The Model of Health Poverty Alleviation in Poor Mountainous Areas in Southwest China: A Case Study of "5+5" Model of Health Poverty Alleviation in Xundian County
2019-09-19WanyingDUZishengYANG
Wanying DU, Zisheng YANG
Targeted Poverty Alleviation and Development Institute, Yunnan University of Finance and Economics, Kunming 650221, China
Abstract Carrying out health poverty alleviation and ensuring the security of basic medical care for the poor are important contents for China to implement the strategy of targeted poverty alleviation and win the battle to get rid of poverty. Xundian Hui and Yi Autonomous County in Yunnan Province is a national poor county integrating "nationality, poverty, mountainous area and old revolutionary base area". In recent years, based on the actual situation, Xundian County has explored an effective way of health poverty alleviation. It has effectively prevented the phenomenon of poverty caused by illness and returning to poverty due to illness, and effectively ensured that Xundian County has successfully achieved the goal of getting rid of poverty. Xundian County finally got rid of the shadow of "poverty" for more than 30 years to become one of the first batch of counties in Yunnan Province to get rid of poverty. This paper makes great efforts to analyze and summarize the specific methods, main achievements, successful experience, lessons and reference about health poverty alleviation in Xundian County. At the same time, it also studies and analyzes the main problems existing in the model, and puts forward the corresponding measures and suggestions, in order to provide a reference for health poverty alleviation in other poor areas.
Key words Poor mountain area, Getting rid of poverty, Health poverty alleviation, Xundian Hui and Yi Autonomous County
1 Introduction
The implementation of the major policies of precisely helping the poor and accurately getting rid of poverty has become the mission of the times to promote the implementation of the 13th Five-Year Plan and to achieve the goal of building a well-off society in an all-round way by 2020[1]. In implementing the strategy of targeted poverty alleviation, it is necessity to steadily realize that the rural poor do not worry about food and clothing, compulsory education, basic medical care and housing security are guaranteed. It is the standard of China to get rid of poverty accurately and the overall goal of winning the battle of getting rid of poverty[2]. The guarantee of basic medical treatment is an important part of the poverty alleviation standard. An important connotation of building a well-off society in an all-round way is to let the masses be cared of in sickness and covered by medical insurance, so as to ensure the health of the people[3]. The 19th CPC National Congress raised the implementation of the strategy of healthy China to the strategic plan of winning the building of a well-off society in an all-round way and embarking on a new journey to the construction of a modern socialist country in an all-round way[4]. It can be said that without the health of the whole people, there will be no well-off society in an all-round way. Many studies have shown that low-income groups are more likely to develop major diseases than high-income groups. Even if the poor get out of poverty, they may be at risk of getting sick, leading to a return to poverty as a result of illness. At the same time, non-poor households also face the risk of becoming new poor households as a result of illness. Poverty and disease interact and go into a cycle over and over again through many connections. Therefore, health poverty alleviation will be a long-term key way of poverty alleviation[5]. The health poverty alleviation is an important battle against poverty. This is related to the vital interests of the masses and the overall situation of getting rid of poverty.
Xundian Hui and Yi Autonomous County is located in the northeast of Yunnan Province, north of Kunming City, inhabited by 25 ethnic groups including the Han, Hui, Yi, and Miao. It is one of the three autonomous counties of ethnic minorities in Kunming, one of the 59 old revolutionary base counties in Yunnan Province, and one of the 592 key counties in poverty alleviation and development work in China. Mountain areas and high and cold areas account for 87.5% of the total area of the county, integrating "nationality, poverty, mountainous areas, and old revolutionary base areas". In 2014, the county had 33 358 registered poor households and 127 960 poor people, with a poverty rate of 26.93%. Among them, 2 743 households and 3 095 people returned to poverty due to illness, and the rate of returning to poverty due to illness was 8.2%. Through the work of getting rid of poverty in recent years, by the end of 2017, 8 poor townships and 113 poor villages in the county had reached the standard of getting rid of poverty. The county has reduced the total number of poor people in rural areas by 126 311. The incidence of poverty fell from 26.93% in 2014 to 0.35% at the end of 2017. The per capita disposable income of rural permanent residents increased from 6 113 yuan in 2014 to 8 229 yuan. Great changes have taken place in urban and rural areas, and the living standards of farmers have improved significantly. The whole county as a whole reached the current standard of getting rid of poverty, and finally got rid of the shadow of "poverty" for more than 30 years to become one of the first batch of counties in Yunnan Province to get rid of poverty. Of the 594 households and 1 649 people in the county who did not meet the poverty alleviation standard at the end of 2017, 647 people returned to poverty due to illness, accounting for 39.2% of the people who did not meet the poverty alleviation standard. In order to effectively prevent poverty caused by illness and returning to poverty due to illness, according to the requirements ofNoticeoftheGeneralOfficeofKunmingMunicipalPeople’sGovernmentonPrintingandDistributingtheImplementationPlanof30MeasuresforHealthPovertyAlleviationinYunnanProvince[Kun Zheng Ban (2017) No.144], Xundian County considers the actual situation, studies and puts forward the "5+5" work model of health poverty alleviation. Through the implementation of this working model, it has explored a road of health poverty alleviation in line with the actual situation of Xundian County. By the end of 2018, the incidence of poverty in Xundian County had further dropped to 0.25%. This model has greatly improved the medical environment of the masses and improved the satisfaction and sense of gain of the masses. It has also provided valuable experience for other poor areas to promote health poverty alleviation.
2 Specific practices of the "5+5" model of health poverty alleviation
Xundian County has set up special "Health Assistance and Poverty Alleviation Sub-headquarters" under the "Xundian Poverty Alleviation Headquarters". This sub-headquarters closely focuses on strengthening the capacity-building of medical services and enhancing the capacity of public health services, and strives to implement the "5+5" work model, so as to effectively prevent poverty caused by illness, returning to poverty due to illness, and inaccurate evaluation.
2.1 Establishing and perfecting the "five guarantees" medical system(i) Basic medical insurance. Zero deductible is implemented for the registered poor people who are hospitalized in township health centers and shall be hospitalized in designated medical institutions in accordance with the norms of graded diagnosis and treatment and referrals. It increases the proportion of reimbursement for basic medical insurance for urban and rural residents. The proportion of reimbursement for normal medical expenses reached 95% in the first-level network settlement medical institutions, 85% in the second-level network settlement medical institutions, and 80% in the third-level network settlement medical institutions. Since 2015, 86.659 million yuan has been reimbursed for medical expenses of poor people in the county.
(ii) Serious illness insurance. The deductible for the reimbursement of serious illness of the registered poor people was reduced from 20 000 yuan to 10 000 yuan, a reduction of 50%. The maximum payment limit for serious illness insurance was raised from 98 000 yuan to 183 000 yuan. In a natural year, if the medical expenses paid by individuals of poor people exceed 10 000 yuan (including 10 000 yuan) within 30 000 yuan in a natural year, 50% of the expenses will be reimbursed; if the medical expenses paid by individuals of poor people exceed 30 000 yuan (including 30 000 yuan) within 40 000 yuan in a natural year, 60% of the expenses will be reimbursed; if the medical expenses paid by individuals of poor people exceed 40 000 yuan (including 40 000 yuan) within 50 000 yuan in a natural year, 70% of the expenses will be reimbursed; if the medical expenses paid by individuals of poor people exceed 50 000 yuan (including 50 000 yuan) within 250 000 yuan in a natural year, 80% of the expenses will be reimbursed. Since 2015, 3.346 million yuan has been reimbursed for serious illness insurance for registered poor people in the county.
(iii) Civil medical assistance. It cancelled the deductible of civil medical assistance for the poor, and the annual cumulative relief ceiling was not less than 100 000 yuan. Since 2015, the county’s registered poor people have gotten civil affairs relief of 4.572 million yuan for medical expenses.
(iv) Government is responsible for the most basic security. After reimbursement through basic medical insurance, serious illness insurance, and civil medical assistance, if the registered poor people meet the standards for referrals, the actual proportion of compensation for hospitalization expenses is less than 90%, and if the annual payment of medical expenses in accordance with the rules for referrals still exceeds the per capita disposable income of local rural residents, the government shall provide the most basic security for the difference. It ensures that the proportion of medical expenses paid by the registered poor in hospital does not exceed 10%, and that the proportion of out-patient expenses does not exceed 20%. The cumulative expenses paid by individuals in a year do not exceed the per capita disposable income of local residents. Since 2015, the government has guaranteed 12.888 million yuan in medical expenses for the registered poor.
(v) Temporary medical assistance. For the registered poor and low-income people in rural areas, after covered by the relief measures such as basic medical insurance, serious illness insurance, civil medical assistance and government insurance, if the cumulative annual self-payment of medical expenses within the scope of the policy may also result in "poverty caused by illness and return to poverty due to illness, temporary medical assistance will be given through the application of poor people themselves. In principle, the amount of relief per person per year does not exceed 20 000 yuan. Since 2015, 3.849 million yuan of temporary medical assistance has been provided for the registered poor people in the county.
2.2 Implementation of five preferential service policies(i) Free participation in insurance for all members. All the registered poor people participate in the basic medical insurance and serious illness medical insurance for urban and rural residents. Some of the individual contributions are guaranteed by the government at the most basic level. All the registered poor people enjoy the benefits related to urban and rural basic medical insurance and serious illness insurance. In 2017, 127 957 registered poor people participated in the basic medical insurance and serious illness medical insurance for urban and rural residents, 100% being insured, with a government subsidy of 23.032 million yuan.
(ii) "Diagnosis and treatment before payment" and "one-stop" settlement services. The service of "diagnosis and treatment before payment" will be carried out for the registered poor people to see a doctor in "health poverty alleviation designated hospitals" (county first people’s hospital, county traditional Chinese medicine hospital and 16 township health centers). There is no need to pay a deposit for hospitalization and treatment is given directly. Health poverty alleviation designated hospitals set up a "service window for the registered poor" and implemented a "one-stop" settlement service. The hospital makes a unified advance of all kinds of reimbursement compensation funds, and the registered poor patients only need to pay their own expenses. In 2017, 160 294 registered poor people went to see a doctor.
(iii) The centralized treatment services for serious diseases. Priority should be given to the centralized treatment of the registered poor people who suffer from childhood leukemia, congenital heart disease, esophageal cancer, gastric cancer, colon cancer, rectal cancer, end-stage renal disease, severe mental illness and so on. In 2017, there were 1 100 registered poor people suffering from 9 categories and 20 kinds of serious diseases in the county. According to the principle of "moving experts for patients", the county first people’s hospital unites with provincial and municipal hospitals to achieve 100% treatment for patients with serious poverty and serious diseases, and to achieve "one person, one file, one plan".
(iv) The family doctor service. The registered poor enjoy the service of family doctors. Basic medical, public health and agreed health management services are provided by a team of family doctors. In 2017, 179 family doctors were set up in the county for 127 957 registered poor households, to offer follow-up services for 511 828 people.
(v) Itinerant medical assistance services. Experts from municipal and county-level hospitals, doctors from township health centers and rural doctors form medical assistance teams to regularly provide free consultation, health guidance and other itinerant medical assistance services to the registered poor. In 2017, 16 urban hospitals in Kunming established a long-term and stable twinning relationship with 2 public hospitals in Xundian County and 16 township health centers. A total of 1 501 medical and technical mentors were sent to receive 12 516 poor patients, and 88 143 yuan of drugs were distributed free of charge. Two hospitals at the county level sent 670 medical and technical guidance personnel, to treat 5 222 poor patients, and distributed 51 885 yuan of drugs free of charge. The 16 health centers at the township level sent 870 medical and technical guidance personnel to treat 8 454 poor patients, and distributed 15 466 yuan of drugs free of charge.
3 Main outcome of "5+5" in health poverty alleviation
Through the implementation of the "5+5" work model of health poverty alleviation, the medical and health work in Xundian County has been continuously improved, and the infrastructure construction has been continuously strengthened. The standardization construction of township health centers and village clinics is up to the standard, and the standardized allocation of facilities and equipment is in place. This has greatly improved the medical environment of the masses, improved the medical conditions in poor areas, won the trust and unanimous recognition of the masses, improved the satisfaction and sense of gain of the masses, and effectively prevented the occurrence of poverty caused by illness and returning to poverty due to illness.
3.1 Comprehensively enhancing the satisfaction and sense of gain of the massesTwo public hospitals and 16 township health centers in the county are designated hospitals for health poverty alleviation, and "health service window for the poor" is set up to open a green channel to facilitate medical treatment. For poor people to see a doctor, "diagnosis and treatment first, paying later" service is implemented, with no need to pay hospitalization deposit, getting direct hospitalization treatment. This greatly facilitates the poor people to see a doctor. The health poverty alleviation designated hospitals built a "one-stop" settlement platform to realize the one-time settlement and reimbursement of patients’ medical expenses. A team of 224 family doctors was formed. A total of 127 957 registered poor people signed contracts with family doctors, with a signing rate of 100%. The team of family doctors provides basic medical care, public health and agreed health management services for the poor, which further enhances the satisfaction and sense of gain of the masses.
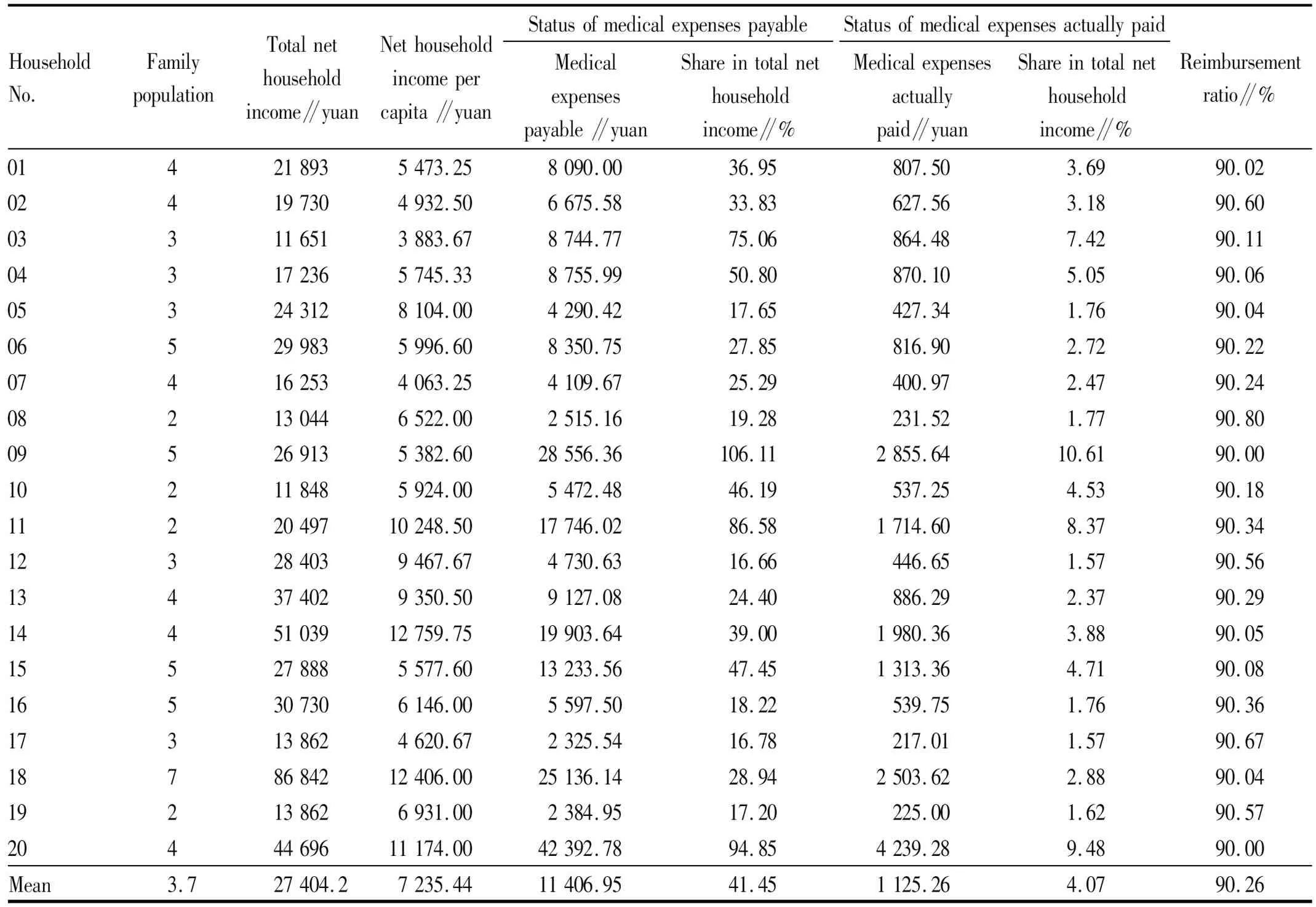
Through the investigation of medical expenses of 20 households suffering from serious illness in 2018, it showed that the medical expenses payable by these 20 households suffering from serious illness in 2018 were 41.45% of the total net income of families on average, with the lowest of 16.66% and the highest of 106.11% (that is, medical expenses payable exceed the total net household income). After reimbursement under the health poverty alleviation policy, the average proportion of medical expenses actually paid to the total net income of households was 4.07%, with the lowest of only 1.57% and the highest of only 10.61%. The proportion of reimbursement was more than 90% (Table 1).
3.2 Reducing the phenomenon of poverty caused by illness and returning to poverty due to illnessThe classified management should be carried out in strict accordance with the "three batches" (centralized treatment of serious diseases for a batch of people, chronic diseases contract management for a batch of people, and most basic serious disease security for a batch of people). Among the poor people in the county, the approved completion rate of the number of people returning to poverty due to illness has reached 100%. A total of 4 468 people were included in "three batches" of the national dynamic management system for health poverty alleviation, of which 985 people needed to be treated for serious diseases, and 985 people had been treated, with a treatment rate of 100%. A group of 3 481 people needed the contract for the chronic illness service, of which 3 472 signed contact, with a signing rate of 99.7%. A group of 2 people needed the most basic security for serious illness, and 2 people were supported, with a rate of 100%. Through the implementation of the "5+5" model of health poverty alleviation, the number of people returning to poverty due to illness in Xundian County has dropped from 3 095 in 2 743 households to 647 in 208 households. At the end of 2018, the incidence of poverty in Xundian County had dropped from 26.93% in 2014 to 0.25%.
Table 1 Questionnaire on the status of medical expenses of some households suffering from serious illness in Xundian County in 2018
HouseholdNo.FamilypopulationTotalnethouseholdincome∥yuanNethouseholdincomepercapita∥yuanStatusofmedicalexpensespayableMedicalexpensespayable∥yuanShareintotalnethouseholdincome∥%StatusofmedicalexpensesactuallypaidMedicalexpensesactuallypaid∥yuanShareintotalnethouseholdincome∥%Reimbursementratio∥%014218935473.258090.0036.95807.503.6990.02024197304932.506675.5833.83627.563.1890.60033116513883.678744.7775.06864.487.4290.11043172365745.338755.9950.80870.105.0590.06053243128104.004290.4217.65427.341.7690.04065299835996.608350.7527.85816.902.7290.22074162534063.254109.6725.29400.972.4790.24082130446522.002515.1619.28231.521.7790.80095269135382.6028556.36106.112855.6410.6190.00102118485924.005472.4846.19537.254.5390.181122049710248.5017746.0286.581714.608.3790.34123284039467.674730.6316.66446.651.5790.56134374029350.509127.0824.40886.292.3790.291445103912759.7519903.6439.001980.363.8890.05155278885577.6013233.5647.451313.364.7190.08165307306146.005597.5018.22539.751.7690.36173138624620.672325.5416.78217.011.5790.671878684212406.0025136.1428.942503.622.8890.04192138626931.002384.9517.20225.001.6290.572044469611174.0042392.7894.854239.289.4890.00Mean3.727404.27235.4411406.9541.451125.264.0790.26
3.3 Continuously improving medical and health workThe construction of medical infrastructure in Xundian County has been continuously strengthened, the standardized construction of township health centers and village clinics has reached the standard, and the standardized allocation of facilities and equipment has been put in place. This has greatly improved the medical environment of the masses and improved the medical conditions in poor areas. Through itinerant medical assistance services, poor households in remote areas can also be diagnosed and treated by high-level doctors. Through the policy of encouraging outstanding medical talents to flow to the grass-roots level, more and more high-quality medical talents go to the grass-roots level, so that the medical and health care at the grass-roots level can be significantly improved, and all kinds of work can be carried out more efficiently.
4 Successful experience of "5+5" model of health poverty alleviation
4.1 Leading and promoting by the government is the premise and guaranteeIn accordance with the requirements ofNoticeoftheGeneralOfficeofKunmingMunicipalPeople’sGovernmentonPrintingandDistributingtheImplementationPlanof30MeasuresforHealthPovertyAlleviationinYunnanProvince[Kun Zheng Ban (2017) No.144], the "5+5" model of health poverty alleviation is an effective policy measure for health poverty alleviation in Xundian County according to the actual situation of Xundian County in the process of implementing30MeasuresforHealthPovertyAlleviationinYunnanProvinceandWorkProgramforHealthPovertyAlleviationinKunmingCity. The operation of the whole model of health poverty alleviation is all based on the support and promotion of the government. All funds for health alleviation are invested by the government. Without government leadership, this model would no longer exist. Therefore, the leadership and promotion of the government is the premise and guarantee of the whole health poverty alleviation model.
4.2 "Five guarantees" and "five preferential treatments" are the central contentThe "5+5" model of health alleviation refers to the above-mentioned "five guarantees" and "five preferential treatments". This is the central content of this health poverty alleviation model. In short, the "five guarantees" include basic medical insurance, serious illness insurance, civil medical assistance, government’s most basic security, and temporary medical assistance. The "five preferential treatments" include free insurance benefits for all people, "diagnosis and treatment before payment" and "one-stop" settlement services, centralized treatment services for serious illness, family doctor signing services, and itinerant medical assistance services. The "five guarantees" and "five preferential treatments" are linked up and support each other, and jointly promote the development of health poverty alleviation work.
4.3 Laying emphasis on strengthening policy advocacy and guidance is a key measureVarious departments at all levels have actively formulated publicity work plans, extensively publicized them in a form that the masses are easy to understand and like to hear and see, stepped up publicity work, and raised the awareness rate of various policies and measures for health poverty alleviation. Various departments vigorously publicize the typical cases and achievements of health poverty alleviation, and create a good public opinion environment and social atmosphere. Through the signing service of family doctors and itinerant medical assistance services, various departments publicize the relevant health poverty alleviation policies to each household. Work teams stationed in villages, cadres in villages and those responsible for helping the poor should do a good job in publicizing policies, and at the same time issue relevant manuals. Only when the policy publicity is good, can farmers understand the policy, enjoy the policy and gain practical benefits from the policy. Placing emphasis on strengthening policy advocacy is an indispensable measure.
5 Implications and reference of "5+5" of health poverty alleviation
5.1 Solving the problem of heavy burden of seeing a doctor for the poor through institutional mechanism innovationIt encourages all localities to set up medical union (medical communities) and actively carry out pilot bundled payment projects. In accordance with the principle that "excess expenditure shall be borne by oneself, and the balance shall be set aside for other purposes", the funds for basic medical insurance, serious illness insurance, medical assistance, most basic security and family doctor signing services for the registered poor people or urban and rural residents in the region will be transferred to the leading hospital of the medical union (medical community). The leading hospital shall be responsible for the medical and health services and medical security of the poor or urban and rural residents. It shall ensure that the annual medical expenses paid by poor people in accordance with the rules for referrals do not exceed the per capita disposable income of local rural residents.
5.2 Establishing policies and measures to encourage the flow of outstanding medical talents to the grass-roots levelSenior professional and technical personnel or doctoral students majoring in medicine working in medical and health institutions at the county level shall be given a living allowance of 1 000 yuan per person per month. Full-time graduate students majoring in medicine shall be given a monthly living allowance of 800 yuan per person. For the senior professional and technical personnel or doctoral students majoring in medicine, full-time graduate students working in township health centers shall be given a living allowance of 1 500 yuan per person per month. Undergraduates who have passed the standardized training of general residents shall be given a living allowance of 1 000 yuan per person per month. Full-time medical graduates who have obtained the corresponding professional qualifications shall be given a living allowance of 1 500 yuan per person per month. Professional and technical personnel with professional titles at or above the county level and health technical personnel with the qualification of medical practitioners shall, from the year of working in villages and towns, who have worked continuously for more than 2 years (including 2 years), shall be given an annual job subsidy of 10 000 yuan per person. It actively strives for international support and continues to implement the recruitment plan for special general practitioners. It encourages doctors in public hospitals to practice in primary medical and health institutions in their spare time.
5.3 Paying attention to the construction of telemedicine service systemIn the first half of 2018, the unified layout of 16 township health centers in the county was completed in basic medical treatment, public health services, traditional Chinese medicine services, and management information systems for children and pregnant women. The health archives database of county residents has been built. Although the construction of telemedicine service system in Xundian County has achieved some results, we still have to strive to complete the construction of national health information platform by 2020. It is necessary to realize the interconnection of data such as electronic medical records, residents’ health records, and the health of the whole population, to achieve the application of full-service information systems in public health, family planning, medical services, medical security, drug supply, industry management, health services, big data mining, scientific and technological innovation, and so on. At the same time, it is necessary to complete the construction of medical imaging, clinical examination, ECG, pathology and other management systems. Relying on the provincial and municipal remote diagnosis and treatment system, it is necessary to build a remote diagnosis and treatment service system covering information sharing between medical institutions at the county and township levels.
5.4 Extensively implementing health promotion and health educationIn order to promote health poverty alleviation, we must first solve the problem of "prevention before illness", which requires that we should do a good job in health education for the whole people and strive to improve the health literacy of residents in poor areas. It is necessary to strengthen the construction of health education institutions and teams, and allocate 3 to 5 health education professional staff to build a health science popularization publicity platform. It is necessary to implement health literacy promotion action projects, and carry out health lecture tours, public service advertisements, health education on infectious diseases such as tuberculosis and AIDS, hypertension, diabetes and other chronic non-communicable diseases and endemic diseases. It is necessary to extensively carry out publicity and education on the basic knowledge and skills of residents’ health literacy. It is necessary to carry out health education for students, the elderly, patients with chronic diseases and other key groups, effectively improve the level of health literacy of residents, and guide the monitoring of health literacy of residents. By 2020, we should strive for the health literacy level of residents to reach 16%.
6 Problems in "5+5" of health poverty alleviation
6.1 Excessive pressure on health poverty alleviation fundsIn accordance with the requirements of the policy of getting rid of poverty, there are 130 202 registered poor people in the county. In 2017, the provinces, cities and counties invested 25.355 million yuan, of which 5 million yuan was invested at the county level. With the continuous growth of the demand of registered poor people for medical treatment, the government funds needed to help the poor will continue to increase in the future. In 2018, the county planned to invest 10 million yuan, and if the provincial and municipal investment is reduced, the county level investment will be more, with a problem of excessive financial pressure.
6.2 Inconvenient cross-regional treatment and reimbursementThe service of "diagnosis and treatment before payment" has been carried out for the registered poor people to see a doctor in "health poverty alleviation designated hospitals" (county first people’s hospital, county traditional Chinese medicine hospital and 16 township health centers). They don’t have to pay a hospital deposit. "One-stop" settlement service has been implemented, and the city’s medical insurance system automatically calculates the medical expenses of the registered poor patients. The hospital pays all kinds of reimbursement compensation funds in a unified way, and the patients only need to pay their own expenses. The registered poor patients from the surrounding Dongchuan, Songming, Luquan and other counties and districts will go to Xundian County health poverty alleviation designated hospitals for treatment. There is a problem that after the "one-stop" settlement, it is very difficult for hospitals to ask for advances from other counties and districts for health and poverty alleviation government funds. In Xundian County, some poor patients go to the surrounding counties and districts to see a doctor, but the county hospitals do not reimburse them in order to avoid the annoyance of demanding advance funds.
6.3 Service capacity of personnel in primary medical institutions still needs to be improvedDue to policy constraints, poor working conditions and low pay at the grass-roots level, the introduction of high-end talent is difficult. Even with the establishment of policies to encourage the flow of outstanding medical talents to the grass-roots level, many medical college students are reluctant to work as rural doctors. Occasionally, those who are working as rural doctors also flow out fast and it cannot retain talents. In addition, of the 524 rural doctors in the county, only 17 have obtained the qualification of assistant medical practitioners or medical practitioners. Other personnel are trained to obtain the qualifications of rural doctors, the professional and technical level is low, and the overall medical service level of the village clinic is not high.
6.4 "Two guarantees" are no longer in placeGovernment’s most basic security and temporary medical assistance were no longer implemented in 2019. An important background to the reasons why these "two guarantees" are no longer implemented is institutional reform. In order to meet the needs of social, political and economic development, it is a great adjustment and reform of the management system, function allocation, organization setup, staffing, as well as the combination mode and operation mechanism of these institutions. After the institutional reform, this part of the work of civil medical assistance has been transferred to the relevant departments of health insurance, and has been adjusted according to the relevant instructions of the provincial level. The "five guarantees" have actually become "three guarantees".
7 Policy recommendations
7.1 Increasing funding and ensuring that funds for health poverty alleviation are effectively spentFirst of all, it is necessary to raise the degree of attention paid by governments at all levels to the work of health poverty alleviation, increase investment and financial support for the cause of health poverty alleviation, and improve the accessibility of poor patients to medical treatment. At the same time, it is necessary to closely focus on the basic strategy of targeted poverty relief and targeted poverty alleviation, with the aim of standardizing the implementation of health poverty alleviation projects and improving the efficiency of the use of financial funds. It is necessary to establish an efficient, convenient and safe mode of project funding supervision to ensure that the projects in the field of health poverty alleviation are implemented. The health poverty alleviation funds should be effectively spent. In addition, special funds for health poverty alleviation should be increased to ensure the basic medical needs of the poor and the normal operation of medical institutions. According to the needs of health poverty alleviation, it is necessary to actively adjust and optimize the expenditure structure, invigorate the stock, make good use of increments, and strengthen the guarantee of health poverty alleviation funds. At the same time, it is necessary to strengthen the supervision of funds to ensure that funds for health alleviation are used in a standardized, safe and effective manner.
7.2 Establishing a settlement mechanism for medical treatment in different places and strengthening cooperation and collaboration among relevant cross-regional departmentsFirst of all, it is necessary to establish a settlement mechanism for medical treatment in different places and explore the methods of medical treatment in different places and settlement on the spot. Secondly, we should encourage and improve the linkage mechanism, aggregate resources to form a joint force, and effectively promote the implementation of work tasks. All departments at all levels should strengthen coordination and cooperation and form a working pattern of linkage between different departments and convergence between different tasks. It is necessary to improve the information-based level of health poverty alleviation work and strengthen information sharing among relevant cross-regional departments. When the registered households seek cross-regional medical treatment, the relevant basic data should be promptly fed back to the relevant departments of the place where the poor people’s residence is registered. The relevant departments shall reimburse the funds advanced by other counties in a timely manner.
7.3 Speeding up the introduction and training of high-end medical personnel and improving the level of medical and health servicesWe should have a comprehensive understanding of the significance of medical talents to the development of medical and health care, and create a good environment for the introduction of medical talents. It is necessary to take the initiative to recruit talents both inside and outside the county. It is necessary to expand our thinking and innovate the mode of introducing talents, such as signing contracts with relevant medical units and experts, and inviting well-known experts to come and guide them. It is necessary to "keep talents at work" and improve working conditions. It is necessary to "keep talents with better treatment" and improve the living environment, and to "keep talents with warm feelings" and improve the interpersonal environment. It is necessary to increase capital investment to improve the introduction of high-end medical talents. It is necessary to attach equal importance to the introduction and training, increase the investment in personnel training, and enhance the ability of personnel training. It is necessary to actively recruit and introduce medical and health personnel, strengthen the building of the team of rural doctors, increase the training of professional capabilities, and improve grass-roots medical and health facilities. Through the corresponding assistance of superior hospitals, we will constantly improve the ability of grass-roots medical and health services.
7.4 Ensuring that the registered poor households in sickness "obtain medical treatment and medical security"Although the "two guarantees" of government’s most basic security and temporary medical assistance are no longer implemented, it is necessary to ensure that the poor people in sickness can have medical treatment and medical protection. It is necessary to ensure that every registered poor person can enjoy the health poverty alleviation policy at all levels of province, city, and county. It is necessary to enable every poor person to "afford to see a doctor, get a good doctor, and have the money to see a doctor". In the work of health poverty alleviation, all relevant departments should make practical measures, do practical things, and get actual results in accordance with the working thinking of "precision as the core, implementation as the key, and ensuring sustainability". In this way, we can effectively ensure that the poor people can see a good doctor, afford to see a doctor, and have access to a doctor.
杂志排行

Asian Agricultural Research的其它文章
- Effects of Water-Soluble Fertilizer on Yield and Quality of Asparagus in Greenhouse under Chemical Fertilizer Reduction
- Effects of Microbial Pesticides on Prevention and Control of Cucumber Downy Mildew
- Difference of Regional Benefits after Linking Newly-added Cropland Quotas with Amount of Land Used for Construction Based on Targeted Poverty Alleviation: A Case Study of Xinjiang
- Inhibition Effects of Salvianolic Acid M and Rosmarinic Acid in Salvia deserta Schang on Human Aldose Reductase
- Outdoor Domestication Cultivation and Survival Mechanism for Tissue Culture Seedlings of Paeonia suffruticosa
- Ecological Compensation-assisted Relocation in Extreme Poverty-stricken Counties in China’s Ecologically Vulnerable Areas: Taking Dongchuan District of Yunnan Province as an Example