Significance of postoperative follow-up of patients with metastatic colorectal cancer using circulating tumor DNA
2019-02-12LucieBeneovTerezalkovRenataPtkovAnastasiyaSemyakinaKateinaMenclovJiPudilMiroslavRyskaMiroslavLevJaromimFilipPazdrekJiHochMilanBlahaMarekMinrik
Lucie Benešová, Tereza Hálková, Renata Ptáčková, Anastasiya Semyakina, Kateřina Menclová, Jiří Pudil,Miroslav Ryska, Miroslav Levý, Jaromír Šimša, Filip Pazdírek, Jiří Hoch, Milan Blaha, Marek Minárik
Abstract
Key words: Circulating tumor DNA; Metastatic colorectal cancer; Postoperative;Radicality of resection; Follow-up; Recurrence
INTRODUCTION
Around 50% of patients with colorectal cancer (CRC) are found to have synchronous liver or extrahepatic metastases at the time of diagnosis or will develop metachronous metastases within several years after surgery[1]. It is known that radical surgical resection - the R0 resection which involves a complete removal of the diseased tissue -is the only effective treatment option, ideally in combination with perioperative chemotherapy[2]. The 5-year survival rate for patients with surgical treatment ranges from 41% to over 70% compared to 5% if not treated[3-5].
Besides removal of metastases, postoperative patient follow-up is no less important as it allows for the timely identification of any progression or recurrence of the disease and prompt therapeutical response - whether by surgery or modification of systematic therapy. The monitoring of patients with metastatic CRC is predominantly based on imaging techniques such as ultrasonography (US), computed tomography(CT), positron emission tomography (PET), magnetic resonance imaging (MRI) or X-ray imaging (XRAY), usually with assessments of serum tumor markers carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9 (CA19-9). Nowadays,molecular biology techniques also play an irreplaceable role in the management of patients with CRC, considering that the decisions on cancer therapy are ever more supported by the knowledge of biological characteristics and genetic profile of the disease[6]. Most recently, the possibility for disease follow-up using circulating tumor DNA (ctDNA) has become available in addition to already implemented mutation profiling from tissue biopsies or resecates[7,8].
The term ctDNA means short fragmented DNA, which has historically been observed in blood circulation of patients suffering with metastatic stages of cancers[9,10]. ctDNA is often referred to as cell-free DNA to emphasize its exogenous nature in comparison to DNA originating from nuclei of the blood cells. Although the exact mechanism of its release into circulation is still subject to debate, there are several probable mechanisms of the ctDNA origin including: Apoptosis; necrosis;active release through lipoproteonucleotidic complexes (virtosomes); phagocytosis;and exocytosis[11]. Due to its exclusive origin in cancerous cells, ctDNA retains the fundamental imprint of its cancer genome including cancer-specific aberrations such as somatic mutations. Therefore, the ctDNA analysis has recently been promoted using the term “liquid biopsy”[12]. The main advantage of liquid biopsy, compared to the “classic” biopsy of tumor tissues is its minimal invasiveness and the associated minimal stress for the patient. Additionally, ctDNA is released to the bloodstream from all tumor foci, and thus a single blood sample contains the complete mutation spectrum of cancer clones present in the patient's body[13].
Besides liquid biopsy, ctDNA testing has proven to be a very promising instrument for long-term, postoperative follow-ups of patients with CRC, particularly in advanced stages. Being minimally invasive, it can be repeated over short periods for a long time with no significant burden to the patient, and moreover, this test shows high sensitivity and specificity to patients with preoperative ctDNA positivity[14]. The approach fundamentally relies on the applied methodology, which must be able to capture < 0.1% of ctDNA on the background of non-tumor DNA. Accordingly, the current techniques include dedicated approaches such as those based on digital PCR,BEAMing or deep sequencing[15]. In all cases, tumor-specific DNA alterations (usually mutations) found in the tumor tissue or occurring with a certain significant frequency in the given cancer are used as ctDNA positivity markers. However, the above mentioned methods have their limitations, particularly in terms of higher demands on the input DNA amount and the costs. Another sensitive, efficient, rapid and affordable method based on the formation of heteroduplexes with subsequent detection using denaturing capillary electrophoresis (DCE) has been used at our center for 10 years. This method can be used to detect a mutated locus in plasma with the sensitivity of 0.03% to 1% depending on the mutation to be determined (Table 1)with input DNA amount of tens of pg[16,17]. The specificity of this ctDNA test is 100%,which means that the presence of ctDNA always provides evidence that a tumor residue or tumor cells are present. As previously shown by us, ctDNA testing using DCE allows patient follow-up in real time, while ctDNA levels correlate very well with the current condition of the patient[17]. As we reported in this paper about a group of patients with metastatic CRC, ctDNA can be used in clinical practice,particularly for the evaluation of the radicality of surgery and for the timely detection of any progression or recurrence of the disease.
MATERIALS AND METHODS
Patients and samples
This study was conducted in cooperation with three prime surgery centers in the Czech Republic in accordance with the Declaration of Helsinki and was approved by ethics committees of the relevant hospitals. The forty-seven patients enrolled in the study had undergone the resection of synchronous or metachronous colorectal cancer metastases and tested positive for ctDNA before surgery, and were thus suitable candidates for postoperative ctDNA follow-up. Patient characteristics are listed in Table 2. All patients signed an informed consent form for the study. A tumor tissue sample was surgically obtained in each case. Peripheral blood samples for ctDNA analysis were collected in an anticoagulant solution before, 1 week after the surgery,and subsequently in several-month intervals during their follow-ups. Clinical patient data including tumor localization and type, surgical radicality, and CEA and CA 19-9 marker levels were also collected.
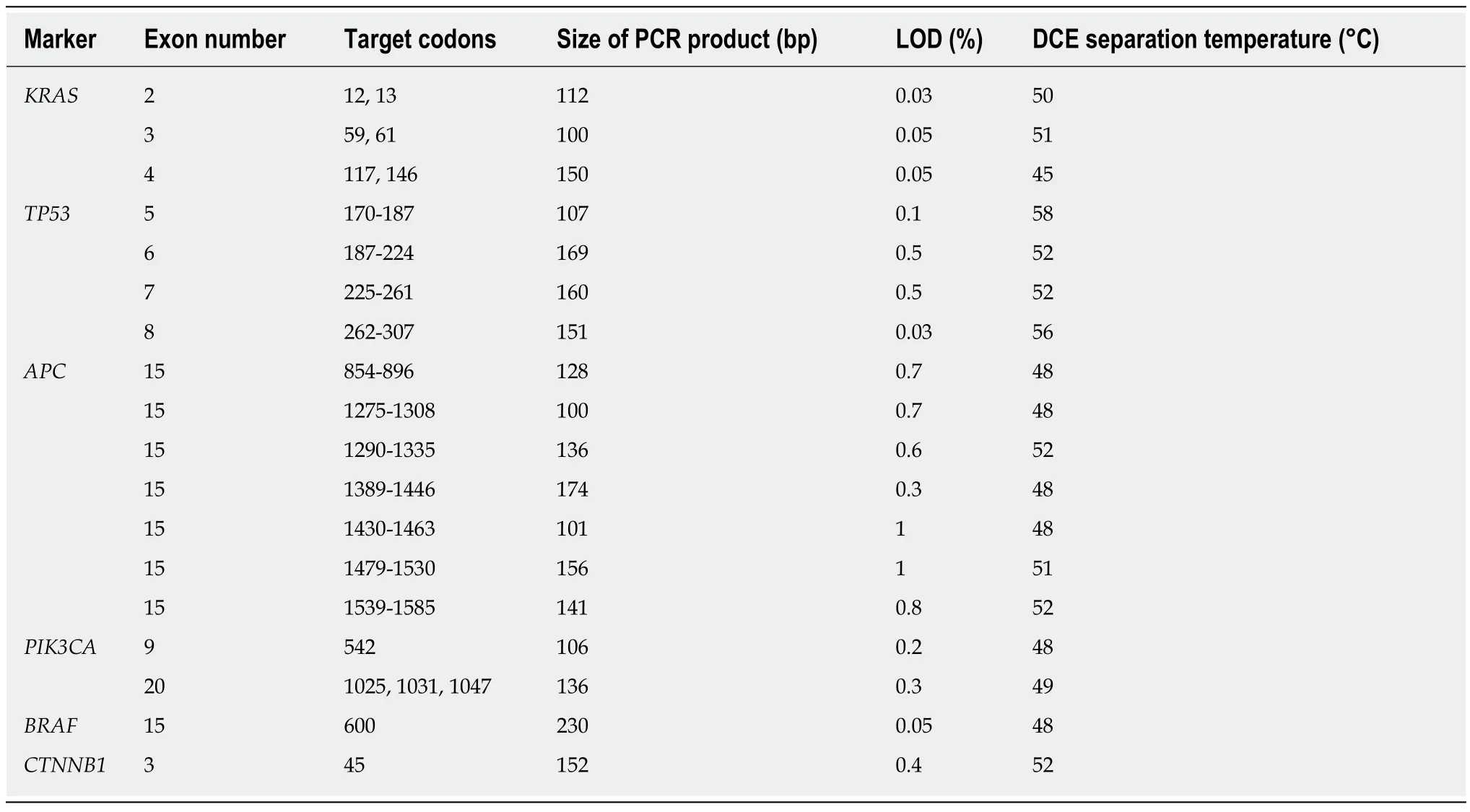
Table 1 Characteristics of the markers used for the mutation analysis[16,17]
DNA isolation and detection of mutations
Mutation profiles were determined in DNA isolated from tumor tissues,subsequently, the detected mutations were analyzed in plasma samples. Tumor DNA was isolated from the samples of native frozen (-20 °C) tissues using the GenElute™Mammalian Genomic DNA Miniprep Kit (Sigma Aldrich, St. Louis, MS, United States). ctDNA was isolated using the NucleoSpin Plasma XS (Macherey-Nagel,Dueren, Germany) from plasma according to the instructions of the manufacturer.Plasma was obtained by centrifugation of blood promptly after collection, and then immediately frozen at -20 °C. The mutations were identified using a panel for the detection of the most commonly mutated loci in theKRAS,TP53,APC,PIK3CA,BRAFandCTNNB1genes, which are characteristic for colorectal cancer (see Table 1 for details). Tumor tissue and ctDNA mutations were detected using PCR with the formation of heteroduplexes and subsequent separation using DCE. The principle of the method has been described previously[18].
Resection radicality and recurrence of the disease
The radicality of surgical removal of colorectal cancer metastases was determined by the pathologist based on examination of the resected samples' margins. Complete resections with no macroscopic or microscopic tumor residues were identified as R0.For R0 resections, the minimum distance of tumor cells from the resection line was > 0 mm. Microscopically incomplete resections, with a presence of tumor cells in the margin detected by the pathologist, were identified as R1. Macroscopically incomplete resections were identified as R2 and were classified as R2a (macroscopic presence of a residue of the primary tumor), R2b (macroscopic presence of distal metastases), R2c(macroscopic presence of any residue(s) of the primary tumor as well as of distal metastases)[19]. The surgical radicality assessments were supplemented with an analysis of postoperative ctDNA.
Disease recurrence was longitudinally monitored and was assessed using imaging methods (most commonly CT, MRI, US, XRAY) and using CEA (normal levels ≤ 5 ng/mL) and CA19-9 (normal levels ≤ 37 U/mL) tumor marker levels. Any abnormalities detected by imaging techniques or elevated levels of at least one tumor marker were considered recurrences. This data were correlated with the presence of ctDNA. The ctDNA was evaluated until recurrence or during the patient's follow-up period.
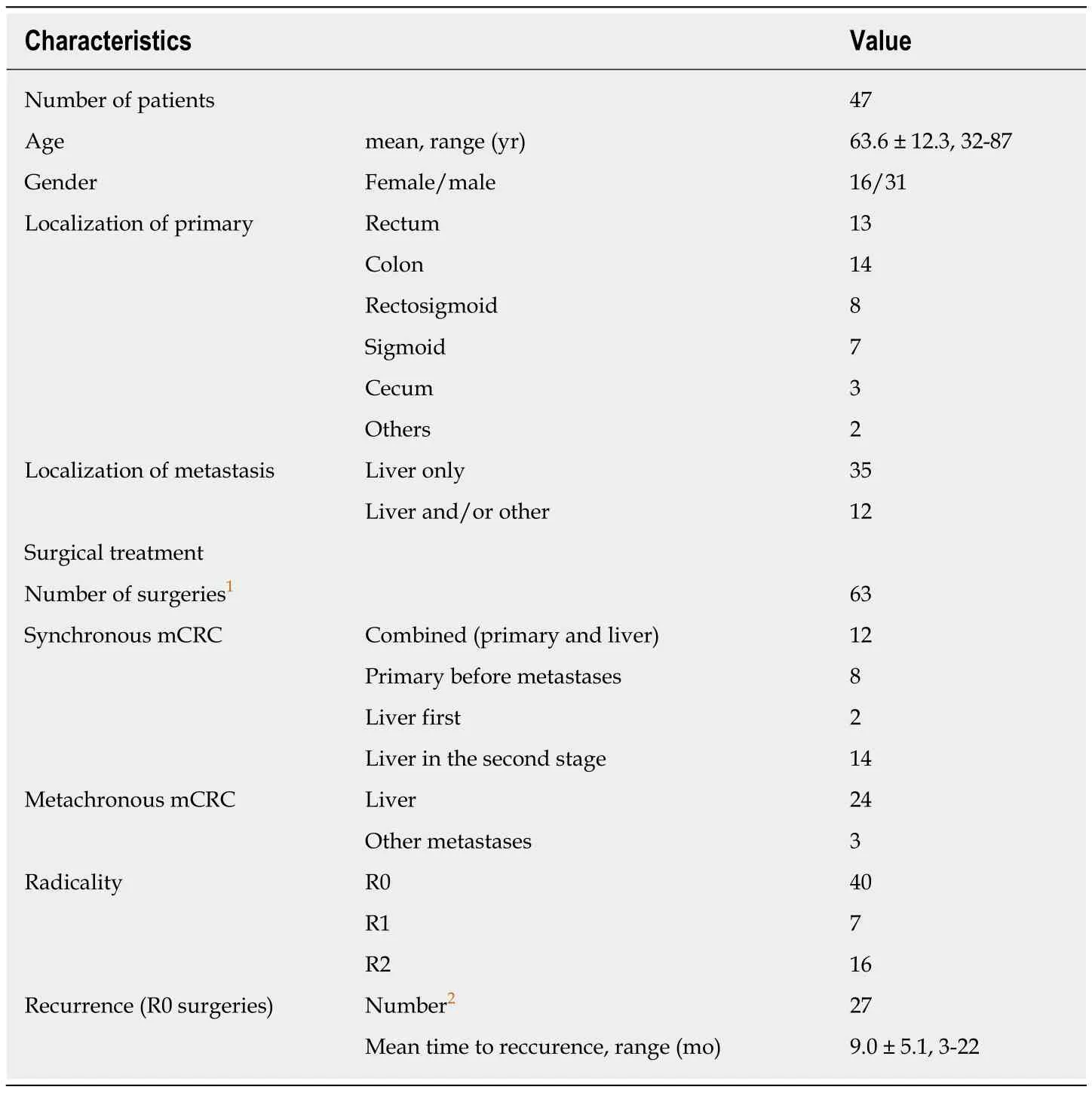
Table 2 Clinical patient data
RESULTS
Detailed information on the 47 patients enrolled in the study is available in Supplementary Table 1. In total, 79 tumor tissue samples (25 from the primary tumor, 6 from lymph nodes and 48 from distal metastases) and 202 plasma samples (51 before surgery, 39 after surgery and 112 during follow-up) were collected over the course of the study. A detailed overview of the collected samples and mutations detected in tumor tissue is provided in Supplementary Table 2.
Sixty-three resections were done during the study (including repeated resections during follow-up), which comprised 40 R0, 7 R1 and 16 R2 resections. A postoperative ctDNA sample to assess the correlation of ctDNA and surgery radicality was available for 39 patients undergoing 50 surgeries (28 R0, 7 R1 and 15 R2) (Table 3; for detailed information see Supplementary Table 1). Among the 28 cases of R0 resection,postoperative ctDNA tested negative in 26 cases (26/28, 93%). After the first of the two remaining R0 surgeries, a RFA of a small metastasis in the liver, the patient continued displaying ctDNA and, subsequently, was diagnosed with disease recurrence within the scar 6 mo after the surgery. The second case of ctDNA positivity after R0 surgery was a right-sided hemicolectomy with metastasectomy. Also, in this case, the recurrence (two new liver metastases) was visibleviaimaging methods 6 months after the surgery.
In 7 cases with R1 resection, postoperative ctDNA was positive 4 times (4/7, 57%)with disease recurrence 3, 3, 4 and 7 mo after surgery in these cases. For the remaining 3 patients with negative ctDNA after R1 surgery (3/7, 43%), two of them had postoperative recurrence after 7 or 22 mo, and the third one has gone 5 months with no recurrence after surgery. Postoperative ctDNA was positive in all 15 patients with R2 resection (15/15, 100%).
Postoperative tumor recurrence was evaluated according to positive results of ctDNA testing, imaging methods and tumor marker assessments. In our set of 32patients undergoing R0 resections of liver metastases and long-term postoperative monitoring, 22 patients had recurrences (22/32, 69%, see Supplementary Table 1). In 17 patients, from whom all parameters for the detection of postoperative tumor recurrence were available, a total of 22 recurrences were confirmed (3 patients had repeated recurrences - 2 and 4 recurrences). Thirteen times (13/22, 59%) the recurrence was simultaneously detected by ctDNA, imaging methods and tumor markers. Seven times (7/22, 32%) the tumor markers were negative and 6 times (6/22,27%) the imaging methods were without evidence of tumor. The ctDNA was not negative even once (0/22, 0%), making ctDNA in our study the most sensitive tool for detecting tumor recurrence of all three methods. In four patients (4/22, 18%) the tumor recurrence was detected by ctDNA only, while imaging methods and tumor markers were negative (Table 4).
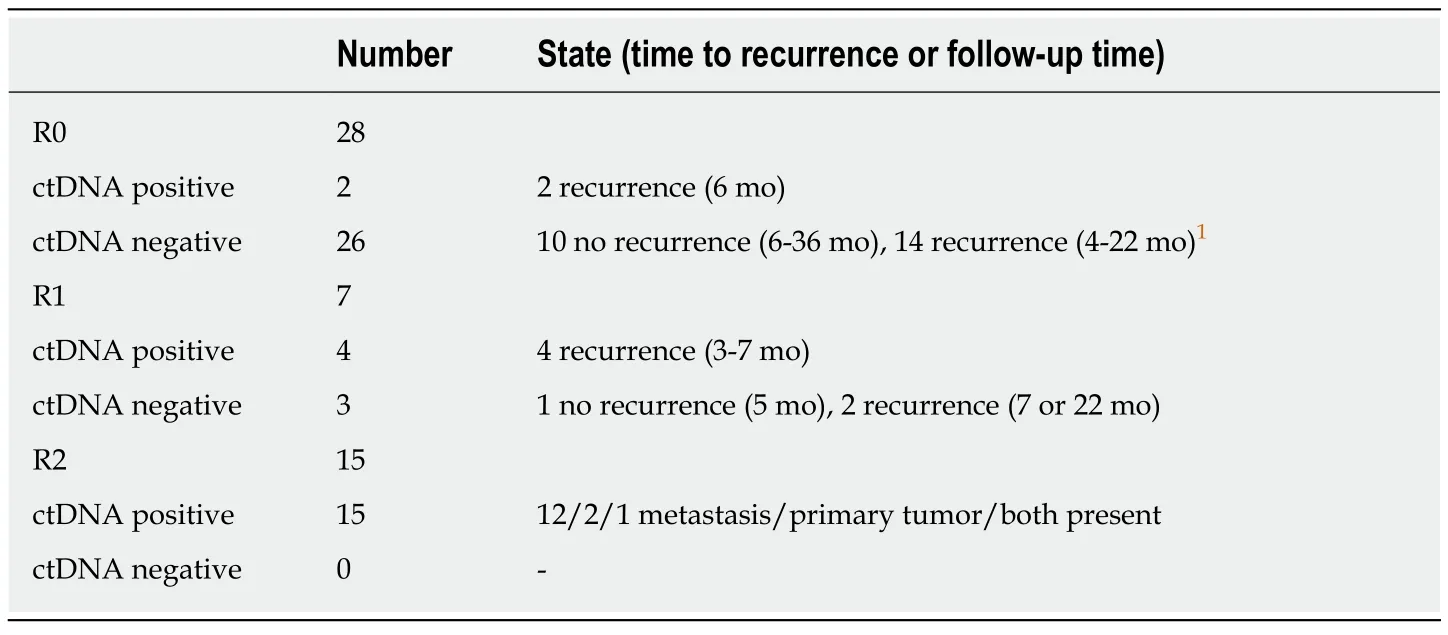
Table 3 Correlation of surgical radicality and postoperative circulating tumor DNA
DISCUSSION
Radicality of surgery is normally assessed based on histological examination of a resected sample and based on the results of imaging methods. However, these examinations cannot indicate any potential presence of circulating tumor cells found in the bloodstream or lymphatic pathways due to a metastatic process or dissemination during surgery. Potential presence of microscopic metastases cannot be demonstrated using histology or imaging methods either. Although the follow-up of tumor marker levels may be useful for detection, their sensitivity and specificity are low[20]. ctDNA is a highly dynamic marker with an approximate half-life of 2 hours,and its levels correspond to the clinical condition of patients with mCRC[17,21]. As we have shown in this paper, a postoperative presence of ctDNA correlates very well with surgery radicality, and its elevated levels in R0 and R1 resections may signal the occurrence of micrometastases and thus help to identify patients with an increased risk of early recurrence for a higher frequency of their follow-up assessments or for an indication of adjuvant therapy[22-24].
To date, only three papers have been published studying the presence of ctDNA immediately after CRC resection. One study in 2005 focused onKRASmutation persistence in the plasma of patients with colorectal cancer in various stages 3 days from radical surgery. As surprisingly indicated by the results, most patients with preoperatively detectedKRASmutations in plasma had the same mutations detected in plasma, also 3 days from radical surgery (7/9, 78%). Only two patients had no mutation detected in the postoperative period (2/9, 22%)[25]. As mentioned in another study, ctDNA can provide information on radicality of primary resection of colorectal cancer, which was illustrated in the case of a patient where evidence of insufficient radicality of the primary surgery was provided based on the presence of postoperative ctDNA[26]. The last study from 2016 showed a correlation between R0 resections and postoperative ctDNA negativity in 75% of patients (6/8) and a correlation between R2 resection and postoperative ctDNA positivity in 67% of patients (2/3), by presenting a set of 11 patients with preoperatively positive ctDNA results, undergoing R0 (8 times) or R2 (3 times) resection[27].
Compared to the above mentioned studies, our study presents the largest group of patients so far with preoperatively detected ctDNA (47 in total) in whom postoperative ctDNA correlation with surgery radicality was followed, and this studyis also the first to report ctDNA correlation with R1 resection. In our group of patients who underwent R1 resections, more than half of them were postoperative ctDNA positive. Considering that in these patients, only a small number of tumor cells were present in the resection margin that they are unlikely to release their DNA into the bloodstream, ctDNA positivity could indicate that there are still other micrometastases not detected by imaging methods. This corresponds to significantly shorter times without recurrence (3, 3, 4 and 7 mo) compared to patients with negative postoperative ctDNA (7 and 22 mo). The presence of micrometastases was also probably recognized in two postoperative ctDNA-positive patients undergoing R0 resection, as their time to recurrence was also very short (6 mo both) when compared to patients with negative R0 postoperative ctDNA (14 times recurrence after 4-22 mo, 10 times no recurrence in surveillance 6-36 mo). Unlike other studies,postoperative ctDNA positivity was captured in all R2 resections (15/15, 100%) in our study, which may be due to the sensitivity of the used detection methods. Our DCE method provides the limit of detection (LOD) of 0.03%-1% (see Table 1), while the studies referred to above used the Temperature Gradient Gel Electrophoresis method with LOD 1%-5%[28]and the Quantitative Polymerase Chain Reaction assay based on allele-specific PCR with LOD 1%-2%[29].

Table 4 Comparison of circulating tumor DNA and standard detection methods
Liver metastatic recurrence occurs in approximately 50% of patients undergoing hepatectomy, while 12% have a recurrence more than once. Considering that repeated hepatectomy combined with systemic therapy may improve overall survival of these patients[30-32], efficient follow-ups for the early detection of recurrence is very important[33].
Tumor markers are commonly used for follow-ups, but so far cannot be used alone to diagnose recurrence, and imaging methods sometimes do not recognize small foci(micrometastases) or, on the contrary, find abnormalities that are not cancer.Examination of ctDNA could be another tool used during follow-up. Our detection method enables high reliability testing (the false positive probability of ctDNA is 0%).In our 22 cases of postoperative tumor recurrence imaging methods and tumor marker results detected a recurrence in 16/22 (73%) and 15/22 (68%) cases,respectively, ctDNA was present in 22/22 (100%) cases. Our results are consistent with the findings of several similar studies that have been performed on a comparable or smaller number of samples[24,26,34-36]. Therefore, we consider our set of 22 recurrences after curative (R0) surgical treatment recorded in our study as adequate to confirm utility of the ctDNA test as a viable tool for the early detection of mCRC recurrence.
Compared to our overall ctDNA detection rate in patients with advanced CRC at the time of the diagnosis (55%-75%), the detection rate in patients previously tested positive for ctDNA is much higher. This data indicates that although the ctDNA release rate into the bloodstream due to the presence of tumor foci differs in various patients with mCRC, for each given patient this phenomenon is relatively stable; thus if ctDNA is detectable in the body when tumor foci are present, it is highly probable that after their complete removal and subsequent recurrence, ctDNA will be detected again.
Although ctDNA detection cannot replace traditional methods used in the followup scheme, it might be a useful supplementary instrument for both the prediction and earlier detection of recurrences, particularly in patients with a higher risk of liver metastatic recurrence[37], and thus it may actually improve the overall survival odds of such patients.
ARTICLE HIGHLIGHTS

extrahepatic metastases at the time of diagnosis, or will develop metachronous metastases within several years after surgery. It is known that radical surgical resection, the R0 resection which involves a complete removal of the diseased tissue, is the only effective treatment option, ideally in combination with perioperative chemotherapy. Besides removal of colorectal cancer metastases, postoperative patient follow-up is no less important as it allows for the timely identification of any progression or recurrence of the disease and prompt therapeutical response.The monitoring of patients is predominantly based on imaging techniques, usually with assessments of serum tumor markers. One of the promising tools for long-term postoperative follow-up is the detection of circulating tumor DNA (ctDNA) in the peripheral blood. Sometimes referred to as a "liquid (re)biopsy" it is a minimally invasive procedure and can be performed repeatedly at relatively short intervals (months or even weeks). The presence of the disease and the actual extent of the tumor burden (tumor mass) within the patient's body can be monitored.This is of particular importance, especially when evaluating radicality of surgical treatment as well as for early detection of disease progression or recurrence.
Research motivation
Radicality of surgery is normally assessed using histological examination of a resected sample and based on the results of imaging methods. However, these examinations cannot indicate any potential presence of circulating tumor cells or microscopic metastases. Also, the main tools used for postoperative patient follow-up, imaging methods and tumor markers, are often not sufficient in early detection of disease progression or recurrence. Tumor markers have low specificity and sensitivity so that they cannot be used alone to diagnose recurrence. Imaging methods are known to fail to detect small foci (micrometastases) or, on the contrary, find abnormalities that are not cancer. Moreover, they cannot be performed frequently due to the radiation exposure. The recently introduced ctDNA testing could present a useful alternative tool. It has proven to be very promising for long-term, postoperative follow-ups of patients with CRC, particularly in advanced stages. Being minimally invasive, it can be repeated frequently for a long time with no significant burden to the patient, and moreover, this test shows high sensitivity and specificity to patients with preoperative ctDNA positivity.
Research objectives
The main objectives of the study were to confirm the radicality of surgery using ctDNA and to compare available methods for detection of recurrence in metastatic CRC (mCRC). It is important to verify whether ctDNA can be used in clinical practice, particularly for the evaluation of the radicality of surgery and for the timely detection of any progression or recurrence of the disease.
Research methods
A total of 47 patients with detected ctDNA and indications for resection of mCRC were enrolled in the multicenter study involving three surgical centers. Standard postoperative follow-ups using imaging techniques and the determination of tumor markers were supplemented by ctDNA sampling. In addition to the baseline ctDNA testing prior to surgery, a postoperative observation was conducted by evaluating ctDNA presence up to a week after surgery and subsequently at approximately three-month intervals. The presence of ctDNA was correlated with radicality of surgical treatment and the actual clinical status of the patient. To test ctDNA,we performed a sensitive, efficient, rapid and affordable method based on the formation of heteroduplexes with subsequent detection using denaturing capillary electrophoresis (DCE).This method can be used to detect a mutated locus in plasma with the sensitivity of 0.03% to 1%depending on the mutation to be determined with input DNA amount of tens of pg. The specificity of this ctDNA test is 100%, which means that the presence of ctDNA always provides evidence that a tumor residue or tumor cells are present. As previously shown by us, ctDNA testing using DCE allows a patient follow-up in real time, while ctDNA levels correlate very well with the current condition of the patient.
Research results
Among the monitored patients, the R0 (curative) resection correlated with postoperative ctDNA negativity in 26 out of 28 cases of surgical procedures (93%). In the remaining cases of R0 surgeries that displayed ctDNA, both patients were diagnosed with a recurrence of the disease after 6 mo. In 7 patients who underwent an R1 resection, 4 ctDNA positivities (57%) were detected after surgery and associated with the confirmation of early disease recurrence (after 3-7 mo). All 15 patients undergoing R2 resection remained constantly ctDNA positive during the entire follow-up period. In 22 cases of recurrence, ctDNA positivity was detected 22 times (100%)compared to 16 positives (73%) by imaging methods and 15 cases (68%) of elevated tumor markers.
Research conclusions
Although ctDNA detection cannot replace traditional methods used in the follow-up scheme, it might represent a useful supplementary instrument for both the prediction and earlier detection of recurrences, particularly in patients with a higher risk of liver metastatic recurrence, and thus it may actually improve the overall survival odds of such patients. And it has also been shown that the ctDNA test is a highly specific and sensitive tool for confirming the radicality of surgical treatment and for the potential prediction of early disease recurrence after R0/R1 surgeries.
Research perspectives
In this study, the high sensitivity of the methodology used to test ctDNA after curative mCRC surgical treatment and also to detect recurrence of the disease was shown. However, to confirm this hypothesis, testing on a larger sample set is required. In particular, it is desirable to obtain a greater number of ctDNA positive and negative results after R1 resections that could be correlated with time to disease recurrence. Similarly, expanding the set of long-term follow-up patients using standard approaches supplemented with ctDNA sampling is warranted.
杂志排行

World Journal of Gastroenterology的其它文章
- Wrap choice during fundoplication
- Pulmonary tumor thrombotic microangiopathy of hepatocellular carcinoma: A case report and review of literature
- Hepatitis C virus eradication with directly acting antivirals improves health-related quality of life and psychological symptoms
- Operative complications and economic outcomes of cholecystectomy for acute cholecystitis
- Diagnostic and prognostic value of lncRNA cancer susceptibility candidate 9 in hepatocellular carcinoma
- Comprehensive multi-omics analysis identified core molecular processes in esophageal cancer and revealed GNGT2 as a potential prognostic marker