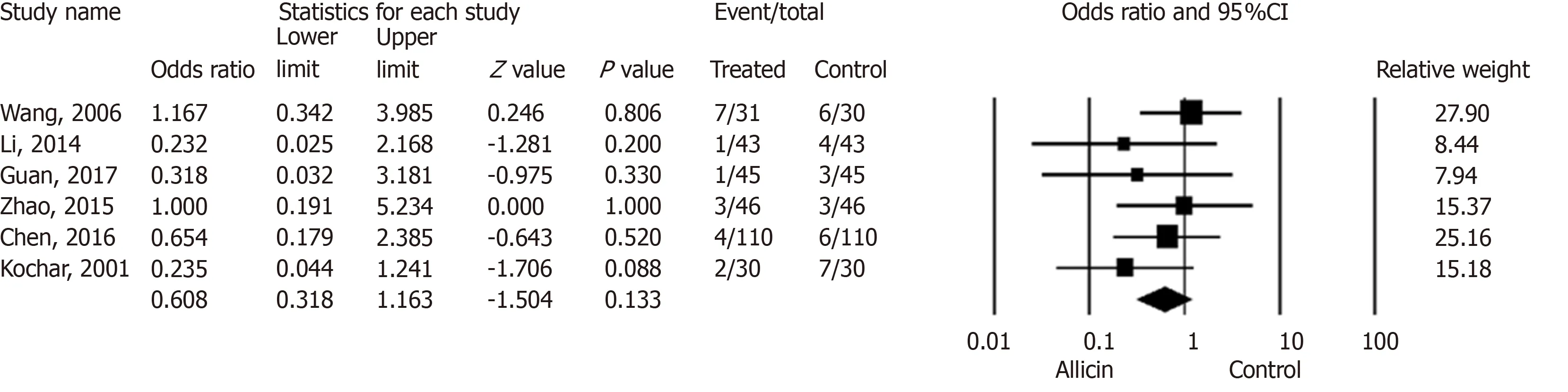
Figure 5 Side effect rates between allicin and control groups (intent-to-treat/per-protocol analysis).

Figure 6 Abdominal pain disappearance times between allicin and control groups.
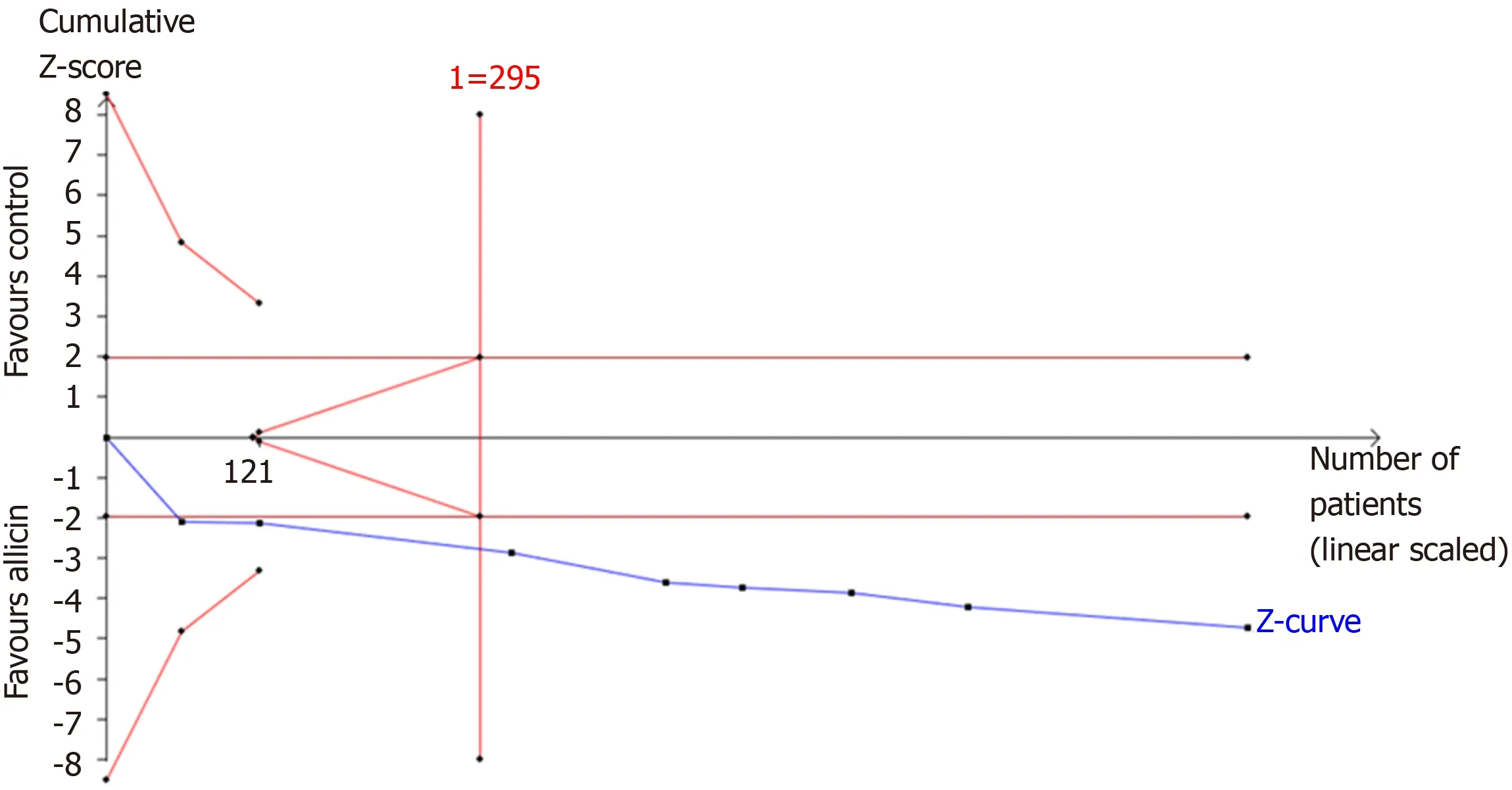
Figure 7 Trial sequential analysis of the eradication rates.
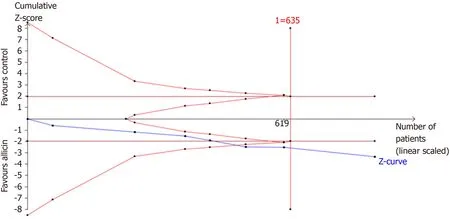
Figure 8 Trial sequential analysis of the healing rates of peptic ulcers.
ARTICLE HIGHLIGHTS
Research background
Allicin (2-propene-1-sulfinothioic acid S-2-propenyl ester, diallyl thiosulfinate), a compound of garlic, was proved to be active in inhibiting Helicobacter pylori (H. pylori) growth in vitro.However, several clinical trials using garlic oil and fresh oral garlic failed to show improvements in H. pylori infection. In recent years, due to developments in pharmaceutical technology,commercial allicin tablets are available, with a series of randomized clinical trials that explored allicin as an add-on therapy to PPI therapy or bismuth containing quadruple therapy to treat H.pylori infection.
Research motivation
Allicin as an add-on therapy to treat H. pylori infection has been trialed, with variable results.Whether allicin could be medicated as an anti-H. pylori drug is still inconclusive.
Research objectives
We performed a meta-analysis to evaluate the efficacy and safety of allicin as an add-on therapy,i.e., allicin plus PPI triple therapy or bismuth containing quadruple therapy for H. pylori infection.
Research methods
Electronic databases including MEDLINE, EMBASE, Web of Science, etc. were searched. A metaanalysis was performed using the fixed-effects model for low heterogeneity and the randomeffects model for high heterogeneity with sensitivity analysis. Bias was evaluated using Egger’s tests. Trial sequential analysis (TSA) was used to evaluate information size and treatment benefits. The Grading of Recommendations Assessment, Development and Evaluation (GRADE)was used to assess the level of quality.
Research results
A total of eight RCTs consisting of 867 participants were included. As a result, add-on therapy of allicin combined with PPI triple therapy (PTT) or bismuth containing quadruple therapy (BCQT)showed a significantly higher eradication rate (93.33% vs 83.56%, P < 0.001) and healing rates of ulcer (86.17% vs 75.87%, P < 0.001). In addition, the total remission rate of peptic ulcers across all allicin groups was significantly higher than that of controls (96.05% vs 86.55%, P = 0.015). Such outcomes were graded as “low” (ulcer healing rates and total ulcer remission rates) or “very low” (eradication rates and side effects rates) according to the GRADE assessment.
Research conclusions
This study provides evidence that allicin improves eradication rates, healing rates, the remission of peptic ulcers, and the remission of abdominal pain, but does not affect side effects when used as an add-on treatment for H. pylori infection and H. pylori related ulcers. In other words, allicin plus PPI triple therapy or bismuth containing quadruple therapy may obtain better therapeutic effects.
Research perspectives
The present review evaluated the efficacy and safety of allicin as an add-on therapy for H. pylori infection, with conclusion that allicin might improve healing rate and symptom remission of H.pylori related ulcers as well as H. pylori eradication rate. However, there are still many questions remaining unclear. On one hand, the exact mechanism of allicin as an anti-H. pylori drug is not clear up till now. On the other hand, further clinical evidence of high quality is still needed since the present evidence is of “low” or “very low” quality.
杂志排行

World Journal of Gastroenterology的其它文章
- Gut-liver axis signaling in portal hypertension
- Role of tristetraprolin phosphorylation in paediatric patients with inflammatory bowel disease
- STW 5 is effective against nonsteroidal anti-inflammatory drugs induced gastro-duodenal lesions in rats
- Superior gallstone dissolubility and safety of tert-amyl ethyl ether over methyl-tertiary butyl ether
- Gender differences in vascular reactivity of mesenteric arterioles in portal hypertensive and non-portal hypertensive rats
- Construction of a replication-competent hepatitis B virus vector carrying secreted luciferase transgene and establishment of new hepatitis B virus replication and expression cell lines