Association between measles antibodies in vaccinated and naturally infected mothers with protective antibodies and the occurrence of measles in their children: A cross-sectional study in the Bavi district of Hanoi
2019-10-17CamNhatNguyenQuynhNgocNguyenThanHuuDaoLeThiQuynhMai
Cam Nhat Nguyen, Quynh Ngoc Nguyen, Than Huu Dao, Le Thi Quynh Mai✉
1Infectious Disease Prevention and Control Department, Center for Disease Control, Hanoi, Vietnam
2Virology Department, National Institute of Hygiene and Epidemiology, Hanoi, Vietnam
ABSTRACT Objective: To determine the concentration and rate of decay of maternal IgG antibodies against measles prevalence in infants of vaccinated or naturally infected mothers and study initial measles immunization occurs in nine-month-old children.Methods: In total, 401 pregnant women and the same number of their subsequent newborns were recruited in the Bavi district of Hanoi in 2016-2017; they were divided into two groups:Older women (born before 1985, n=201) and younger women (born after 1990, n=200).Samples were collected at fi ve time-points; week 36 of pregnancy, birth (cord), and 3, 6, and 9 months after birth. Measles-specif i c IgG antibody levels were recorded.Results: In total, 77.06% of the 401 pregnant women were seropositive for measles-specif i c IgG antibodies. A signif i cantly greater proportion of mothers aged 30 and older (88.06%)and their newborn ( 93.53%) were seropositive compared to the mothers aged 25 and younger (66.00%), and their newborn (72.00%) (P<0.001). The infants of older mothers had significantly higher geometric mean titres (GMT) of measles IgG antibodies than the infants of younger mothers (P<0.001) at all time-points of the study period . The proportion of measles IgG antibodies together with GMT decreased from 82.97% (506.96) at the age of three months to 23.19% (45.22) at the age of nine months.Conclusions: This study provides a profile of maternal antibodies against measles in Vietnamese infants and investigates the early susceptibility to measles in both the infants of vaccinated mothers and mothers with naturally acquired immunity. These data suggest that determining the appropriate age for measles vaccination is paramount for the elimination of measles in Vietnam.
Keywords:Infant Measles Seropositive National Expanded Program of Immunization Vietnam
1. Introduction
Children are born with immature immune systems, and maternal immunization can be useful in protecting infants for several months during their fi rst year of life[1-4]. In Vietnam, the fi rst dose of the measles vaccine is administered to children at the age of nine months [5,6]. The coverage rate has been reported at more than 90%.However, the exposure of measles to infants younger than nine months has been conf i rmed. Therefore, the abilities of the protective maternal antibody against measles must be considered[5-7].
Measles reemerged during 2008-2010 in Vietnam with 7 948 confirmed cases[9] and again in May 2013, when cases were reported from 24 cities and provinces, including the major urban centers of Hanoi and Ho Chi Minh[7]. In 2014, a measles epidemic occurred in Hanoi with a record-breaking number of 1 700 cases that killed at least 100 children[7,9]. Of these children, a number of young children (under the age of nine months) were determined indicating a need for the investigation into the protection of maternal antibodies against measles in young infants in Vietnam.The objective of this study was to determine the seroprevalence of maternal measles IgG in pregnant women and their infants not yet eligible for vaccinations by taking measurements at fi ve different time points (a longitudinal study) to gain an insight into the decrease in protection from the maternal antibodies around the age of fi rst year.
2. Material and methods
2.1. Study design
This cross-sectional and questionnaire-based seroprevalence study was conducted from January 2016 to December 2016 at 30 communes in the Bavi district in Hanoi, based on the Commune Population Register System (CPRS)[8]. The Expanded Program for Immunization (EPI) has been operating in the Bavi district since 1990 with a measles vaccination coverage range between 90%-99%.There was no recent measles epidemics, though there was a widely spread outbreak in Hanoi in 2014 with a small number of conf i rmed cases (13) being reported at eight communes in Bavi[9,10].
2.2. Participants and sample size
The study involved 401 pregnant women and same number of their subsequent newborns recruited from 30 communes in the Bavi district of Hanoi. The women visited community medical centers or Bavi General Hospital for routine examinations and delivered babies at these locations between January 2016 and December 2016.Participants completed a questionnaire on demographics, validated vaccination history, and medical history. Growth parameters,breastfeeding, daycare attendance, and immunization data were also collected.
We classif i ed pregnant women into two groups. The fi rst group consisted of those who were 30 years old or older (born before 1985,when the EPI was not applied) with natural immunity to measles.The other group was vaccinated and aged below 25 (born after 1990,when EPI coverage was at a higher rate), and we sought vaccination documentation for each woman in this group.
There were no exclusion criteria except for refusal to participate.The sample size necessary for this study was 401 pregnant women containing 201 in the >30 years group and 200 in the <25 years group. The sample took into account the prevalence of natural measles immunization levels in 95% of women aged over 30 years and a vaccinated level of 85% in women aged below 25 years, an alpha error of 5%, and a precision of ± 0.007.
All participants gave informed consent. We collected 5 mL of intravenous blood from the enrolled women at the last routine examination (36 weeks or later of gestational age), at birth (5 mL of umbilical cord blood), and in all infants (2 mL) at the third month (90-119 days), sixth month (180-209 days), and ninth month(270-299 days). All samples from infants were collected during vaccination schedules, except for umbilical cord blood. Serum was separated from the blood samples and stored at -20 ℃ until transfer to the Microbiological Laboratory of the Hanoi Center for Disease Control.
2.3. Determination of antibodies
We used an enzyme-linked immunosorbent assay (ELISA; SIEMENGermany) for the quantitative measurement of measles antibodies. Based on the test criteria according to the manufacturer’s instructions with 99.6%sensitivity: The anti-measles virus was negative when ΔA <0.100 (cutoff), the anti-measles virus was positive when ΔA> 0.200, and the anti-measles virus was equivocal when 0.100 ≤ ΔA ≤ 0.200. The quantitative results of the antibodies were calculated according to the following formula: Log10 mIU / mL = α × ΔAβ. The α and β values were provided according to the biological set in the barcode table.
2.4. Statistical analysis
We conducted analyses on the decay of maternal antibodies in infants over time and estimated the individual time to immunity loss in relation to the antibody concentration of their mothers.
Data analysis using Stata software version 14.2, and differences between women aged 30 or older and women aged 25 or younger were determined with the nonparametric chi-square or Fisher’s exact test, as appropriate. Correlations between the interval and nominal variables with the anti-measles IgG antibody were determined by the Pearson and Eta coefficient, respectively.
2.5. Ethics approval
The Ethics committee of the National Institution of Hygiene and Epidemiology approved conducting this study based on the protocol described in the Methods section (IRB-VN01057-22-2016). We obtained written consent from all participants, and signed consent forms were kept in an archive of records for this study.
3. Results
3.1. Population
We analyzed data from 401 women and their subsequent newborns.Of these women, 201 were born before 1985 with a mean age of(33.30±2.89) years old, and 200 were born after 1990 with a mean age of (21.58±2.13) years old. Of all participating women, 59.35%(238/401) were expecting their fi rst child, 32.67% were expecting their second child (132/401), and 7.98% were expecting their third child (32/401).
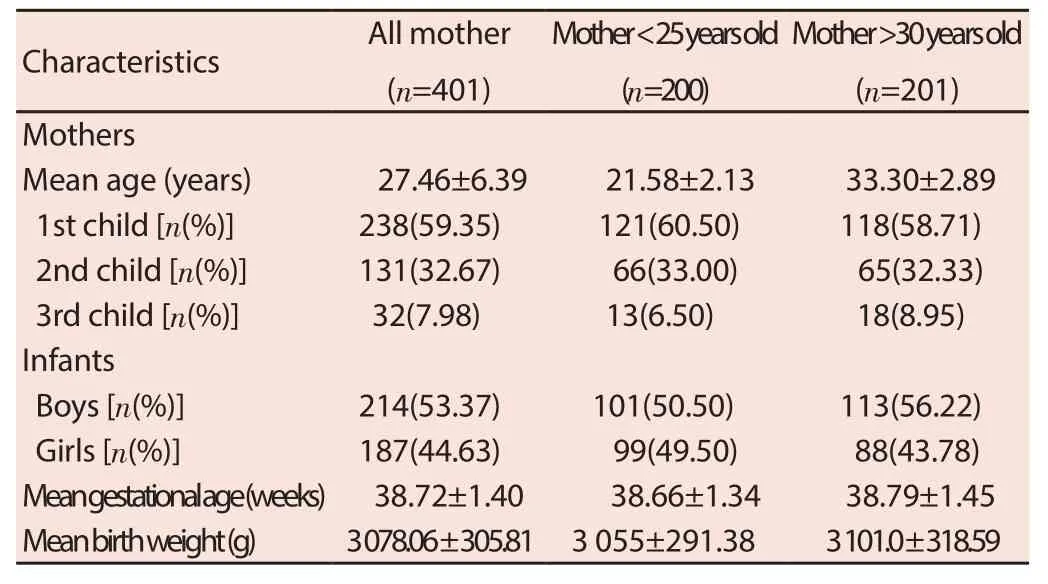
Table 1. General characteristics of both women and their infants.
3.2. Prevalence of seropositivity for measles in the general population
Sera from 401 women and same number of their newborns were examined for the anti-measles antibody titer. The sera were collected at week 36 of pregnancy for the enrolled women and from the umbilical cord blood of newborns. Overall, 309 mothers(77.06%) and refers of 332 infants aged 9 months and younger(82.79%) were positive for anti-measles IgG. A total of A total of 132 (132/200, 66.00%) mothers with positive anti-measles IgG and 144 (144/200, 72.00%) newborns were in the age 25 and under group, and 177 (177/201, 88.06%) mothers and 188 (188/201,93.53%) newborns were in the aged 30 or older group (Table 2).There were signif i cant differences in measles antibody positive(P<0.001) and GMT (P<0.005) of mothers among three groups,and the differences in measles antibody positive (P<0.001) and GMT (P<0.005) of newborns were also signif i cant among three groups. The ratios of GMT (newborn/mother) of all participants was 1.33, 1.46 for mothers <25 years, and 1.29 for mothers >30 years.
Overall the GMT of IgG at week 36 of pregnancy was 705.05 mIU/mL(95% CI: 604.66-822.10) and of the newborn was 938.85 mIU/mL (95%CI: 809.24-1 089.23). A signif i cant difference of GMT was found when comparing the <25 years old and >30 years old group and their newborns. The GMT in younger women below the age of 25 was 452.73 mIU/mL (95% CI: 370.24-553.60) and in women aged 30 and over was 1 095.89 mIU/mL (95% CI: 881.89-1 361.03).Similarly, the GMT of maternal IgG in mothers under 25 years old had signif i cantly fewer antibodies in the cord blood compared to the newborns of mothers older than 30 (P<0.001) (Table 2).

Table 2. Seroprevalence of pregnant women at 36 weeks and geometric mean titres (GMT) (95% CI) of IgG against measles and protective titer for two studied groups of mother and their newborn.
3.3. Decay of maternal anti-measles IgG during infancy
Anti-measles antibody seropositivity in infants significantly decreased as time progressed. The total number of seropositive individuals was 316 at the age of three months; 252 at the age of six months, and 93 at the age of nine months (Table 3). The GMT of anti-measles IgG was 506.96 mIU/mL (95% CI: 444.64-578.92) in infants aged three months; 217.29 mIU/mL (95% CI: 187.78-251.43)in infants aged six months, and dropped abruptly to 45.22 mIU/mL(95% CI: 38.25-53.47) in infants aged nine months (Table 3). The proportion of infants positive for anti-measles IgG reduced from 78.80% at the age of three months to 23.19% at the age of nine months (Table 3).
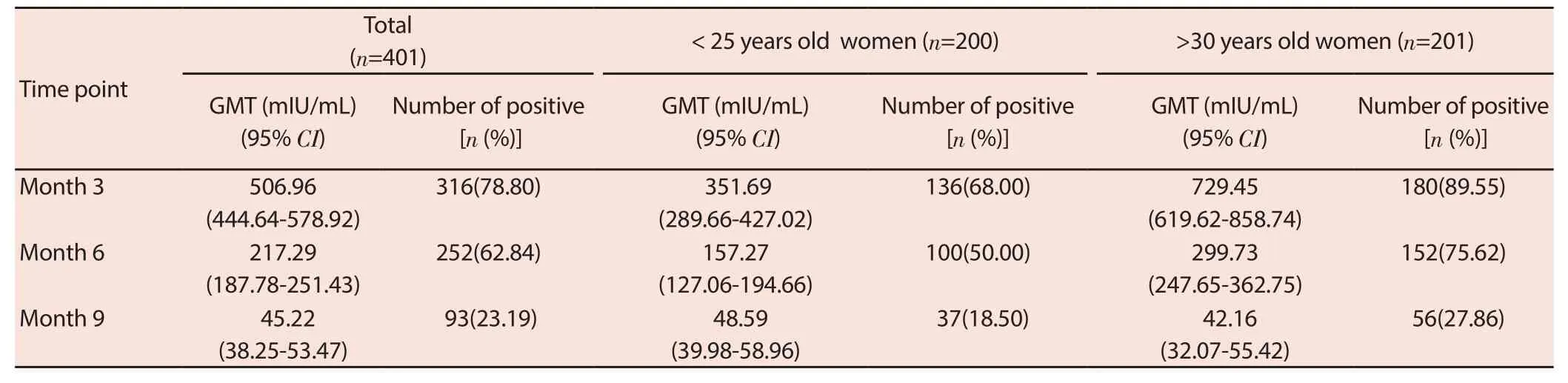
Table 3. GMT(95% CI) of IgG against measles and number of positive samples at each time-point in infants aged 9 months or younger.
The GMT of anti-measles IgG of infants of women aged >30 years was higher than those of women aged <25 years as well as the percentage of infants being seropositive for measles. In mothers >30 years old, infant seropositivity was 89.55%, 75.62%,and 27.86% at time-points of three, six, and nine months,while,the infants of women <25 years old were also positive for anti-measles IgG at approximately 68.00%, 50.00%, and 18.50%. This percentage was signif i cantly lower compared with the infants of mothers >30 years old (P<0.001). GMT decreased remarkably with the increasing age of infants. However, the anti-measles IgG titer differed significantly between these groups. The GMT of the measles antibody was lower in infants whose mothers were younger than 25 years old than in infants whose mothers were older than 30 years old (Table 3). This difference was found to be statistically signif i cant (P<0.001). At nine months of age, a very low concentration of anti-measles antibodies were identif i ed in the infants of both groups (GMT = 48.59 mIU/mL in mother younger than 25 years old group and 42.16 mIU/mL in mother older than 30 years old, respectively) (Table 3), and the difference was not signif i cant (P=0.068).
4. Discussion
Because of their relative immunological immaturity, infants are usually not immunized until after two to three months, with the most common exception of neonatal Bacillus Celmette-Guerein(BCG) immunization. Maternal antibodies have been proposed as a means of protecting infants during sensitive times in the development of their immune system[2,11-13]. However, the loss of maternal measles antibodies in infants before the vaccination age has been reported as potentially causing measles outbreaks during the fi rst year of life[14-20]. Our study aims to determine the maternal measles antibody decline in infants before the fi rst dose of the measles vaccine in the immunization program. Since the National EPI was fi rst introduced in Vietnam in 1981, it became one of six national targeted health programs in 1985. By 2009,90% of children less than one-year-old in Vietnam were recorded as being vaccinated against six diseases (diphtheria, tetanus,pertussis, poliomyelitis, measles, and tuberculosis)[5,7]. Our study was conducted in 2016 to analyze the maternal measles antibodies in the infants of two groups of women; those older than 30 years(born before 1985) and those younger than 25 years (born after 1990) to investigate the presence of maternal antibodies against measles induced by vaccination and natural exposure[5-8,21]. A total of 401 pregnant women and their children were enrolled in the study who lived in the Bavi district of Hanoi, where a longitudinal demographic surveillance system was established, and health care data have been generated since 1999(FilaBavi). Therefore, our follow-up studies on the pregnant women and their infants were done without difficulties in sampling and missing participation during the study period was minimized. Furthermore, the general characteristics of the women and their infants were similar in both groups. There was no evidence that gestational age, delivery by cesarean section, or the newborn’s weight was signif i cantly related to seroprevalence.
Antibodies to the measles virus are transferred to the baby in utero across the placenta and through breastfeeding. These antibodies are critical for protecting infants from infection during their fi rst months of life. Our study identif i ed the levels of antimeasles IgG in pregnant women and their infants. Our results showed a higher GMT of antibodies to the measles virus in pregnant women born before 1985, who may have a history of natural exposure to measles. This fi nding has been observed in several developed countries. However, this information is less documented in developing countries. Our results could provide additional data for vaccine guideline development for childbearingaged women[5-8,15-21].
Many studies undertaken in various countries have documented that the GMTs of cord blood antibodies were higher than the GMTs of maternal antibodies. A comparison of the GMTs of the anti-measles IgG in cord blood with the maternal blood found a ratio of 1.33 in our study. This fi nding is similar to those found in studies from China (1.042) and the UK (1.68) by ELISA assay[14-17].
While maternal antibodies are important for protecting infants during the first months of life, several reports have indicated that maternal antibodies interfere with the development of infant immune responses. Therefore, the development of an optimal schedule of measles vaccination based on measurements of the duration of passive immunity against measles in infants is necessary. We investigated the seroprevalence of maternal antibodies to measles in Vietnam from birth until nine months of age. Our results indicate a proportion of seropositivity decreasing from 78.8%, 62.84%, and 23.19% with increasing age (three, six,and nine months). This fi nding indicates that almost all infants at nine months of age have a significant decrease in maternal antibodies. These results are similar to other studies in Africa,Asia, America, and Europe[14-18]. Lowering maternal antibody protection results in an increased period of susceptibility to natural infection before vaccination eligibility. This is because measles vaccinations occur at the age of nine months as scheduled by the National EIP. However, our data support the recommendation that it is necessary to redesign the strategy for eliminating measles in Vietnam, as well as in developing countries.
This study has some potential limitations. The protective antibodies may have been misclassified due to the laboratory test used. We expressed measles IgG in U/mL according to manufacturer instructions, since testing methods and the def i nition of protection used varied among studies. Therefore, our results may not be useful for comparing the measles seroprevalence prof i les with others reported using plaque reduction neutralization test or Hemagglutination Inhibition assays.
This study was conducted in the Bavi district in Hanoi from January 2016 to December 2016. More than 95% coverage has been achieved for fi ve vaccines nationally; BCG, polio, measles fi rst and second doses, and diphtheria- pertussis-tetanus (DPT)by EPI in Vietnam since 2008. However, these data are not representative of the Vietnamese infant population. This is an additional limitation of our study.
Our results conf i rm the higher maternal measles IgG antibody rates and higher geometric mean titers of mothers born before 1985 and their infants than the infants of mothers born after 1990 in Vietnam. The two groups in our study differed markedly in the age of the pregnant women. However, we observed no differences in the decline of the maternal measles antibodies between them,suggesting that the mother’s age (often a correlation of vaccination status) does not determine the rate of antibody decay. Children lose the protection of their maternal antibodies and become susceptible to measles before their fi rst measles vaccinations are received. This fi nding provides an opportunity for re-addressing the age at which the fi rst dose is received in Vietnamese children.
Conflicts of interest statement
The authors declare that they have no competing interests.
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Inhibitory effects of methanolic Olea europaea and acetonic Acacia laeta on growth of Babesia and Theileria
- Curcuma angustifolia ameliorates carbon tetrachloride-induced hepatotoxicity in HepG2 cells and Swiss albino rats
- Chemoprotective activity of aqueous leaf extract of Acalypha wilkesiana against cyclophosphamide-induced toxicity in rats
- Long-term safety follow-up of children from a randomized-controlled phaseⅡb proof-of-concept efficacy study of the live, attenuated,tetravalent dengue vaccine (CYD-TDV) in Thailand
- Ebola virus disease: Recent advances in diagnostics and therapeutics