Presence and role of stem cells in ovarian cancer
2019-08-28NatasaKendaSusterIrmaVirantKlun
Natasa Kenda Suster,Irma Virant-Klun
Natasa Kenda Suster,Department of Gynecology,Division of Obstetrics and Gynecology,University Medical Centre Ljubljana,Ljubljana 1000,Slovenia
Irma Virant-Klun,Department of Human Reproduction,Division of Obstetrics and Gynecology,University Medical Centre Ljubljana,Ljubljana 1000,Slovenia
Abstract
Key words: Ovarian cancer; Cancer stem cells; Very small embryonic-like stem cells;Epithelial-mesenchymal transition
OVARIAN CANCER
Ovarian cancer is the leading cause of death amongst all the gynecological tumors affecting a large population of women worldwide.According to National Cancer Institute data from the United States of America,incidence between 2008 and 2014 was 11.6 per 100000 women per year.As the five-year surviving rate in this period only reached 47.4%,the number of deaths increased to 7.2 per 100000 women per year.
Ovarian cancer presents a heterogeneous group of tumors: Epithelial,germ cell,and stromal cell tumors.Approximately 90% of ovarian cancer belong to the malignant epithelial tumor (carcinomas) group and,based on histopathology,immunohisto-chemistry,and molecular genetic analysis,five main types of carcinoma are currently known: high grade serous carcinoma,70%; low grade serous carcinoma< 5%; endometrioid carcinoma,10%; clear cell carcinoma,10%; and mucinous carcinoma 3%[1,2].Different epithelial malignancies have,in addition to their different origin and morphologies,different biological behaviour[3].Low grade serous carcinoma arises from fallopian tube,endometrioid carcinoma,clear cell carcinoma,and seromucinous carcinoma arise from endometriosis,mucinous carcinoma arises from germ cells,and malignant Brenner tumor arises from transitional epithelium[3].All are slow-growing tumors which develop progressively from benign and borderline precursor lesions to malignancy[4].They are genetically stable,characterized by mutations in different genes:KRAS,BRAF,PTEN,ß-catenin,and others[4].High grade ovarian serous carcinoma,on the other hand,has a high level of genetic instability and is characterized byTP53mutation,and loss of BRCA1 and BRCA2 function[3].It is fast-growing and highly aggressive neoplasm,with massive disease in the omentum and the mesentery,usually accompanied by ascites[3].There are two models considered,high grade ovarian serous carcinoma arising from the ovarian surface epithelium or from the fallopian tube[5].As both tissues are derived from the same embryologic origin,high grade ovarian serous carcinoma may arise from two different sites that undergo similar changes[5].Progenitor cells from different sites may respond similarly[5].However,BRCA deficiency and simultaneously presence of the intraepithelial carcinoma in the fallopian tube (serous tubal intraepithelial carcinoma) make fallopian tube model of high grade ovarian serous carcinoma origin more relevant[3,5].
爸爸说现在森林里的人太多了。劳拉常常听到斧头砍在树上发出震耳的嘭嘭声,那可不是爸爸在砍树;也常常听到枪声在森林中回荡,那也不是爸爸在打枪。木屋旁的小路已经被人踩成了大路。几乎每一天,正在玩耍的劳拉和玛丽都会停下来,惊讶地看着马车发着嘎吱嘎吱的声音从这条路上缓慢地通过。
Pursuant to insufficient screening and nonspecific symptoms,such as abdominal discomfort and bloating,early diagnosis of the disease is challenging[6].Consequently,70% of ovarian cancer patients are usually diagnosed at advanced stages (III and IV),with metastatic sites disseminated widely within the peritoneal cavity,retroperitoneum,and even in distant organs[7].Treating disease in its advanced course is demanding and often unsuccessful,so defining the origin of ovarian cancer and performing suitable prophylactic surgery like oophorectomy or salpingectomy may save many lives[8].
To achieve complete removal of macroscopic tumors,patients with advanced disease receive radical debulking surgery in combination with neoadjuvant and/or adjuvant platinum and taxane combined chemotherapy[9,10].The majority of patients initially respond well to treatment; however,tumors eventually relapse in over 70% of cases,resulting in chemoresistance and fatal disease[11].The general opinion is that the microscopic tumor residue that remains after surgical debulking and standard chemotherapeutics' limitations contribute to the likelihood of tumor relapse.Therefore,the five-year survival rate for advanced tumors is less than 30%,with only modest improvement in survival evidenced in recent decades[12,13].
Recent findings in the field of cancer stem cells (CSCs) in ovarian cancer are important,in terms of its explanation of tumor initiation pathogenesis,dissemination and recurrence after treatment,and also in terms of using CSC components as targets for ovarian cancer target therapy[11,14].In this review article,we will discuss the current research on CSCs in ovarian cancer,focusing on CSCs development and their role in tumor formation,progression and recurrence after,allegedly,successful treatment.
OVARIAN CSCs
The CSC model proposes that tumor initiation,growth and progression are fueled and sustained by undifferentiated cancer cells endowed with self-renewal on the one hand and differentiation on the other[15].Ovarian carcinoma,based on its biological behavior and clinical course,represents a typical example of CSC-driven disease[15].It is a highly aggressive cancer which spreads widely within the abdominal cavity and distant organs,even when primary ovarian tumors are still small and barely detectable.Despite aggressive treatment with debulking surgery and cytostatic chemotherapeutics,which at first reduce the size of tumors and temporarily improve patient signs and symptoms,ovarian cancer relapses in over 70% of all cases.It is believed that a highly-potent subpopulation of ovarian CSCs that “survive” treatment cause disease relapse[16].Moreover,dormant ovarian CSCs able to repopulate again,lead to even more aggressive,drug-resistant disease[16].The phenotype and molecular status of ovarian CSC population have still not been defined.It is known that CSC phenotype is not uniform amongst the various cancer types and even of those tumors of the same histological type,and it can changevis à vis in vitroculture condition[17].Ovarian cancer manifestation seems to involve different types of stem cells interplaying in this complex process.Cells heterogeneity within tumors may influence disease course and its response to treatment in terms of drug resistance[18].We know little about ovarian CSC location and CSC progenitors,but recent studies have aided in understanding CSC evolution and location within tumors[19,20].An important task for the future is to determine the population of progenitor stem cells involved in ovarian cancer formation and progression.
ROLE OF CSCs IN OVARIAN CANCER PATHOGENESISWITH RESPECT TO VERY SMALL EMBRYONIC-LIKE STEM CELLS
The exact mechanisms by which normal ovarian cells transform into aggressive ovarian cancer cells still remain elusive.As with other adult tissue and organs,different research groups have detected very small embryonic-like (VSEL) stem cells with diameters of up to 5 μm in human adult ovaries[21-23].These cells have been further characterised and differentiatedin vitro[21-23].It has been proposed that these small stem cells originate in the embryonic epiblast and remain dormant in adult human tissue and organs from the embryonic period of life[24].VSEL stem cells in ovaries are mostly located in the ovarian surface epithelium of healthy women[22].They express several genes related to pluripotency and germinal lineage,especially primordial germ cells[25].
她继续失踪从未和他联系。他回到澳洲。如常开始工作,运动,与年轻女孩重新约会,与她们上床。却始终无法忘记炎热的万象,在旅馆房间铺着刺绣白床单的单人床上,那个脖子后面有汉字刺青的女子。她的神情冷淡奇幻。她说的话他总是无法理解。她的身体一直在对他发出呼唤。他的心在某种被禁锢般的思念中碎裂。开始终日隐隐作痛。
Small tumor-initiating stem cells were also discovered in the ovaries and ovarian cell cultures of patients with borderline ovarian tumors[26].These cells spontaneously formed tumor-like structuresin vitroand,after fluorescence-activated cell sorting,evidenced different gene expression profile in comparison to their counterparts from healthy,non-malignant ovarian tissue[26].Results revealed that SOX17,forkhead box(FOXQ1,FOXL2),and homeobox (HOXD9) genes,known to regulate the cell growth,proliferation,differentiation,embryo development,and the establishment of body axes during embryogenesis,may play an important role in the transformation of“healthy” small stem cells into “cancerous” cells[26].Amongst the multitude of interesting genes,MUC16/CA125,the most widely-used ovarian cancer biomarker,was highly upregulated in small putative stem cells from borderline ovarian tumors in comparison to cells from healthy ovaries,hESCs,and fibroblasts[26].Interestingly,the small stem cells from healthy ovarian tissue did not form tumor-like structuresin vitro[26].A similar population of small stem cells was later on observed in situ in ovarian serous carcinoma slides[20,27].A population of small stem cells with diameters of up to 5 μm contain NANOG-positive cells with nuclei,which made up almost all cell volume,and were clearly seen amongst the epithelial cells of the ovarian surface epithelium[27].In this vicinity,there was also present a population of bigger round cells with diameters of 10-15 μm with similarly large nuclei,positively stained for mesenchymally-derived cell (vimentin) and pluripotency (NANOG,SSEA-4,and SOX2) markers[27](Figure1).Different stem cells observed in ovarian tumor tissue indicate the presence of different types of stem cells in ovarian cancer.Smaller stem cells resembling VSEL stem cells are suggested as progenitor stem cells which remain dormant from the embryonic period of life to regenerate damaged tissue,but can,in cases of inappropriate body condition,transform into bigger-CSCs involved in cancer manifestation.
Other researchers,likewise focusing on ovarian CSCs,observed similar cells,smaller spherical with diameters of up to 5 μm and larger elliptical or fibroblast like with diameters of up to ≥ 10 μm,both with stem cells characteristics[19,28].Cells with coexpression of stem cell markers (OCT4,SSEA4),CSC markers (ALDH1/2,CD44 and LGR5) and proliferation marker (KI67)[19]were evidenced in the ovarian cortex.Interestingly,in a few cases,only non-proliferating stems or CSCs (SSEA4+/KI67- or ALDH1/2+/KI67-),or only proliferating (KI67+) cells were observed,which indicates a dynamic process in which different populations of cells are involved forming fascinating cellular hierarchy[19].
ROLE OF EPITHELIAL-MESENCHYMAL TRANSITION IN TUMOR FORMATION,INVASION,METASTASIS AND CHEMORESISTANCE
Many studies report that ovarian carcinogenesis is associated with epithelialmesenchymal transition (EMT)[19,27].Based on our own experimental experience and data from the literature,we suggest that small,spherical VSEL stem cells present amongst epithelial cells in the ovarian surface epithelium induce EMT by growing into larger (diameter approximately10-15 μm),NANOG and vimentin-positive spindle/elliptical shaped cells,and transform into mesenchymal-like stem cells(Figures 1 and 2); surrounding epithelial cells are not excluded from the EMT process and support it in unknown ways[27].Different signals from tumor microenvironment might be involved in a network of interactions that activate so-called EMT programs[29-31].Cancer cells are,beside epithelial cells,surrounded by a large variety of stromal cells,such as fibroblasts,myoblasts,lymphocytes and macrophages,and endothelial cells and pericytes recruited to tumor vasculature[32].Paracrine and juxtacrine signals in such microenvironment include different members of the transforming growth factor superfamily,epidermal growth factor,fibroblast growth factor,hypoxia-inducible factor,Wnt,Notch,and many others[33].
EMT is also considered a key step in CSC metastases[41].Mesenchymal properties,acquired by carcinoma cells during EMT,promote invasion into the extracellular matrix and further dissemination.Transformed tumor cells spread throughout the organism,where they present a reservoir that expands and refills cancer cell populations[42].Circulating tumor cells with a fully-mesenchymal state display lower metastatic potential compared to hybrid epithelial/mesenchymal cells undergoing partial EMT[43].Interestingly,not all cancer cells are able to undergo EMT at the same time and even those which have activated EMT may not be sufficient for metastasis[44].Furthermore,in cases of colorectal cancer,it has been shown that EMT occurs only in a subset of cells at the invasive front of primary carcinoma,usually associated with stromal components[45].
2.企业在信息平台建设中的职责和权利。职业经理人信息平台建设主要是为企业的人才需求而服务,企业是最大的受益者,所以企业的职责主要包括提供职业经理人真实绩效技能信息、兑现职业经理人的劳动合同、查询企业拟选聘职业经理人信息等。
Epithelial trait loss and mesenchymal characteristic acquisition,such as vimentin and myosin presence,which occurs during EMT,enable invasive cellular motility which enhances tumor progression[39].Elliptical fibroblast-like cells with stem cell characteristics and positive pluripotency and mesenchymally-derived cell markers seen in high grade ovarian serous carcinoma,invaded ovarian tissue by changing their round shape into mesenchymal-like phenotype involving elongations and protrusions[27].By promoting high degrees of cell invasion,EMT increases tumor malignancy[36,40].
EMT is a basic physiological cell reprogramming event active in tissue remodeling during embryogenesis and,later in life,during the regeneration of adult tissue in cases of injury.During EMT,cells acquire unique mesenchymal cells characteristics,like epithelial cell polarity,intracellular adhesion and loss of specific cell surface markers.Pursuant to cytoskeletal change,cells subsequently gain a mesenchymal-like phenotype.The acquisition of mesenchymal characteristics during EMT occurs progressively,where fully epithelial and mesenchymal phenotype represent just the extreme edges[34].This plastic and dynamic process involves several intermediate states,including so-called hybrid phenotypes in which cells express epithelial and mesenchymal features[35,36].Cells expressing such hybrid epithelial/mesenchymal phenotype do not only play a fundamental role in embryogenesis,but also in cancer formation and progression[37,38].
装配式混凝土结构,结构的实质其实就像“搭积木”一样的方式。其结构系统、内部加载系统、外部维护系统等,都可以通过在工厂或者施工现场提前预制而成。可通过加强套筒灌浆连接或钢筋锚固搭接连接,将散装预制件连接成一体,形成可靠的建筑结构。装配式混凝土结构通过预先制造构件,并根据施工图纸现场进行组装、搭接或连接成具有可靠传力和承载体系的结构。这种方法节省能源,易于拆除,节能环保,防止噪音污染,而且具有设计多样化,施工速度快,节省劳动力,提高劳动效率,构件可重复利用等多种优点。是现代社会建设和发展不可或缺的、这种开拓和创新是具有里程碑意义的。
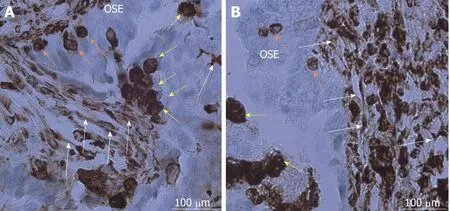
Figure1 Cancer stem cells in ovarian cancer tissue sections after immunohistochemistry for vimentin.A,B:Vimentin-positive small stem cells (≤ 5 μm) in ovarian surface epithelium (orange arrows,A and B) are developing into bigger round cells (10-15 μm) (yellow arrows,A and B) and mesenchymal-like stem cells (white arrows,A and B)by making elongations and protrusions.Legend: brown color-positivity for vimentin.Red bar: 100 μm.
Identification of CSCs relies on the presence of markers.In ovarian cancer many markers are used to confirm the presence of CSCs (Table1).Isolated CSCs can then be tested for stemnessin vitrothrough spheroid forming assay,andin vivowith limiting dilution assays to examine the tumorigenicity of the sample on the animal model[26,63,64].
每当阳光普照的时候,家家户户都会把家中的腊味拿出来,一排排整齐地挂在晾衣竿上。腊肠红艳欲滴;火腿形如琵琶;鸡鸭则被树枝撑开,张牙舞爪;还有鸭胗、鸭肝之类的内脏,也用麻绳儿串起来,结成美味的穗子……那场面壮观极了。当腊味的香气越来越醇厚,年夜饭也就不远了。
3.1 磁化组PFS混凝处理造纸废水,最终出水的余铁含量比未磁化组降低了47.6%;亚铁含量比未磁化组降低了53.0%;磁化组出水的pH值低于未磁化组。磁化组中PFS充分参与混凝沉淀,最终出水的含铁量低于未磁化组。
OVARIAN CSC MICROENVIRONMENT
Defining the niche that supports ovarian CSCs must consider the clinical course of the disease.The evolution of ovarian cancer,its origin in the ovarian surface epithelium or in the distal part of fallopian tube,its progression,and especially its peritoneal dissemination,indicates the existence of multiple types of niches.Within primary tumors,multiple stromal cell types are involved in the formation of a pro-tumorigenic microenvironment[52].Tumor cells release several soluble factors and proteins that mobilize the population of tumor cells to settle in distant organs and tissues[53].3D cultures that displayed the early dissemination of ovarian cancer into peritoneal mesothelium reveled,that cancer cells induce mesothelial cells to synthesize fibronectinviasecretion of transforming growth factor beta-1[54].Ascites,frequently accompanying advanced disease,represents a unique type of ovarian CSCs microenvironment.Interleukin 6,being elevated in ascites,triggers the JAK /STAT3 signaling pathway,which plays an important role in ovarian CSC function[55-57].The Wnt/beta-catenin pathway is another pathway involved in communication between ovarian cancer cells and ascites,thus its inhibition presents potential therapeutic target for ovarian cancer[58].The adipose tissue,especially omentum,provides another microenvironment,optimal for ovarian cancer lesions.Omental adipocytes enable nesting,invasion,and migration of ovarian cancer cells,and provide energy for rapid tumor growth[59].
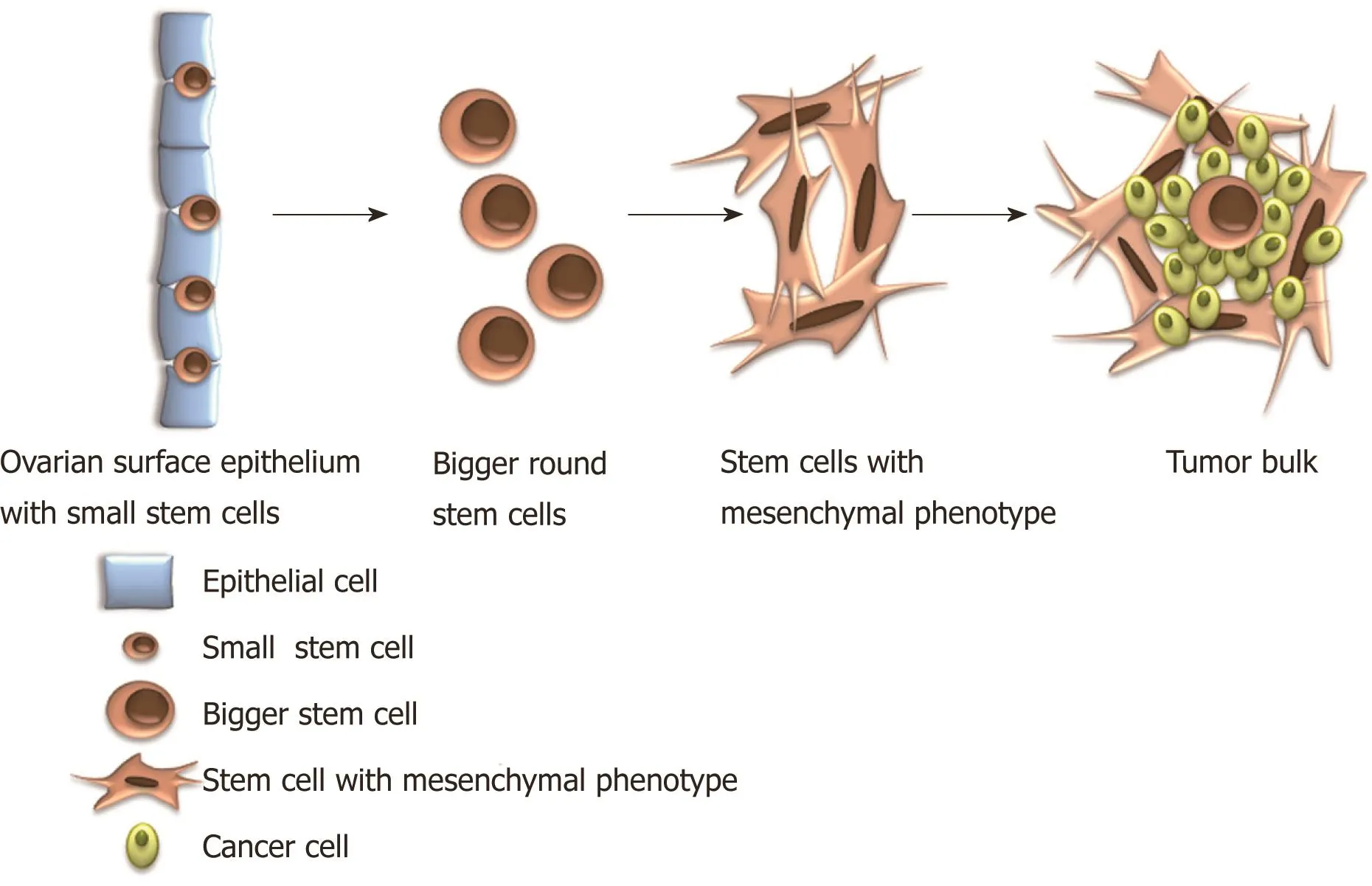
Figure2 Hypothetical model of epithelial-mesenchymal transition.Small,progenitor very small embryonic-like stem cells (diameters of about 5 μm) among the epithelial cells in the ovarian surface epithelium develop into bigger round cells (diameters of 10-15 μm) and (in)-directly undergo transformation into mesenchymal-like stem cells.
Beside soluble factors and proteins secreted by ovarian cancer cells,the role of extracellular vesicles in the formation of pre-metastatic niche and metastatic colonization has been investigated[60].Exosomes play an important role in intercellular signaling and in transportation of genetic information[60].They are coordinators between tumor cells,stromal cells and the extracellular matrix through the shuttling of different lipids,proteins,double-stranded DNAs,RNAs,non-transcribed RNAs,and microRNAs[60].Ovarian cancer derived exosomes were reported to transfer CD44 into mesothelial cells,upregulating matrix metalloproteinase 9 that facilitates cancer cell nesting and invasion[61].Exosomes in epithelial ovarian cancer have also promising therapeutic potential as they are related to immune system,tumor microenvironment and tumor angiogenesis[62].Extracellular vesicles have created new perspective on diagnosis,prognosis,treatment,and drug resistance in ovarian cancer,however,knowledgebase has so far been limited,so further research is needed.
OVARIAN CSC IDENTIFICATION: THE BIOMARKERS
The presence of a major cytoskeletal component of mesenchymal cell vimentin was,further to metastatic progression,also related to primary (intrinsic) resistance or poor response to chemotherapy[46,47].Tumor cells undergoing EMT gain the ability to disarm body antitumor defence,resist apoptosis and anticancer drugs[47].Morphological and functional changes involved in EMT related processes (generation and maintenance of CSCs,tumor invasion,metastasis formation and chemoresistance)require robust reprogramming of gene expression,which is partially accomplished at the transcriptional level of gene expression and partially in gene expression's posttranscriptional regulation[44].A well established factor regulating EMT is the activation of the signal transducer and activator of the transcription 3 (STAT3) pathway[48].As EMT represents the main event in terms of cancer manifestation and progression,it is becoming a promising target for therapeutic intervention[42,49].
8月31日,康朴(中国)川渝大区二级商招商会暨特肥新品发布会在眉山召开。据悉,本次发布会旨在推进康朴(中国)特肥在川渝大区的战略合作项目,将全球顶级的高端产品和先进的肥料“减量增效”技术带到川渝地区。
There are multiple surface biomarkers used to identify CSCs in ovarian cancer.CD117 was demonstrated to be the first cell surface marker for the ovarian CSCs.Its expression correlates with tumor formation,chemoresistance,and poor prognosis of disease[65-67].CD 133 is one of the most commonly reported ovarian CSC surface markers.It is associated with a number of stem characteristics,like tumor formation,disease progression,chemoresistance,and poor prognosis[68-71].It was also studied as a target for a cancer target therapy[72].Other common CSC surface markers are CD24,CD44,EpCAM and ROR1.CD24 is associated with tumor formation,metastasis,poor prognosis,chemoresistance,and recurrence of disease[73-77].Similar characteristics are correlated with CD 44[78-81].Surface markers can be used alone or in combination with other ovarian CSC markers.
In addition to cell surface markers,the enzyme aldehyde dehydrogenase 1(ALDH1) is used to identify CSCs in ovarian cancer.Several studies correlate ALDH1 expression with cell proliferation,migration promotion,poor survival,and chemoresistance[82-84].Conversely,inhibition of ALDH1A1 in a mouse model sensitized the tumors to treatment[85].The expression of ALDH1 alone or in combination with cell surface stem cell markers is an accepted method for CSC identification in ovarian cancer.
NANOG is a transcription factor that,along with transcription factors OCT4 and SOX2,plays a key role in pluripotency and self-renewal maintenance in undifferentiated embryonic stem cells[86].NANOG,OCT4 and SOX2 are commonly expressed also in ovarian CSCs[87,88].Their expression is associated with poor prognosis and chemoresistance[88-92].NANOG also regulates epithelial-mesenchymal transition[93].c-Myc is another key oncogenic transcription factor that participates in tumor pathogenesis[94].Its knockdown by let-7d increases ovarian cancer cell sensitivity to a genistein analog[95].Future studies on pluripotency factors expressed in ovarian CSCs will provide additional data on how cancer stemness is maintained.
CSCs often display a slow-cycling rate,making them resistant to standard chemotherapy and radiotherapy,which target actively proliferating cells[110,111].By remaining in the G0 phase of the cell cycle,CSCs maintain inactivity.As most treatment regimens target actively-dividing cells in the S or M phase of the cell cycle,CSC quiescence presents a significant issue in terms of successful treatment.Subpopulations of inactive ovarian CSCs,which survive,allegedly,successful treatment with cytostatic chemotherapy,might be the cause of high-frequency ovarian cancer relapse[15].Resistant dormant CSCs “wake up” later and cause tumor recurrence[15].As relapsed tumor is richer in CSCs,it becomes more chemoresistant than primary ovarian tumor (Figure3).
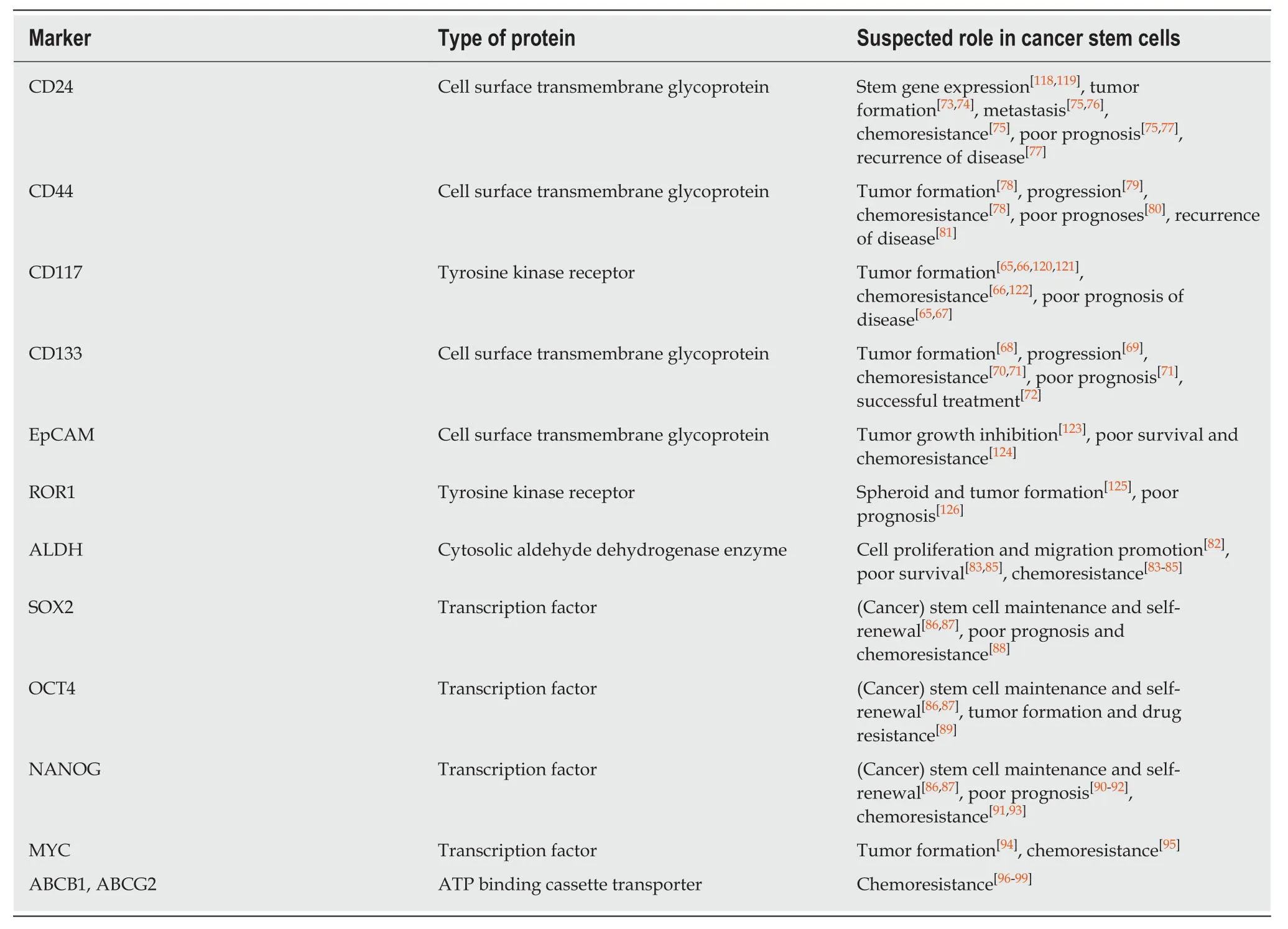
Table1 Putative ovarian cancer stem cell markers and their relevance.
Another way in which ovarian CSCs can be identified is by the ability to efflux DNA-binding dyes resulting in a side population using flow cytometry.For dye effluxion CSCs should express ATP binding cassette transporters such as MDR1/ABCB1 and ABCG2 that can efflux chemotherapeutic agents and so contribute to chemoresistance[96-99].
OVARIAN CSCs IN THE ERA OF “OMICS” AND GENE EXPRESSION PROFILING
Although CSCs can cause different processes such as tumor initiation,malignant proliferation,relapse and multi-drug resistance,the way to eliminate CSCs remains unknown.The modern molecular genetic methods enable to study the ovarian CSCs in more detail,in terms of their gene expression profile (e.g.,whole genome sequencing).An increasing number of studies try to elucidate whether the different stem cells compartments that are apparently present in ovarian cancer differ at the DNA level.These studies showed a niche-dependent gene expression profile of heterogeneous intratumoral populations of stem cells,which make a task to target ovarian CSCs even more difficult[100].
It was found thatTP53is the most frequently mutated gene in high grade ovarian cancer[101].About 50% of these tumors showed defective homologous recombination due to germline and somaticBRCAmutations,epigenetic inactivation of BRCA and abnormalities of DNA repair genes.Along this,somatic copy number alterations are frequent in these tumors,especially defective NOTCH,RAS/MEK,PI3K and FOXM1 pathway signaling[101].Some of them are associated with patients' prognosis[101].Other subtypes of ovarian cancer were characterised by a different mutational spectrum:Low grade ovarian serous carcinoma has increased frequency ofBRAFandRASmutations,mucinous cancers have a mutation inARID1A,PIK3CA,PTEN,CTNNB1and inRASgenes[101].Some data also suggest that TERT C228T promoter mutations may have an important role in progression of adult granulosa cell tumors[102].Intensive research was focused on relation between the gene expression profile and ovarian CSCs.For identification of CSCs positivity for some markers,including CD133,CD44,CD117,CD24,EpCAM,LY6A,and ALDH1,was used.
An important task remains to elucidate the originating CSCs (e.g.,VSELs) and common characteristics of different populations of stem cells involved at different stages of ovarian cancer.Some studies compared the gene expression profile of ovarian CSCs in ovarian cancer of different grades,including advanced disease compared to normal ovarian surface epithelium,to identify the key pathways,and specific molecular signatures involved in the manifestation of ovarian cancer at different stages[103].Comparison of genome-wide expression profiles in ovarian CSCs revealed a mass of differentially expressed genes.Among these genes,NAB1andNPIPL1were commonly upregulated,whereas the genesPROS1,GREB1,KLF9andMTUS1were commonly downregulated,regardless of the stage of a disease[103].These genes regulate the cellular components such as centrosome,plasma membrane receptors,and basal lamina,and may participate in biological processes such as cell cycle regulation,chemoresistance and stemness induction.Moreover,the gene coexpression extrapolation screening by the Connectivity Map revealed several smallmolecule compounds (such as SC-560,disulfiram,thapsigargin,esculetin and cinchonine) with potential anti-ovarian CSCs properties targeting ovarian CSC signature genes[103].
All these and several other data indicate that the gene expression profile and the presence of specific mutation/genomic aberration may help to identify the culprit of the CSC compartment.The improvements in our understanding of the molecular and stem cell basis of ovarian cancer should lead to more efficacious treatment.
OVARIAN CSC CLINICAL SIGNIFICANCE
As previously mentioned,ovarian cancer,according to its biological features and clinical characteristics,represents a typical CSC-driven malignancy[15].Ovarian CSCs,including VSEL stem cells,play an important role in tumor formation and dissemination,thus advancing disease progression[19,104].Tumor cell spheroids from ascites,which frequently accompany ovarian cancer,can survive and proliferate even in the absence of abdominal wall and/or abdominal organ adhesion.This characteristic represents one of the fundamental properties of CSCs,which is also usedin vitrowhen assessing cell stemness as sphere formation presence in suspension culture[105].Ascites,being rich in tumor cells with stem-like properties,is an important CSC source[106-109].
比如,保时捷911这个大家族里的一个分支如果组织一次聚会,那肯定会吸引无数的关注,它们有一个共同的特点—与赛车分割不开的紧密联系。
Many studies support this thesis.In metastatic and relapsed ovarian cancer,a remarkable increase in CD44 level,a putative CSC marker,was observed in comparison to primary tumors[112].CD44 was found overexpressed in drug-resistant ovarian cancer cell lines and up-regulated in tumor recurrence following chemotherapy[112].Increased nuclear NANOG expression,another putative CSC marker,was significantly associated with reduced chemosensitivity and poor overall and disease-free survival[90].NANOG has been suggested as a potential predictor of survival and is involved in the ovarian carcinoma chemoresistance mechanism[91].Several other studies have investigated various putative ovarian CSC marker expression in correlation with clinico-pathological signs of aggression,poor disease prognosis and chemoresistance,and they have all provided similar results[65,71,81,85,113].
Ovarian CSCs' strong implication in terms of disease clinical course is,similarly,supported by functional genomics studies which,based on gene expression profiles,identified different tumor subtypes rich in stemness-associated genes which,when expressed,relate to poor prognosis[114,115].
(2)R2={T×M,T×P,T×Q,Q×P}。其中T×M,T×P,T×Q,Q×P均为R2的子集,依次表示任务与物料视图间两节点的关系组成的集合、任务与工艺视图间两节点的关系组成的集合、任务与质量视图间两节点的关系组成的集合、质量与工艺视图间两节点的关系组成的集合。
In conclusion,EMT as well as its reversal,mesenchymal-epithelial transition,represents a highly dynamic process in tumor cells which may be triggered by VSEL stem cells present amongst epithelial cells in the ovarian surface epithelium layer.Cancer stemness seems to be more associated with partial-EMT phenotype than fullydriven EMT[34,44,50].In line with this concept is the concept of CSC plasticity,which postulates that CSCs are able to switch between different states,including a non-stem state[51].
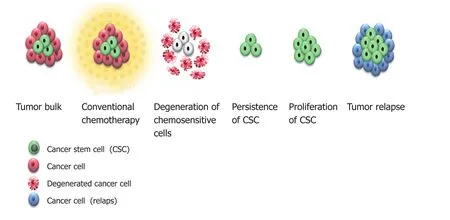
Figure3 Diagrammatic representation of treatment influence on ovarian cancer.Cancer cells are sensitive to standard treatment with cytostatic chemotherapy leading to cells destruction and reduction of tumor size.Cancer stem cells are resistant to standard treatment with cytostatic chemotherapy,so they persist and further proliferate,leading to tumor relapse even richer in cancer stem cells and resistant to standard chemotherapy.CSC: Cancer stem cell.
OVARIAN CSCs AS THERAPEUTIC TARGETS
There are multiple pathways involved in promoting stem cell phenotype and chemoresistance in terms of ovarian cancer.Each pathway could potentially be therapeutically targeted with pathway inhibitors.If a therapeutic goal is to eliminate CSCs,more studies are needed to define which subpopulation of CSCs should to be targeted.Small,VSEL stem cells,proposed to be progenitor stem cells involved in ovarian cancer triggering and progressionviaEMT and interaction with other types of stem cells,might represent potential targets.
Before introducing CSC target therapy in clinical practice,we should think about the many challenges concerning stem cell inhibition.CSCs share epitopes with normal stem cells,so treatment regimens targeting CSCs may also harm normal stem cells,which would increase drug toxicity and the risk of adverse side effects.An ideal therapeutic agent should selectively target CSCs above normal stem cells,so further biological CSC characterization,particularly the underlying mechanisms regulating their function,is required.
虽然社会公众在城市更新中大都是以“弱势群体”的面貌出现,但是作为城市更新直接的利益相关者,有着巨大的潜力。事实上,从西方国家城市更新的发展历程与现实经验看,公众参与城市更新已经成为不容忽视的力量。在国内当前城市更新运行机制中,由于社区公众个体利益和诉求的分散化,其在城市更新中充当的往往是“虚位主体”的角色。由于社区公众对于城市更新的方案设计、利益结构的冲击甚至是城市更新的进程都会有不同程度的影响,因此作为城市更新整体利益结构的一环,其潜力是巨大的。
The development of novel CSC treatments also requires a thorough understanding of the complex genomic profile of ovarian cancer,since its heterogeneity might influence treatment response[104,116].
本文先对我国目前地理信息资源成果管理的现状进行了分析,在对地理信息成果进行管理时,以数据库与基础测绘数据库等设置为数据来源,并以数据中心为基础利用数据仓库的方法对地理信息数据进行统一的管理,在大数据时代对多样化数据、海量数据的管理提供了科学合理的方式,提升我国地理信息管理效率。
Finally,only a small fraction of cells within the tumor would be eliminated by CSC target therapy,so treatment response,shrinking of the tumor bulk,may require some time to become visible.Therefore,a combined therapeutic approach with cytotoxic chemotherapy and/or other treatment regime should be introduced to reduce tumor bulk[117].Treatment success should then be estimated in terms of tumor bulk shrinkage and the eradication of CSC populations for which identification of reliable ovarian CSC biomarkers is critical,so it can be used in clinical practice.
CONCLUSION
Successful ovarian cancer treatment depends on ovarian CSC eradication,as CSCs present the driving force of disease manifestation,progression and recurrence pursuant to conventional treatment.There are three potential targets for ovarian CSC eradication: CSC markers,CSC signaling pathways implicated in renewal and CSC niche.
Due to the heterogeneous nature of ovarian cancer,there are probably more markers identifying different subpopulations of ovarian CSCs,and diverse signaling pathways involved in CSC renewal.In terms of identifying CSC specific markers and signaling pathways,and additionally exploring ovarian CSC microenvironment,cancer cell lines are helpful,butin vitrotumor formation analysis should be upgraded by analysing ovarian cancer patient tumor tissuein vivo.Selected ovarian CSC markers,signaling pathways and factors from CSC microenvironment should then be tested in clinical practice,where their expression,influence and inhibition should be correlated,not only with disease outcome,but also in terms of their influence on chemoresistance.In vitroandin vivoinvestigation of CSC properties and their microenvironment properties may lead to novel therapeutic regimens for ovarian cancer elimination and relapse prevention.
Despite the tremendous progress made in recent years in the field of ovarian CSCs,a number of issues should be considered.Firstly,ovarian cancer presents a heterogeneous group of tumors and stem cells.A high level of heterogeneity makes identifying a target for a wide population of ovarian cancer patients difficult; to mitigate this,more phenotypic,genetic and epigenetic studies of ovarian cancer patient CSCs need to be performed.Secondly,we still don't know if different CSC populations arise from common progenitor cells and which CSC populations are the most critical to target.We suggest a population of small,VSEL stem cells as progenitor stem cells needs be better elucidated.CSC subpopulations probably change during cancer progress,and specific CSC subpopulations might play a role at certain disease phases.Finally,do varying marker profiles signify different subpopulation of CSCs and how does CSCs microenvironment influence markers expression? These and many other questions in the field of CSCs should be answered in order to introducing personalised medicine in the treatment of ovarian cancer.
ACKNOWLEDGEMENTS
The authors would like to thank Shawn Nicholas Thomson for proofreading the article and Eva Skuk for technical preparation of figures.
猜你喜欢
杂志排行

World Journal of Stem Cells的其它文章
- Targeting cancer stem cells in drug discovery: Current state and future perspectives
- Induced pluripotent stem cells,a giant leap for mankind therapeutic applications
- Using transcription factors for direct reprogramming of neurons in vitro
- Predicting differentiation potential of human pluripotent stem cells: Possibilities and challenges