Systematic review: Renin-angiotensin system inhibitors in chemoprevention of hepatocellular carcinoma
2019-06-13MicheleBaroneMariaTeresaViggianiGiuseppeLosurdoMariabeatricePrincipiAlfredoDiLeo
Michele Barone, Maria Teresa Viggiani, Giuseppe Losurdo, Mariabeatrice Principi, Alfredo Di Leo
AbstractBACKGROUND Neoangiogenesis is one of the key pathogenetic mechanisms in hepatocellular carcinoma (HCC). Modulation of the renin-angiotensin system (RAS) by angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin receptor blockers (ARBs) seems to be a possible adjuvant therapy for HCC, due to the antiangiogenic and anti-fibrogenic activity of these drugs.AIMTo elucidate the role of ARBs and ACE-Is in HCC.METHODS We performed an electronic search of the literature using the most accessed online databases (PubMed, Cochrane library, Scopus and Web of Science),entering the query terms "angiotensin-converting enzyme inhibitors" OR "ACE inhibitors" OR "ACE-I" AND "hepatocarcinoma*" OR "hepatocellular carcinoma;moreover "angiotensin II type 1 receptor blockers" OR "ARBs" AND"hepatocarcinoma*" OR "hepatocellular carcinoma". Eligibility criteria were: (1)prospective or retrospective clinical studies; (2) epidemiological studies; and (3)experimental studies conducted in vivo or in vitro. Abstracts, conference papers,and reviews were excluded a priori. We limited our literature search to articles published in English, in peer-reviewed journals.RESULTS Thirty-one studies were selected. Three interventional studies showed that ACEIs had a significant protective effect on HCC recurrence only when used in combination with vitamin K or branched chain aminoacids, without a significant increase in overall survival. Of six retrospective observational studies, mainly focused on overall survival, only one demonstrated a prolonged survival in the ACE-Is group, whereas the two that also evaluated tumor recurrence showed conflicting results. All experimental studies displayed beneficial effects of RAS inhibitors on hepatocarcinogenesis. Numerous experimental studies, conducted either on animals and cell cultures, demonstrated the anti-angiogenetic and antifibrotic effect of ACE-Is and ARBs, thanks to the suppression of some cytokines such as vascular endothelial growth factor, hypoxia-inducible factor-1a,transforming growth factor-beta and tumor necrosis factor alpha. All or parts of these mechanisms were demonstrated in rodents developing fewer HCC and preneoplastic lesions after receiving such drugs.CONCLUSION In humans, RAS inhibitors - alone or in combination - significantly suppressed the cumulative HCC recurrence, without prolonging patient survival, but some limitations intrinsic to these studies prompt further investigations.
Key words: Cirrhosis; Renin; Angiotensin; Survival; Cancer prevention; Hepatocarcinoma ses/by-nc/4.0/
INTRODUCTION
Liver cancer is the fifth most common cancer and the second most frequent cause of cancer-related death globally[1]. In particular, it is much more common in men than in women, and if we refer solely to more developed countries, it is the sixth leading cause of cancer death in men[2].
Hepatocellular carcinoma (HCC) represents about 90% of primary liver cancers and usually develops in patients with underlying liver cirrhosis[1]. Etiologic factors are most frequently represented by chronic viral hepatitis [hepatitis B virus (HBV) and hepatitis C virus (HCV)], alcohol intake, and non-alcoholic steatohepatitis (NASH),which all together are responsible for about 80% of HCC[3].
One of the major cancer hallmarks of HCC is the process of neoangiogenesis, which is thought to occur early in the carcinogenetic process. Even if the pathogenetic mechanisms responsible for the neoangiogenesis remain to be clarified, it is plausible that the intervention of proangiogenic growth factors occurs as a result of signals mediated by hypoxia-inducible transcription factors[4].
As a result of the involvement of angiogenesis, clinical studies have been focused on anti-angiogenic biological agents in HCC treatment[5-7]. However, this therapeutic approach to cirrhotic patients has been frequently associated with severe side effects,and it is burdened by high costs and contraindications to their long-term administration[8]. Inexpensive and easily manageable drugs could represent an alternative therapy with a proven safety profile on long-term administration. From this point of view, angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin II type 1 receptor blockers (ARBs) seem to be a possible candidate for adjuvant therapies for HCC, as a consequence of their well-known anti-angiogenic and anti-fibrogenic activity[9-11]. Theoretically, ACE-I and ARBs could also have a role in HCC primary prevention since they reduce both neovascularization and the development of liver fibrosis[10].
We decided to perform this study as the possible role of renin-angiotensin system(RAS) inhibitors in the prevention of HCC is still an attractive field of research, as suggested by the recently published experimental and clinical studies. In order to better clarify this issue, in this systematic review, we performed a search of studies in this field. Using this method, we selected 31 studies, mainly focused on experimental data.
MATERIALS AND METHODS
Data sources and searches
Literature was selected in August 2018, focusing on studies regarding ACE-Is, ARBs and HCCs. For this purpose, an electronic search of the literature was conducted using the online databases PubMed, Cochrane library, Scopus and Web of Science,entering the query terms "angiotensin-converting enzyme inhibitors" OR "ACE inhibitors" OR "ACE-I" AND "hepatocarcinoma*" OR "hepatocellular carcinoma;moreover "angiotensin II type 1 receptor blockers" OR "ARBs" AND"hepatocarcinoma*" OR "hepatocellular carcinoma" were used. Further relevant articles were hand-searched using the references of the selected studies.
Study selection
Eligibility criteria were: (1) prospective or retrospective clinical studies; (2)epidemiological studies; and (3) experimental studies conducted in vivo or in vitro.Abstracts, conference papers, and reviews were excluded a priori. We limited our literature search to articles published in English, in peer-reviewed journals.
Data extraction and quality assessment
We conducted the articles selection using a two-step approach, to evaluate whether they matched the eligibility criteria. The first phase was based on titles and abstracts,and the second on full-text examination. This procedure was performed by two of the authors (Viggiani MT and Principi M), and the percentage of agreement demonstrated high inter-rater reliability (97.4%). Lastly, discrepancies in data extraction were resolved by introducing a third, experienced arbitrator (Losurdo G).
In cases of studies analyzing overlapping periods from the same registry/database,we considered only the study that examined the more extended period and the more significant number of patients.
RESULTS
As shown in Figure 1, the combined search of electronic databases identified 231 articles. Three additional articles were hand-searched using references of the selected studies. After removing duplicates, 86 articles were screened. On the basis of the abstract evaluation, 33 articles were excluded since they did not match the eligibility criteria. The evaluation of full-text articles led to exclude 15 additional manuscripts.We found a meta-analysis on the beneficial effects of ACE-I/ARBs against several tumors[12]; this study was excluded since it took in consideration only a trial on HCC that we had already included as a single study[13]. Finally, ten reviews were excluded since they evaluated the same studies on the relationship between ACE-Is or ARBs already selected. At the end of our selection, only 31 studies were included in the present review.
Clinical studies
Table 1 reports the characteristics of all clinical studies selected. We found only three interventional studies, all performed by the same authors, which examined the influence of a putative antitumoral treatment after randomization of the patients[13-15].These studies evaluated the influence of ACE-Is, given alone or in combination with either vitamin K or branched chain aminoacids (BCAA), on HCC recurrence, showing a significant protective effect of ACE-I only when used in combination with vitamin K or BCAA. Patients were enrolled when they had a low number and low size tumors susceptible to radiofrequency ablation (RFA) treatment and were excluded in the event of early recurrence (within 3 mo). No significant increase in overall survival was observed in any of the three studies.
Six more recent retrospective observational studies evaluated the effect of ACE-Is or ARBs on overall survival (OS) and/or time to recurrence in patients who underwent different HCC treatments (Table 1). Ho et al[16]evaluated the effect of ACEI or ARB exposure within the first six months after initiating antiviral agents in a highrisk HBV and HCV large cohorts of patients and did not find any protective effect of these drugs on HCC development adjusted for potential confounders. Surprisingly, in HCV patients without cirrhosis, diabetes, and hyperlipidemia, they found an increased HCC risk associated with ACE-I or ARB use in (HR = 4.53, 95%CI: 1.46-14.1). Hagberg et al[17]restricted the study population to patients with hypertension(both cases and controls). Also, in this case, no protective effect was observed with ACE-I or ARB use. However, patients were already defined exposed (cases) after receiving at least two prescriptions for ACE-I and/or ARBs before the index date.Walker et al[18], included subjects that were exposed to ACE-I treatment 12-24 mo before the first recorded liver cancer diagnosis without finding any protective effect.
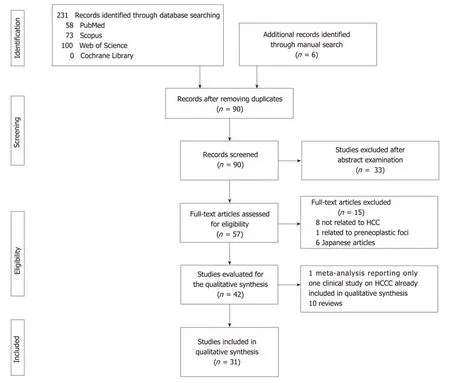
Figure 1 PRlSMA flow diagram describing the process of study selection. HCC: Hepatocellular carcinoma.
Differently from what observed by the previous authors, Pinter et al[19]found a prolonged overall survival in HCC patients treated with sorafenib/supportive therapy and already receiving ACE-I or ARBs for a median duration of treatment of 12.7 mo. Also, Facciorusso et al[20]reported a prolonged overall survival in HCC patients treated with RFA and already receiving ARBs (but not ACE-I) for at least the previous two years. In this study, a significantly longer disease-free survival in patients receiving ARBs (HR = 0.47; 95%CI: 0.27-0.82, P = 0.009)[20]was reported. In the last clinical study, by Karibori et al[21]the treatment of hypertension with ACE-Is or ARBs did not improve overall survival after tumor resection in HCV-HCC patients with or without cirrhosis compared to the related controls. Interestingly, HCC-HCV cirrhotic patients with hypertension treated with other antihypertensive drugs had a significantly reduced overall survival compared to HCC-HCV cirrhotic patients receiving either ACE-Is or ARBs or no antihypertensive treatment (P = 0.029). Finally,hypertension had no influence on the prognosis of inpatients with HCC related to other etiologies[21].
An additional study, not listed in Table 1, analyzing the association between the use of statins in HBV-infected patients and the risk of HCC, reported that the use of ACE-I for more than one year did not significantly influence the protective effect of statins against HCC development[22]. However, in this study, a large number of patients in the statin group (62%) was diabetic and therefore probably using4Adjusted for age, gender, Child-Pugh class and α-fetoprotein. Time to recurrence was significantly reduced in patients receiving angiotensin II type 1 receptor blockers (P = 0.009). RFA: Radiofrequency ablation; OS: Overall survival; OR: Odds ratio; HR: Hazard ratio; ACE-Is: Angiotensin-converting enzyme inhibitors; ARBs: Angiotensin II type 1 receptor blockers; Vit.: Vitamine; CI: Confidence interval; HCC: Hepatocellular carcinoma; HBV: Hepatitis B virus; HCV: Hepatitis C virus; Pts.: Patients. NS: No significance.metformin or thiazolidinediones, which have been demonstrated to profoundly reduce HCC risk[23], and therefore could have also overcome the effect of ACEI/ARBs.
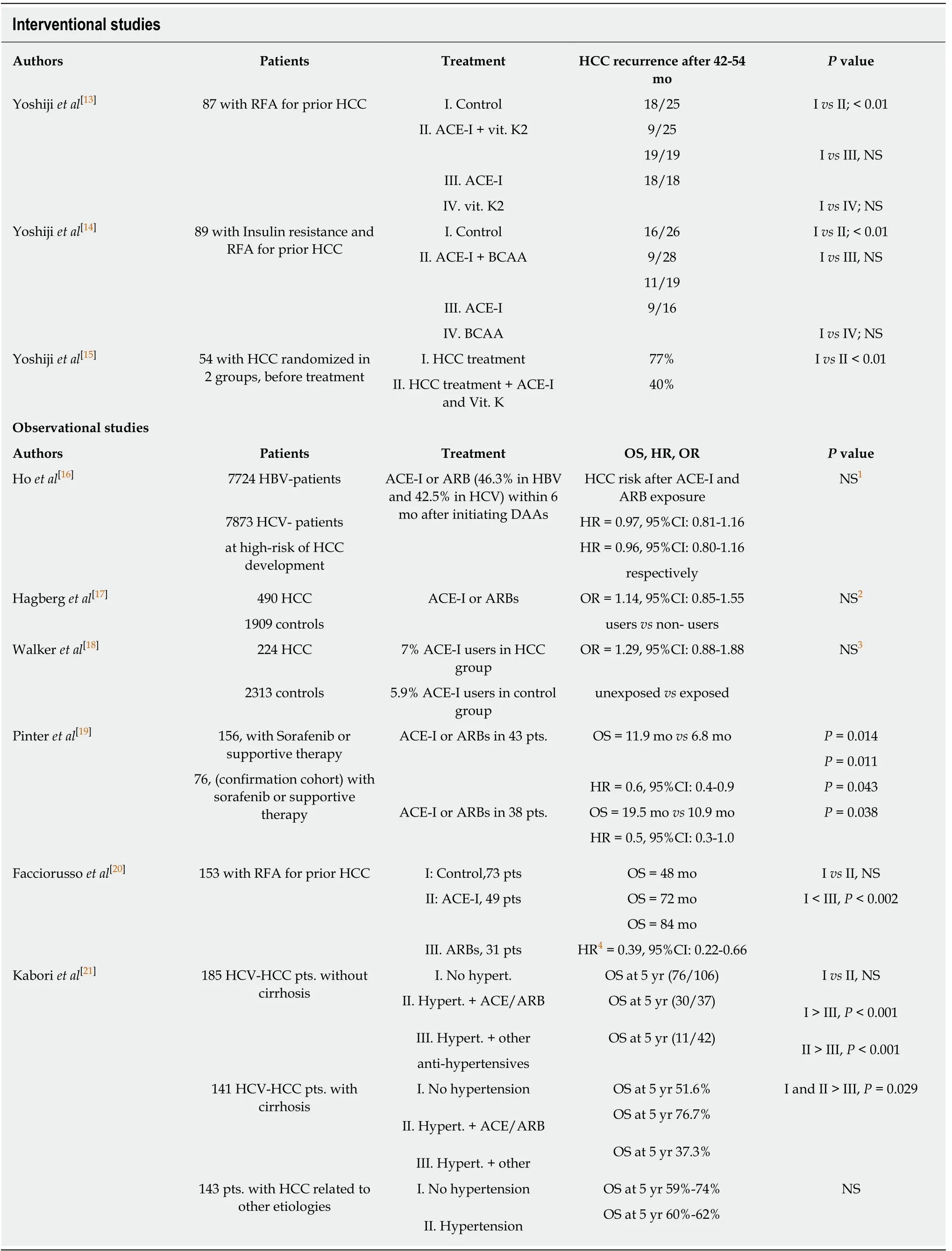
Table 1 Clinical studies on the effect of angiotensin-converting enzyme inhibitors or angiotensin ll type 1 receptor blockers exposure in patients affected or at high risk of hepatocellular carcinoma
To our knowledge, the only case report that matched our selection criteria describes the protective effect of an ACE-I used in combination with vitamin K2 in a patient with a dysplastic nodule on liver cirrhosis. After one year of treatment, the authors describe a reduction of α-fetoprotein (AFP) and AFP-L3 and the disappearance of the dysplastic nodule[24].
Experimental data
The most consistent data on the potential role of ACE-Is and ARBs in HCC prevention/cure come from experimental in vitro and in vivo studies.
Diethylnitrosamine model
Table 2 summarizes all studies performed either in mice or rats using the diethylnitrosamine (DEN) model. Saber et al[25]showed that sorafenib or fosinopril,perindopril and losartan, prolonged overall survival of mice. Both ACE-Is and losartan brought about an improvement in the histological situation, similar to that determined by sorafenib, with regression of malignant histological features. However,only sorafenib and perindopril significantly reduced α-fetoprotein levels as compared to controls. Additionally, sorafenib and anti-hypertensive drugs significantly decreased the transforming growth factor (TGF)-β, tumor necrosis factor (TNF)-α,matrix metalloproteinase (MMP)-2 and vascular endothelial growth factor (VEGF)serum levels compared to controls; however, the administration of perindopril was even more effective than sorafenib in the reduction TNF-α level. The authors conclude their study suggesting that the reduction of inflammatory cytokines, in particular,TNF-α, could have been mediated by the inhibition of phosphorylation-induced NFκBia degradation and phosphorylation of NFκBp65. Therefore, the RAS inhibition may have a dual anticancer effect mediated by the suppression of inflammation and angiogenesis. The same group repeated the same experiment[26]in mice and confirmed the data about the regression of cellular atypia in HCC, but they did not observe a positive effect on animal survival using ACE-Is or ARBs alone, or in combination with sorafenib. In another study[27], albino DEN-treated mice received perindopril,leflunomide, curcumin alone or in combination. While all DEN-treated mice developed HCC, the prevalence of HCC decreased to 37.5% under curcumin, and 25%under leflunomide and perindopril and no mice developed liver dysplastic lesions in the combination arm. This finding paralleled with the reduction of angiogenesis,immunohistochemically evaluated by CD31, an antigen widely used as a marker of neovascularization[28]. Finally, the authors also demonstrated a dramatic reduction of hypoxia-inducible factor (HIF)-α. Mansour et al[29]tested captopril, perindopril, and losartan in male albino rats treated with DEN. Some of the rats receiving DEN plus an active drug also received carbon tetrachloride to stimulate cell proliferation. The administration of captopril and losartan induced a marked reduction of α-fetoprotein and almost halved the levels of VEGF, fibroblast growth factor (FGF) and TGF-β1 only in rats in which hepatocarcinogenesis was promoted by DEN. On the other hand,MMP-2 activity was inhibited by all three drugs in HCC-rats while the levels of tissue inhibitor of metalloproteinase (TIMP)-1, a negative regulator of MMP2, were increased only by the treatment with losartan and perindopril. This study provided exciting results since it demonstrated a prophylactic effect on the mechanisms of hepatocarcinogenesis when ARBs and ACE-Is were given two weeks before DEN injection and not at the same time.
In another model, in addition to DEN treated standard rats, BALB-c mice underwent an injection of HCC cell line. In these mice, the administration of perindopril or 5-fluorouracil alone was not able to reduce the size of HCC[30], while the combination of the two drugs produced much better results thanks to the increased apoptotic activity and the reduction of both the CD31-mRNA and VEGF expression in HCC tissue. Interestingly, the number of preneoplastic lesions was decreased only by the ACE-I, and the addition of 5-fluorouracil enhanced this effect. Lastly, on the basis of additional in vitro studies, they concluded that ACE-I and 5-fluorouracil might reduce the tumor growth by inhibiting neovascularization, which in turn may induce apoptosis of the tumor cells, rather than via direct inhibition of tumor cell proliferation.
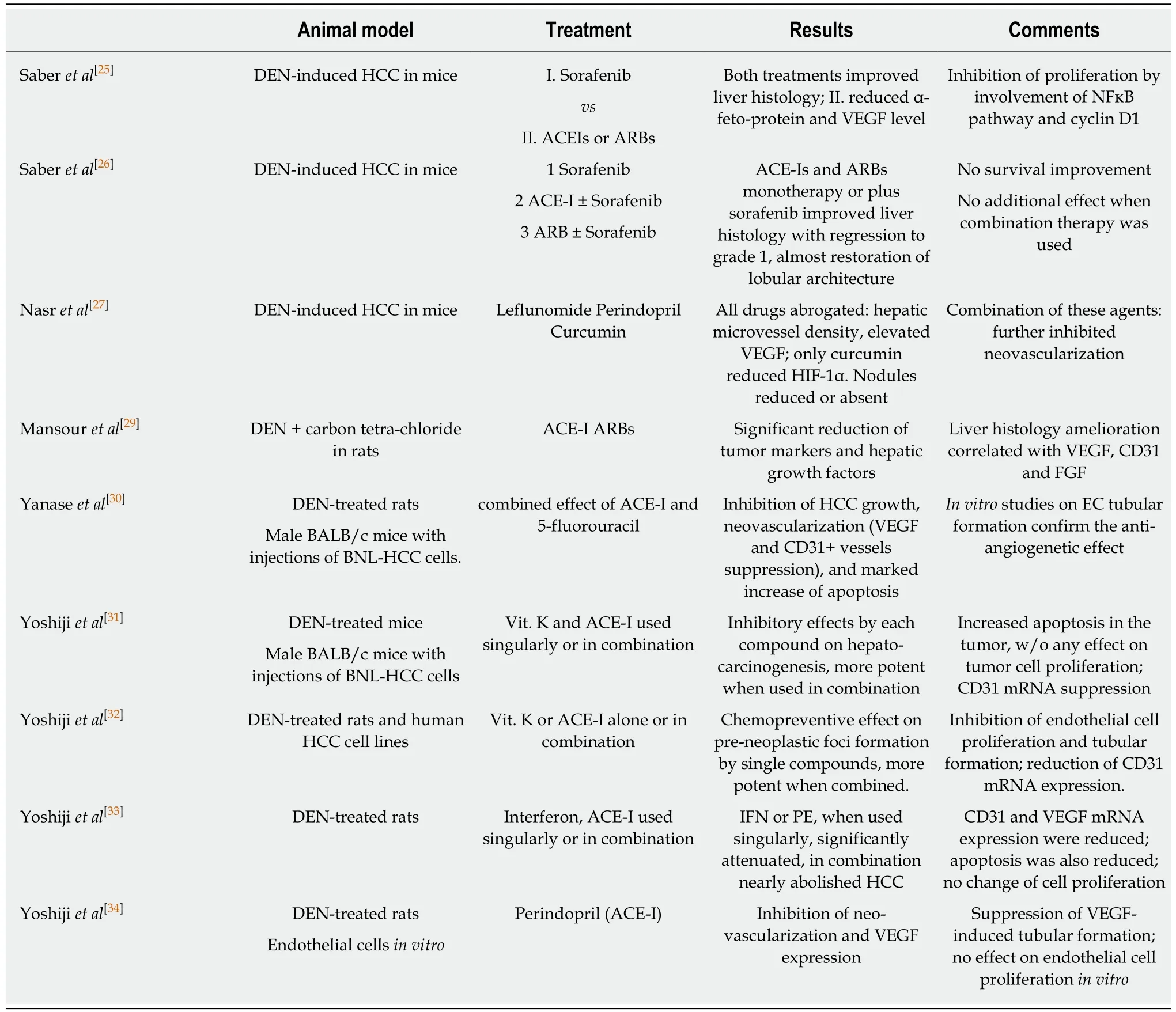
Table 2 Studies on the effect of angiotensin-converting enzyme inhibitors or angiotensin ll type 1 receptor blockers in diethylnitrosamine-induced hepatocellular carcinoma animal models
Yoshiji et al[31]analyzed the effect of perindopril, vitamin K or their combination,both in DEN model and in mice injected with BNL-HCC cell line. They showed that HCC was significantly inhibited by the treatment with vitamin K and ACE-I, and their combination produced an even more potent inhibitory effect compared to the single agents. These results were observed in both models and were associated with mRNA-CD31 suppression and promotion of apoptosis (the number of TUNELpositive cells was significantly increased by treatment with vitamin K and ACE-I compared to the control group), while the proliferative activity was not influenced.The same group replicated this protocol[32]both in rats and HepG2 cells with the aim of studying proliferation and angiogenesis. They found that vitamin K and ACE-I inhibited endothelial cell tubule formation and endothelial cell proliferation in a dosedependent manner while only vitamin K inhibited tumor cell proliferation. In another similar experience[33], BALB/c mice treated with DEN and receiving either perindopril or interferon-beta or a combination of them experienced a substantial reduction in the number of nodules/liver that was maximal (less than one nodule/liver) in the group receiving both drugs. These findings paralleled the reduction of CD31-mRNA and the increase of the apoptotic index within nodules. In another study of the same group[34]perindopril, given at low or high doses, did not influence the production of VEGF in cultured endothelial cells but was able to suppress their migration and formation of tubules. In the same study, perindopril hampered the development of preneoplastic liver lesions in DEN-treated animals, probably induced by the suppression of CD31,which paralleled the reduction of the number of lesions.
Other models
Several studies (Table 3) adopted a xenograft model in which in BALB/c mice received an injection of HCC cell lines. Using this model, Fan et al[35]demonstrated an enhanced immunohistochemical expression of angiotensin receptor 1 (AT1R) in cancer tissue, which correlated with VEGF receptor A. The administration of candesartan reduced the mean diameter of tumors and suppressed AT1R expression and decreased microvascular density. The authors then examined the effects of angiotensin II and candesartan on the expression of AT1R protein in SMMC-7721 and HepG2 cell lines using Western blotting and found that candesartan down-regulated the expression of AT1R protein induced by angiotensin II with a dose-dependent relationship, as well as angiotensin II-induced production of VEGF-A. On the other hand, when angiotensin receptor 2 was transduced by an adenoviral vector in HCC cell lines and murine orthotropic liver graft, it inhibited cell proliferation with a significant decrease of S-phase cells and an increase of G1-phase cells, probably mediated by the alteration of expression of CDK4 and cyclinD1[36]. Therefore, it was hypothesized that apoptosis was secondary to activation of p38 MAPK, pJNK,caspase-8 and caspase-3 and inactivation of pp42/44 MAPK (Erk1/2). In another model, using the BNL-HCC cell line transferred into BALB/c mice[37], both perindopril and interferon-beta reduced the volume of HCC, with an even higher magnitude when administered together. Additionally, the authors showed that this effect was mediated by the promotion of apoptosis, the reduction of cell proliferation and the inhibition of neo-angiogenesis proven by the reduction of CD31 positive cells and the suppression of VEGF protein within the tumor. Yoshiji et al[38]used a retroviral vector to enhance the expression of VEGF in the BNL-HCC cell line. In this way, they found that perindopril reversed the production of VEGF and that the ability of cells to migrate was directly dependent on VEGF levels. When these manipulated cells were injected in BALB/c mice, they discovered that VEGF over-expression within HCC did not modify the angiotensin-2 expression, thus suggesting that, in this model, VEGFmediated tumor growth was not influenced by angiotensin 2. Lastly, similarly to previous studies, it was reported that perindopril inhibited CD31 expression. The same group[39]used the BNL-HCC allograft model in BALB/c mice to show that perindopril, temocapril, and captopril had an inhibitory effect on total HCC volume burden, although the effect of perindopril was much stronger than other ACE-Is.Finally, they showed that perindopril reduced mRNA-VEGF expression and ACE enzyme activity, suppressed microvessel density and inhibited tubule formation in endothelial cells.
The long-term administration of a choline-deficient/low-methionine diet is another way of inducing steatohepatitis, liver cirrhosis, and HCC in rodents. Using this model, Tamaki et al[40]showed that none of the male Wistar rats receiving telmisartan developed HCC, while 54.6% of the control rats developed the tumor. The latter condition was associated with an increase of HIF-1α and protein and VEGF mRNA.Furthermore, telmisartan inhibited the up-regulation of TGF-β1, connective tissue growth factor (CTGF), and TNF-α mRNA levels. The same diet-induced HCC model was adopted by Noguchi[41]. In this case, male Fisher-344 rats were treated with perindopril and eplerenone, a selective aldosterone blocker. Such drugs reduced both the liver fibrosis index and TGF-β. When administered in combination, they reduced the density of hepatic stellate cells and inhibited their proliferation through the reduction of aldosterone and angiotensin 2. Finally, both eplerenone and aldosterone attenuated the CD31 positive vessels in the liver along with inhibition of preneoplastic lesions (less than 4 foci/cm2vs about 8 foci/cm2in the control group) and,even in this report, a suppression of VEGF was recorded. Therefore, authors concluded that the effects of eplerenone and ACE-I were not simply due to the suppression of RAS, but other pathways, notably the hampering of the fibrosis process in this steatohepatitis model, could be involved.
Since insulin resistance status promotes neovascularization and has been associated with an increased risk of HCC, Yoshiji et al[42]initiated hepatocarcinogenesis by DEN in obese diabetic Otsuka Long-Evans Tokushima Fatty (OLETF) rats undergoing partial hepatectomy and used BCAAs and ACE-I, alone or in combination, at clinically comparable low doses, to assess the antineoplastic activity of these compounds. Both BCAAs and ACE-I significantly attenuated the development of dysplastic lesions, along with the suppression of both angiogenesis and VEGF expression. Used in combination, these two agents exerted an even more potent inhibitory effect. Finally, BCAAs and ACE-I induced an inhibitory effect on tubule formation in cultured endothelial cells showing a similar efficacy[42].
In a further three studies[43-45], the effect of ACE-Is or ARBs was tested only on cell lines. In particular, in HLF, HLE, HuH-7 and PLC/PRF/5 lines, it was demonstrated that telmisartan, but not valsartan, losartan and irbesartan, was able to arrest cell proliferation[43]. Similarly, only telmisartan blocked the cell cycle in phase G1 and reduced the population of cells in phase S, possibly by reducing the expression of cyclin D1 and cyclin E. Additionally, it was demonstrated that the block of proliferation could be secondary to the induction of AMPK/mTOR signaling in HCC cells. Finally, telmisartan increased the levels of phospho-p53 and decreased the levels of survivin in HLF cells, thus promoting HCC apoptosis, and it also inhibited angiogenesis by increasing bFGF levels in HLF cells as detected by the protein array.In Hep3B and QGY-7703 cells[44], it was shown that staphylococcal nuclease domain containing-1 (SND1) could play a role in promoting hepatocarcinogenesis and cell migration by triggering TGF-β signaling, a mechanism that was mediated by increasing activation of angiotensin receptor 1. In this experiment, losartan reduced the migration and invasive potential of HCC cells. Cook et al[45]transfected Ang(-S)Exp/pSVL plasmid, which causes the production of a stable, non-secreted form of angiotensinogen, in H4-II-E-C3 rat hepatoma cells. Thus, they discovered that this novel cell clone exhibited enhanced proliferation, which was blocked by losartan, but not by candesartan, although they were equally effective in competing with Ang II/AT1 receptor interactions on the cell surface. Furthermore, the addition of phenylarsine oxide, a molecule that blocks angiotensin receptor internalization,abolished the effect of losartan. Therefore, the authors concluded that losartan could be effective mainly on intranuclear angiotensin receptor.
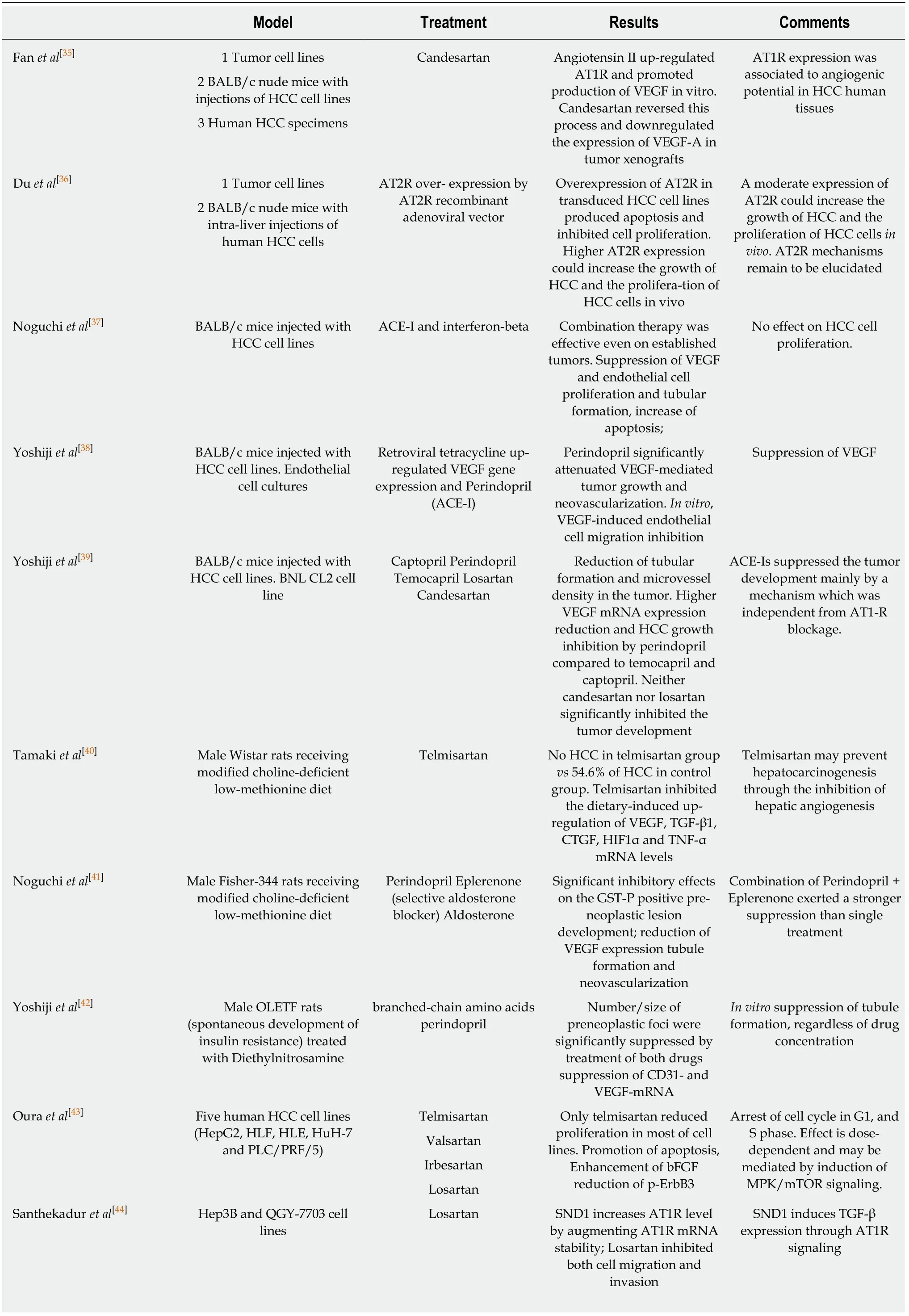
Table 3 Experimental studies on the effect of angiotensin-converting enzyme inhibitors or angiotensin ll type 1 receptor blockers in different hepatocellular carcinoma animal models and in hepatocellular carcinoma cell lines

Ang II: Angiotensin receptor; AT2R: Angiotensin II type 2 receptor; ACE-Is: Angiotensin-converting enzyme inhibitors; ARBs: Angiotensin II type 1 receptor blockers; HCC: Hepatocellular carcinoma; VEGF: Vascular endothelial growth factor; TNF: Tumor necrosis factor; TGF: Transforming growth factor; OLETF: Otsuka Long-Evans Tokushima Fatty.
DISCUSSION
The interest in the potential beneficial effects of RAS inhibitors against HCC started about two decades ago. Since then, several in vitro studies, using either different tumor cell lines or cell lines manipulated through adenoviral vectors, and numerous in vivo models have been used to demonstrate the antitumoral effect of RAS inhibitors on hepatocarcinoma development. We had to wait about 10 years for the first clinical study on the possible role of ACE-Is administration in the recurrence of HCC[13]. This study, designed as a randomized trial, was followed within a couple of years by two similar randomized trials from the same authors, all demonstrating the efficacy of the ACE-I perindopril in reducing tumor recurrence when used in combination with other drugs[13-15]. Interestingly, this effect was associated with a significant reduction of VEGF[13-15]and alpha-fetoprotein[13,14]serum levels. However, a significant effect on survival was not observed in any of these studies. The latter result requires some comments: only the first of these three studies reported a survival analysis (reported as “data not shown” in the other studies), which was interrupted at 42 mo, although the survival rate in the control group and the group receiving a combined treatment was 84% and 96%, respectively[13]. In consideration of this trend, we do not really know whether a longer period of follow-up would have led to significant survival differences. Moreover, it is plausible that a delayed recurrence in patients prevalently in Child A class (75%-87.5%) could also prolong their survival.
The more recent human studies are all observational retrospective cohort or casecontrol studies[7,16-21]. All these studies evaluated the effect of ACEIs and/or ARBs on overall survival. Among them, only one took into consideration tumor recurrence whereas another evaluated disease-free-survival[20,21]. With regard to tumor recurrence, the study of Facciorusso et al[20]was performed on patients with characteristics very similar to those reported in the randomized trials (patients with a low number and small-size tumors susceptible to RFA treatment). In addition, only patients undergoing antihypertensive therapy for at least two years before RFA were included to allow a reasonable induction period for the antiangiogenic and antifibrotic effects of such drugs. This study demonstrated a significant beneficial effect of ARBs, not only on time to recurrence but also on the overall survival after a period of observation of 96 months, which is twice the one reported in the randomized trials.
The study on disease-free survival was focused on metabolic factors, including obesity, diabetes, and hypertension, on patients undergoing HCC resection[21]. In this case, patients had a more advanced tumor disease, as demonstrated by the presence of pulmonary and bone metastasis at the follow-up, and underwent a liver resection including either one segment, more than one segment or even hemihepatectomy, plus removal of additional contiguous segments. In this study, neither overall survival nor disease-survival was improved by the anti-hypertensive treatment. However, the authors underline the fact that patients receiving angiotensin II-blocking agents had a better disease-free and overall survival rate than hypertensive patients not treated with angiotensin II-blocking agents.
The other observational studies conducted only on overall survival rates did not produce conclusive results since the treatment with RAS inhibitors was beneficial in one study[19], did not influence survival in two studies[17,18], and resulted either ineffective or even associated with an increased HCC risk in non-cirrhotic HCV patients in another study[16].
Among the possible explanations for these discrepancies, the different time of exposure to antihypertensive drugs assumes particular importance if we consider that RAS inhibitors would require a reasonable induction period to counteract the carcinogenetic process through their antiangiogenic effects. In the various studies, the antihypertensive treatment preceded for a variable period the first recorded liver cancer diagnosis or started at the time of HCC diagnosis, and the comparison of exposure during the follow up was difficult. Other explanations are the characteristics of the tumor (susceptible to surgical resection or locoregional therapy or advanced),the different stages of the underlying liver disease, and the concomitant pharmacological therapies/comorbidities potentially influencing tumor biology.
All experimental studies lead to concordant conclusions on the beneficial effects of RAS inhibitors on hepatocarcinogenesis, with some difference within the same drug class. However, it should be highlighted that this beneficial effect was mainly based on the demonstration that ACE-Is or ARBs inhibit the process of angiogenesis, the most studied and extensively exploited biological mechanism. The main aspects explored included: the involvement of VEGF serum levels or VEGF protein or mRNA expression[25,28-30,33-35,37-42]in endothelial cell growth and differentiation[46]; the contribution of HIF-1[28,40]as a transcription factor for VEGF[47]; the use of CD31[29-33,42][also known as platelet endothelial cell adhesion molecule 1 (PECAM-1)] to recognize endothelial cells[48]; endothelial cell proliferation and tubular formation in vitro and/or in vivo[30,32,34,37,39,41,42], a multi-step process triggered by VEGF[49].
Inhibition of tumor cells proliferation and induction of apoptosis are two mechanisms that have also been studied to explain how RAS inhibitors could counteract hepatocarcinogenesis. Some authors report an inhibitory effect of RAS inhibitors on tumor cell proliferation[25]or describe a block of proliferation secondary to the induction of AMPK/mTOR signaling[43], all studies performed by Yoshiji et al[30-33]and by others[35,37]do not confirm these findings, and one study even describes a pro mitogenic effect of angiotensin II[45]. Moreover, a complete overview of this aspect requires a better definition of the role of VEGF as a potential autocrine growth factor on tumor cells[46]and the relationship between angiotensin receptor 1 (AT1R) and angiotensin receptor 2 (AT2R)[36,50,51].
More consistent data seem to demonstrate the proapoptotic effect of RAS inhibitors on hepatic cancer cells[31,33,36,37,43].
Finally, the last possible antitumor mechanism related to the use of RAS inhibitors could consist of the suppression of inflammation by the reduction of TNF-α[25,40], TGFβ[25,29,40,41]and MMP-2[25,29], and an increase of tissue inhibitor of metalloproteinase(TIMP)-1, a negative regulator of MMP2[29].
All mechanisms mentioned above supporting the anti-tumor activity of RAS inhibitors were studied in HCC models, mostly induced by the carcinogenetic agent DEN or in rodents with xenotransplanted tumors, except in two studies[40,41]that used choline-deficient/low-methionine diets to induce steatohepatitis related HCC. Viral hepatitis still represents the principal cause of HCC in humans. The demonstration of a similar protective effect of ACE-I or ARBs in an animal model that mimics the progression of viral-related liver disease in humans, such as the HBV transgenic mouse model[52], would strongly support previous experimental data. In addition,since ACE-Is have been able to produce a prophylactic effect on hepatocarcinogenesis[29,32,33], this model could be used to test the RAS inhibitor influence on the expression of genes that are involved early on in the carcinogenesis[53]. In fact, the adoption of transgenic mouse models is widely used to test the effect of drugs or nutrients to counteract the process of carcinogenesis[54]. Finally, to clarify if RAS inhibitors could influence the progression toward overt HCC in humans, it is necessary to design randomized, controlled trials in which the treatment with these anti-hypertensive drugs is initiated in patients at high risk of HCC. Cirrhotics with a low number (≤ 3) of small tumors (≤ 3 cm) or a single larger tumor (≤ 5 cm), with a complete tumor ablation would be the ideal patients for this study considering that HCC recurrence at 3 years is observed in 48%-53% and 28%-33% in the presence of HCV infection or after HCV eradication, respectively[55,56].
In conclusion, all experimental data strongly support the ability of RAS inhibitors to counteract HCC development. In humans, this protective effect was confirmed when RAS inhibitors were used, prevalently in combination with other drugs, to prevent HCC recurrence. On the other hand, even if the results of RAS inhibitors on patient survival seem to be inconsistent, these findings are less conclusive. Further studies are necessary to evaluate whether their prolonged use could influence the progression of cirrhosis toward HCC.
ARTICLE HIGHLIGHTS
Research background
Hepatocellular carcinoma (HCC) represents about 90% of primary liver cancers and usually develops in patients with underlying liver cirrhosis. One of the major cancer hallmarks of HCC is the process of neoangiogenesis, which is thought to occur early in the carcinogenetic process.Theoretically, angiotensin-converting enzyme inhibitors (ACE-Is) and angiotensin II type 1 receptor blockers (ARBs) could have a role in HCC primary prevention since they reduce both neovascularization and the development of liver fibrosis.
Research motivation
The possible role of renin-angiotensin system (RAS) inhibitors in the prevention of HCC is still an attractive field of research, as suggested by the recently published experimental and clinical studies.
Research objectives
To elucidate the role of ARBs and ACE-Is in HCC.
Research methods
Literature was selected in August 2018, focusing on studies regarding ACE-Is, ARBs and HCCs.For this purpose, an electronic search of the literature was conducted using the online databases PubMed, Cochrane library, Scopus and Web of Science. Eligibility criteria were: (1) prospective or retrospective clinical studies; (2) epidemiological studies; and (3) experimental studies conducted in vivo or in vitro. We conducted the articles selection using a two-step approach, to evaluate whether they matched the eligibility criteria.
Research results
Thirty-one studies were selected. Three interventional studies showed that ACE-Is had a significant protective effect on HCC recurrence only when used in combination with vitamin K or branched chain aminoacids, without a significant increase of overall survival. Among six retrospective observational studies, mainly focused on overall survival, only one demonstrated a prolonged survival in ACE-Is group, whereas the two of them that also evaluated tumor recurrence showed conflicting results. All experimental studies displayed beneficial effects of RAS inhibitors on hepatocarcinogenesis. Numerous experimental studies, conducted either in animals and cell cultures, demonstrated the anti-angiogenetic and anti-fibrotic effect of ACE-Is and ARBs, thanks to the suppression of some cytokines such as vascular endothelial growth factor, hypoxia-inducible factor-1a, transforming growth factor-beta and tumor necrosis factor alpha. All or part of these mechanisms were demonstrated in rodents developing less HCC and preneoplastic lesions after receiving such drugs.
Research conclusions
Our systematic analysis of the literature allowed us to partially reinterpret the data supporting the ability of RAS inhibitors to counteract HCC. While there is reasonable research supporting their ability to reduce the HCC recurrence rate, we think that the conclusions of the randomized clinical trials on overall survival underestimated the potential use of these compounds. These conclusions are further supported by the solid experimental data on the anti-angiogenetic activity of RAS inhibitors, which all suggest their clinical use in the prevention of HCC development.
Research perspectives
We also proposed enlarging the future research on the relationship between RAS inhibitors and HCC to other possible anti carcinogenetic mechanisms.
杂志排行

World Journal of Gastroenterology的其它文章
- From 2-dimensional to 3-dimensional: Overcoming dilemmas in intestinal mucosal interpretation
- Optimizing radiotherapy with immune checkpoint blockade in hepatocellular carcinoma
- Contribution of pancreatic enzyme replacement therapy to survival and quality of life in patients with pancreatic exocrine insufficiency
- Hepatocellular adenoma: An unsolved diagnostic enigma
- Trimethylamine N-oxide attenuates high-fat high-cholesterol dietinduced steatohepatitis by reducing hepatic cholesterol overload in rats
- Brucea javanica oil emulsion improves the effect of radiotherapy on esophageal cancer cells by inhibiting cyclin D1-CDK4/6 axis