Effect of Blumgart anastomosis in reducing the incidence rate of pancreatic fistula after pancreatoduodenectomy
2019-06-13YaTongLiHanYuZhangChengXingChengDingWenMingWuQuanLiaoTaiPingZhangYuPeiZhaoMengHuaDai
Ya-Tong Li, Han-Yu Zhang, Cheng Xing, Cheng Ding, Wen-Ming Wu, Quan Liao, Tai-Ping Zhang,Yu-Pei Zhao, Meng-Hua Dai
AbstractBACKGROUND Pancreatic fistula is one of the most serious complications after pancreatoduodenectomy for treating any lesions at the pancreatic head. For years, surgeons have tried various methods to reduce its incidence.AIM To investigate and emphasize the clinical outcomes of Blumgart anastomosis compared with traditional anastomosis in reducing postoperative pancreatic fistula.METHODS In this observational study, a retrospective analysis of 291 patients who underwent pancreatoduodenectomy, including Blumgart anastomosis (201 patients) and traditional embedded pancreaticojejunostomy (90 patients), was performed in our hospital. The preoperative and perioperative courses and longterm follow-up status were analyzed to compare the advantages and disadvantages of the two methods. Moreover, 291 patients were then separated by the severity of postoperative pancreatic fistula, and two methods of pancreaticojejunostomy were compared to detect the features of different anastomosis. Six experienced surgeons were involved and all of them were proficient in both surgical techniques.RESULTS The characteristics of the patients in the two groups showed no significant differences, nor the preoperative information and pathological diagnoses. The operative time was significantly shorter in the Blumgart group (343.5 ± 23.0 vs 450.0 ± 40.1 min, P = 0.028), as well as the duration of pancreaticojejunostomy drainage tube placement and postoperative hospital stay (12.7 ± 0.9 d vs 17.4 ± 1.8 d, P = 0.031; and 21.9 ± 1.3 d vs 28.9 ± 1.3 d, P = 0.020, respectively). The overall complications after surgery were much less in the Blumgart group than in the embedded group (11.9% vs 26.7%, P = 0.002). Patients who underwent Blumgart anastomosis would suffer less from severe pancreatic fistula (71.9% vs 50.0%, P =0.006), and this pancreaticojejunostomy procedure did not have worse influences on long-term complications and life quality. Thus, Blumgart anastomosis is a feasible pancreaticojejunostomy procedure in pancreatoduodenectomy surgery. It is safe in causing less postoperative complications, especially pancreatic fistula,and thus shortens the hospitalization duration.CONCLUSIONSurgical method should be a key factor in reducing pancreatic fistula, and Blumgart anastomosis needs further promotion.
Key words: Blumgart anastomosis; Pancreaticojejunostomy; Postoperative pancreatic fistula; Pancreatoduodenectomy; Incidence
INTRODUCTION
Pancreaticoduodenectomy (PD), mostly known as the Whipple procedure, has been the standard technique for treating a wide variety of lesions at the pancreatic head for many years[1-4]. With the development of surgical techniques, improvements in surgical equipment, and progress in perioperative management, the mortality rate of PD has been reduced to <3% in high-volume academic medical centers[5-8]. However,the rate of postoperative morbidities, including postoperative pancreatic fistula(POPF, 3%-45%), delayed gastric emptying (7%-37%), anastomotic stenosis (3.3%-30%), infection (2.5%-23.3%), and abdominal bleeding (5%-12%)[9-13], remains as high as 30%. Among them, POPF is one of the most relevant and harmful complications. It is defined as leakage of pancreatic secretions from the damaged pancreatic duct after surgery. POPF can cause abdominal bleeding, infection, anastomotic leakage,pancreatic pseudocysts, or even enzymatic mediastinitis[10,14-16]. These conditions increase not only the hospitalization time and related cost, but also the risk of hospital death[10,14-16].
Pancreaticojejunostomy (PJ) is a major procedure in PD for reconstruction of the digestive system. The technique used to perform PJ determines the incidence rate of POPF to some degree[17-19]. The security of PJ and the risk of POPF are considered to be related to the texture of the pancreas, the diameter of the main pancreatic duct, and many other factors[17]. The traditional technique that has been used for PJ in PD and that is still used worldwide involves embedding the resected pancreatic end into the small intestine in an end-to-end fashion. This allows the anastomotic stoma to be quite large. In 2000, Blumgart proposed a U-style duct-to-mucosa anastomotic procedure that was expected to more safely reduce the rate of POPF[18,19]. In this article, we share our experiences and clinical data regarding PD to identify the differences and advantages of these two kinds of PJ procedures. We also provide suggestions regarding pancreatic surgical treatments in the Chinese population, as well as a supplement of the risk calculator of POPF, to improve the prevention of POPF after PD.
MATERIALS AND METHODS
From January 2008 to December 2014, 402 patients underwent PD for benign or malignant lesions at the pancreatic head at Peking Union Medical College Hospital.Six experienced surgeons were involved in this study and all of them performed both Blumgart anastomosis and traditional embedded PJ. The inclusion criteria were: (1) A history of treatment by standard PD, excluding pylorus-preserving PD, pancreatic head resection with segmental duodenectomy, and duodenum-preserving pancreatic head resection; (2) availability of complete preoperative, intraoperative,postoperative, and follow-up data; (3) and provision of written informed consent for the operative procedures and related data. The exclusion criteria were: (1) A history of extensive PD procedures with vascular resection and anastomosis, or combined resection of other organs; and (2) a history of surgical treatment of any upper abdominal lesions before the current hospital admission. As a result, 291 patients were included in our study; 201 underwent Blumgart anastomosis, and 90 underwent traditional embedded PJ.
Preoperative examinations, including measurement of blood parameters, liver function, kidney function, and tumor markers as well as the performance of ultrasound and contrast-enhanced computed tomography, were routinely performed on all patients. Other auxiliary examinations were performed as necessary to obtain further information regarding the lesions. Intraoperative information including the operation time, blood loss, blood transfusion, pancreatic texture, diameter of the pancreatic duct, and other parameters were collected along with postoperative information including complications, hospitalization time, reoperation, hospital death, and other data. Routine biochemical parameters were measured in our hospital’s clinical laboratory. Postoperative complications were evaluated according to the modified Clavien-Dindo classification[20], and delayed gastric emptying, biliary fistula, abdominal bleeding, and intraperitoneal infection were diagnosed according to the classification of the International Study Group on Pancreatic Surgery(ISGPS)[21,22]. We regarded Clavien-Dindo grade ≥ 3 complications, and ISGPS grade ≥B delayed gastric emptying as severe in our study.
According to the definition established by the International Study Group of Pancreatic Fistula (ISGPF), POPF is an abnormal communication between the pancreatic ductal epithelium and another epithelial surface containing pancreasderived enzyme-rich fluid[16,23,24]. According to the updated definition of POPF by the ISGPF in 2016[16], “biochemical leak” is an “increased amylase activity > 3 times upper limit institutional normal serum value” instead of grade A POPF. Grade B and Grade C POPF remains the same definition.
The study was reviewed and approved by the Peking Union Medical College Hospital Institutional Review Board. Fisher’s tests, t-tests, and t’-tests were used in statistical analyses, which were performed using SPSS 22.0 (IBM Corp., Armonk, NY,United States) and Prism 7 (GraphPad Software, La Jolla, CA, United States). A Pvalue < 0.05 indicated a statistically significant difference.
RESULTS
Patients’ demographic and clinical characteristics
The basic characteristics of the 291 patients are summarized in Table 1. Overall, 201 patients underwent PD with Blumgart anastomosis; 109 were male and 92 were female, with an average age of 53.28 years. Ninety patients underwent PD with traditional embedded anastomosis; 41 were male and 49 were female, with an average age of 54.54 years. There were no significant differences in these basic characteristics between the two groups.
With respect to the patients’ medical history and personal history, there were no significant differences in preoperative diabetes, cholecystolithiasis, cardiovascular disease, smoking, or drinking between the two groups. No significant differences were found in the preoperative laboratory parameters (serum albumin, total bilirubin,direct bilirubin, cancer antigen, and other parameters) or the diameter of the lesion at the pancreatic head as detected by adjuvant examinations (Table 1).
Although the postoperative pathological diagnoses varied among the patients, the relative proportion did not show significant differences. Pancreatic ductal adenocarcinoma was the most common pathological diagnosis of the mass at the pancreatic head in our study and required adequate tumor resection and lymph node dissection. Solid-pseudopapillary tumors were usually seen in young patients, while pancreatitis was related to excessive drinking. No significant differences were found in the incidence of intraductal papillary mucinous neoplasm, cystic lesions, or neuroendocrine tumors (Table 1). We also calculated and analyzed the cases of each anastomosis for each surgeon, and found no statistically significant differences. Thus,surgeons themselves were not an influential factor in our study.
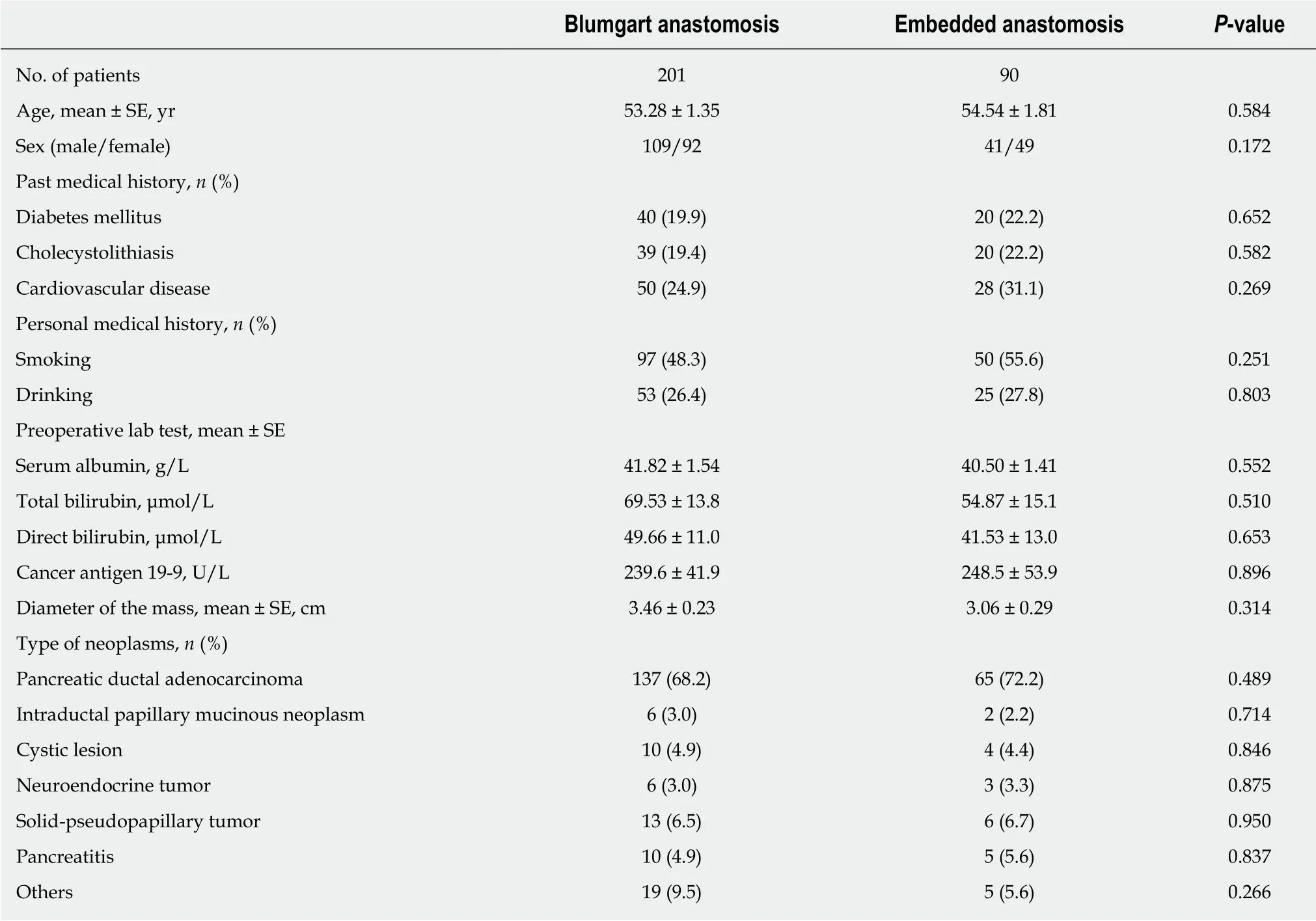
Table 1 Demographic and clinical characteristics of 291 patients
Perioperative results and long-term follow-up status
The mean operative time was significantly shorter in the Blumgart group than in the embedded group (343.5 ± 23.0 min vs 450.0 ± 40.1 min, P = 0.028), while the intraoperative blood loss volume and blood transfusion rate were not significantly different. The diameter of the pancreatic duct, the texture of the pancreas, and the insertion of Wirsung duct were not significantly different between the two groups(Table 2).
Two patients died at the hospital after their surgery. Twelve patients in the Blumgart group and eleven patients in the embedded group underwent a secondary operation mainly because of abdominal bleeding. The overall Clavien-Dindo grade ≥3 complications and the duration of PJ drainage tube placement were significantly different between the two groups (11.9% vs 26.7%, P = 0.002; and 12.7 ± 0.9 d vs 17.4 ±1.8 d, P = 0.031, respectively). POPF, as the most important observation point in our study, indicated the advantages of Blumgart anastomosis. More patients in the embedded group than in the Blumgart group developed grade B and C POPF (15.6%vs 8.0%, P = 0.049; and 5.6% vs 1.5%, P = 0.050, respectively). In contrast, there were no significant differences in abdominal bleeding, intraperitoneal infections, biliary fistula, or delayed gastric emptying between the two groups. Nevertheless, the postoperative hospitalization duration was shorter in the Blumgart group than in the embedded group (21.9 ± 1.3 d vs 28.9 ± 1.3 d, P = 0.020). Consequently, Blumgart anastomosis was a practicable procedure for PJ, with a safer outcome in terms of POPF development. Blumgart anastomosis could reduce the duration of PJ drainage tube placement and the postoperative hospitalization duration (Table 2).
Using the POPF risk score calculator[25-28], we compared all 291 patients according to their POPF ISGPF grade (<B, 253 patients; ≥B, 38 patients) and summarize their age,sex, body mass index, method of PJ, pathologic diagnoses, pancreatic texture,pancreatic duct diameter, and intraoperative blood loss in Table 3. We found that the PJ technique was a contributory factor to POPF. Patients who underwent Blumgart anastomosis during PD were more likely to develop mild POPF (only biochemical leak or no pancreatic fistula) (71.9% vs 50.0%, P = 0.006), while other parameters showed no significant differences. Therefore, Blumgart anastomosis could be a decisive protective factor for POPF (Table 3).
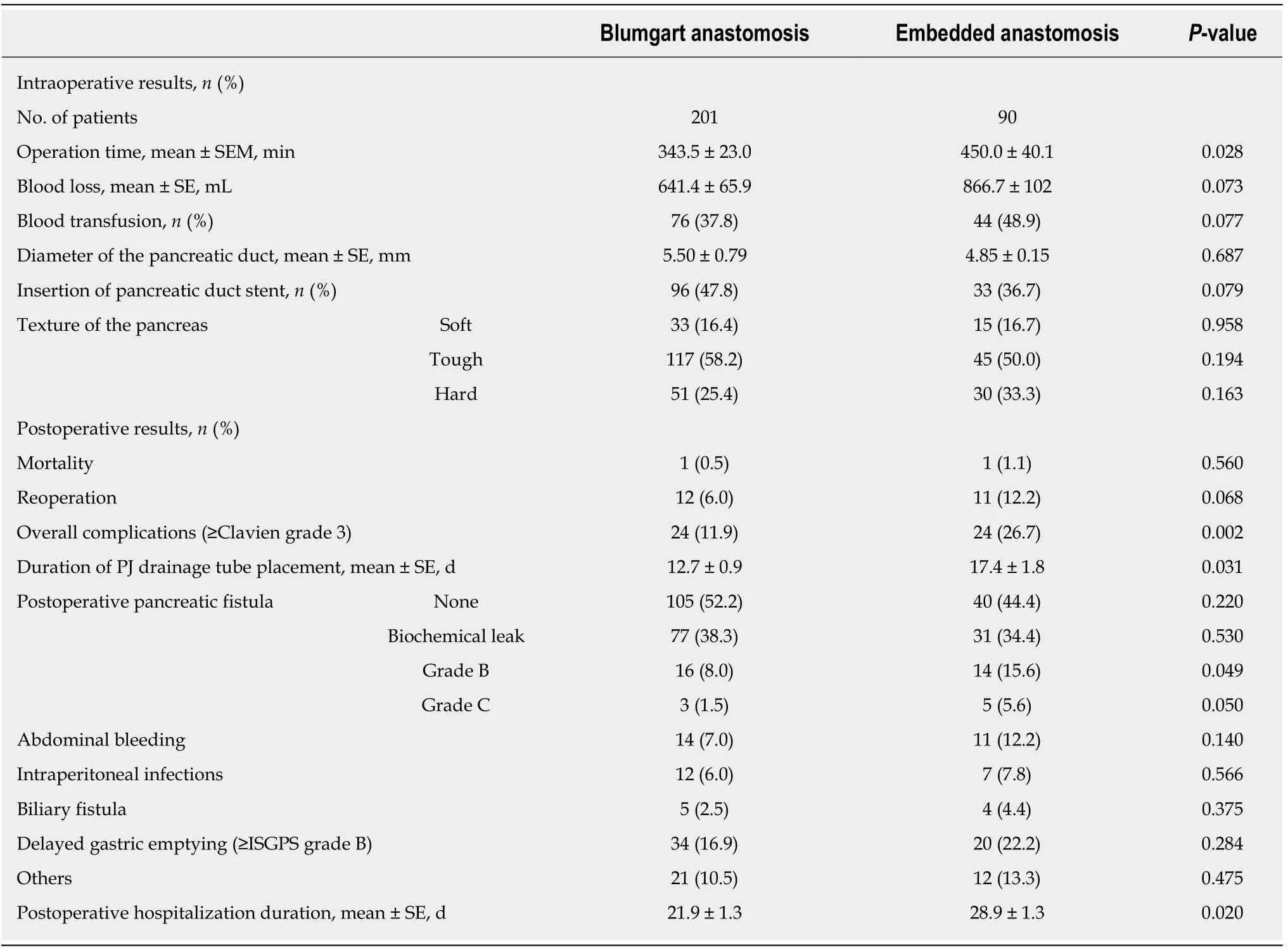
Table 2 lntraoperative and perioperative statuses
The follow-up period was dependent upon the pathological diagnosis of the mass at the pancreatic head. Overall, the maximum survival period of the patients with benign or low-grade malignant lesions was > 60 mo after PD. However, the 5-year survival rate of patients with pancreatic adenocarcinoma was < 10%. No patients in our study developed delayed POPF. No more than 8% of patients had an anastomotic stenosis several years after surgery, while the interventional treatments were beneficial. Blumgart anastomosis did not affect the long-term status.
DISCUSSION
PD has long been the standard technique for treatment of any lesions at the pancreatic head[1,2,29]. The first two-stage excision procedure was not accomplished until 1909, and Whipple and Child finally evolved it into a regular operation in 1940 and 1944[3,4]. The mortality rate associated with PD in the mid-19thcentury was extremely high, leading to a strict evaluation of surgeons’ qualifications[30-33]. With the development of modern surgery, PD is now very safe.
However, because of the substantial surgical damage and high level of difficulty in PD, the postoperative morbidity is still very high[9-13]. When a patient has undergone a pancreatic surgery, the most likely cause of POPF is leakage of the pancreatic-enteric anastomosis[16]. Although the comprehensive conditions and advantages of modern surgery have swiftly developed during the past few decades, POPF still remains one of the most harmful complications after pancreatic surgery, and its incidence still ranges from 3%-45% at high-volume centers[27,34-41]. The updated POPF grade is referenced in the Methods section to provide a clearer understanding of the POPFrelated mortality rate, morbidity rate, hospital stay, and economic impact in this article[42-45].
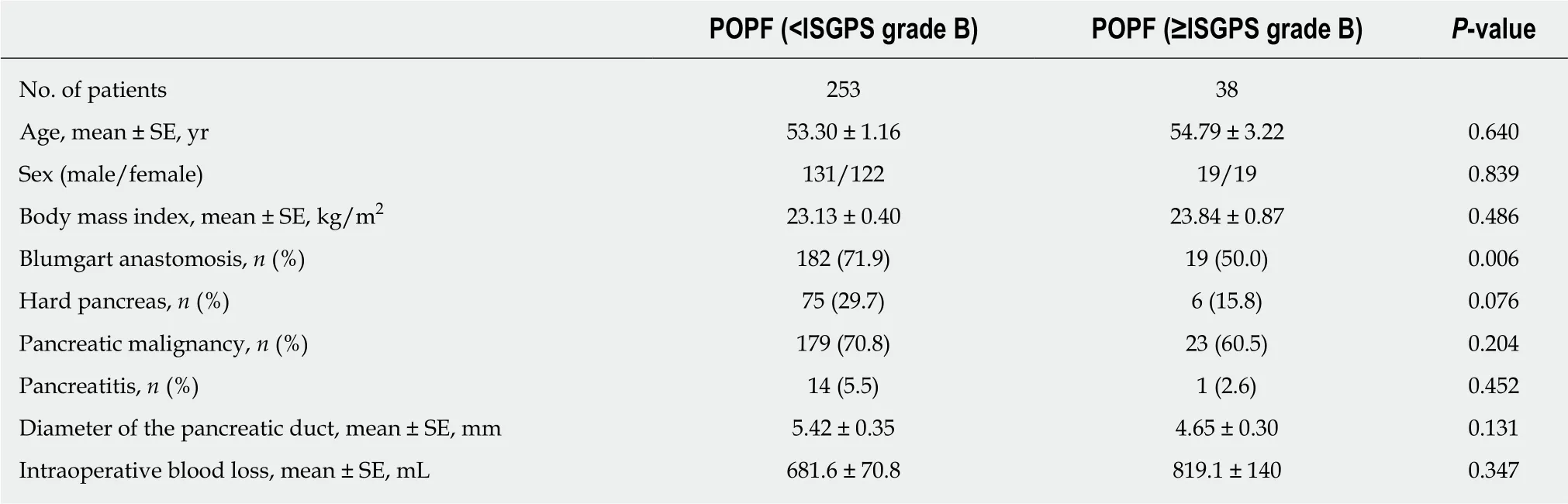
Table 3 lnformation of the patients with postoperative pancreatic fistula
The POPF risk score calculator regards the pancreatic texture, pathology, pancreatic duct diameter, and intraoperative blood loss volume as the most important factors indicating the severity of POPF[25-28]. A softer pancreas, diseases other than pancreatic cancer and pancreatitis, a smaller pancreatic duct, and a higher blood loss volume during the operation will result in a more severe clinical situation and a higher ISGPF grade of POPF. Preventive therapy is suggested in patients with a higher POPF risk score before their condition becomes uncontrollable. A good nutritional status, normal levels of serum albumin and hemoglobin, and the use of somatostatin are necessary to increase the success rate in treating POPF. Nevertheless, all of these preventive measures and treatments are dependent upon a reliable PJ procedure during PD.Assurance of the PJ procedure is an independent protective factor in avoiding POPF[17,18].
Because many parts of the digestive system are resected during PD, reconstruction is very important to maintain the vital activity of this system. As the name suggests,PJ is a procedure that involves reconnection of the remnant pancreas and the jejunum.After the reconstruction, the pancreatic duct is connected to the jejunum, and enzymerich pancreatic juice is able to enter the intestinal tract to assist with digestion.Traditionally, PJ is an end-to-end, embedded procedure in which a small part of the remnant pancreas is placed into the jejunum. In 2000, Blumgart devised a novel ductto-mucosa, U-shaped anastomosis to reconnect the remnant pancreas and the jejunum[18,19]. In the present article, we share our data and experiences to prove the superiority of Blumgart anastomosis in reducing the risk of POPF in Chinese patients[46-51].
In the embedded anastomosis, the end of the jejunum is sutured to cover the end of the remnant pancreas. This procedure is classic but complicated, greatly increasing the operative time and causing relatively more blood loss according to our study.Additionally, the repeated suturing and knotting cause damage to the pancreas and the end-to-end anastomosis causes an extension of the jejunum wall, resulting in a thinner wall of protection outside the end of the pancreas. If the remnant pancreas is thick, the protection will be weaker, and the clinical situation will worsen. Moreover,because the pancreatic stump is completely exposed in the intestine, the activated trypsin slows the healing of the anastomotic stoma and increases the incidence rate of POPF. In 1996, Peng improved this procedure by only placing simple sutures at the anastomotic stoma to reduce the destructive effect of repetitive placement of sutures on the end of the pancreas; however, the problems induced by trypsin and an oversized pancreatic stump still existed, and the intraoperative time was not shortened. In comparison, none of these issues are problematic in the duct-to-mucosa,U-shaped Blumgart anastomosis[18,19].
Furthermore, the pancreatic remnant can be tightly fixed to the seromuscular layer of the jejunum in modified Blumgart anastomosis. Meanwhile, a duct-to-mucosa suture will reinforce the anastomotic stoma and free the pancreatic tissue from tension and shear forces[18,19]. As a result, Blumgart anastomosis was welcomed by many surgeons once it was reported. Although some studies showed no obvious advantages of Blumgart anastomosis over other PJ procedures, and other studies did not compare Blumgart anastomosis with the traditional embedded anastomosis,Kleespies, Fujii, and Grobmyer supported the excellence of the Blumgart procedure in their articles[47-52]. Based on the present study, which involved a clear retrospective analysis of 291 patients and a follow-up period of >5 years, we are able to strongly recommend Blumgart anastomosis in PD in Chinese patients.
According to our study, the advantages of Blumgart anastomosis were shorter operative time, shorter duration of PJ drainage tube placement, shorter postoperative hospitalization time, less postoperative complications, better situation of POPF, and better postoperative recovery. Besides, Blumgart anastomosis was safe and accessibility, without disadvantages in patients’ long-term follow-up status, which indicated its non-inferiority. Consequently, we strongly recommended this PJ procedure in PD. However, according to the experiences of surgeons, Blumgart anastomosis may be hard to perform when the main pancreatic duct was too thin.When the diameter of the main pancreatic duct was less than 1 mm, there may be no proper stent to be used. In such situation, traditional embedded PJ would be able to protect the main pancreatic duct from being sewn and closed. On the other hand, if an applicable stent could be used to sustain the main pancreatic duct, Blumgart anastomosis was still preferred.
In some other studies, sex, body mass index, and preoperative blood glucose level were also significant factors associated with POPF[53]. All of these factors can be related to or result from alcohol intake, resulting in changes in the pancreatic texture.On the other hand, variations in intraoperative blood loss may be associated with abdominal adhesions, which is reflected by the serum levels of systemic inflammatory factors including the erythrocyte sedimentation rate, C-reactive protein level, and others. Additionally, the diameter of the pancreatic duct can be detected in some elaborate ultrasonic preoperative adjuvant examinations. As a result, the POPF risk score calculator could be changed to a preoperative pancreatic fistula risk score calculator that includes sex, body mass index, alcohol intake, diabetes, pathology (by preoperative puncture), pancreatic duct diameter (by preoperative examinations), and levels of serum inflammatory factors (by preoperative laboratory tests). To verify this hypothesis, a prospective study is ongoing in our hospital with more complete preoperative details to describe and predict the risk and grade of POPF. Certainly, we have established Blumgart anastomosis as the standard PJ procedure in our research.We hope that we can now finally provide valuable advice to our patients to help them change their living habits before their pancreatic operation. This will increase the possibility of avoiding this harmful postoperative complication and achieving a better outcome after pancreatic surgery. More studies, especially prospective randomized controlled studies, are needed to promote Blumgart anastomosis in PD, and to improve the risk prediction of POPF after PD.
ARTICLE HIGHLIGHTS
Research background
Postoperative pancreatic fistula (POPF) is a serious complication of pancreaticoduodenectomy(PD). Surgical procedure of pancreaticojejunostomy (PJ) in PD is closely related to POPF, and the traditional method is embedding the remnant pancreatic end into the small intestine. Since the incidence rate of POPF remains high, Blumgart anastomosis, a new U-style duct-to-mucosa procedure of PJ, was proposed. However, there were no enough data to support the benefits of Blumgart anastomosis in reducing the rate of POPF. Thus, our present study would give more evidence, analysis, and suggestions to make the postoperative recovery after PD better.
Research motivation
We analyzed and explained the details and benefits of Blumgart anastomosis compared with traditional embedded PJ in PD. We proved that a better choice of PJ procedure could certainly reduce the incidence rate of POPF, and subsequently reduce the mortality of pancreatic surgery.
Research objectives
We suggested to add the surgical methods into the risk calculator of POPF, and the technique of Blumgart anastomosis should be further promoted.
Research methods
In this observational study, a retrospective analysis was made to compare the preoperative,intraoperative, perioperative, and long-term follow-up courses between 201 patients with Blumgart anastomosis and 90 patients with traditional embedded PJ in PD.
Research results
Blumgart anastomosis took less operative time, less days of PJ drainage tube placement, and less postoperative hospital stay. The overall complications were reduced, including the incidence rate of severe POPF. These results indicated the advantages of Blumgart anastomosis in PD, and noninferiority in long-term status. More studies, especially prospective clinical trials, are needed to confirm our findings.
Research conclusions
The new findings of this study are the detailed benefits of Blumgart anastomosis, and the new theory, original insights, and new hypotheses are to take surgical methods into the consideration of the risk calculator of POPF. The appropriate summarizations of this study are the benefits of Blumgart anastomosis in intraoperative and postoperative courses, as well as its non-inferiority features in the long-term statuses. There were neither basic experiments nor new statistical methods used. Blumgart anastomosis needs further promotion in the future.
Research perspectives
To further promote Blumgart anastomosis, more studies, especially prospective randomized controlled trials, are needed. Besides, since surgical methods are important in reducing postoperative complications of PD, new PJ procedures could be proposed based on Blumgart anastomosis.
杂志排行

World Journal of Gastroenterology的其它文章
- From 2-dimensional to 3-dimensional: Overcoming dilemmas in intestinal mucosal interpretation
- Optimizing radiotherapy with immune checkpoint blockade in hepatocellular carcinoma
- Contribution of pancreatic enzyme replacement therapy to survival and quality of life in patients with pancreatic exocrine insufficiency
- Hepatocellular adenoma: An unsolved diagnostic enigma
- Trimethylamine N-oxide attenuates high-fat high-cholesterol dietinduced steatohepatitis by reducing hepatic cholesterol overload in rats
- Brucea javanica oil emulsion improves the effect of radiotherapy on esophageal cancer cells by inhibiting cyclin D1-CDK4/6 axis