社区获得性压力性损伤现况调查及对策研究
2019-09-25郑惠渊蹇婷婷张颖向德兵
郑惠渊 蹇婷婷 张颖 向德兵

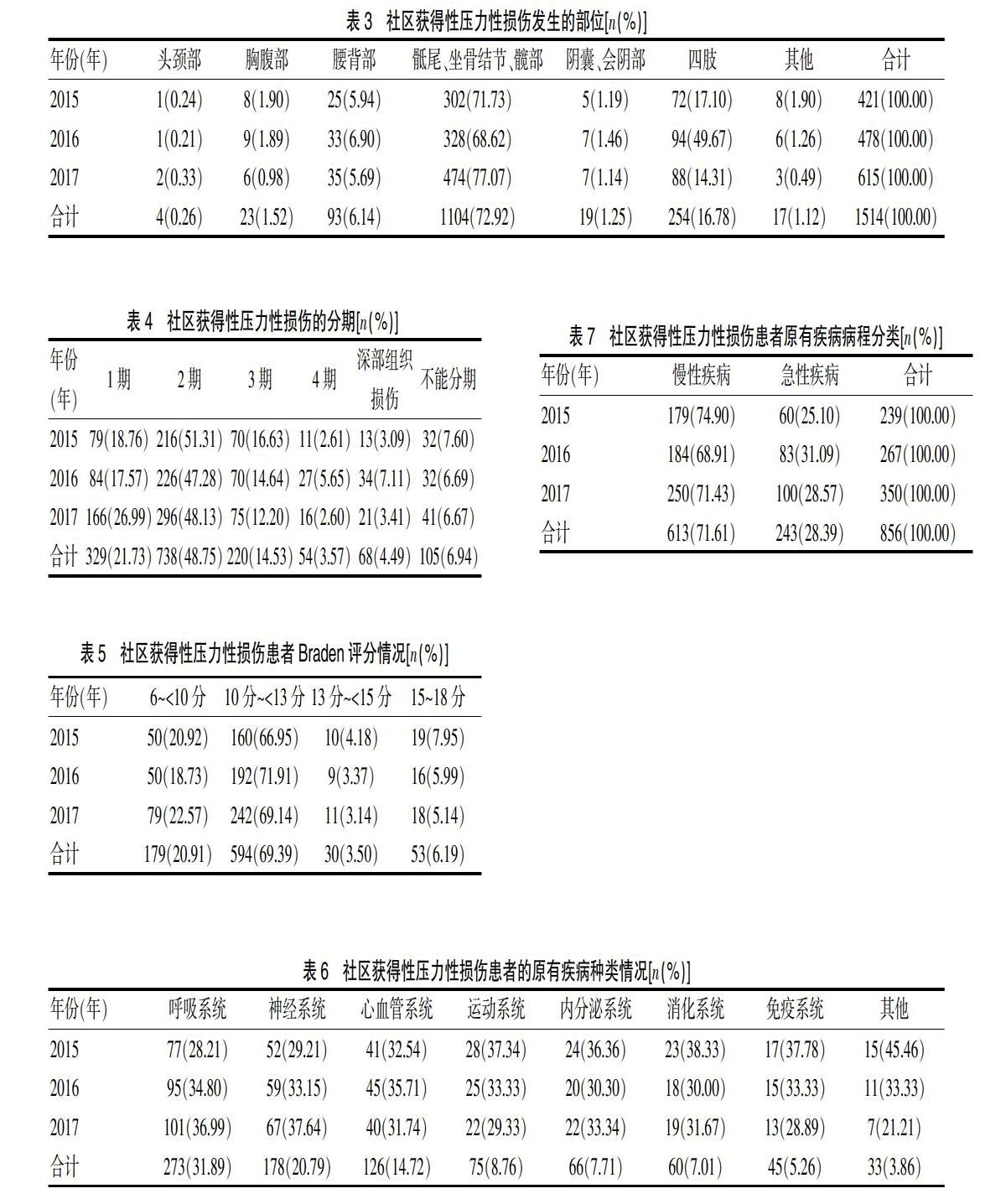
[摘要]目的 探討社区获得性压力性损伤发生的特点,为构建合理的防治体系提供依据。方法 对重庆市江津区中心医院2015年1月~2017年12月入院时有社区获得性压力性损伤的856例患者进行调查,重点调查年龄、患者来源、发生部位、分期、Braden评分、疾病种类、病程。结果 在年龄方面,26~<50岁占7.36%,50~<60岁占6.89%,60~<70岁占17.41%,70~<80岁占32.01%,80~<90岁占30.72%,≥90~105岁占5.61%。在患者来源方面,家庭占72.08%,养老机构占6.31%,其他医院占21.61%。在发生部位方面,头颈部占0.26%,胸腹部占1.52%,腰背部占6.14%,骶尾部、坐骨结节部、髋部占72.92%,阴囊、会阴部占1.25%,四肢占16.78%,其他占1.12%。在分期方面,1期占21.73%,2期占48.75%,3期占14.53%,4期占3.57%,深部组织损伤占4.49%,不能分期占6.94%。在Braden评分方面,6~<10分占20.91%,10~<13分占69.39%,13~<15分占3.50%,15~18分占6.19%。⑥在疾病种类方面,呼吸系统占31.89%,神经系统占20.79%,心血管系统占14.72%,运动系统占8.76%,内分泌系统占7.71%,消化系统占7.01%,免疫系统占5.26%,其他占3.86%。在疾病病程方面,慢性疾病占71.61%,急性疾病占28.39%。结论 高龄、居家慢性疾病患者是社区获得性压力性损伤的高发人群。医务人员应针对现状,构建合理的防治体系,早期采取有效的防治措施,减少压力性损伤的发生,减轻家庭及社会负担。
[关键词]社区获得性压力性损伤;防治;风险管理;对策
[中图分类号] R195.4 [文献标识码] A [文章编号] 1674-4721(2019)7(b)-0151-04
[Abstract] Objective To explore the characteristics of community-acquired stress injuries and to provide the basis for constructing reasonable prevention and treatment system. Methods A total of 856 patients with community-acquired stress injury who were admitted to Center Hospital of Jiangjin District in Chongqing City from January 2015 to December 2017 were investigated. The focus of the survey was age, source of patients, location of occurrence, stage, Braden score, type of disease and course of disease. Results In the aspect of age, patients who were below 50 years old accounted for 7.36%, 50-60 years old accounted for 6.89%, 60-70 years old accounted for 17.41%, 70-80 years old accounted for 32.01%, 80-90 years old accounted for 30.72%, over 90 years old accounted for 5.61%. In the aspect of source of patients, patients from their families accounted for 72.08%, old-age institutions accounted for 6.31%, and other hospitals accounted for 21.61%. In the aspect of occurrence, the proportion of injuries which occurred on head and neck was 0.26%; while that of chest and abdomen was 1.52%; waist and back was 6.14%; sacral tail, sciatic nodules, hip was 72.92%; scrotum, perineum was 1.25%; limbs was 16.78%; others was 1.12%. In the aspect of staging, injuries at stage 1 accounted for 21.73%, stage 2 accounted for 48.75%, stage 3 accounted for 14.53%, stage 4 accounted for 3.57%, deep tissue damages accounted for 4.49%, and injuries which could not be staged accounted for 6.94%. In the aspect of Braden score, 6-<10 points accounted for 20.91%, 10-<13 points accounted for 69.39%, 13-<15 points accounted for 3.50%, and 15-18 points accounted for 6.19%. In the aspect of types of diseases, the proportion of diseases related to respiratory system was 31.89%, while that of nervous system was 20.79%, cardiovascular system was 14.72%, exercise system was 8.76%, internal system was 7.71%, digestive system was 7.01%, immune system was 5.26%, and others was 3.86%. In the aspect of disease course, chronic diseases accounted for 71.61%, sudden illnesses accounted for 28.39%. Conclusion The high risk group of community-acquired stress injury is elderly patients with chronic diseases at home. It is necessary for medical staff to set up a reasonable prevention and treatment system on the basis of current situation. Constructing a reasonable prevention and treatment system in an early stage can effectively cut down the occurrence of stress injuries, reduce economic loss, and lessen family and social burdens.