Persistent risk for new, subsequent new and recurrent hepatocellular carcinoma despite successful anti-hepatitis B virus therapy and tumor ablation: The need for hepatitis B virus cure
2019-02-21BriannaShinnAaronMartinRobertCobenMitchellConnJorgePrietoHowardKroopAnthonyDiMarinoHieWonHann
Brianna J Shinn, Aaron Martin, Robert M Coben, Mitchell I Conn, Jorge Prieto, Howard Kroop,Anthony J DiMarino, Hie-Won Hann
Abstract Hepatitis B virus (HBV) is one of the most significant hepatocarcinogens. The ultimate goal of anti-HBV treatment is to prevent the development of hepatocellular carcinoma (HCC). During the last two decades, with the use of currently available anti-HBV therapies (lamivudine, entecavir and tenofovir disoproxil fumatate), there has been a decrease in the incidence of HBV-associated HCC (HBV-HCC). Furthermore, several studies have demonstrated a reduction in recurrent or new HCC development after initial HCC tumor ablation. However, during an observation period spanning 10 to 20 years, several case reports have demonstrated the development of new, subsequent new and recurrent HCC even in patients with undetectable serum HBV DNA. The persistent risk for HCC is attributed to the presence of covalently closed circular DNA (cccDNA) in the hepatocyte nucleus which continues to work as a template for HBV replication. While a functional cure (loss of hepatitis B surface antigen and undetectable viral DNA) can be attained with nucleos(t)ide analogues, these therapies do not eliminate cccDNA. Of utmost importance is successful eradication of the transcriptionally active HBV cccDNA from hepatocyte nuclei which would be considered a complete cure. The unpredictable nature of HCC development in patients with chronic HBV infection shows the need for a complete cure. Continued support and encouragement for research efforts aimed at developing curative therapies is imperative. The aims of this minireview are to highlight these observations and emphasize the need for a cure for HBV.
Key words: Hepatitis B; Hepatocellular carcinoma; Antiviral therapy; Persistent Risk for hepatocellular carcinoma; Tumor ablation
INTRODUCTION
Since the discovery of hepatitis B virus (HBV) by Blumberg et al[1]in 1965 and the development of the first HBV vaccine in 1983, much knowledge has been obtained regarding the pathogenesis, hepatocarcinogenesis, epidemiology and molecular biology of HBV as well as the antiviral treatment.
With vaccination, there has been a decrease in the number of infected people globally especially in the younger generations. There has also been a significant increase in survival of HBV infected individuals due to antiviral treatment and earlier detection of hepatocellular carcinoma (HCC) with simultaneous antiviral treatment.
However HBV is still responsible for 786000 deaths in 2010 with 341000 from HCC and 312000 attributed to cirrhosis[2].
HBV is a major public health issue with more than 257 million carriers living today,and up to one million who die annually from HBV-related liver disease including HCC[3,4]. HCC is the sixth most common cancer and the third leading cause of cancer deaths worldwide. Chronic infection with HBV is responsible for 50% of HCC cases worldwide[5,6]. Current therapies available to treat chronic hepatitis B (CHB) include interferon and the nucleos(t)ide analogues (NAs): Lamivudine, adefovir, entecavir,telbivudine, tenofovir disoproxil fumarate and the recently FDA-approved tenofovir alafenamide. Several studies have been conducted in the past to assess the impact of antiviral therapies, specifically lamivudine, entecavir and tenofovir, on disease progression and HCC development[7-10]. Multiple studies have demonstrated that for patients diagnosed with HBV-related HCC, improved survival can be attained with adjuvant antiviral therapy following curative liver resection and/or local tumor ablation[11,12].
Current antiviral therapies used to treat CHB control viral replication through inhibition of reverse transcriptase and subsequent interruption of HBV DNA formation. While treatment can slow and/or prevent the progression of liver disease,it does not eliminate the covalently closed circular DNA (cccDNA) from infected hepatocytes and is therefore unable to cure the infection. As a result, patients usually require lifelong therapy to control viral replication and help prevent hepatocarcinogenesis.
However, it has been reported that despite several years of antiviral therapy, a persistent risk for carcinogenesis still exists[13-15]. Studies have also demonstrated that even after more than a decade of successful HBV suppression, the risk for HBV-related HCC remains[16-18]. The aims of this minireview are to bring light to these observations and emphasize the need for a cure for HBV[19-21].
HBC REPLICATION CYCLE AND HEPATOCARCINOGENESIS
HBV related hepatocarcinogenesis has been extensively described in the past[22-27].HBV is an enveloped partially double-stranded relaxed circular DNA virus of the Hepadnaviridae family. The viral replication cycle begins when HBV recognizes highlysulfated heparin sulfate proteoglycans on the hepatocyte surface and gains entry by binding the liver-specific receptor, sodium taurocholate co-transporting polypeptide(NTCP or SLC10A1)[28,29]. Once in the cell, the virus enters the hepatocyte nucleus where the relaxed circular DNA is converted to cccDNA. While little is known about the formation and regulation of cccDNA, it is thought that most of the steps needed for this conversion are provided by the host cell[19-21,30]. Viral cccDNA remains in the nucleus of the infected host cell and is used as the template for transcription of four viral mRNA intermediates. These mRNA intermediates eventually undergo translation to produce seven viral proteins including DNA polymerase and the core protein. One of these mRNA intermediates, called pregenomic RNA, is critical for the viral replication. It undergoes reverse transcription and serves as the template for new viral DNA. The newly formed viral DNA and viral proteins form viral nucleocapsids that obtain HBV envelope proteins prior to being released from the hepatocyte as mature enveloped virions[19-21,30]. These virions then go on to infect other hepatocytes.
As to HBV associated hepatocarcinogenesis, inside the hepatocyte nucleus, HBV DNA integration with the host genome takes place during the acute phase of infection[31,32]. This integration is thought to be one of several mechanisms that leads to carcinogenesis and HCC. Activation of cellular oncogenes, inactivation of tumor suppressor genes, chronic liver injury, inflammation and regeneration, activation of cellular proto-oncogenes, suppression of growth regulating genes and increased HBx protein have all been implicated in the development of HCC[33](Figure 1).
CURRENT ANTIVIRAL THERAPIES FOR CHRONIC HBV AND THE IMPACT ON HCC INCIDENCE
Current therapies available to treat CHB include interferon and NAs: lamivudine,adefovir, entecavir, telbivudine, tenofovir disoproxil fumarate and the recently FDA-approved tenofovir alafenamide. While interferon works through immune modulation and has a weak antiviral effect, the NAs inhibit viral replication through direct inhibition of viral reverse transcriptase. The goal of these antiviral medications is to improve quality of life and survival by preventing the progression of CHB and development of cirrhosis and HCC. Currently the treatment objectives are categorized as shown in Table 1. While a “functional cure” is defined as the loss of hepatitis B surface antigen (HbsAg) and/or seroconversion to antibody to hepatitis B surface antigen with undetectable serum HBV DNA, it is important to remember that this is not a complete cure[19]. This complete cure is what is desperately needed to end the persistent risk for HCC.
Decreased incidence of HCC with antiviral therapy
While a complete cure is not yet available, several studies have assessed the impact of NAs on disease progression and HCC development. A randomized controlled trial by Liaw et al[7]randomized patients with advanced fibrosis or cirrhosis secondary to CHB to receive daily Lamivudine or placebo for up to 5 years. HCC occurred in 17/436(3.9%) of patients treated with Lamivudine and 16/215 (7.4%) of patients who received placebo (P = 0.047). After a median treatment duration of 32.4 mo, the incidence of HCC was significantly reduced in the Lamivudine group and the study was stopped[7].
A retrospective study by Eun et al[8]conducted from March 1997 to February 2005 also showed a decreased incidence of HCC with use of lamivudine in patients with chronic HBV and compensated cirrhosis. HCC occurred in 4.9% of patients in the group treated with Lamivudine with sustained viral suppression compared to 25% of patients in the untreated group.
Similar results have also been shown with newer antivirals such as entecavir and tenofovir. Hosaka et al[9]assessed the risk of HCC in patients with CHB treated with entecavir compared to a control group of treatment-naïve patients. After 5 years of treatment, patients treated with entecavir had a cumulative HCC incidence of 3.7%compared to 13.7% in the treatment-naïve group (P < 0.001). Similarly, Kim et al[10]examined the incidence of HCC in patients treated with tenofovir disoproxil fumerate(TDF). Patients with CHB, including those with cirrhosis, were treated with TDF and assessed for incidence of HCC. The investigators found that there was a decreased incidence of HCC noted by the third year of treatment with TDF compared to the predicted incidence.
Improved survival with antiviral therapy after the development of HCC
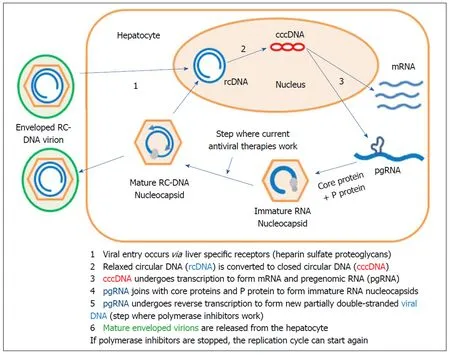
Figure 1 Hepatitis B replication life cycle.
Since the first antiviral drug for HBV became available, antiviral therapy has been used in patients following surgical resection or local ablative therapy for HBV-associated HCC. Longer survival with concomitant antiviral therapy following tumor ablation has been observed in a number of studies conducted in Japan, Hong Kong,Taiwan and China since 2007. Similar observations of improved survival were first reported in the United States in 2011[34]. A meta-analysis conducted by Yuan et al[11]reviewed sixteen of these studies in an effort to investigate the effect of antiviral therapy after curative therapy in patients with HBV-associated HCC. The papers in the analysis included four studies from China, three from Hong Kong, one from Taiwan, six from Japan and one from the United States. The meta-analysis looked at the impact of NAs on the one and three year recurrence rates, as well as one, three and five year overall survival and disease-free survival rates. The results revealed that NAs significantly reduced the recurrence of HBV-related HCC after curative therapy and improved both overall survival and disease-free survival[11].
Liu et al[12]also conducted a meta-analysis to assess the effect of adjuvant antiviral therapy following hepatectomy and/or percutaneous ablation for HBV-related HCC.They looked at twenty-one studies that compared antiviral therapy with placebo or no treatment. The primary end-points assessed were recurrence-free survival and overall survival. While this meta-analysis did have some limitations including significant between-study heterogeneity and most of the studies being observational in nature,NAs did show a significant improvement in prognosis after curative treatment in patients with HBV-associated HCC[12].
Development of new HCC while on successful antiviral therapy
While overall incidence of HCC has reduced with antiviral therapy, HCC can still develop despite successful viral suppression, most commonly in patients with cirrhosis. The most commonly reported cases of HBV-associated HCC developed within five to ten years despite antiviral therapy[13-15]. However, recent observations at the Liver Disease Prevention Center, Division of Gastroenterology and Hepatology of Thomas Jefferson University Hospital have demonstrated development of HBV-associated HCC even after a decade of successful viral suppression[16,17]. Patients from these observations were maintained on antiviral treatment anywhere from 5.2-18.4 years with undetectable serum HBV DNA for up to 12.4 years before HCCdevelopment. Due to close monitoring and follow up, most of the tumors were discovered early and were ablated successfully (Table 2)[17].

Table 1 Definition of hepatitis B virus cure[19]
Development of the subsequent new and recurrent HCC
After resection or ablation of the initial HCC, the patients were continued on antiviral therapy and maintained successful viral suppression. However, the persistent risk for subsequent new and recurrent HCC in this patient population has been observed. We recently described three cases of subsequent new and recurrent HCC in patients who underwent successful initial tumor ablation and had suppression of serum HBV DNA for years. Figure 2 depicts these three patients and shows the time from their HBV diagnosis to the initial HCC and eventual development of subsequent new and recurrent HCC. One of these patients described in Figure 3 was diagnosed as HbsAg(+) in 1987. She did not receive antiviral therapy as it was not available until after 1998. In 2000, thirteen years later, she was diagnosed with HCC. Following successful transarterial chemoembolization (TACE) and radiofrequency ablation she was maintained on antiviral therapy for five years at which point she was found to have a 1.1 cm × 0.8 cm arterially enhancing lesion with washout appearance near the previously treatment site on abdominal magnetic resonance imaging consistent with recurrent HCC. She underwent TACE and was maintained on antiviral therapy for another ten years at which point she developed another 0.8 cm recurrent HCC despite an undetectable serum HBV DNA[18].
Need for HBV Cure
Without eradication of cccDNA from infected hepatocytes, HBV continues to carry the risk of development of HCC despite functional cure being achieved as described above. As we become more aware of the persistent risk for new, subsequent new and recurrent HCC, we become more aware of our need for a cure for HBV infection.Antiviral therapy is able to control viral replication and slow the progression of liver disease in the majority of treated patients, but the persistence of cccDNA and continual suppression of the innate and adaptive host immune response causes a persistent risk of hepatocarcinogenesis. Several steps in the HBV replication cycle have been identified as potential targets for future therapies. These therapies can be separated into four categories based on their target of action: (1) complete inhibition of HBV replication; (2) restoration of host innate immunity and adaptive anti-HBV T and B cell responses; (3) selective sensitization of HBV infected hepatocytes to immune elimination; and (4) direct targeting of cccDNA[21].
Complete inhibition of HBV replication: The first category, complete inhibition of HBV replication, should have in theory already been achieved with existing NAs.However, complete inhibition of HBV replication is not achieved with NAs alone since inhibition of DNA polymerase is only one step of the entire HBV replication cycle. If this had been achieved, we would see elimination of HBV DNA and even cccDNA as infected hepatocytes are replaced. In addition to direct inhibition of HBV DNA polymerase, other steps in the replication cycle are being targeted. Entry inhibitors are being investigated and work through targeting the NTCP receptor preventing de novo infection of hepatocytes as well as the spread of the virus from infected hepatocytes to non-infected hepatocytes. Capsid inhibitors are also being investigated and have the potential to work at several different steps in the HBV replication cycle where the capsid is essential including genome packaging, reverse transcription, intracellular trafficking and re-importation into the nucleus. These therapies have the potential to augment the action of NAs and lead to complete inhibition of HBV DNA[19].
Restoration of host innate and adaptive immunity: In regards to restoration of host innate and adaptive immune responses, several targets have been identified.However, the challenge of stimulating an antiviral immune-mediated response without triggering detrimental anti-HBV flares is difficult. Inhibiting HBV geneexpression has been investigated with RNA interference and nucleic acid polymers.Checkpoint inhibitors such as anti-PD-1 monoclonal antibodies currently used in oncology are also being investigated. In HBV, the HBV-specific CD8+ T cells express high levels of inhibitory molecules so inhibition of these checkpoint molecules can rescue HBV-specific CD8+ T cells. Engineering HBV-specific T cells through transfer of HBV-specific T cell receptors and therapeutic vaccines aimed at stimulating HBV-specific T cell immunity in patients chronically infected with HBV are also under investigation. Finally, toll-like receptor agonists are being developed to help recognize the virus and subsequently stimulate production of interferon-alpha and other cytokines in an effort to activate natural killer cells and other lymphocytes[21].

Table 2 Development of hepatocellular carcinoma in patients with cirrhosis on long-term antiviral therapy[17]
Immune elimination of HBV infected hepatocytes: The third category of therapies under investigation includes medications that target cellular inhibitor of apoptosis proteins (cIAPs). These proteins have been found to attenuate TNF signaling during HBV infection which leads to restricted death of infected hepatocytes. This lack of infected hepatocyte death leads to viral persistence. Birinapant, a specific therapy currently being investigated in preclinical models, antagonizes cIAP and has shown anti-HBV activity[21].
Direct Targeting of cccDNA: The final category of potentially curative HBV therapies under investigation involves direct targeting of cccDNA. There are several strategies to target cccDNA which include inhibition of cccDNA formation, destruction of cccDNA and functional silencing of cccDNA through targeting proteins involved in cccDNA transcription and/or stability. Given the knowledge we have regarding persistent cccDNA and impaired immune responses in patients with CHB, it is likely that a combination of these newly investigated therapies will need to be used in order to achieve complete cure[21].
CONCLUSION
The ultimate goal of HBV treatment is to prevent the development of HCC and death from the virus. Of utmost importance is successful eradication of the transcriptionally active HBV cccDNA from hepatocyte nuclei. While we currently aim for a functional cure with loss of HBsAg and undetectable viral DNA, a complete cure can only be attained with eradication of cccDNA. The several concerns regarding the unpredictable nature of HCC development in patients with CHB shows the need for a cure and we should continue to support and encourage research efforts aimed at developing curative therapies.
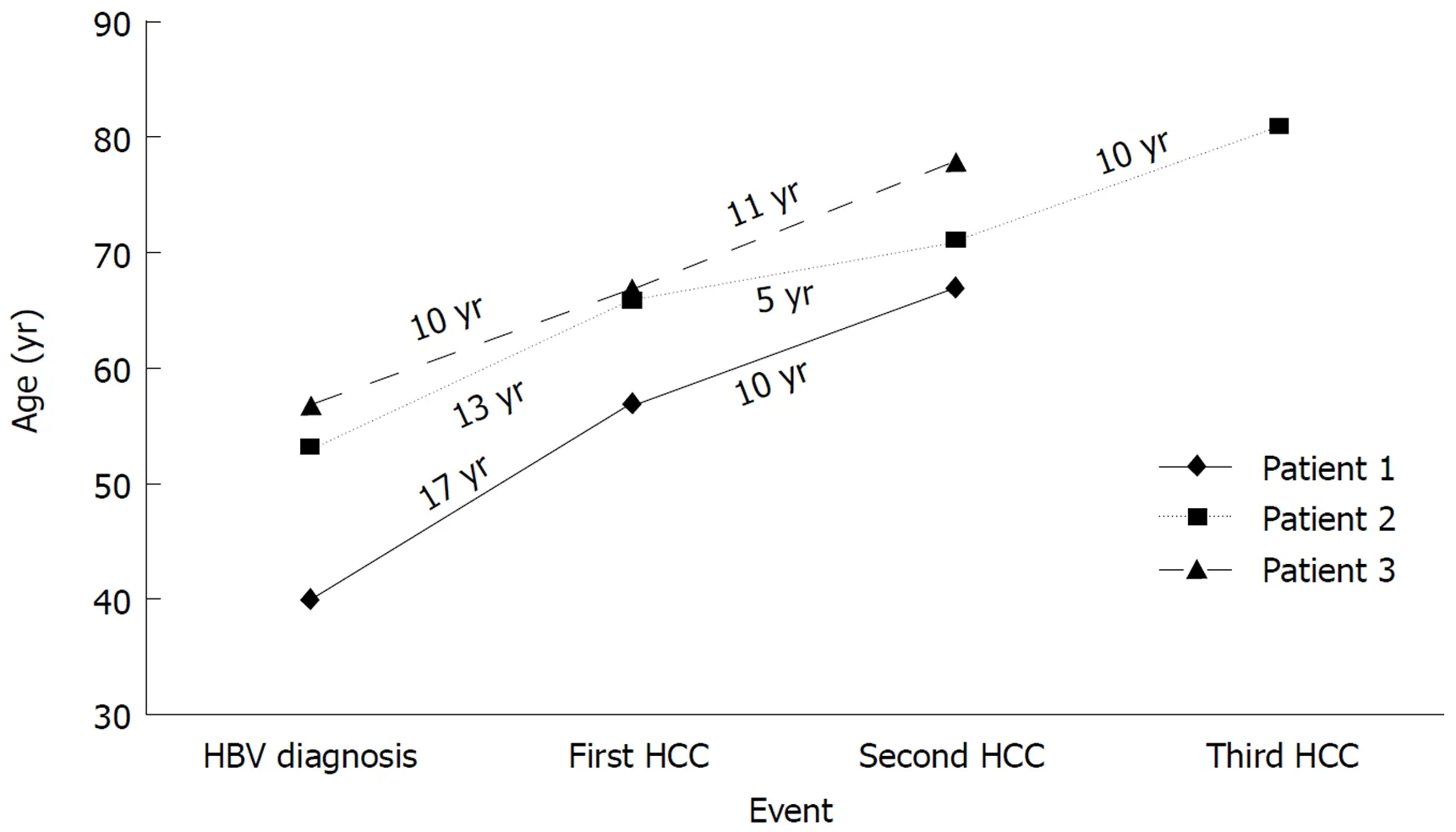
Figure 2 Hepatocellular carcinoma in three patients with chronic hepatitis B[18]. HCC: Hepatocellular carcinoma; HBV: Hepatitis B virus.
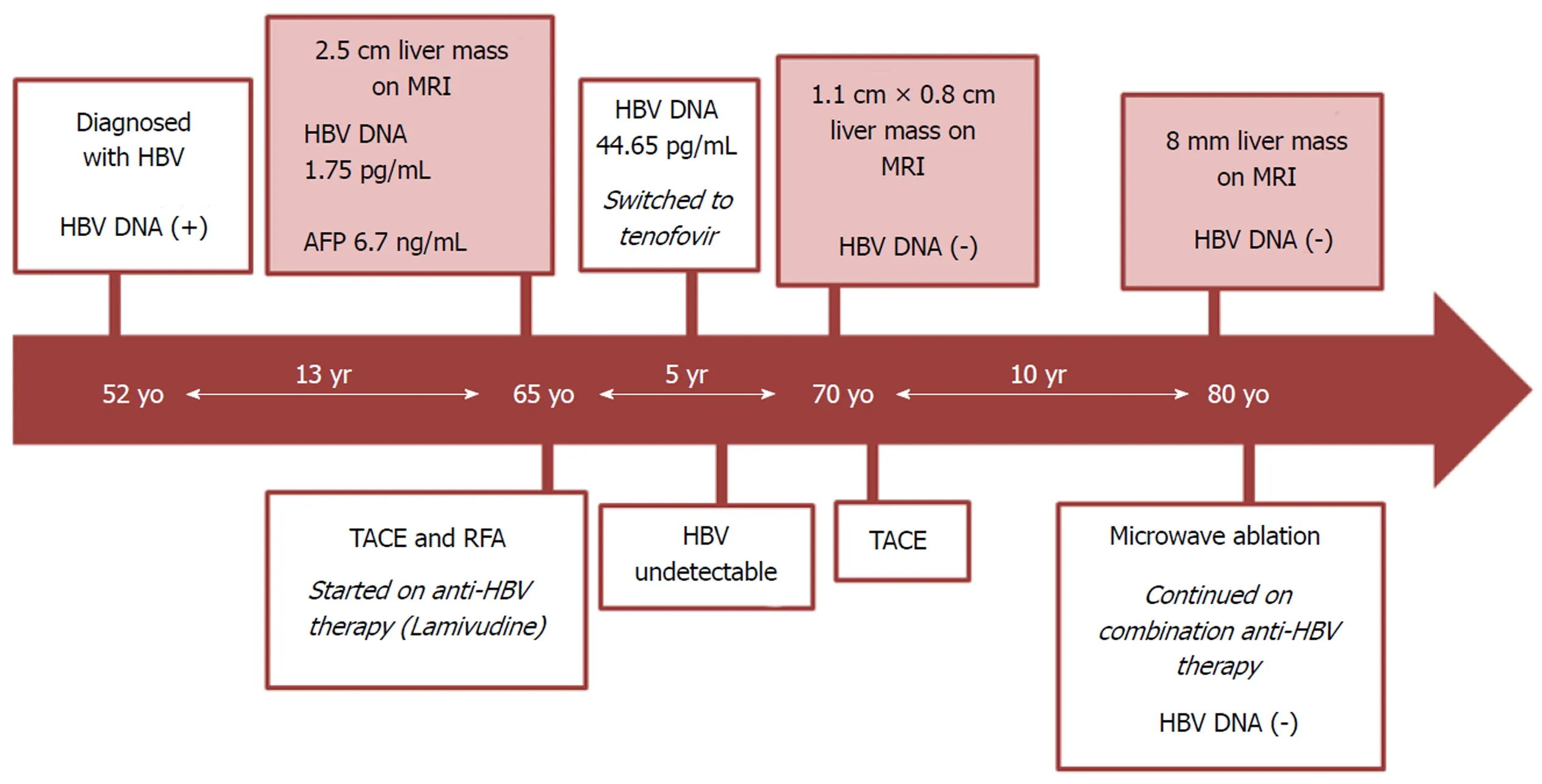
Figure 3 Persistent risk for recurrent hepatocellular carcinoma in a patient with chronic hepatitis B[18]. HCC: Hepatocellular carcinoma; HBV: Hepatitis B virus;MRI: Magnetic resonance imaging; TACE: Transarterial chemoembolization; RFA: Radiofrequency ablation.
杂志排行

World Journal of Hepatology的其它文章
- Hepatocellular carcinoma in non-cirrhotic liver: A comprehensive review
- Treatment of primary sclerosing cholangitis in children
- Hepatitis in slaughterhouse workers
- Serum biomarkers and risk of hepatocellular carcinoma recurrence after liver transplantation
- Temporal trends of cirrhosis associated conditions
- Clinical factors associated with hepatitis B screening and vaccination in high-risk adults