Fracture of allograft interbody spacer resulting in post-operative radiculopathy:A case report
2019-04-24AndrewsKyleAndreaRowlandJacobStirtonHosseinElgafy
Andrews Kyle,Andrea Rowland,Jacob Stirton,Hossein Elgafy
Abstract
Key words: Transforaminal lumbar interbody fusion;Interbody fusion;Allograft interbody spacer;Postoperative radiculopathy;Graft breakage;Case report
INTRODUCTION
Transforaminal lumbar interbody fusion (TLIF) is a surgical technique that is utilized for lumbar pathologies for which segmental fusion is indicated[1-5].This method was developed to improve upon previous surgical methods such as anterior or posterior lumbar interbody fusion.Its unilateral approach can reduce the risk of durotomy,nerve damage,or epidural fibrosis relative to posterior lumbar interbody fusion while decreasing incidence of vascular injury and procedure time relative to anterior lumbar interbody fusion[2,5,7].
Prosthetic allograft interbody spacers are utilized during TLIF procedures to restore anterior column support and disc height in patients with degenerative disc disease and spondylolisthesis[4,8-11].The demineralized surface of the implant’s allogenic bone provides osteoconductivity to aid in osteogenesis and scaffolding for new bone formation along its surface and successful interbody arthrodesis[12,13].
Instrumentation or bone graft-related complications of the TLIF procedure typically involve graft misplacement or migration,screw fracture or misplacement,or rod breakage[14-21].The authors report on a complication involving a fractured allograft spacer that displaced into the neural foramen impinging on the exiting nerve root during a two-level TLIF.Revision surgery was carried out to remove the broken allograft fragment from the right L5 foramen.To the best of the authors’knowledge,a complication such as this has not been described in the literature.
CASE PRESENTATION
Chief complaints
A 50-year-old male who had previously undergone L5/S1 laminectomy,instrumentation and attempted posterolateral fusion presented to the clinic 2 years after this procedure with chronic low back pain and numbness/pain radiating down his right lower extremity,and to a lesser degree the left lower extremity.
Imaging examination
Computed tomography scan and magnetic resonance imaging confirmed L5/S1 nonunion with hardware loosening and adjacent segment disc degeneration and spinal stenosis.Risks,benefits,and alternative management were discussed and the patient elected to proceed with hardware removal,L4/5 decompression using a rightsided approach,and L4-S1 TLIF and posterior spinal fusion with iliac crest autograft.The procedure was carried out as planned with an allograft interbody spacer impacted into the anterior half of the disk space at both the L4/5 and L5/S1 levels without any obvious intraoperative complication.Soon after awaking from anesthesia,the patient began complaining of right leg radiculopathy along the L5 dermatome.Plain films (Figure 1A and B) showed no obvious complication.Computed tomography scan was then obtained which revealed allograft spacer fracture with fragment displacement into the right L5 neural foramen (Figure 2A-C).
从表1可以看出,淮河流域干旱分区共分为5个一级区,10个二级区。就5个一级区、10个二级区而言,大区内部具有其相似性,尤其是在农业干旱发生的层面上,而二级区之间又有区域差异性,以下对各区域的特点进行分析,可为各分区干旱治理技术的发展提供科学依据。
TREATMENT
The patient was subsequently taken back to the operating room for revision.The broken allograft pieces were identified and extracted (Figure 3).The intact portion of the allograft interbody spacer was left in place.Immediately following the procedure the patient’s pain improved,and he was discharged home on post-operative day 2.
OUTCOME AND FOLLOW-UP
Over subsequent clinic visits,right leg L5 radicular pain resolved,and in the last follow-up 12 mo after the index procedure computed tomography scan confirmed sound interbody and posterolateral fusion with no foraminal bone fragment or stenosis (Figure 4A and B,and Figure 5A-C).
DISCUSSION
Complications resulting from the interbody fusion procedures have been well reported since the technique was first described by Harmset al[22]in 1982.These complications,however,have typically involved infection,durotomy,bleeding,malpositioned hardware,or pseudoarthrosis[5,11,17,19,21].Hardware failure reports have been limited to interbody device migration/subsidence,screw fracture,or rod breakage[18,20,23-25].Savilleet al[26]showed that when a posterior lumbar interbody fusion spacer is compressed,failure is observed by subsidence of the graft into the upper or lower vertebral bodies and never internally within the graft itself.There have been case studies reporting vertebral fracture following TLIF procedures that may have resulted from the implantation process itself[26].
The interbody fusion technique involves using vertebral endplate shavers to prepare the disc for the fusion.The graft size is determined using trial spacers.Starting with a smaller size trial spacer and under lateral view fluoroscopic guidance,the trial spacer is gradually increased until the most secure fit is achieved,and then selected for the corresponding graft size.The current case reported is unique as part of the graft was sheared off,which resulted in fractured pieces migrating to the right L5-S1 neural foramen,compressing the exiting nerve root,and resulting in right L5 radiculopathy.The remaining bulk of the interbody spacer remained intact and well positioned.No damage to the vertebral bodies was noted.
According to Janssenet al[27],allograft spacers have been tested to withstand 25000 N of force compared to the compressive strength of a vertebral body itself as 8000 N.This assumes that the compressive strength of the spacer was equally distributed across the surface of the spacer,as opposed to a localized force applied to a portion of the spacer.As the patient experienced a limited axial load on his vertebrae following surgery,it is unlikely the fracture of the spacer occurred post-operatively.No reports were found of the surgeons experiencing significant difficulty or resistance during the insertion of allograft interbody spacers.Typically,a trial spacer is used to determine appropriate spacer size to achieve good vertebral body distraction and press-fit placement prior to inserting the interbody device.This makes it less likely that a poor interbody spacer size choice can explain the resulting fractured spacer.A systemspecific insertion tool was used to implant the spacer decreasing the chance of damage occurring during graft insertion.
There are reports of bone allograft fracture in orthopedic surgery,such as after bone tumor resection.Aponte-Tinaoet al[28]reported fractured allografts in 19 out of 135 (14%) patients with segmental intercalary bone allograft reconstruction of the lower extremity.The kidney shaped allograft spacer used in the current report is freeze-dried.It is recommended by the manufacturer to reconstitute the graft in saline prior to use to decrease brittleness.After preparation of the disc space,the allograft spacer is inserted into the space with an implant holder,and then an impactor is used to fully seat the spacer into the intervertebral disc space.Possible causes for graft breakage could be one or a combination of the following:insufficient reconstitution of the graft prior to insertion,the impactor used to seat the graft is smaller than the spacer that may lead to shearing of part of the spacer,or the spacer was microscopically cracked prior to its insertion resulting in the graft weakening and breaking.
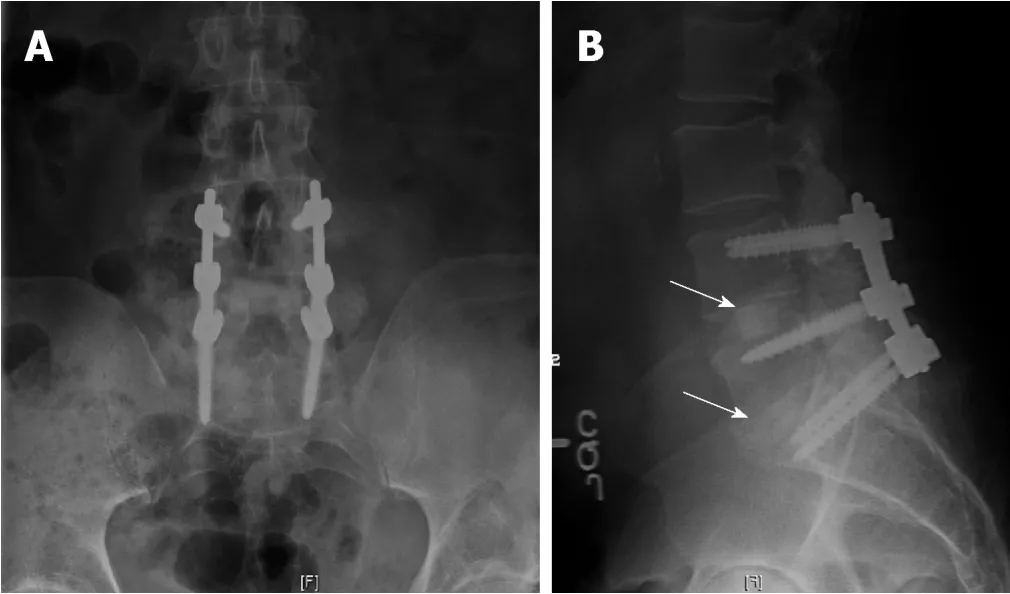
Figure1 Post-operative radiographs showed good spinal alignment with hardware in good position and interbody spacer at each level is under the midsection of the disc space (arrows).
CONCLUSION
Displacement of broken allograft interbody spacer following TLIF procedures can result in neurological sequelae that require revision.Though this complication was found during a TLIF procedure,any lumbar interbody fusion technique is subject to this complication in the event a prosthetic allograft spacer is used.To avoid such an occurrence,the authors recommend allowing sufficient time for the reconstitution of the graft in saline prior to use to decrease brittleness,to use an impactor size that is as close as possible to the spacer size and meticulous inspection of the cortical allograft spacer for any visible imperfection prior to insertion.
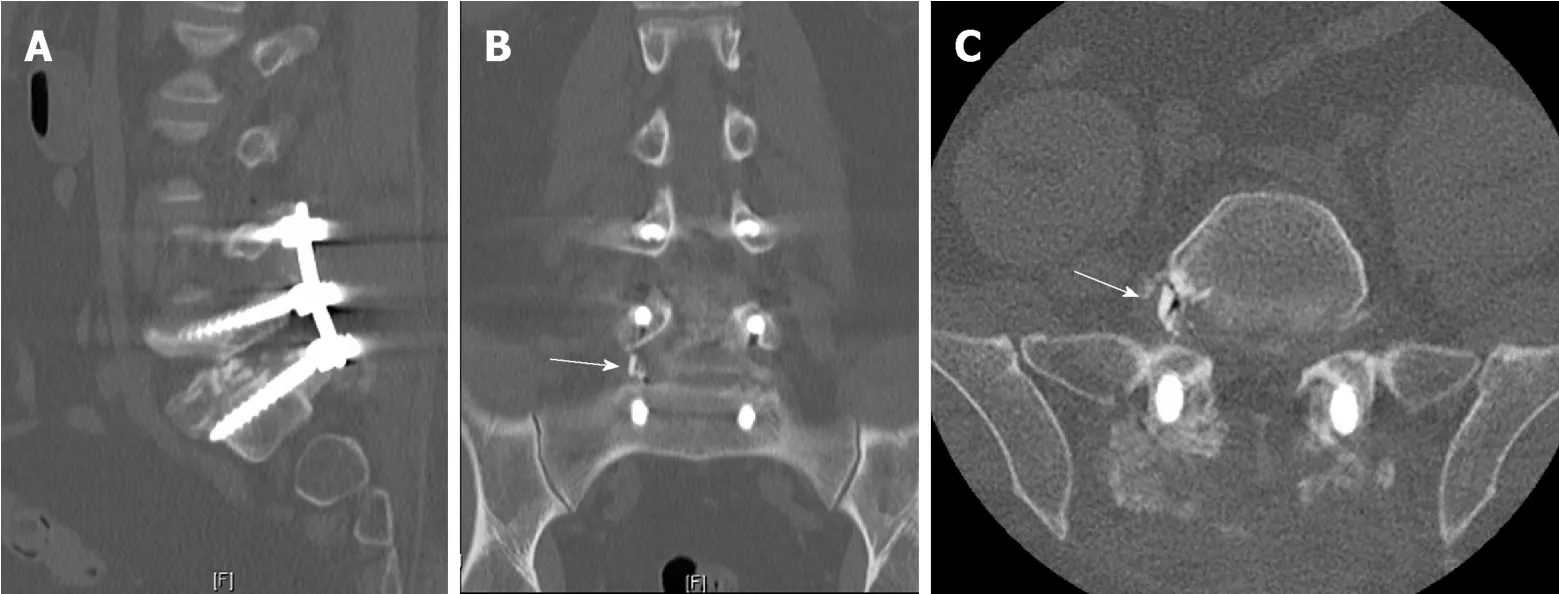
Figure2 Postoperative computed tomography scan.

Figure3 Fragments of prosthetic allograft interbody spacer extracted from right L5 neural foramen.
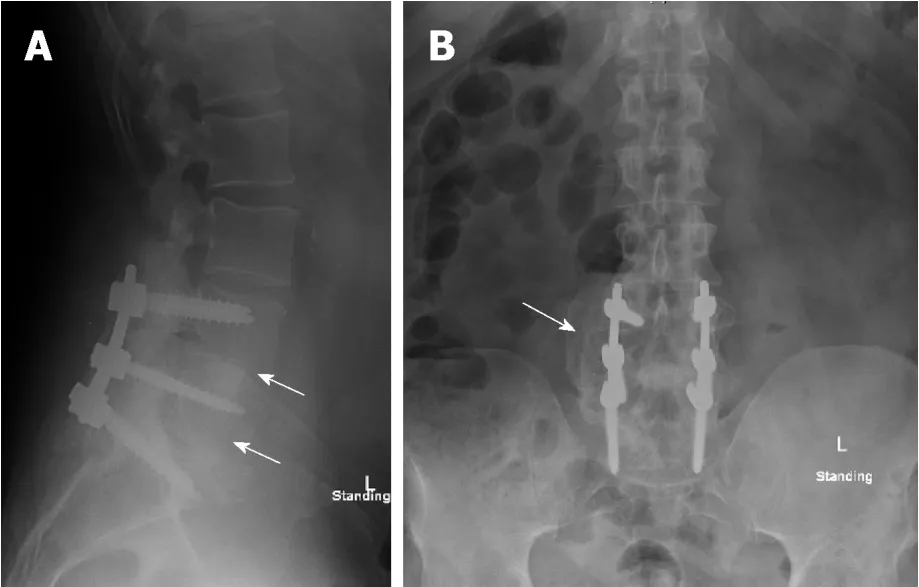
Figure4 One-year post-operative radiographs showed interbody fusion and posterolateral fusion mass (arrows).
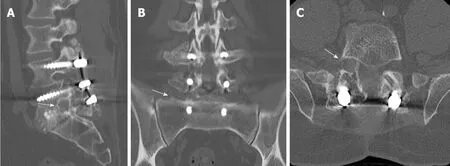
Figure5 One-year post-operative computed tomography-scan.
猜你喜欢
杂志排行

World Journal of Orthopedics的其它文章
- Investigational growth factors utilized in animal models of spinal fusion:Systematic review
- Growing pains:What do we know about etiology? A systematic review
- Recalcitrant distal humeral non-union following previous Leiomyosarcoma excision treated with retainment of a radiated nonangiogenic segment augmented with 20 cm free fibula composite graft:A case report