Recalcitrant distal humeral non-union following previous Leiomyosarcoma excision treated with retainment of a radiated nonangiogenic segment augmented with 20 cm free fibula composite graft:A case report
2019-04-24MartinGathenGraysonNorrisSimonKayPeterGiannoudis
Martin Gathen,Grayson Norris,Simon Kay,Peter V Giannoudis
Abstract
Key words: Humerus;Fibular graft;Bone tumor;Osseous defect;Implant failure;Leiomyosarcoma;Case report
INTRODUCTION
After resection of musculoskeletal tumors and following radiotherapy,bone necrosis,osteopenia or radiation-induced neoplasm can be seen[1].Osteoradionecrosis after radiotherapy often shows a long latent period and the incidence rate is described between 1%-11%.Noteworthy,pathologic fractures become a feared complication and can occur even years after therapy[2].
When pathological fractures occur non-operative therapy rarely provides satisfactory return of function or pain relief.Stabilisation with different methods such as plate fixation,intramedullary nails,external fixators and segmental prosthetic implants can be used with reported osteosynthesis failure rates between 12.2%-22%[3,4].In cases of segmental bone defects especially those associated with soft-tissue defects,reconstructive options remain limited.Additionally,the presence of previous radiated bone with no inherent angiogenic properties makes this problem even more challenging[3].
In the herein case study,we report the management of a recalcitrant distal humeral non union with implant failures after tumor resection and radiotherapy.Our strategy of optimum fixation accompanied by biological augmentation led to a successful outcome.
CASE PRESENTATION
Chief complaints
A 52-year-old female patient was referred to our institution with persistent pain of the right humerus due to recurrent implant failure and non-union of the right humerus
History of present illness
Ten years previously,the fracture area she was being treated for,had been diagnosed with a grade 2 Leiomyosarcoma.After surgical resection and free tissue transfer(groin flap for covering),a post-operative radiotherapy with 60Gy in 30 fractions was prescribed.The patient then sustained a closed fracture of the right humeral shaft whilst lifting a light object.The fracture was then stabilised with a retrograde nail but fixation failed after 18 mo (Figure 1).
The fracture was next revised to a double plate fixation and biological enhancement was achieved with the implantation of autologous bone grafting harvested from the pelvic iliac crest (Figure 2).However,14 mo after the revision,the patient presented with non-union associated with implant failure and was referred to our institution (Figure 2).
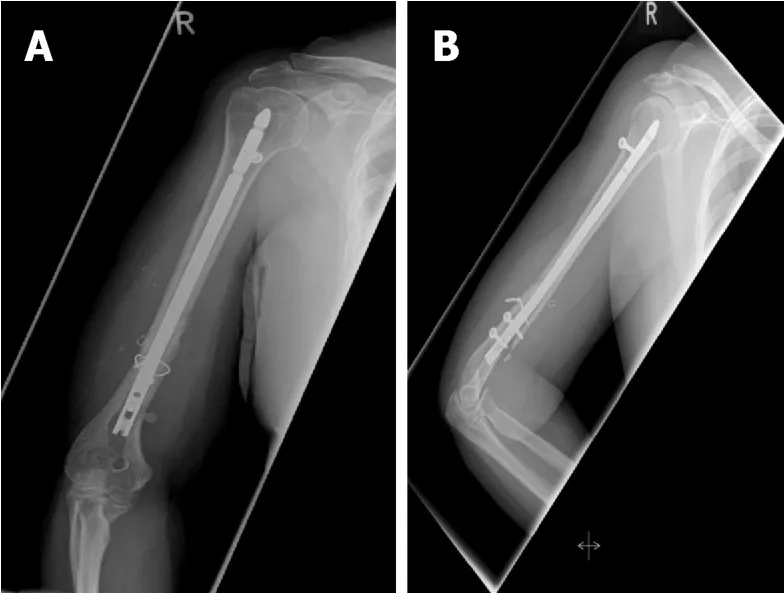
Figure1 Implant failure after intramedullary nailing.
History of past illness
The patient had a free previous medical history.
Physical examination
The patient showed movement dependent pain of the right upper arm.Due to the implanted double plate fixation there was no instability.After radiation and previous surgery the skin was compromised by massive scar tissue formations.The patient showed no clinical signs of infection and no neurological deficits.
Laboratory examinations
Blood analysis as well as urine analysis were normal.Electrocardiogram,chest X-ray and arterial blood gas were also normal.
Imaging examinations
A staging computed tomography and magnetic resonance imaging scan of the upper arm showed no local recurrence or metastatic disease.
FINAL DIAGNOSIS
Distal humeral non-union associated with implant failure after resection of a Leiomyosacroma and following radiotherapy.
TREATMENT
Due to the previous radiotherapy and concerns about the possibility of low-grade infection,a two-stage revision was planned.Initially,the implants were removed and the non union area was debrided with multiple tissue samples sent to microbiology.A defect of 2.5 cm was created.Temporary stabilisation was performed using a compound osteosynthesis with nancy nails and bone cement followed by wound closure (Figure 3).The notes from the referral hospital center were requested in order to identify the extent of the previous bone radiated area.Two out of the 5 culture specimens grew staphylococcus aureus and the patient was treated with appropriate antibiotics for a period of 6 wk.
During the second stage and despite the induction of the induced membrane (IM)(which can promote bone regeneration),it was felt that autologous bone grafting in isolation would not be successful since the bone edges around the non union site were lacking angiogenic capacity and healing potential[5].The zone of the previous radiotherapy was assessed to have been from the olecranon fossa to 20 cm proximally just below the lesser tuberosity.In view of the extent area of radiated bone it was decided to leave this section of humerusin situand considered it in our reconstruction strategy as a scaffold.
A composite fibula vascularised graft was harvested from the ipsilateral tibia 20 cm in length and the vascular graft was connected to the brachial artery.The fibula graft was placed anterior laterally and two plates were used for stabilisation.One to provide continuity to the distal and proximal radiated humeral segments and the other to stabilise the fibula on the humerus (Figure 4).The previous created bone defect was addressed by shortening of the humeral shaft by 2.5 cm.Autologous bone graft was implanted distally.

Figure2 Second implant failure after ORIF.
OUTCOME AND FOLLOW-UP
After a period of 6 months osseous healing was observed.Twelve months following reconstruction one plate was removed due to soft tissue irritation.At final follow up(2 years later),hypertrophy of the fibula graft was noted with restoration of right arm function (Figure 5).The range of motion was full flexion,minus 200of full extension and full supination pronation of the forearm.Shoulder movements were full and pain free.
DISCUSSION
Pathological fractures of the humerus are common and associated with high reoperation rates[6].Sarahrudiet al[4]analysed the treatment of 39 patients with pathological humerus fractures and reported a complication rate of 14.6%.They found intramedullary stabilization to be most reliable for fractures of the diaphysis and ORIF preferable for the treatment of metaphyseal fractures and for patients with a solitary metastasis[4].In a different study,a cemented hemiprosthesis for proximal fractures was found most suitable and intramedullary nailing for lesions in the diaphysis[6].
Previous radiotherapy in the medical history of pathological fractures and particularly non union complicates treatment options and fracture healing potential due to radiation-induced osteopenia and loss of bone vitality.In our case there were 2 previous attempts of reconstruction without success.Although the masquelet technique was employed[5],it was felt that even with the presence of the IMin situ,which is highly vascular,containing growth factors and osteoprogenitor cells,the chance of healing was low.Consequently,it was deemed essential to bring vascularity to the region and structural support with the free fibula composite vascularised graft being the ideal option to bridge the avascular area of the humerus.Moreover,the retainment of the humeral avascular segment would simplify the reconstruction process by acting as a scaffold within the local environment.The double plate approach provided adequate mechanical stability until evolution of healing occurred.
Segmental defects in long bones are challenging tasks especially when further factors such as poor soft tissue,osteonecrosis or infections are present.A variety of techniques and their combinations have been described such as bone transportation,IM Technique,autograft bone grafting,and megaprosthesis[7-9].
Using a vascularized fibula graft is a highly sophisticated technical procedure with potential complications including non-union,graft fracture and donor site morbidity.Advantages include the straight configuration and dual vascularity (endosteal and periosteal).The method provides shorter duration than therapy with bone transportation and a tendency for hypertrophy in response to microscopic stress fractures[10,11].The IM Technique is described for diaphyseal defects from 5 cm to 25 cm allowing formation of bone by means of endochondral ossification with high union rates of 90%[12].
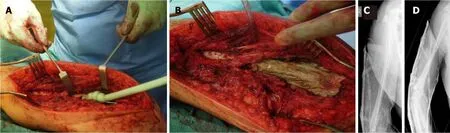
Figure3 Induced membrane technique.
In our case we employed a combination of techniques,including the IM,autologous bone grafting for the distal humerus segment,a composite vascular fibula graft and retainment of the radiated-devitalised humeral segment as a scaffold.One may argue that it is controversial that the avascular bone was leftin situbecause it is a widely accepted concept to resect avascular bone tissue completely[13,14].However,this approach was found useful,eliminating the need of considering the use of a megaprosthesis and facilitating the reconstruction process by acting as a bridge allowing implantation of the fibula graft.
CONCLUSION
We believe that the presented management of treatment of a recalcitrant humeral non-union with a background of previous pathological fracture following radiotherapy for leiomyosacroma is a promising alternative and should be considered as an option of treatment,when contemplating reconstruction of such complex cases.
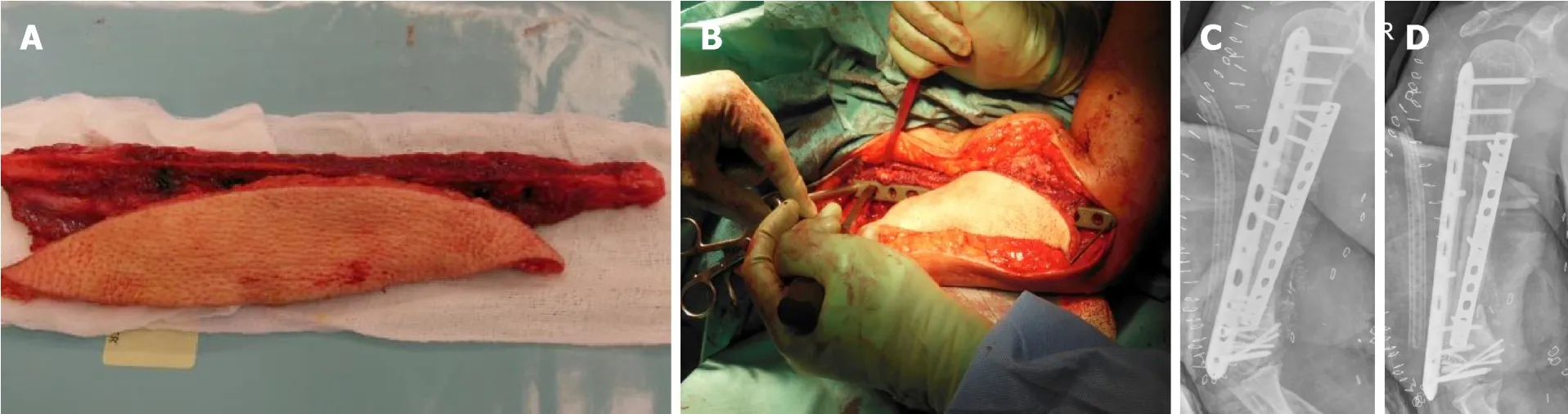
Figure4 Vascularized fibula graft and plate fixation.

Figure5 Final result.
