Diabetes in the Kokan region of India
2019-02-20PatilSuvarnaKadamShrutiDesaiMarutiJoglekarCharudatta
Patil Suvarna, Kadam Shruti, Desai Maruti, Joglekar Charudatta
Abstract BACKGROUND BKL Walawalkar Hospital is situated near the village of Dervan in the Kokan region of the state of Maharashtra in India. A survey of 2200 surrounding villages showed 51.8% adults had body mass index (BMI) below <18.5 kg/m2 and only 4.5% were overweight. A survey of 11521 adolescent girls from rural schools showed 64% prevalence of thinness. In the same region, government survey reported the prevalence of diabetes around 7%, and 70% prevalence of leanness.This reinforced the fact that the overall population of Kokan is lean. Hence, we decided to investigate body composition of diabetic people from our hospital clinic by carrying out a clinic-based case control study.AIM To study body composition of diabetics in a rural clinic of Kokan.METHODS In a case-control study, 168 type 2 diabetic patients (102 men) attending the outpatient department at a rural hospital and 144 non-diabetic controls (68 men)in the Chiplun area of the Kokan region were recruited. History of diabetes (age of onset, duration), anthropometric measurements (height, weight, waist and hip circumference) were recorded. Body composition was measured by bioimpedance using the TANITA analyzer.RESULTS More than 45% of diabetic subjects had a 1st degree family history of diabetes, and more than 50% had macrovascular complications. The average BMI in diabetic subjects was 24.3 kg/m2. According to World Health Organization standards,prevalence of underweight was 8% and that of normal BMI was around 50%.Underweight and normal diabetic subjects (men as well as women) had significantly lower body fat percentage, higher muscle mass percentage, lower visceral fat and lower basal metabolic rate when compared to their overweight counterparts.CONCLUSION The diabetic population in Kokan has near normal body composition, and BMI has considerable limitations in assessing body composition and it also lacks sensitivity for assessing risk for diabetes in this population. High prevalence of family history of diabetes may point towards genetic predisposition. Leanness is an inherent characteristic of this population and its metabolic significance needs further investigations with a larger sample size.
Key words: Body composition; Diabetes; Metabolism; Malnutrition; Kokan
INTRODUCTION
Recent years have seen a considerable increase in the burden of chronic noncommunicable diseases (diabetes, hypertension and coronary heart disease) in clinical practice in urban India. Recent studies in urban populations have shown an unexpectedly high prevalence of diabetes, and the prevalence is rising rapidly[1]. Type 2 diabetes mellitus (T2DM), previously called non-insulin dependent diabetes mellitus (or NIDDM) is a familial disease, on the verge of becoming a pandemic in developing countries like India[2].T2DM is the most prevalent form of diabetes seen in India and constitutes more than 95% of the diabetic population[3]. Migrant Indians in Canada, Britain, the Netherlands, United States and Singapore also have a higher prevalence of diabetes compared to the native populations[4-8].
In contrast, the prevalence of diabetes and coronary heart disease in rural India has been shown to be low. However, there are very few prevalence studies in rural India[9-11]due to remoteness of the villages and lack of health infrastructure for epidemiological studies. Rapid socio-economic developments over the last 2 decades have made the rural population particularly vulnerable to non-communicable diseases. Therefore, there is a need to obtain reliable data on non-communicable diseases in rural India, study the risk factors, and plan effective preventive measures.
In Europe and America, the majority of patients with T2DM are obese. In 1965,Tripathyand Kar[12]highlighted leanness among elderly diabetics in India. Other studies in India have reported a prevalence of low body weight/lean T2DM ranging from 1.6% to 26%[13,14]. A review by Dulloo et al[15]highlighted limitations of body mass index (BMI) in assessment of body composition and lack of sensitivity for assessing disease risk, particularly in those who have normal or slightly elevated body weight.
BKL Walawalkar Hospital, situated near the village of Dervan in Ratnagiri district of the state of Maharashtra, has actively promoted rural health care through a variety of education and holistic outreach programs for more than 22 years. The hospital serves the poor socio-economic class populations of the adjoining villages. In 2003-2010 our hospital carried out house-to-house surveys of 2200 villages in the area. In this survey, 51.8% of the subject had BMI < 18.5 kg/m2and only 4.5% were overweight, with BMI > 25 kg/m2. A survey of 11521 adolescent girls from rural schools conducted between 2011 and 2017 showed that 64% of the girls were in grade 1 to 3 of thinness, based upon International Obesity Task Force standards. Stunting was seen in 22% to 28% of the girls. Thus, the overall population of Kokan is lean in their body stature.
The National Family Health Survey[9]conducted by the government of India reported on the prevalence of diabetes in the same region based on random blood sugar as 9% among men and 5.8% among women. The same survey also reported more than 70% prevalence of leanness based on BMI among men as well as women.This again reinforced the leanness of the population of Kokan. Hence, we decided to investigate more about body composition of diabetic people from our hospital clinic by carrying out a clinic-based case control study. The health infrastructure in our hospital provided us the opportunity to study the profile of diabetic as well as nondiabetic subjects.
MATERIALS AND METHODS
This study was carried out in the outpatient department of BKL Walawalkar Hospital and Rural Medical College in the Ratnagiri district.
Diabetic patients from the outpatient department were enrolled in the study. Nondiabetic control subjects were mostly spouses of the patients in the hospital or were from the hospital staff.
The following data was recorded from the clinical history for diabetic subjects: age at diagnosis of diabetes; family history of diabetes; and history of macrovascular complications (hypertension, ischemic heart disease, cardiovascular disease and cerebral vascular disease) and microvascular complications (nephropathy,neuropathy and retinopathy).
The following anthropometric parameters were measured on diabetic as well as non-diabetic subjects: height; weight; waist and hip circumferences. BMI and waist-tohip ratio (commonly known as WHR) were calculated. Subjects were classified as underweight, normal and overweight using World Health Organization standards for BMI[16]. Those with BMI < 25 kg/m2, that is those who were underweight or normal,were classified as lean. We used International Diabetes Federation criteria[17]for the waist circumference to classify the subjects as centrally obese.
Body composition was assessed on all the subjects using the Tanita BC 420-MA analyzer (Tanita Corporation, Tokyo, Japan). It measured bioelectrical impedance by passing alternating current through the subject to measure the water content. Body composition measurements (fat mass, lean mass, total body water) were obtained as mass as well as percentage. In addition, we also obtained visceral fat, fat free mass,total body water (TBW) as mass as well as percentage, and basal metabolic rate(BMR).
In total, 201 diabetic subjects reported to the outpatient department of medicine.Those with diabetes with pregnancy, severe chronic illness, pancreatic disease and type-1 diabetes were excluded. After these, 168 diabetic subjects (102 men) were left to form the sample of diabetic subjects. We recruited 144 non-diabetic control subjects(68 men).
Statistical methods
Data is presented as mean ± SD for continuous and as percent for categorical variables. Analysis of variance and χ2test was used to compare continuous and categorical variables for differences in groups. Comparison of anthropometric parameters between diabetic and non-diabetic subjects was adjusted for current age.All analyses were performed using SPSS 16.0 (SPSS Inc., Chicago, IL, United States).
Ethics
Informed and written consent was obtained from all the subjects for use of their data.Ethical approval from the institute's ethics committee was also obtained for the data analysis.
Our institute's ethics committee is registered with the government of India. Earlier,its registration number was EC/755/INST/MH/2015. The registration expired in August 2018 and was subsequently renewed, with the new registration number as EC/755/INST/MH/2015/RR-18.
The study was conducted from January 2018 to June 2018.
RESULTS
Subject characteristics
Table 1 shows clinical characteristics (age, anthropometry and body composition measurements) of subjects. Non-diabetic subjects (men as well as women) were significantly younger (P < 0.001). In diabetic subjects the mean age of diagnosis of diabetes was similar for men and women. Height was similar in both sexes, when comparing diabetic and non-diabetic. Diabetic women were heavier and had higher BMI. Diabetic women also had higher hip circumference. Both diabetic men and women had significantly higher WHR. Body fat percentage as well as mass was similar in diabetic and non-diabetic men but it was significantly higher in diabetic women. In both sexes the muscle mass percentage was similar between diabetics and non-diabetics but diabetic men had higher muscle mass. Diabetic women had higher visceral fat. Diabetic and non-diabetic subjects (men as well as women) had similar TBW and TBW% but BMR was higher in diabetic women compared to non-diabetic women.
Table 2 shows the categorical data. In diabetic subjects the proportion of those with 1stand 2nddegree family history of diabetes was similar in both sexes. No control subject had family history of diabetes. A substantial number (around 70%) of diabetic subjects reported macrovascular complications. Diabetics (men as well as women) had higher proportion of those overweight and centrally obese compared to their nondiabetic counterparts.
Body composition and BMI
In diabetic subjects of both sexes, those lean had significantly lower body fat(percentage as well as mass), lower muscle mass but high muscle mass percentage,lower visceral fat, lower fat free mass, higher total TBW%, but lower TBW and BMR compared to their overweight counterparts. Similar differences were observed in nondiabetic subjects between those lean and overweight of both sexes, except for TBW%which was similar in lean and overweight non-diabetic women (Tables 3 and 4).
DISCUSSION
There are many reports on the profile of diabetic subjects in rural regions of India[18-28]but this is the first report from the Ratnagiri district of the Kokan area. Although from a small sample size, our data demonstrated that more than 50% of the men as well as the women subjects with diabetes were lean with a BMI well below the normal BMI cutoff of 25 kg/m2. Our study is clinic-based and not community-based. The National Family Health Survey[9]conducted by the government of India determined the prevalence of diabetes in the same region based on random blood sugar, being 9%among men and 5.8% among women. The same survey also found more than 70%prevalence of leanness based on BMI among men as well as women. This could be because the population in this region is constitutionally small.
Body composition depends on genetic makeup, dietary habits, physical activities,and susceptibility to chronic illness. Lean diabetes has been described in many populations across the world[29,30], and there have been extensive reports on lean diabetes in India. A prospective study across nine centers in India found about onefourth of T2DM patients to be lean or with BMI below 19 kg/m2. Prevalence of type 2 lean DM across the centers varied from 11% to 25%[13]. A recent report[31]showed significantly higher prevalence of T2DM without overweight and obesity in Indians compared to white Caucasians in the United States. Diabetes in lean patients has been described before[32,33]. There are reports on lean diabetes from other regions of South Asia, India, and Africa[29,34,35]. Populations described in these reports were lean, had a history of childhood malnutrition, and had poor socioeconomic status.
Another notable observation in our subjects was the increased muscle mass percentage but low BMR in lean subjects compared to those overweight subjects.Usually, BMR is directly proportional to muscle mass and as a metabolic response to starvation, the the primary concern is to supply energy to the brain[36]. In our study,the BMR was less in spite of better muscle mass. This could be because of less caloric intake despite heavy physical activity. Adverse intrauterine or early postnatal environment with insufficient nutrients has been suggested as a mechanism of beta cell failure in lean diabetics[29]. Another Indian study[37]found that type 2 diabetics had an unfavorable body fat distribution, with an increase in visceral fat compared to that in non-diabetics. However, there are differing opinions on the causality of this association[38,39].
Visceral fat is more important than total body fat, as excess visceral fat is a risk factor for both pre-diabetes and diabetes, being more so in Indians compared to other Asian populations. In our study, the diabetic subjects had higher visceral fat, andwithin the diabetics those who are lean had significantly lower visceral fat.Significantly higher muscle mass percentage in the low and normal BMI group of diabetics than in those overweight shows that BMI has limitations pertaining to detailing of body composition. This striking peculiarity in type 2 diabetics in our subjects is bound to influence the natural history of diabetes and it needs further study.
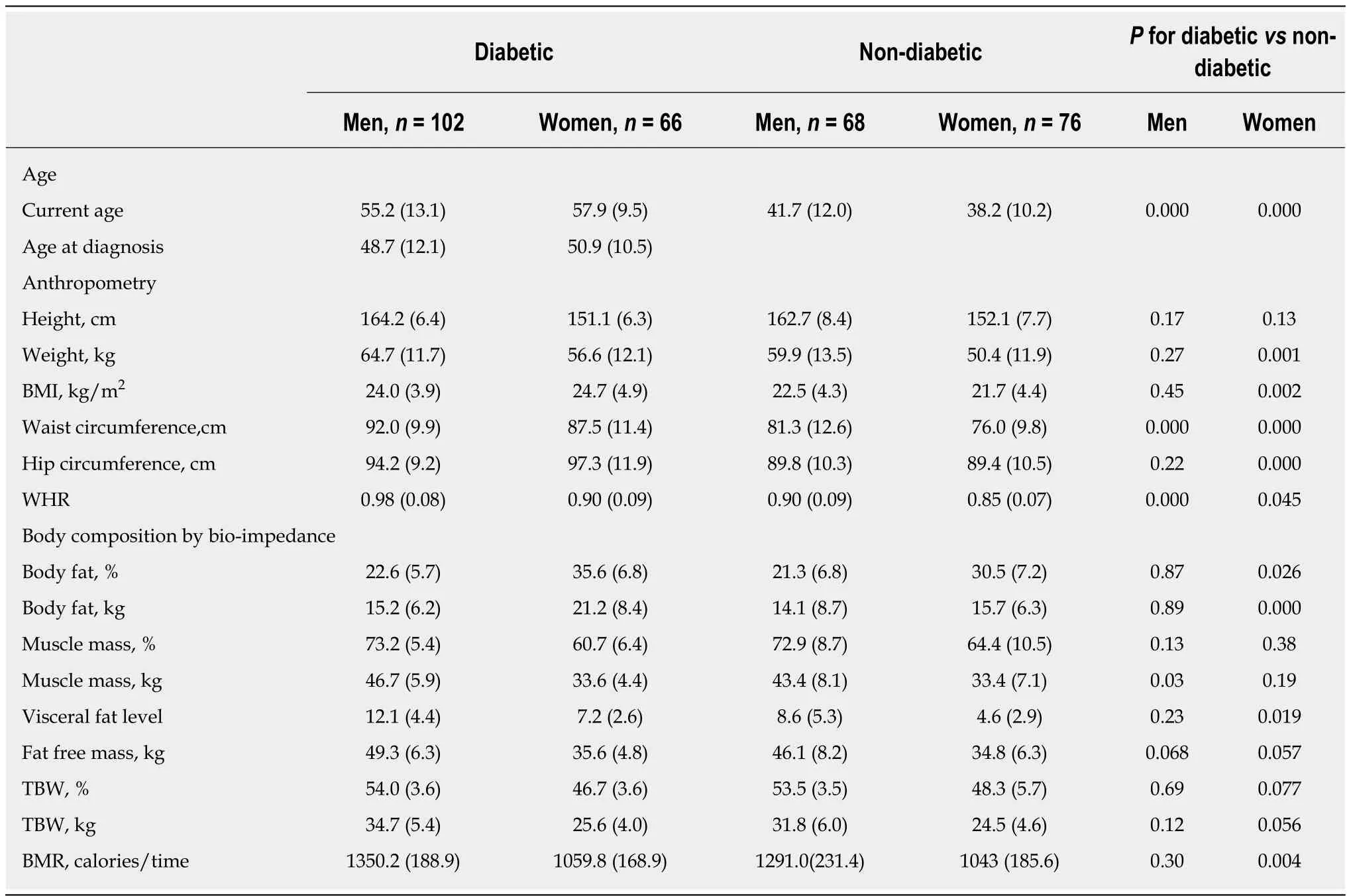
Table 1 Anthropometry and body composition
The Kokan region is characterized by mountainous terrain with poor soil quality,hot humid weather, poverty and deep-rooted superstitions which have led to widespread malnutrition amongst people[40]. Our hospital is located in a remote, rural area, and our study population is from a tribal region. A study from our center on 1290 school-going rural adolescents found underweight prevalence of 72%[41]. In a pilot study on adolescent girls from Kokan, a high prevalence of micronutrient deficiencies was also found. More than 65% were deficient in calcium, zinc and folic acid, and were malnourished[42]. In our hospital, 41.9% of the babies delivered were low birth weight (birth weight < 2500 g)[43]. The Tata Memorial Rural Out Reach Program (known as TMCROP) was implemented by our hospital in all 2200 villages in Kokan, and all villagers were screened for cancer by household survey. In that survey, 51.7% population had a BMI less than 18.5 kg/m2and only 4.5% could be classified as obese. These findings highlighted the leanness of the population of Kokan.
In our current study, more than 40% had family history for diabetes, which may suggest genetic predisposition; although, we do not have any genetic data on our subjects. Inadequacy of BMI in distinguishing leanness has suggested future studies should investigate the role of body composition in the development of lean diabetes[44].
Our study has some notable strengths. It has yielded the first report from the Kokan region, where malnutrition is very much prevalent. Unlike many other reports on diabetic subjects from other regions of India[18-28], we have collected the data on body composition. There are, also, many limitations to our study. The sample size is small and it used cross-sectional data from a rural diabetic clinic. No sample size calculations were done. We were only able to recruit a smaller number of controls,making the study prone to bias. We were constrained by the remoteness of the areawhere the hospital is situated. We could not use Dual-Energy X-Ray Absorptiometry(commonly known as DEXA; the current gold standard for body composition)because of the high equipment costs. We measured the body composition by bioelectrical impedance, using the TANITA body composition analyzer, which is a low cost, convenient and noninvasive technology, but concerns have been raisedin the past about the validity of the analyzer[45,46]and there is an urgent need to develop an ethnicity-specific equation for the Asian Indian population. We could not report on other cardiovascular risk markers (lipids, blood pressure) nor on the socioeconomic status of the participants as very little data were available as a part of patient history.We are aware of the fact that these subjects were diagnosed with diabetes at much earlier age. Recruitment of controls from the hospital setting has induced inherent selection bias. Thus, there is a need for a large community-based prospective study investigating the role of lean mass in development of diabetes in this region.
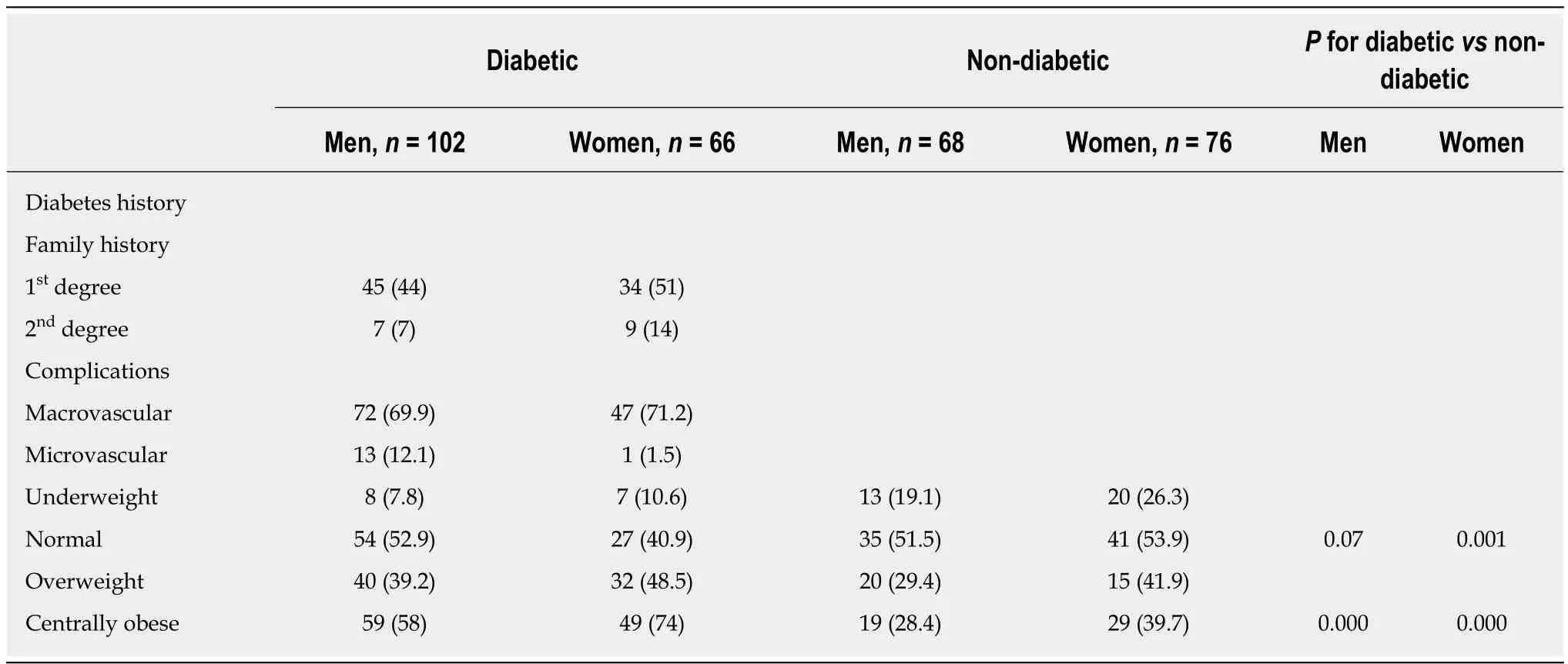
Table 2 Family history, diabetic complications, and anthropometric morbidity
To conclude, we attempted to investigate the role of lean body mass in development of diabetes in the predominantly underweight diabetic population of Kokan. The underlying mechanism of lean diabetes has not yet been fully explored and more studies are needed. The diabetic population in Kokan has near-normal body composition, and BMI has considerable limitations. Therefore, the physiological process producing these deviations in body composition and its metabolic significance need further investigations using larger sample sizes.
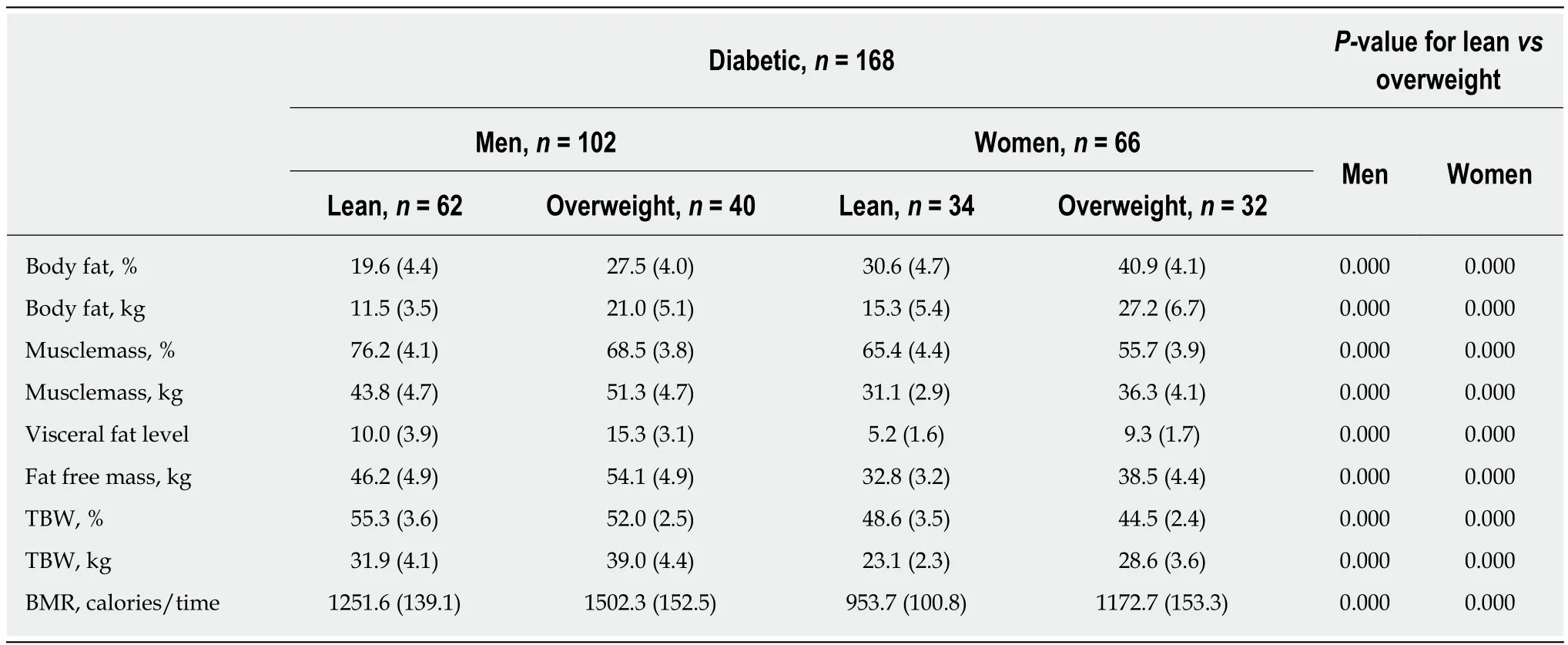
Table 3 Body mass index and body composition in diabetics
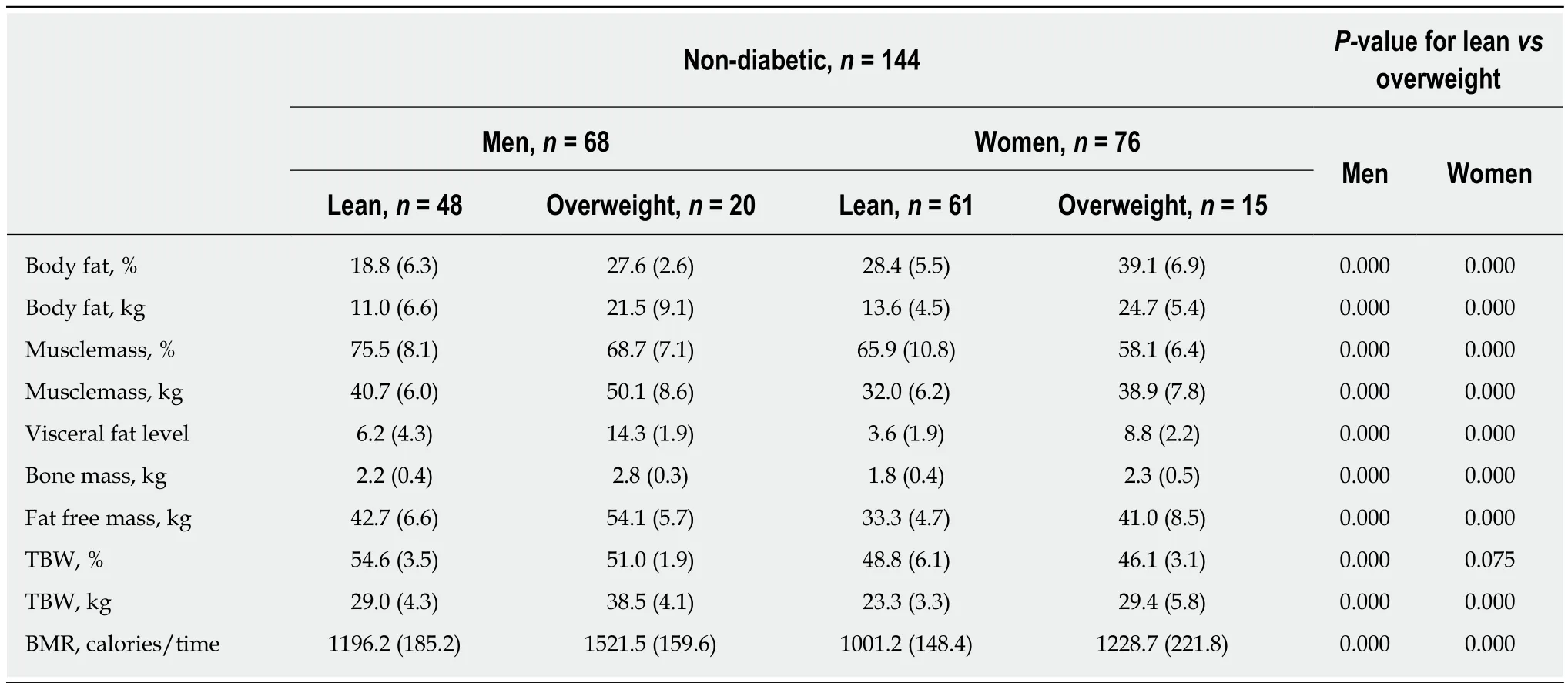
Table 4 Body mass indexand body composition in non-diabetics
ARTICLE HIGHLIGHTS
Research background
Recent years have seen a considerable increase in the burden of diabetes, hypertension and coronary heart disease in clinical practice in urban India. Recent studies in urban populations have shown an unexpectedly high prevalence of diabetes, and the prevalence is rising rapidly.
Research motivation
BKL Walawalkar Hospital carried out house-to-house surveys of 2200 villages in 2003-2010. In that survey, 51.8% of the subjects hadbody mass index (BMI) < 18.5 kg/m2 and only 4.5% were overweight, with BMI > 25 kg/m2. Another survey of 11521 adolescent girls from rural schools that was conducted in 2011-2017 showed that 64% of the girls had grade 1 to 3 thinness, based on the International Obesity Task Force standards, and stunting was seen in 22% to 28% of the girls.Thus, the overall population of Kokan is lean in their body stature. The same survey also found a more than 70% prevalence of leanness based on BMI among men as well as women. This, again,reinforced the leanness of the population of Kokan.
Research objectives
In order to investigate body composition of diabetic people from the BKL Walawalkar Hospital Clinic, a clinic-based case control study was carried out.
Research methods
One hundred sixty-eight type 2 diabetic patients (102 men) attending the outpatient department at a rural hospital and 144 non-diabetic controls (68 men) in the Chiplun area of the Kokan region were recruited. History of diabetes and anthropometric measurements were recorded,and body composition was measured by bioimpedance using the TANITA analyzer. All analyses were performed using SPSS 16.0 statistical software.
Research results
In this study, more than 45% of diabetic subjects had a 1stdegree family history of diabetes, and more than 50% had macrovascular complications. The average BMI in the diabetic subjects was 24.3 kg/m2. Underweight and normal diabetic subjects (men as well as women) had significantly lower body fat percentage, higher muscle mass percentage, lower visceral fat and lower basal metabolic rate compared to their overweight counterparts. Our data pave the way for a new theory of undernutrition as a risk factor in predisposing the Kokan population to diabetes.
Research conclusions
Undernutrition should also be considered as a risk factor for diabetes in lean patients. The molecular basis and physiological adaptations to undernutrition need to be explored.
Research perspectives
Lean diabetics had significantly lower body fat percentage, higher muscle mass percentage,lower visceral fat and lower basal metabolic rate compared to overweight diabetics. This could indicate a metabolic response to less caloric intake despite heavy physical activity, and this mechanism needs to be investigated. The diabetic population in Kokan has near-normal body composition and BMI has considerable limitations. Therefore, the physiological process producing these deviations in body composition and its metabolic significance need further investigations on a larger scale.
ACKNOWLEDGMENTS
Faculty of Medicine Department, BKL Walawalkar Rural Medical College.
杂志排行

World Journal of Diabetes的其它文章
- Exploratory metabolomics of metabolic syndrome: A status report
- Early vs late oral nutrition in patients with diabetic ketoacidosis admitted to a medical intensive care unit
- Relationship between sonographically measured median nerve cross-sectional area and presence of peripheral neuropathy in diabetic subjects
- Effects of diabetic ketoacidosis in the respiratory system
- Update on biomarkers of glycemic control