Induced pluripotent stem cells,a giant leap for mankind therapeutic applications
2019-08-28JosBraganJoAndrLopesLeonardoMendesSilvaJoMiguelAlmeidaSantos
José Bragança,João André Lopes,Leonardo Mendes-Silva,João Miguel Almeida Santos
José Bragança,João André Lopes,Leonardo Mendes-Silva,João Miguel Almeida Santos,Department of Biomedical Sciences and Medicine,University of Algarve,Faro 8005-139,Portugal
José Bragança,João André Lopes,Leonardo Mendes-Silva,João Miguel Almeida Santos,Centre for Biomedical Research (CBMR),University of Algarve,Faro 8005-139,Portugal
José Bragança,ABC - Algarve Biomedical Centre,Faro 8005-139,Portugal
Abstract
Key words: Induced pluripotent stem cells; Reprogramming; Cell-based therapy; Stem cell banking; Disease modelling
INTRODUCTION
In 2006,Kazutoshi Takahashi and Shinya Yamanaka reported for the first time the reprogramming of induced pluripotent stem cells (iPSC) from mouse somatic cells by forced expression of the transcription factors Oct4,Sox2,Klf4 and c-Myc,now termed Yamanaka factors[1].Subsequently,the Yamanaka factors,or other combinations of factors were successfully used to reprogram a wide range of mouse or human somatic cells into iPSC[2-5].iPSC achieve a high degree of dedifferentiation and acquire properties similar to those of embryonic stem cells (ESC).Indeed,iPSC and ESC are morphologically indistinguishable,andin vitrothese cells have the potential to differentiate into cells of the three germ layers (ectoderm,endoderm and mesoderm)and to originate virtually all cells of adult organisms.Like mouse ESC,mouse iPSC have the capacity to aggregate and integrate the inner cell mass,and participate in the development of an embryo upon injection into a host blastocyst and its subsequent transfer into a foster pseudo pregnant female.Additionally,iPSC which contribute to the germline have the potential to generate viable and fertile animals[6-9].
This novel reprogramming strategy applicable to human cells raised a great interest in the scientific and medical community,as iPSC represent an alternative source of pluripotent cells to human ESC.Moreover,iPSC present the advantage of being derived from somatic cells collected in a non-invasive manner,harbouring the individual's genetic background,thus being autologous and limiting immune rejections[10].iPSC also overcome ethical concerns associated to the derivation of human ESC from blastocysts.At present,advancements and refinements have been made to the original reprogramming procedure to circumvent some critical experimental issues,such as the delivery of the reprogramming factors with integrative vectors.Although Yamanaka factors are commonly used for reprogramming iPSC,other transcription factors,epigenetic regulators,microRNAs and/or small molecules have been shown to cooperate or substitute Yamanaka factors for the process.Reprogrammed cells are currently an invaluable tool forin vitrodisease modelling,high-throughput screens for drug discovery and toxicity tests.In addition,reprogramming raises the possibility for the derivation of patient-specific autologous cells for personalized therapies[11].Here,we introduce some of the challenges remaining to be faced to originate iPSC in a reliable fashion and with the quality required for safe clinical applications.We also present the current and future applications and therapeutic strategies involving iPSC to improve health.
CHALLENGES TO OVERCOME
The constant visitation to the initial reprogramming strategy by many researchers worldwide has led to the understanding of the molecular bases and to the improvement of the cell reprogramming process,bringing iPSC closer to safe clinical applications.However,the full translational potential of iPSC is still hampered by flaws,such as the inefficiency and the frequent incomplete reprogramming of the cells,andde novomutations occurring during the reprogramming process and during the cultivation of generated iPSC[5,12].The efficiency to reprogram somatic cells into iPSC remains low (often much less than 1%),and likely further decline in aged cells or in cells with a high number of divisions,and by the action of the reprogramming factors themselves which trigger a senescence-like response[13-16].Intriguingly,paracrine factors secreted by senescent cells have been reported to facilitate the reprogramming of non-senescent cells by Yamanaka's factors,in vivoin mouse tissues[17].In any case,the reprogramming of aged-cells and senescent cells has been successfully achieved and gave rise to rejuvenated iPSC with properties similar to those originated from young somatic cells[13,18,19].
Exhaustive studies of many iPSC worldwide have invariably indicated the existence of disparities in gene expression between iPSC and ESC,some of which may be attributed to genetic and epigenetic background variations already present in the somatic cells and ESC.However,the full impact of the minute number of differentially expressed genes in iPSC properties and specification during differentiation remains unknown.A variability in X chromosome inactivation and reactivation of human female iPSC has also been observed[5,20-23].Indeed,some human iPSC maintained the inactivation of the X chromosome during the reprogramming process,while others displayed both X chromosomes reactivated or with abnormal/partial reactivation.The stability of the X chromosome reactivation/inactivation may also vary with the cultivation of the cells overtime,the freezing and thawing processes required for the long-term conservation of these cells.This may result in a mixed population of iPSC displaying discrepant biological properties due to variable states of X chromosomes activation and inactivation.In addition,the inactivation of X chromosomes may occur randomly during differentiation[7].These points are of particular interest if iPSC are to be used to model early human embryonic development,X-linked diseases that depend on the activation of one or both X chromosomes and inherited sex-modulated disorders,such as autism[20-23].Moreover,teratoma formation assays,performed routinely to determine the pluripotency of iPSC,do not discriminate between chromosome X activation/inactivation status,and other specific tests have to be performed to determine X chromosome status[21].
De novopoint mutations and genetic variations occurring during the initial steps of the reprogramming process have been reported by several research groups[24-28].The mutations may not only occur in open chromatin regions including protein coding regions and transcriptional regulatory elements,but also in non-coding regions such as lamina-associated heterochromatin due to oxidative stress aggressions[24].Chromosomal aberrations,such as abnormal chromosome number have also been described in iPSC and ESC[29].Fibroblasts are commonly the favourite primary cell source for reprogramming,but these cells are very resistant to genomic alterations.Thus,cells less tolerant for the accumulation of mutations and genomic aberrations should be identified and preferably utilized for reprogramming.Mutations also accumulate in mitochondrial DNA of somatic cells with age,and are likely to limit the metabolic function and affect the energy supply in iPSC-derived differentiated cells,thus affecting their potential for disease modelling,drugs screens and therapeutic applications[30,31].
Another foreseen advantage of iPSC is the capacity to generate them for autologous purposes (Figure1),in order to produce cells tolerated by the host organism.However,this high expectation of immune tolerance was questioned by the elimination of mouse iPSC transplanted in isogenic mice[32].The immune responses were attributed to partial reprogramming and genomic instability of the iPSC,and the transplantation of terminally differentiated cells did not show immunogenicity[33].This observation suggests that differentiated cells from iPSC,which are the cells envisioned to be used in therapeutic approaches,would not trigger aggressive immune response in patients.Nevertheless,the immunotolerance of cells prepared autologously from iPSC has to be assessed and controlled for safe clinical applications,which may still require a preventive immunosuppression of the patients.Thus,for the safe use of iPSC in clinical,and even to model diseases faithfully,it is important to further understand the genetic and epigenetic mechanisms underlying the reprogramming process and obtain protocols to generate iPSC with the highest quality,and purity,and test their integrity and functionality.
PROMISING NON-THERAPEUTIC APPLICATIONS FOR iPSC
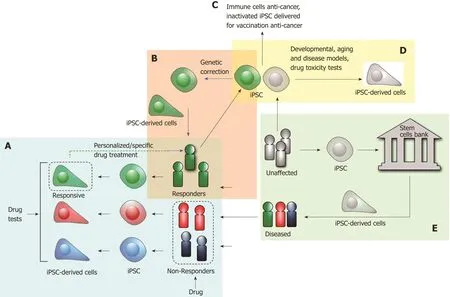
Figure1 Applications of human induced pluripotent stem cells.A: Pharmacotherapy can be optimized to the patients by testing the drugs on cells differentiated from patient-derived induced pluripotent stem cells (iPSC) to model the disease (blue panel).This approach may be used to determine the adequate treatment plan to specific patients and to limit side effects or non-responsiveness experienced by conventional clinical approaches supported by medical history and examinations,and test results to implement the treatment based on generic clinical approaches; B: iPSC-derived from patients may also be corrected for genetic defects and consequently used to treat the patients in cell-based or regenerative therapies (orange panel); C: iPSC may be used to derive immune cells to eliminate cancer cells,or to be inactivated and injected to vaccinate people against cancer cells; D: iPSC used to study developmental processes,model diseases and test drugs to assess toxicity in specific cell types (yellow panel); E: iPSC originated from non-diseased individuals are being characterized and preserved in Biobanks worldwide for allogenic cell-based therapies in HLA matched patients (green panel).iPSC: Induced pluripotent stem cells.
iPSC technology allows the reprogramming of cells from individuals in the context of their genetic background,and the genetic and epigenetic behaviours of iPSC have been showed to reflect those of the proper cells of a donor individual[34,35].Therefore,iPSC are considered a great tool to model human diseases,and if reprogrammed from cells of a patient with genetic variations causing the disease,iPSC have the potential to generate cells or tissue-like structuresin vitromimicking those of the patient affected by the disease of interest (Figure1).However,inter and intra-clonal (epi)genetic variability of iPSC acquired during reprogramming and or the differentiation process may confound the results and the outcomes of experiments or therapies involving iPSC.A thorough analysis of iPSC and other control cells,such as the original cells used for reprogramming,have to be performed.For instance,the comparison of several iPSC lines obtained from different donors and control cells is recommended to reliably appreciate the impact of the genetic variations in the disease and to limit the variability in the outcomes which is inherent to iPSC clones'differences.The correct differentiation of iPSC into the target cells relevant to model the disease of interest is also critical,and is often hampered by the limited knowledge about the experimental conditions leading to the proper cell differentiation and the variability existing in the differentiation processes[35].The major challenge for disease modelling using iPSC remains to establish the right cell type(s) with a phenotype which represent accurately the pathological aspects of the disease of interest.Another interesting feature is that iPSC are pluripotent and their differentiation can be triggered in order to mimic early steps of embryonic development,which make them a cell source of choice to study congenital or early age onset diseases (Figure1).Many groups have already used iPSC to model the pathophysiology of a variety of diseases,such as cardiovascular diseases,neuronal and neurological disorders,and cancer amongst others[34-36].However,for diseases which are multigenic and/or agedependent with late onset,or complex and systemic,iPSC may be more difficult to use for establishing a disease model[35,37].Organoids,which are 3-dimensional cellular structures mimicking the organization and functions of organs or tissues,may also be generated by differentiation of iPSC to obtain more complex cellular modelsin vitro.In addition,iPSC are also an invaluable tool to study the genetic pathways involved in diseases in well-controlled environments,and to test the effect of novel and known drugs in patient-derived iPSC (Figure1).
Interestingly,primary cancer cells from different types of human cancers,such as melanoma,gastric cancer,glioblastoma and pancreatic ductal adenocarcinoma,among others,have been successfully reprogrammed into iPSC or at least into pluripotent cells,offering new possibilities to study early stages of cancer initiation and progressionin vitro[38,39].iPSC might be especially useful to model cancers emerging at young ages or with familial inherited characteristics,since these cancers have an early onset which may be promoted by the embryonic developmental process itself,which is recapitulated to a large extent during iPSC differentiation.An obvious limitation to this model is that it fails to be submitted to environmental factors such as chemical pollution,smoking and virus infection,among others,that may contribute to tumorigenesis.Another limitation comes from the fact that iPSC reprogramming process changes the epigenetic status of the original source cell,which in the case of cancer cells may also contribute to their tumorigenic nature.
iPSC can also be used for toxicity tests and drug discovery screening studies to treat diseases in a more personalized manner[40].Indeed,numerous studies have indicated that iPSC recapitulatein vitrothe response of the cell-donor individuals to drug expositionin vivo.This observation implies the possibility to perform highly accurate and personalized preclinical trialsin vitrousing iPSC or iPSC-derived cells (Figure1).Since pre-clinical phase trials are critical to decide about the progression of drug development for clinical applications,thorough experiments and control methods have yet to be implemented and standardized to test new drugs[41].In 2011,the US Food and Drug Administration/FDA has established a set of guidelines to manufacture and evaluate the quality of cells and tissues derived from stem cells for patients' regenerative medicine applications,but do not make recommendations for the use of cells forin vitroassays.The International Society for Stem Cell Research/ISSCR has also released recommendations to guide physicians,ethical committees and review boards to evaluate early-phase stem cells based clinical trials(“Stem Cell-Based Clinical Trials: Practical Advice for Physicians and Ethics/Institutional Review Boards”,http://www.isscr.org/docs/default-source/clinical-resources/isscr-stem-cell-based-clnical-trials-practical-advice_final_23jan2018.pdf?sfvrsn=2).However,these efforts to prepare guidelines and recommendations to set gold standards and to evaluate the quality of products derived from iPSC,or stem cells in general,forin vitro(pre) clinical assays and drug toxicity testing have to be continued to reach a safe and reliable use of stem cells.
REPROGRAMMING CELLS FOR ANTI-AGING AND CANCER TREATMENT
An interesting concept of cell-aging reversionin vivo,which has allowed to prolong the lifespan of a mouse model of premature aging,has also emerged with the reprogramming technology[42].Indeed,the short-term exposure to Yamanaka factors has contributed to a partial reprogramming of cells,and amended the physiological and cellular hallmarks of aging,due to a probable remodelling of the epigenetic marks which are acquired during aging[42].Further understanding of the partial reprogramming timings and markers may harness balanced conditions to obtain rejuvenated cells with a full potential to perform their functions and with a minimal dedifferentiation state to avoid oncogenic risks[43].Partial reprogramming approaches and the consequent epigenetic rejuvenation may serve to develop future interventions for the treatment of age-related diseases,improvement of health and longevity[42,43].
Recently,the potential of iPSC for immunotherapy was explored,with a particular interest in the quest for treatment of cancers[44].Indeed,iPSC were used to derive human dendritic cells and macrophages which have a potent antigen presenting activity with the capacity to activate T-cells,thus presenting a great potential to be used for cancer immunotherapies.Indeed,iPSC reprogrammed from T-cells (isolated from peripheral blood mononuclear cells) have been shown to retained the expression of the original T-cell receptor/TCR rearrangement[45].Thus,these cells could be a source for illimited production of specific clones of T-cells,bypassing their residence in the thymus for their development and maturation.Human tumour antigen-specific cytotoxic T-cells have also been generated by several groups,and iPSC can also be engineered to harbour chimeric antigen receptors/CAR targeting cancer cells[46].Natural Killer cells harbouring CAR constructs targeting tumours have also been generated from iPSC,and showed to inhibit the growth of tumoursin vivo[47].These approaches may serve to develop effective treatments for refractory oncologic malignancies.Furthermore,a recent report has showed that iPSC may express tumour-associated antigens and be used for autologous tumour vaccination[48].Indeed,the injection of irradiated mouse iPSC and adjuvant CpG (successfully used in tumour vaccination) in mouse,triggered a strongin vivoimmune response which controlled the tumour growth from breast cancer,melanoma and mesothelioma injected cells.Thus,the injection of irradiated-iPSC led to the instatement of a broad anti-tumoral immune status able to restrain the development of multiple cancers without any overt adverse effect[48],suggesting that this approach has the potential to be translated in clinical applications.
ONGOING CLINICAL TRIALS
Many promising therapeutic applications are currently being tested in preclinical experiments using iPSC-derived cells for their potential to generate functional cells able to replace damaged or dysfunctional tissues in patients[49].However,the era of human clinical trials using iPSC-derived cells has already started.Indeed,the first reported clinical trial involving iPSC-derived cells was designed to treat the Age-Related Macular Degeneration (AMD),a disease that affects the macula of the eye and results in the blur of the central vision[50,51].In 2013,sheets of retinal pigment epithelial(RPE) cells,differentiated from patient-derived iPSC,were transplanted into the eyes of a patient suffering AMD.Six months after transplantation,the patient visual treatment acuity was improved with no safety-related concerns.However,as the second trial participant was ready to start,two mutations,that were not present in the original reprogrammed fibroblasts,were detected in the RPE cells used to treat the first patient.While further analysis revealed that the risk of carcinogenesis was low,the study was halted and only resumed in 2016.The first formal trial using iPSC was approved in 2016 when Cynata Therapeutics launched the first clinical trial using an allogeneic iPSC-derived mesenchymal stem cell called CYP-001[51].Cynata Therapeutics just recently concluded the Phase 1 clinical trial of CYP-001 for the treatment of steroid-resistant acute graft versus host disease/GvHD,and the results showed positive safety and efficacy data for the treatment of the disease.Cynata Therapeutics is currently planning a phase 2 trial.In 2018,the Kyoto University announced the first clinical trial to treat Parkinson's disease using iPSC-derived dopaminergic progenitors to be transplanted into human patients.The objective of this trial will be to evaluate the safety and efficacy of the transplantation of iPSC-derived dopaminergic neurons into the brain of Parkinson's disease patients[52-54].In the oncological front,the American Company Fate Therapeutics has recently approved the usage of a NK cell-based cancer immunotherapy for the treatment of advanced solid tumours with cells derived from a clonal master characterized iPSC line[55].This study is expected to evaluate the safety and tolerability of multiple doses of these cells in subjects who have progressed or failed with immune checkpoint inhibitors therapy.Recently,a clinical trial has been approved to generate sheets of cardiomyocytes that surgeons plan to implant into the heart of three patients with heart diseases[56].While some companies and researchers are patiently waiting for the results of clinical studies concerning the iPSC regenerative potential,others are currently looking into other therapeutic strategies.For instance,with CRISPR-Cas9 technologies,stem cell biologists are attempting to repair mutated genes in human iPSC before using iPSC-derived cells to treat the patients.
iPSC BANKING
The use of iPSC for autologous therapeutic purposes seems more appropriate,since the cells derived from the patient should present a reduced risk of immune rejection[10].However,in light of recent findings,an autoimmune reaction to iPSC-derived cells may not be completely avoided[57].In addition,the use of iPSC from patients for autologous purposes may,in many cases,require the correction of genetic defects that contribute to the pathology (Figure1).On the other hand,having allogenic iPSC already generated,characterized and tested for the absence of contaminating agents and for the integrity of the (epi)genome would save time in the preparation of iPSC-derived cells needed for engraftment and treatment of patients.In this case,the human leucocyte antigens/HLA of iPSC should be typed in order to be able to quickly match the cells with the patients in need[58,59].In principle,this strategy would reduce the costs and the number of “off-the-shelf” iPSC samples that could be stored in biobanks.Indeed,a few hundreds of homozygous iPSC lines could provide a match for more than 90% of genetically homologous populations[60,61].However,banking the total number of iPSC necessary to match all haplotypes of multi-ethnic populations with genetic heterogeneity,such as the population of North America,may be much more challenging and costly[62].Nevertheless,a number of banking initiatives,both to store iPSC for research and clinical purposes,are in progress in Europe,Asia and North America,with coordinated standards to have a well-documented,traceable and quality controlled repository of iPSC[59,63].However,the banking initiatives do not reach a consensus in the general public and scientists,since there are only a few clinical trials ongoing with results that remain to prove that iPSC-derived cells are useful for successful therapies.In addition,there is a debate on which financial entities (private or public) should support the high costs of these initiatives[64].It is also important to set high standard regulation and quality control for iPSC production,characterization and cell preservation,as well as their use in clinical environments.Finally,it is also utterly important to provide the general public,and patients in particular,all the necessary information about the procedures and the risks associated to the use of iPSC-derived cells,the limitations of these novel approaches,and to be realistic with the expectations of the patients.
CONCLUSION
The ability to generate pluripotent stem cells,iPSC,from human somatic cells using a simple experimental approach easy to implement,has undeniably opened new possibilities for modelling diseases and to undertake developmental studies that could never have been performed before (Table1).The bulk of the molecular mechanisms involved in the reprogramming process has been largely unveiled,which has already allowed great improvements in the iPSC generation process.Consequently,iPSC have achieved a quality sufficient to be used in novel clinical approaches.The use of patient-derived iPSC offers the possibility to develop and test patient-specific pharmacotherapies and derive stem cells which may be corrected for genetic defects before their use for autologous purposes (Figure1).In the field of cancer,the study of iPSC biology and their reprogramming mechanism has not only provided new insights in epigenetic changes contributing to cancer,but has positioned iPSC as a cell source to originate immune cells with great potential for the development of immunotherapies against cancer.The inactivated iPSC themselves are now thought to be instrumental for future vaccinations and to provide protection against cancers.
Even studies of incomplete reprogramming processes of iPSC have provided new means to revert aging in cells and paved the way for future research directions aiming to treat age-related diseases and to improve health in longevity.In prevision of their future potential use in therapies,stem cells and iPSC research communities are coming together to set up guidelines and recommendations to delineate the best approaches and practices to obtain and characterize iPSC with the highest quality necessary to derive cells for clinical applications.Efforts are also made worldwide to organize biobanks with traceable information and quality to store iPSC,that would be ready for prompt clinical interventions.There is no doubt that iPSC technology has helped basic and clinical researchers to make a leap forward in many fields of basic and applied research,including cell-based therapies.This relatively recent and evolving technology has rapidly opened a conduit between the bench and the bedside,and is already the object of several pioneering clinical trials to treat various diseases,including neurodegenerative diseases.Although these clinical assays may seem premature to many scientists and clinicians,their results are awaited with high expectations and will be determinant to accelerate and diversify clinical interventions based on iPSC-derived cells.
Although many technical hurdles remain to be surpassed for iPSC technology to fully reach its potential.In just over ten years after its first development this technology has remarkedly led to several clinical applications,and provide new ways of obtaining disease modelsin vitroto better study the mechanism of human pathologies and to improve patients' treatment in a more adequate and personalized manner.Thus,iPSC technology has already been “a giant leap” in terms of obtention of human cells with incredible versatility and potential for therapeutic applications.
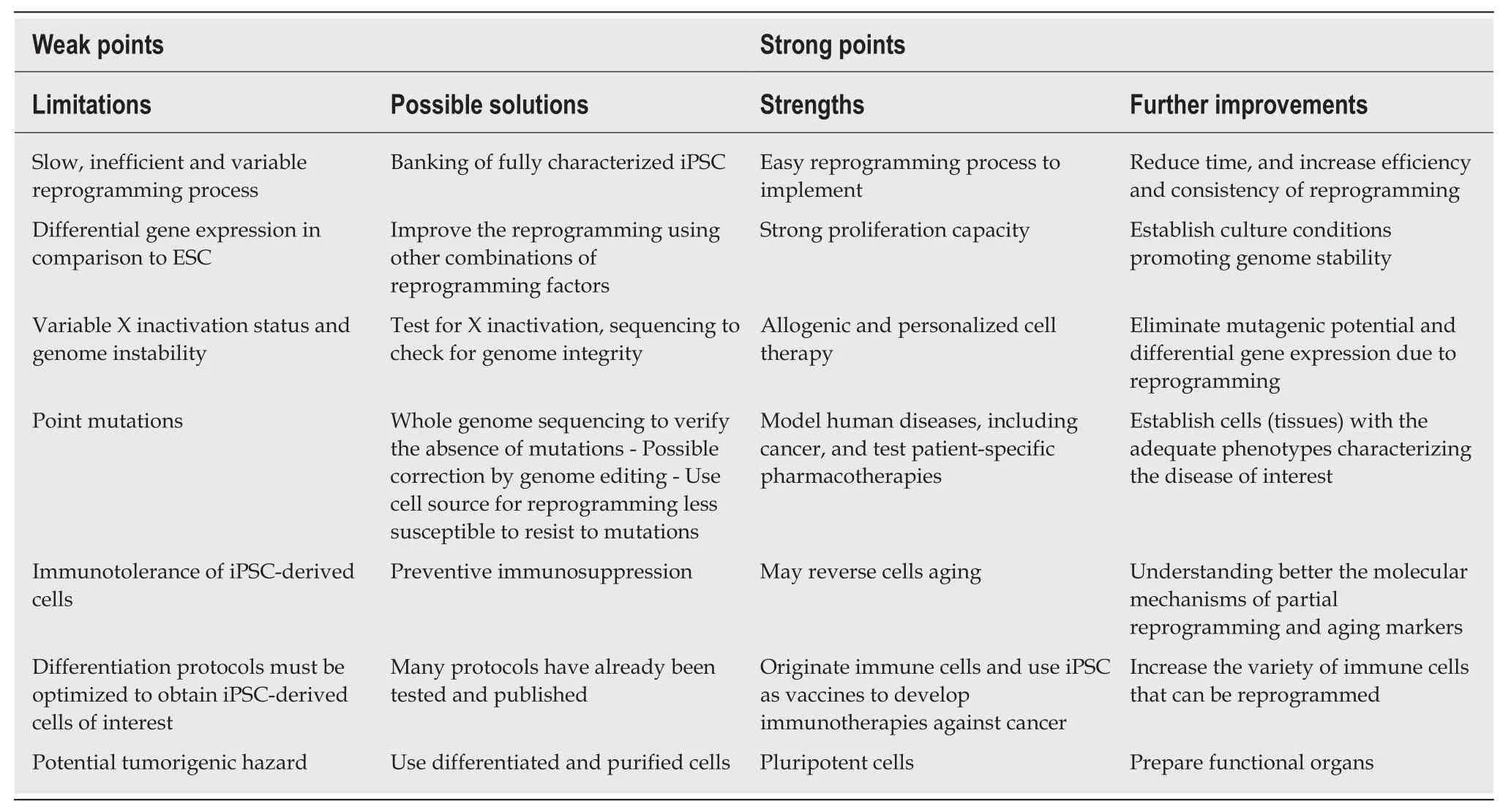
Table1 Some weak and strong points of induced pluripotent stem cells technology
ACKNOWLEDGEMENTS
The authors thank José António Belo (New University of Lisbon),Rui Gonçalo Martinho (University of Aveiro) and Clévio Nóbrega (University of Algarve) for insightful discussions.
杂志排行

World Journal of Stem Cells的其它文章
- Presence and role of stem cells in ovarian cancer
- Targeting cancer stem cells in drug discovery: Current state and future perspectives
- Using transcription factors for direct reprogramming of neurons in vitro
- Predicting differentiation potential of human pluripotent stem cells: Possibilities and challenges