Update on biomarkers of glycemic control
2019-02-20MajaKrhaMarijanaVuLovren
Maja Krhač, Marijana Vučić Lovrenčić
Abstract Attaining and maintaining good glycemic control is a cornerstone of diabetes care. The monitoring of glycemic control is currently based on the self-monitoring of blood glucose (SMBG) and laboratory testing for hemoglobin A1c (HbA1c),which is a surrogate biochemical marker of the average glycemia level over the previous 2-3 mo period. Although hyperglycemia is a key biochemical feature of diabetes, both the level of and exposure to high glucose, as well as glycemic variability, contribute to the pathogenesis of diabetic complications and follow different patterns in type 1 and type 2 diabetes. HbA1c provides a valuable,standardized and evidence-based parameter that is relevant for clinical decision making, but several biological and analytical confounders limit its accuracy in reflecting true glycemia. It has become apparent in recent years that other glycated proteins such as fructosamine, glycated albumin, and the nutritional monosaccharide 1,5-anhydroglucitol, as well as integrated measures from direct glucose testing by an SMBG/continuous glucose monitoring system, may provide valuable complementary data, particularly in circumstances when HbA1c results may be unreliable or are insufficient to assess the risk of adverse outcomes. Long-term associations of these alternative biomarkers of glycemia with the risk of complications need to be investigated in order to provide clinically relevant cut-off values and to validate their utility in diverse populations of diabetes patients.
Key words: Diabetes mellitus; Hemoglobin A1c; Fructosamine; Glycated albumin; 1,5-anhydroglucitol; Plasma glucose; Glucose variability; Diabetic complications
INTRODUCTION
Attaining and maintaining good glycemic control is the cornerstone of diabetes care[1].The results of the seminal Diabetes Control and Complications Trial (DCCT) clearly evidenced that glycemic control is causatively related to microvascular complications in type 1 diabetes[2]. A long-term follow-up in the Epidemiology of Diabetes Interventions and Complications Study (EDIC) confirmed that keeping glycemia as close as possible to its normal range with intensified insulin therapy ameliorated both microvascular and cardiovascular complications for 30 years in the same cohort of patients[3].
Similar evidence of the beneficial effect of intensive glucose control practices in reducing the risk of diabetic complications, adverse cardiovascular outcomes and mortality were shown in type 2 diabetes patients in both the United Kingdom Prospective Diabetes Study (UKPDS) intervention and in follow-up trials[4,5].However, although additional intensification of glucose control in type 2 diabetes patients provided some benefits[6,7], it was associated with serious adverse outcomes such as an increased overall mortality[8]that was most likely due to severe hypoglycemia as a side-effect of a more aggressive antihyperglycemic therapy[9].These data indicated that a personalized approach to glycemic goals that uses clinically validated biomarkers rather than a “one-size-fits-all” concept may provide a valid rationale for optimal diabetes care.
The concept of glycemic control monitoring is currently based on self-monitoring of blood glucose (SMBG) and laboratory testing for hemoglobin A1c (HbA1c), which is a surrogate biochemical marker of the average glycemia level over the previous 2-3 mo period[10]. HbA1c emerged as a key determinant of the risk cut-off for diabetic complications and as a setting point for optimal glycemic control in both DCCT and UKPDS trials, and it is considered to be a gold standard of diabetes care in contemporary clinical practice[11]. HbA1c provides valuable, standardized and evidence-based information that is relevant for clinical decision-making; however,several biological and analytical interferences, as well as clinical conditions, limit its accuracy in reflecting the true glycemia level[12,13]. Recent technological advances in the field of continuous glucose monitoring systems (CGMS) have revealed new insights in short-term glucose dynamics which are not reflected by HbA1c, although it seems to be relevant in assessing the risk of diabetic complications[14,15].
Thus, alternative glycemic markers that provide reliable information about glycemic control in addition to and beyond HbA1c are needed to improve the quality of clinical care across a heterogeneous diabetes population[16,17].
The aim of this narrative review is to provide a critical update on the use of HbA1c and alternative biomarkers of glycemic control, with a particular emphasis given to the need for a personalized approach in utilizing and interpreting different tests in a clinically meaningful manner.
HBA1C
HbA1c results from the posttranslational modification of hemoglobin A by the nonenzymatic covalent binding of glucose to the N-terminal valine of the β-globin chain[10]. This reaction is termed glycation and affects all structural and circulating proteins with free amino-acid residues that are available for binding monosaccharides. The glycation of hemoglobin is a two-step chemical reaction whereby glucose covalently binds to the free amino-groups within globin chains[18].The first step of this process results in labile aldimine (a Schiff base), which can either dissociate or further convert to a stabile ketoamine by an Amadori rearrangement,depending on the glucose concentration in the blood[10]. HbA1c was first observed as a minor chromatographic fraction of adult hemoglobin in 1958 and was named according to its chromatographic column elution sequence[19], but its relevance in diabetes was revealed in 1969 by Rahbar[20], who observed significantly higher HbA1c values in diabetic patients. Since glycation is a nonenzymatic reaction, it complies with the law of mass action. Thus, assuming normal erythropoiesis and a stable hemoglobin concentration, HbA1c reflects the average glycemia level during one red blood cell life cycle (2-3 mo)[21].
Considering the high biological variability, the dynamics of glucose, as well as the limitations of blood glucose monitoring technology, at that time, the possibility of obtaining an integrated average glycemia value by the measurement of a single biomarker elicited immense interest and provided a powerful tool in both diabetes research and clinical management. HbA1c testing was soon facilitated by the development of a new analytical methodology that was suitable for use in clinical laboratories.
Various analytical methods for HbA1c determination commonly utilize either of the two principles (Table 1): (1) HbA1c separation from other hemoglobin fractions that is based on charge differences using either chromatography or electrophoresis; or(2) the direct measurement of HbA1c by specific binding (immunochemistry or affinity) or enzymatic cleavage[22]. Due to differences between these analytical methods in their use of different principles and a lack of standardization, HbA1c testing inherently suffers from a significant between-method variability which has seriously affected its clinical accuracy in the longitudinal monitoring of average glycemia with different methods and comparing the results of the DCCT- and UKPDS-derived targets. Heterogeneity of molecular entities that were measured by different methods significantly contributed to the analytical variability, as the glycation reaction involved not only β-N-terminal valine but also other accessible amino groups within the α and β-globin chains, and these results depended on the type of analyte that was captured by a particular method[12]. Thus, the standardization of the HbA1c measurement and reporting that included a uniform definition of the analyte was shortly identified as one of the most important issues in diabetes care[23,24].
Clinical harmonization was accomplished within the National Glycohemoglobin Standardization Program (NGSP), which was established by the American Diabetes Association (ADA) and the American Association of Clinical Chemistry (AACC). The goal of the NGSP was to harmonize the HbA1c results that were obtained by different methods with the highly reproducible but insufficiently specific method (ionexchange chromatography) that was used in the DCCT and UKPDS trials, thereby enabling the traceability and comparability of results to the evidence-based clinical criteria[25]. Almost simultaneously to the NGSP, the International Federation of Clinical Chemistry (IFCC) set up an HbA1c Standardization Program that was aimed at designing a comprehensive reference system with both reference methods and a primary reference standard for a structurally-defined analyte[23,26,27]. The comparison between the two reference systems revealed an excellent linear correlation between the DCCT- and IFCC-reference systems but significantly lower HbA1c values with the latter, more specific method. This finding raised concerns regarding the risks of deterioration of the glycemic control with the adoption of the new reference system,which had been reported previously[28].
In 2010, a Global Consensus on HbA1c measurement and reporting was issued by an international committee representing the ADA, European Association for the Study of Diabetes (EASD), International Diabetes Federation (IDF), IFCC and International Society for the Pediatric Diabetes (ISPAD)[29]. Briefly, the Global Consensus defined the IFCC reference as the only valid anchor for commercial methods calibration and a dual reporting of the HbA1c results as mmol/mol (IFCC-related units) and % (NGSP/DCCT-related units). A master equation describing the relationship between the two reference systems should be used for the interconversion of the results:
HbA1c NGSP/DCCT (%) = 0.09148 × HbA1c IFCC (mmol/mol) + 2.152
HbA1c IFCC (mmol/mol) = 10.93 × HbA1c NGSP/DCCT (%) - 23.50
Editors of scientific journals were encouraged to require both units of HbA1c reporting to promote the clarity and comparability of results between studies that used HbA1c as an outcome measure and to facilitate the combination of these results in meta-analyses. The Global Consensus definitely enabled the uniform traceability and improved analytical quality of HbA1c measurements[12]; however, it failed to harmonize the reporting of these results, as different countries use different reporting units, which may thus complicate a direct comparison of results across the world[30].
Today, the analytical procedures for HbA1c measurement are harmonized and the between-method/laboratory variabilities have been gradually reduced towards adesirable goal, which is a coefficient of variation (CV) < 3.5%[12]. Regarding the withinlaboratory imprecision, current guidelines recommend a CV < 2% for NGSP-HbA1c equivalents[31], and this is achievable with almost all of the commercially available laboratory methods apart from point-of-care systems for HbA1c testing, which still need improvement[22]. However, global harmonization and ongoing efforts to improve the analytical quality[32]cannot obviate the limitations of HbA1c measurement due to the hemoglobin-related interferences.

Table 1 Characteristics of the analytical methods for hemoglobin A1c measurement
It has long been recognized that hemoglobin variants interfere with HbA1c synthesis and measurement, and this interference depends on the nature of the congenital disorder afflicting hemoglobin synthesis and the analytical method that is used to measure HbA1c[22]. Thalassemia traits, HbS, HbC, HbE and HbF are among the most abundant hemoglobin-related interferences[33]. Additionally, other posttranslational modifications of hemoglobin such as carbamylation by uremic toxins in end-stage renal disease may significantly interfere with some HbA1c assays[34]. It should be noted that the majority of interferences have been mitigated by improvements of analytical methodologies, and the remaining interferences have been depicted and rigorously scrutinized. A comprehensive list of HbA1c methods that have been characterized for their susceptibility to hemoglobin-related interferences is available and is continuously updated on the NGSP website[35].
Biological confounders influencing the accuracy of HbA1c as a glycemic marker have emerged as a significant issue after analytical harmonization, despite the fact that a substantial intraindividual variability in HbA1c values was recognized long ago. Studies on the relationship between HbA1c measurements and average glycemia levels revealed a strong linear correlation with a wide interindividual variability, e.g.,an HbA1c of 7% (53 mmol/mol) could correspond to an average glucose concentration ranging from 6.8 to 10.3 mmol/L[36]. Physiological factors such age and ethnicity, as well as genetics, seem to be major determinants of this variability.
Age was found to be associated with a gradual increase of HbA1c levels in nondiabetic individuals independently of sex and level of glycemia, indicating that age-specific reference intervals/clinical cut-off points may improve the clinical accuracy of this test in both the diagnosis and management of diabetes[37]. There are ethnic differences in HbA1c values even when glycemia levels are the same; a recent meta-analysis revealed that Caucasians have slightly lower HbA1c values in comparison to persons of other ethnic groups[38]. While the clinical relevance of this finding needs to be further investigated, the authors concluded that a better understanding of the molecular mechanisms behind this observed between-race variability in HbA1c may improve its clinical applicability.
Recent genetic studies have revealed that multiple genomic loci are associated with HbA1c levels, and this could provide a plausible explanation for the physiological factors determining its variability and clinical utilization towards a more personalized approach[39]. Among the 60 genetic variants that were found to influence HbA1c, 19 variants associated with glycemic pathways were identified, and among the rest of variants that were involved in nonglycemic pathways, 22 erythrocytic variants were found[40]. Among these, a variant on the X chromosome coding for glucose-6-phosphate dehydrogenase (G6PD) was associated with a significantly higher HbA1c variability in populations of African ancestry when compared to other ethnic groups.This highly prevalent variant is associated with a shorter erythrocyte lifespan and,consequently, falsely decreased HbA1c levels, which may have serious impacts for diabetes care in afflicted individuals[40].
Nonglycemic factors affecting HbA1c levels include erythropoiesis, hemoglobin synthesis and conditions influencing red blood cell survival. Deficiency anemias generally elicit falsely increased HbA1c levels due to the increased levels of aged erythrocytes that are found in patients with this disease, whereas falsely decreased HbA1c levels can be observed in hemolytic anemias of any cause[41].Nonhematological conditions influencing HbA1c values include pregnancy, chronic renal failure and certain medications[22]. Variability in the normal erythrocyte lifespan is another significant confounder of HbA1c accuracy. Malka et al[42]recently proposed a mechanistic mathematical model integrating hemoglobin glycation and red blood cell kinetics that provided a personalized insight into average glucose levels and reduced the occurrence of diagnostic errors due to a misinterpretation of average glycemia (as reflected by HbA1c) by more than 50%. The applicability and clinical utility of the proposed model have yet to be determined.
Furthermore, part of the variability in HbA1c is considered to be a consequence of differences in glycation rate, which is a concept that was proposed as the “glycation gap” 15 years ago[43]. The glycation gap hypothesis is based on the differences between the intra- and extracellular surrogate markers of average glycemia, i.e., HbA1c and fructosamine, and it was proposed as an explanation to the commonly encountered clinical problem of discrepancy between various glycemia measures that cannot be attributed to any other confounding factor[44]. In spite of subsequent evidence from a twin study that shows that the glycation gap may be a genetically determined characteristic of an individual[45], this concept has been considered implausible by some authors due to the lack of validating data or supporting evidence of the underlying mechanism[46]. Nevertheless, an accumulating body of evidence indicates that glycemic variability, as assessed by either the glycation gap or another discordance measure called the hemoglobin glycation index[47], is indeed associated with adverse diabetes-related outcomes such as mortality, micro- and macrovascular complications, and hypoglycemic episodes that are associated with intensive treatment[48,49]. Interindividual heterogeneity in glucose transport across the erythrocyte membrane was proposed as a possible explanation for inconsistencies between HbA1c and other measures of glycemia[50]. Genome-wide association studies also support the plausibility of the glycation gap concept since one of the identified loci, FN3K, encodes fructosamine-3-kinase, which is an enzyme that is involved in deglycation of glycated proteins[39]. Dunmore et al[51]recently reported a significant difference in the erythrocyte fructosamine-3-kinase activities between glycation gap categories and pinpointed FN3K both as a novel predictor of the risk for development of and as a potential target for the prevention of diabetic complications.
Current clinical guidelines recommend regular HbA1c testing twice a year in all diabetic patients who achieve their glycemic targets, and they recommend an increased frequency of testing not to exceed four times a year for patients who have changed therapy and/or have not achieved their treatment goals[1]. The general recommendation is to keep the HbA1c levels < 7% (53 mmol/mol); however, the target should be individualized for individual patients depending on the diabetes duration, age or life expectancy, CVD and other comorbidities, hypoglycemia unawareness and psychosocial factors[52]. A reference change value of 0.5% (5 mmol/mol) in the longitudinal monitoring of an individual patient is considered to be clinically significant[22].
The use of HbA1c as a diagnostic test for diabetes with a diagnostic cutoff set at an HbA1c level of 6.5% (48 mmol/mol) has recently been recommended by prominent professional organizations and by the Word Health Organization[53,54]. Low intraindividual biological variability, the stability of the analyte and the independence of results to the prandial status were the most pronounced advantages of HbA1c over plasma glucose, while higher costs and the limited availability of the test were considered as its disadvantages[55]. However, the diagnostic accuracy of HbA1c at a given threshold was found to be poor in many studies[56-58], as well as in a recent global surveillance on the prevalence and diagnosis of diabetes[59], which is at least in part a consequence of numerous biological confounders[38,60]. A comprehensive list of biological, (patho) physiological and pharmacological factors that may influence the synthesis, measurement and/or interpretation of HbA1c is presented in Table 2.
GLYCATED PROTEINS
Fructosamine (1-amino-1-deoxy fructose) is a common term for all glycated plasma proteins. It is a ketoamine that is formed by the irreversible nonenzymatic binding of glucose to plasma proteins in a process called glycation. Glycation is a nonenzymatic process where a labile Schiff base (aldimine) is formed at an early stage and is subsequently rearranged to a stabile Amadori product (ketoamine) due to the covalent binding of glucose to the lysine, arginine and cysteine amino-group residues within protein molecules[61].
Glycated albumin (GA) is formed in a similar reaction as fructosamine and is specific to albumin molecule[62]. In conditions that are associated with high glucose levels, plasma proteins are exposed to greater glycation, which leads to increasedfructosamine and GA formation. Fructosamine and GA reflect the average blood glucose concentration during the lifetime of either total plasma proteins or albumin,both of which are within the range of two to three weeks[63].
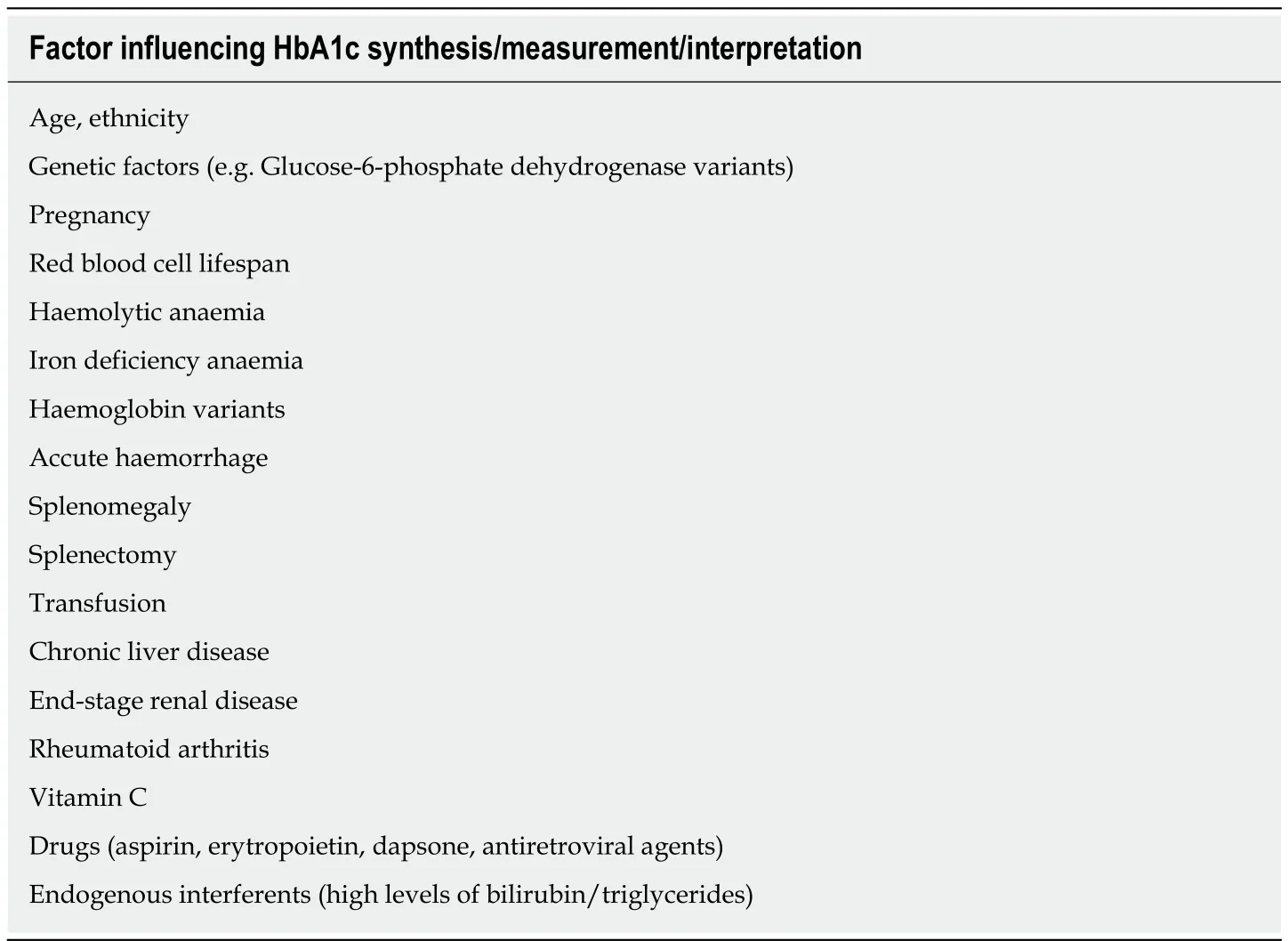
Table 2 Biological, (patho)physiological and pharmacological factors influencing hemoglobin A1c
Despite the fact that albumin is a major constituent of plasma proteins,fructosamine and GA may not be considered as totally equal measures of glycemia due to their differences in analytical procedures and their currently established clinical performance. Fructosamine was identified long ago, but the lack of analytical standardization and problems with the assay's specificity and susceptibility to interference by hyperlipidemia limited its use in diabetes management. Additionally,there was insufficient evidence to correlate fructosamine and GA with long-term outcomes in patients with diabetes[64].
However, over the years, the development and improvement of methods for determining fructosamine and GA have paved the way for many studies that focused on their analytical and clinical significance. Affinity chromatography[65], ion-exchange chromatography[66]and high-performance liquid affinity chromatography[67]were all developed as methods for the direct measurement of GA along with liquid chromatography-tandem mass spectrometry (LC-MS/MS) as a “gold standard”[68].However, these methods are complicated and expensive and require dedicated equipment and expertise, and this has limited their routine use. Consequently,simpler and more affordable colorimetric and enzymatic methods, applicable on various automated analytical platforms, were developed for use in clinical laboratories[69]. Enzymatic methods showed a better analytical performance and were free of colorimetric interferences (e.g., bilirubin)[70-72]. Various commercial kits are available for GA measurement depending on the type of enzyme that was used in the reaction and the units used to express the results (µmol/L, mmol/L or % GA fraction).
Currently, the method of choice for fructosamine determination is the second generation of the nitroblue tetrazolium colorimetric procedure, in which there is a separation of glycated from nonglycated proteins based on their differences in chemical reactivity[73]. The assay itself is inexpensive, rapid, simple, highly specific and free of interferences from uric acid or polylysine. Nevertheless, despite many improvements, this method is still sensitive to rapid changes in ambient temperature and interferences from extremely high levels of some compounds with reducing properties, such as bilirubin and vitamin C[64]. Still unresolved is the issue of whether the resulting fructosamine measurements should be corrected for either total protein or albumin concentrations. The results are relatively ambiguous[74], but it was recently reported that correcting the fructosamine measurement for proteins may improve its correlation with HbA1c and its overall performance in detecting diabetes[75].
Given the faster protein metabolic turnover, fructosamine and GA values reflect shorter-term glycemia levels rather than HbA1c. Additionally, fructosamine and GA are not influenced by anemia or hemoglobinopathies such as HbA1c is, and they can therefore be used in conditions where HbA1c is not reliable due to analytical or biological interferences[62]. In conditions such as pregnancy[76]and treatment modifications[77]fructosamine and GA can detect changes in average blood glucose earlier than HbA1c and thus provide more timely information about the achievement of glycemic control[62,78,79].
Both fructosamine and GA are the markers of choice when glycemic control needs to be assessed in patients with severe chronic kidney disease (CKD) (stages 4 and 5)[80].Additionally, in stage 5 CKD patients on hemodialysis, GA can be used as a predictor of overall survival and cardiovascular mortality[81]. Due to the reduced production and lifespan of red blood cells and to erythropoietin treatment in CKD patients,HbA1c cannot be used as reliable marker, as it can significantly underestimate the true glycemic status in these patients[82].
The distribution of GA in healthy subjects has been described in diverse populations[83,84]. The Large Atherosclerosis Risk in Communities (ARIC) study was conducted in a cohort of almost 12000 participants and proved a strong association of fructosamine and GA with the incidence of diabetes and microvascular complications(prevalent retinopathy and risk of CKD)[85]. Together with fructosamine, GA was reported to be strongly associated with HbA1c and fasting glucose[86]. Furthermore, a recent study by Bellia et al[87]evaluated the potential clinical usefulness of GA for the diagnosis of diabetes in an asymptomatic Caucasian population (specifically in Europe) with an elevated risk of developing diabetes. At the GA cut-off of 13.5%, a high sensitivity (88.9%; 95%CI: 65.3-98.6) and a good specificity (60.4%; 95%CI: 54.8-65.9), was demonstrated for its possible screening use in similar subjects[87].
It is important to note that fructosamine and GA measurements are not reliable in some physiological and pathological conditions. Every clinical condition that can affect protein and albumin metabolism (nephrotic syndrome, hyperthyroidism,glucocorticoid therapy, liver cirrhosis, etc.) may affect these results, where they would also require careful interpretation[14,62]. Additionally, similar to HbA1c, fructosamine and GA are determined by genetic variants that are associated with both glycemic and nonglycemic components, both of which should be considered when putting the results in a clinical context[84].
1,5-ANHYDROGLUCITOL
1,5-Anhydroglucitol (1,5-AG) is a monosaccharide that is structurally identical to D-glucose with the absence of the C-1 hydroxyl group. It is derived mainly through food intake and also absorbed by the intestine at a rate of approximately 4.4 mg/d. The main source of 1,5-AG is soy beans, but small amounts can be found in rice, pasta,fish, fruits, vegetables, tea, milk and cheese. The metabolic role of 1,5-AG is still quite unknown. It circulates in body in its free form and can be found in all organs and tissues (1,5-AG pool) with the total amount several times higher than that in plasma[88]. A negligible amount is presumed to be synthesized de novo[89]. 1,5-AG intake is regulated by its urinary excretion, and 99.9% of 1,5-AG is reabsorbed by the kidneys by the specific sodium glucose active cotransporter (SGLT4)[88,90]. Reabsorption is competitively inhibited by glucose. When the plasma glucose level exceeds the renal threshold for glucosuria (approximately 10 mmol/L), 1,5-AG is excreted in the urine,which results in a rapid reduction of its serum levels[91]. Thus, low values of 1,5-AG reflect both high circulating glucose levels and glucose fluctuation, or so-called hyperglycemic excursion[92]. This biomarker may be useful to differentiate between diabetic patients with well-controlled HbA1c but with extensive glucose fluctuations[93]. After normoglycemia is restored, the 1,5-AG concentration returns to its normal value at a rate of 0.3 µg/ml per day, and it can take up to 5 wk for this value to increase up to its normal level[94]. Due to its half-life of approximately 1 to 2 wk, 1,5-AG can be used as a potential marker for short-term glycemia[95]. Additionally,there is evidence that 1,5-AG reflects the 2-h postprandial glucose (PPG) values of the 2 preceding weeks in moderately controlled patients and is more sensitive and specific than HbA1c[96]. PPG values are especially important for clinical decisionmaking concerning changes in the diet or in changes of the pharmacologic treatment of diabetes and overall glycemic control[97].
1,5-AG can be measured in serum, EDTA-plasma and urine samples. There are two commercially available enzymatic kits for its blood measurement: the Glyco-MarkTM(GlycoMark, Inc) kit that is used in United States and the Determiner-L (Kyowa Medex, Tokyo) kit that is used in Japan. Both of these methods can be applied to automated chemistry analyzers. Recent data has shown a good between-method comparability despite slightly different results that were obtained in the same samples[98]. Another method for the determination of 1,5-AG is chromatography,specifically gas chromatography-mass spectrometry (GC/MS) and high-performance liquid chromatography (HPLC). These methods are sensitive and precise but require sample preparation and are time-consuming and cumbersome[99]. Urine, a sample with lower 1,5-AG levels, requires a more sensitive method such as liquid chromatography/mass spectrometry (LC/MS) or HPLC[100].
Regarding its association with diabetes and microvascular complications, the ARIC study provided evidence that 1,5-AG levels were associated with prevalent retinopathy and incident CKD, particularly in patients who were diagnosed with diabetes. Despite the low association in nondiabetic subjects, there was a good risk prediction of incident diabetes in both groups[86,101].
The results obtained from patients with certain conditions such as kidney disease or pregnancy must be carefully interpreted due to the changes in renal function during these conditions which influences the threshold for glucose excretion.Nevertheless, 1,5-AG can be reliable in subjects with mild to moderate renal insufficiency as a marker for glycemic control[102]. Furthermore, 1,5-AG can be helpful in cases when frequent adjustments in therapy are required and glycemic control has to be maintained[94].
Given the limitations of HbA1c and the recently collected evidence on the clinical utility of nontraditional markers of glycemia, their implementation in clinical practice is expected. The recently published reference intervals provide the most valuable tool in facilitating the translation of these biomarkers into routine clinical practice. In a healthy reference population of almost 1800 individuals, the reference ranges for fructosamine, GA and 1,5-AG were reported as 194.8-258.0 µmol/L, 10.7%-15.1% and 8.4-28.7 µg/mL, respectively[103].
DIRECT MEASURES OF GLYCEMIA
Fasting and postprandial plasma glucose (FPG and PPG, respectively) are obvious measures of glycemia, providing “snapshot” glucose values for primary use in targeting treatment goals, which are currently set at ranges of 4.4-7.2 mmol/L for FPG and < 10.0 mmol/L for PPG[1]. The contributions of these measures to HbA1c have been evaluated[104], and significant association of PPG with cardiovascular risks was evidenced[105]. Daily plasma glucose values are readily available to patients who perform SMBG as a part of their regular diabetes care but reviewing and interpreting the cumulative SMBG results may propose a significant challenge for healthcare professionals[106].
Advances in both the analytical accuracy and software supporting SMBG, the development of continuous glucose monitoring sensors and, most recently, flashglucose sensing technology, have prompted the development and validation of new,metrics-derived surrogate markers of glycemia which have improved our understanding of the complex glucose dynamics and have provided new tools for patients and healthcare providers in achieving optimal control of diabetes and reducing the frequency of acute and chronic complications of diabetes[13,14].
Among the integrated SMBG-derived metrics, the glycemic risk assessment diabetes equation (GRADE) and average daily risk range (ADDR) were found to best correspond with the degrees of risk of hypo- and hyperglycemia that were associated with the glucose profile[107], and they showed positive correlations with HbA1c and negative correlations with c-peptide levels[108].
As opposed to the SMBG-derived profiles, which are based on a limited number of static plasma glucose measurements throughout the day, CGMS enable a continuous insight into daily glycemia, thus enabling an individualized approach and offering a powerful tool for patients in achieving their glycemic targets and mitigating glycemic excursion. CGMS has yielded previously unreachable measures of glycemia such as average glucose exposure, time in range, hypo- and hyperglycemia and glycemic variability (glucose excursions). The glycemic variability was considered to be a significant risk factor for developing complications that was not reflected by HbA1c levels[13]. The advantages of using SMBG to improve patient outcomes have been amply evidenced in studies targeting various vulnerable populations of patients with diabetes such as children[109], pregnant women[110], the elderly[111], and the patients suffering from diabetic kidney disease[112]and from hypoglycemic episodes[113].However, the high costs, insurance-related limitations and patient- and healthcare provider-related attitudes still hinder a wider utilization of CGMS. The recently published International Consensus on Use of Continuous Glucose Monitoring is an encouraging step forward and is aimed at providing technical and clinical recommendations on the use of CGMS in conjunction with HbA1c, and it provides a comprehensive insight into the state-of-the-art evidence supporting CGMS-derived metrics to improve patient care and clinical outcomes[114].
CONCLUSION
Hyperglycemia is a key biochemical feature of diabetes that should be rigorously controlled and maintained in a range as close to normal as possible to mitigate the risk of diabetic complications. Both the level of and exposure to hyperglycemia, as well as glycemic variability, contribute to the pathogenesis of diabetic complications, with different patterns of disease pathogenesis in patients with type 1 or type 2 diabetes.Despite its analytical and biological limitations, HbA1c remains the key biomarker of long-term glycemic control. However, it has become apparent in recent years that other glycated proteins, 1,5-AG, and integrated measures from direct glucose testing by SMBG/CGMS may provide valuable data complementary to HbA1c, particularly in circumstances when the HbA1c results may be unreliable or insufficient to assess the risk of adverse outcomes (Table 3). Long-term associations of these alternative biomarkers of glycemia with the risk of diabetic complications need to be investigated to provide clinically relevant cut-off values and validate their utility in diverse populations of patients with diabetes.

Table 3 Characteristics of glycaemic biomarkers
杂志排行

World Journal of Diabetes的其它文章
- Exploratory metabolomics of metabolic syndrome: A status report
- Early vs late oral nutrition in patients with diabetic ketoacidosis admitted to a medical intensive care unit
- Relationship between sonographically measured median nerve cross-sectional area and presence of peripheral neuropathy in diabetic subjects
- Diabetes in the Kokan region of India
- Effects of diabetic ketoacidosis in the respiratory system