Super-selective arterial embolization in the control of acute lower gastrointestinal hemorrhage
2019-04-22LiangShanLvJingTaoGu
Liang-Shan Lv, Jing-Tao Gu
Liang-Shan Lv, Department of Gastroenterology and Interventional Radiography, Xi’an Gaoxin Hospital, Xi’an Jiaotong University, Xi’an 710075, Shaanxi Province, China
Jing-Tao Gu, Department of Vascular Surgery, First Affiliated Hospital of Xi’an Jiaotong University, Xi’an 710061, Shaanxi Province, China
Abstract
Key words: Lower gastrointestinal bleeding; Embolization; Infarction; Bowel;Hemorrhage; Selective arterial embolization
INTRODUCTION
Transcatheter embolization has been accepted as an effective and safe method for treating acute upper gastrointestinal (GI) bleeding[1-7].Treatment of acute lower GI bleeding (any site below the ligament of Treitz) using this technique has not reached a consensus, because of the belief that the risk of intestinal infarction in this condition is extremely high[8-12].The purpose of the study is to evaluate the effectiveness and safety of this technique in a retrospective group of patients who underwent embolization for acute lower GI bleeding.
MATERIALS AND METHODS
This study is a retrospective review of patients who underwent super-selective arterial embolization for acute lower GI bleeding from June 2008 to January 2017.The study included 31 patients with 24 men and 7 women whose average age was 66.3(from 36 to 81) years.They suffered from life-threatening acute GI bleeding.Twentyone patients were in frank cardiogenic shock, with systolic blood pressure levels less than 80 mmHg.Packed red blood cell transfusions with the amount ranging between 4 and 11 units were transfused to compensate for massive blood loss.Moreover, 14 patients underwent endoscopic evaluation before radiologic intervention.
Embolization therapy was performed on patients in a specialized angiographic suite with advanced diagnostic and interventional therapeutic capabilities.Standard 4-Fr or 5 Fr catheters for selective diagnostic arteriography were used in each patient.When the site of active bleeding was seen, super-selective catheterization was performed using latest generation of co-axial catheters.The clinicians planned to perform embolization in all 31 patients, and ultimately, it was performed in 26 patients.For the remaining 5 patients, sufficient space for safe embolization could not be achieved.Embolization that involved branches of the superior mesenteric artery was performed in 21 patients, and embolization that involved the inferior mesenteric artery was performed in 5 patients.The catheter tip was positioned just adjacent to the site of active bleeding whenever possible.Only gelfoam fragments of 1 to 2 mm were used as embolic agent in 16 of 26 patients.Microcoils from 2 mm to 4 mm in diameter were used in 10 of 26 patients, and the remaining 6 patients were additionally administered with a few polyvinyl alcohol particles (PVA; Contour emboli 355 μm to 500 μm) to achieve complete hemostasis.Control of hemorrhage, as evidenced by cessation of extravasation and obliteration of pseudoaneurysms, was confirmed by repeat arteriography.
After embolization, they were monitored for postoperative bleeding and signs of intestinal infarction.Several outcomes were analyzed, including rate of initial technical success, rebleeding rate within 7 d after embolization, and complication rate of all patients.
RESULTS
A total of 31 patients were involved in this experiment (24 males and 7 females), and the median age was 66.3 (range:36 to 81 years) years.Transcatheter embolization was used in 26 of 31 patients with acute lower GI bleeding.There were mainly three kinds of embolization utilized to control the hemorrhage (Table 1).Initial technical success was obtained in 26 of 31 patients (83.8%) who were willing to undergo embolization.Sufficiently selective catheterization to permit embolization could not be achieved in 5 patients.
The bleeding was more likely to happen in the proximal colon and the outcome showed that the majority cases of hemorrhage were located in the right colon (Table 2).Embolization therapy resulted in successful hemostasis in all 26 patients (100%) in whom embolization was possible.Rebleeding at less than 7 d after embolization occurred only in 1 patient (3.8%).Rebleeding occurred at 1 d after embolization in this patient who went to the operating room for resection.Furthermore, no complication was recorded during the embolization.During the post-procedure period, no ischemic complication occurred, based on clinical observation of all patients and endoscopy in selected patients.
DISCUSSION
Super-selective arterial embolization has become an effective method to rapidly and safely control upper GI bleeding[1,2,4,6,7,13].In contrast to upper GI bleeding, bleeding originating distally to the ligament of Treitz has always been viewed more conservative due to the bowels, especially the large bowels.Because a relative deficiency of collateral blood supply, transcatheter embolization is a challenging procedure with a significant risk of bowel ischemia[8,10,12,14].Transcatheter arterial embolization for lower GI bleeding was first reported in 1975[15].Consequently,several case reports and small series followed, showing excellent results.Furthermore,in the early 1980s, complications of bowel infarction were recognized.Hanet al[10]reported 23 cases of colonic embolization at five hospitals, with three episodes of bowel necrosis.Then embolization for lower GI bleeding was reserved in patients with highest surgical risk.With improvements in coaxial catheters and embolic agents(microcoils, gelfoam, and PVA particles), there was renewed interest in embolization in the treatment of lower GI bleeding.Okazakiet al[16]published a series involving 10 consecutive embolizations in 9 patients for lower GI bleeding.They used microcatheters and PVA particles to achieve hemostasis in all cases in which no case of bowel infarction and only 2 cases of asymptomatic mucosal ischemia were noted by endoscopy.
In this present study, we approached 21 patients with lower GI bleeding who were willing to undergo embolization.Embolization was technically possible in 16 patients,and hemostasis was achieved in all of them.One patient (6%) experienced rebleeding and required bowel resection.Five patients could not achieve embolization because the catheter tip could not be positioned adjacent to the site of active bleeding.It must be emphasized that safe and effective embolization requires super-selective catheterization.Distal catheter may be desirable in some cases, for which a co-axial system is often required.We perform embolization as distally as possible.If the catheter tip was not in a sufficiently peripheral position, embolization was not implemented.
Reported rate of bowel ischemia after embolization ranged from 0% to 22% in the literature[8,12,17].In this study, no patient developed bowel infarction.To avoid bowel infarction after embolization, careful technique and preparation for turning down the embolization are pivotal, particularly when a suitable catheter position cannot be achieved[14,18,19].Nevertheless, it is also important to choose a suitable embolic agent.Various options are available for embolic agent, which include microcoils, gelfoam,and PVA, and the outcome also varies according to which material is chosen and how it is utilized.Gelfoam is used as a temporary embolic agent and is relatively safe, but it is not conductive to complete embolization and the rate of recurrent bleedings is higher than other embolic agents.PVA particles achieve rapid and complete embolization of target artery, regardless of the artery type and diameter.However,the complication rate is higher than other agents owing to the high risk of non-targetembolization.Microcoils are the embolic agents used in 10 of 26 patients.They can be clearly seen on the lateral fluoroscopic image and are easily and accurately positioned.Although we used gelfoam fragments and PVA particle safely and successfully, there are also some disadvantages of these agents.For example, they are not so radiopaque that the final resting position cannot be easily controlled, which increases the difficulty to manipulate the quantity of the agents.We performed embolization with gelfoam fragments and PVA particles, which is a less tightly controlled procedure than embolization with microcoils and is more likely to trigger bowel infarction.
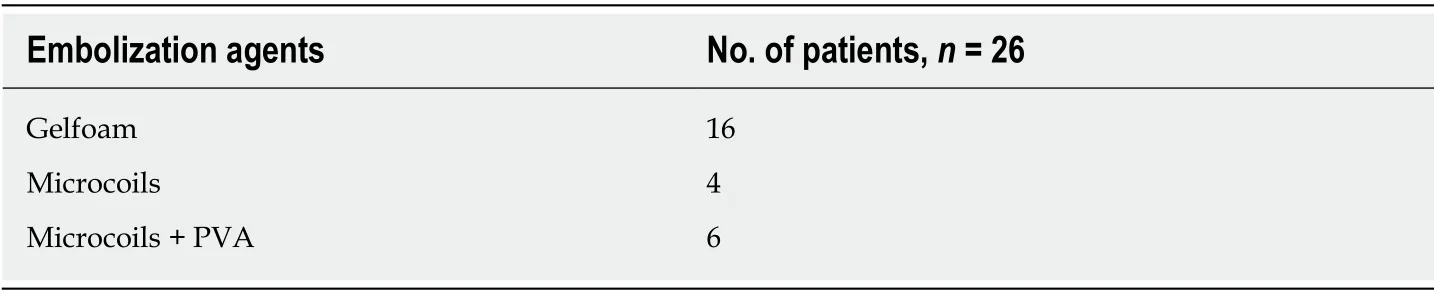
Table 1 Embolization agents
In summary, our results suggest that super-selective arterial embolization for acute lower GI hemorrhage is effective and safe.This procedure should be the initial treatment in patients who suffer severe bleeding that requires angiography and have indication for super-selective catheterization.With super-selective embolization, the risk of symptomatic bowel ischemia can be minimalized.
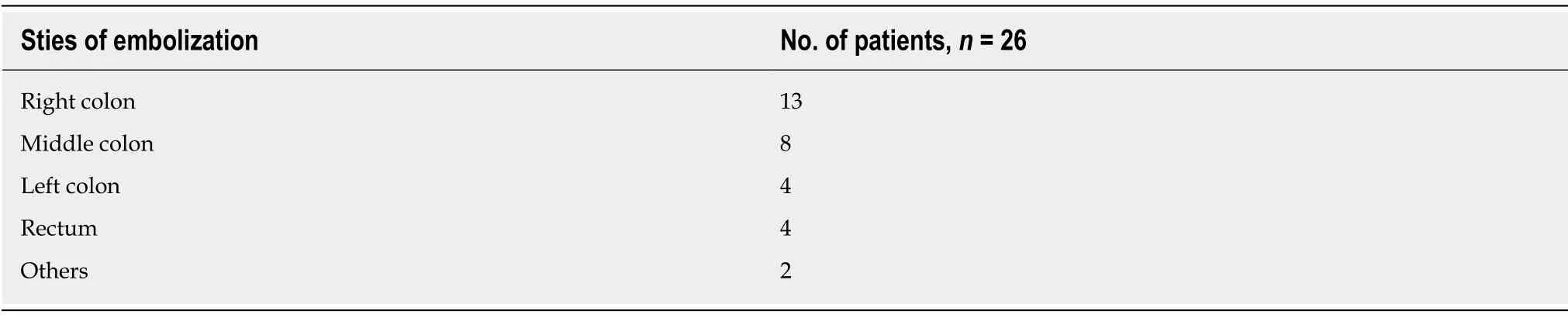
Table 2 Sties of embolization
ARTICLE HIGHLIGHTS
Research background
Acute gastrointestinal (GI) bleeding is an emergency condition that can lead to significant morbidity and mortality.Embolization is considered the preferred therapy in the treatment of lower GI bleeding when it is unrealistic to perform the surgery or vasopressin infusion in this population.Treatment of acute lower GI bleeding (any site below the ligament of Treitz) using this technique has not reached a consensus because of the belief that the risk of intestinal infarction in this condition is extremely high.The purpose of the study is to evaluate the effectiveness and safety of this technique in a retrospective group of patients who underwent embolization for acute lower GI bleeding.
Research motivation
Because of a relative deficiency of collateral blood supply, transcatheter embolization is a challenging procedure with a significant risk of bowel ischemia.
Research objectives
To evaluate the efficacy and safety of super-selective arterial embolization in the management of acute lower GI bleeding.
Research methods
This study is a retrospective review of patients who underwent super-selective arterial embolization for acute lower GI bleeding.After embolization, they were monitored for postoperative bleeding and signs of intestinal infarction.Several outcomes were analyzed,including rate of initial technical success, rebleeding rate within 7 d after embolization, and complication rate.
Research results
The bleeding was more likely to happen in the proximal colon, and the outcome showed that the majority cases of hemorrhage were located in the right colon.Embolization therapy resulted in successful hemostasis in all 26 patients (100%) in whom embolization was possible.Rebleeding at less than 7 d after embolization occurred only in 1 patient (3.8%).Rebleeding occurred at 1 d after embolization in this patient who went to the operating room for resection.No complication was recorded during the embolization and during the post-procedure period, and no ischemic complication occurred.
Research conclusions
Super-selective arterial embolization for acute lower GI hemorrhage is effective and safe.This procedure should be the initial treatment in patients who suffer severe bleeding that requires angiography and have indication for super-selective catheterization.With super-selective embolization, the risk of symptomatic bowel ischemia can be minimalized.
Research perspectives
To avoid bowel infarction after embolization, careful technique and preparation for turning down the embolization are pivotal, particularly when a suitable catheter position cannot be achieved.In addition, it is also important to choose a suitable embolic agent.
杂志排行

World Journal of Clinical Cases的其它文章
- Colorectal cancer:The epigenetic role of microbiome
- Human podocyte injury in the early course of hypertensive renal injury
- Relationship between acute hypercarbia and hyperkalaemia during surgery
- Surgical treatment ofpatients with severe non-flail chest rib fractures
- End-stage liver disease score and future liver remnant volume predict post-hepatectomy liver failure in hepatocellular carcinoma
- Treatment of hemorrhoids:A survey of surgical practice in Australia and New Zealand