Diagnosis of Toxoplasma gondii infection in pregnant women using automated chemiluminescence and quantitative real time PCR
2019-01-30EhsanAhmadpourElmiraZargamiMahmoudMahamiOskoueiAdelSpotinAbbasShahbaziHosseinSamadiKafilSabaRajabiPariaAlizadehYagoobAzadiRezaBahajFirouzShahrivarAleksandraBarac
Ehsan Ahmadpour, Elmira Zargami, Mahmoud Mahami-Oskouei, Adel Spotin, Abbas Shahbazi, Hossein Samadi Kafil, Saba Rajabi, Paria Alizadeh, Yagoob Azadi, Reza Bahaj,Firouz Shahrivar, Aleksandra Barac
1Infectious and Tropical Disease Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
2Students Research Committee, Tabriz University of Medical Sciences, Tabriz, Iran
3Department of Parasitology and Mycology, Faculty of Medicine, Tabriz University of Medical Sciences, Tabriz, Iran
4Drug Applied Research Center, Tabriz University of Medical Sciences, Tabriz, Iran
5Clinic for Infectious and Tropical Diseases, Clinical Centre of Serbia, Faculty of Medicine, University of Belgrade, Serbia
Keywords:Toxoplasmosis Toxoplasma gondii Chemiluminescence immunoassay Real time PCR Pregnancy
ABSTRACT Objective: To identify serodiagnosis and quantification of Toxoplasma gondii (T. gondii)infection among pregnant women in Salmas, northwest of Iran. Methods: In this crosssectional study, 276 blood samples were collected from pregnant women referred to the health care centers in Salmas city. The demographic variables were also recorded. Titers of anti-Toxoplasma IgM and IgG antibodies (Ab) were determined using the chemiluminescence immunoassay. Quantitative real-time PCR targeting the T. gondii repeated element gene was also performed on the blood sample. Results: Out of all, 19.92% (55/276) and 2.17% (6/276)patients were seropositive for anti-Toxoplasma IgG and IgM Ab, respectively. Moreover, the presence of T. gondii DNA was observed in 12.31% (34/276) blood samples. A signi ficant relationship was observed between the IgG Ab seropositivity and contact with the cat asa risk factor (P=0.022). Conclusions: The seroprevalence rate of T. gondii infection in pregnant women is relatively low. Consequently, the seronegative pregnant women are at risk, anda considerable rate of positive blood samples for the presence of parasite′s DNA should not be ignored. Besides, quantitative real-time PCR could be considered as an accurate method for diagnosis of acute toxoplasmosis especially when the precise results are of the most importance in pregnancy. Limiting contact with cats is also suggested for pregnant women.
1. Introduction
Toxoplasma gondii(T. gondii), an obligate intracellular parasite, infects almost all warm blooded animals and is of great importance when cause infections in humans. Toxoplasmosis is highly prevalent infection throughout the world andT. gondiiinfection is considered as a serious public health problem, with more than 30% of the human populations infected[1,2]. The parasite can infect humans by ingesting undercooked or raw meat containing tissue cysts of the parasite. Furthermore, it can be also transmitted by eating fruits, vegetables and other food sources contaminated by the parasite′s oocysts. The soil is also reported to be a potential source of human infections[2,3].
T. gondiiinfection is mostly mild and asymptomatic,however, it can cause severe complications to the fetus or immunocompromised humans.T. gondiican transmit the infection during pregnancy to the fetus through placenta and cause congenital toxoplasmosis[2,4]. Therefore, pregnant women,as well as children with congenital infection, are important risk groups. In seronegative pregnant women, acquired primaryT.gondiiinfection may affect pregnancy and leads to miscarriage or fetal disorders[5,6]. Acute toxoplasmosis in pregnant women like other healthy non-pregnant individuals is usually asymptomatic.One of the most seen clinical manifestations of acute infection is regional lymphadenopathy[2]. Chronic maternal infection usually does not affect the fetus. Although pregnant women withT. gondiiinfection generally have no symptoms, the acute infection during pregnancy can lead to potentially tragic outcomes for the fetus and newborn[2,6].
Fetus or neonate with congenital toxoplasmosis may suffer from visual defects, hearing loss, neurological complications,hematological disorders, seizures, and/or death. Encephalitis,hydrocephalus, hepatitis, microcephalus, lymphadenopathy and death are the other consequences of the congenital toxoplasmosis[7]. Generally the clinical manifestations in infected fetus depend on the maternal immune response, the parasite virulence, and the trimester of pregnancy. Hence, rapid diagnosis and treatment are essential for reducing the severity of the fetal disease[7,8].
Toxoplasmascreening test for pregnant women is part of the TORCH panel (T. gondii, rubella, cytomegalovirus and herpes infections)[9]. The diagnosis of toxoplasmosis is complicated and challenging. Diagnosis of the infection is mostly based on the serological tests, determining concentrations of anti-ToxoplasmaIgM and IgG antibodies (Ab) in the patients′ sera. These antibodies can last for months or even years after acute infection, thus these methods cannot differentiate recent infection from past infection.In fact, the use of molecular techniques, that are sensitive and rapid, is crucial for the early diagnosis of congenital toxoplasmosis and active toxoplasmosis in pregnancy[4,8]. Therefore, the aim of the present study was to identify serodiagnosis, and quanti fication ofT. gondiiinfection among pregnant women referred to the health care centers in Salmas city, northwest of Iran, in 2016.
2. Materials and methods
2.1. Sample collection
In this cross sectional study, 276 blood samples were collected from pregnant women referred to the health care centers in Salmas city, North West of Iran, from the 1st May 2016 to the 1st December 2016 (Figure 1). The study was approved by the Ethical Committee of Tabriz University of Medical Science (No. 94/2-5/17). All pregnant women signed informed consent for enrollment to the study. Demographic variables were collecting by interview:previous contact with cats; clinical symptoms; educational status;occupation; age; history of consuming raw and undercooked meat,unpasteurized milk or raw vegetable.
The taken blood samples were divided into two groups, one for serum isolation which was left sedentary to clot, and the other in sodium-heparin tubes for buffy coat isolation. Serum samples were isolated after centrifugation of the clotted blood at roughly 2 500 rpm for 10 min. The isolated sera were kept frozen at -20 ℃ until being examined. The buffy coat was also isolated by spinning the blood sample containing anti-coagulant at 1 500 rpm for 10 min and stored in 70% ethanol at -20 ℃ for DNA extraction.
Figure 1. Geographical position of Salmas district, northwest of Iran.
2.2. Determination of anti-Toxoplasma IgM and IgG antibodies
Anti-ToxoplasmaAbs were determined by Ab capture chemiluminescence immunoassay (CLIA) using anti-ToxoplasmaIgG and IgM Abs CLIA kits (LIAISON® Toxo IgM and IgG,DiaSorin S.P.A, Italy) applied in LIAISON device (DiaSorin,Germany). The tests were performed by the device automatically according to the manufacturer′s setting. Samples with IgM Ab titer<6 IU/mL were regarded as negative, 6 to 8 IU/mL as borderline and ≥8 IU/mL as positive results. Furthermore, samples with IgG Ab titer <7.2 IU/mL were graded as negative, 7.2 to 8.8 IU/mL as equivocal and ≥8.8 IU/mL as positive results[8]. All borderline results were twice repeated.
2.3. DNA extraction
The buffy coats were washed twice with phosphate-buffered saline to remove the ethanol, and DNA was extracted using blood genomic DNA extraction mini kit (YTA co., Iran). The extracted DNA samples were kept frozen at -20 ℃ for further use.
2.4. Quantitative-PCR
Quantitative PCR reactions (Q-PCR) were performed as previously described[10,11] in 20 µL of reaction volume with SYBR Green qPCR Master Mix 10 µL (YTA co, Iran) mixed with 1.4 µL template DNA, 7 µL distilled water and 0.8 µL of each primer at a concentration of 1 pmol/µL. The following primers were used for ampli fication of 164-bp fragment of repeated element (RE) gene fromT. gondii; F 5′-AGG GAC AGA AGT CGA AGG GG-3′ and R 5′-GCA GCC AAG CCG GAA ACA TC-3′. The amplification protocol was: 10 min at 95 ℃℃, 40 cycles at 94 ℃ for 30 s(denaturation), 55 ℃ for 30 s (annealing), and 72 ℃℃ for 30 s(ampli fication). Ampli fication was done by magnetic induction cycler real time PCR machine (Bimolecular system, Australia).Tubes and plastic materials were used as provided by Bimolecular system for magnetic induction cycler machine. All experiments were done in triplicate. Melting curve analysis was performed to verify the correct product size and to ensure the absence of side products or primer dimmers. Also, Toxoplasma DNA extracted from tachyzoites (RH strain) and water were used as the template for positive and negative control, respectively. In order to evaluate the number of parasites in the blood samples, Q-PCR threshold cycle value was used according to standard curve obtained with DNA samples from a range of serial dilutions (1××107-1××101parasite/mL) of RH strain tachyzoites.
2.5. Data analysis
Data was recorded and analyzed with the SPSS v.18 software(SPSS Inc., Chicago, ILL, USA) using Mann-Whitney andChisquare tests. The P value <0.05 was considered as signi ficant.
3. Results
In total, 276 pregnant women, with the mean age±standard deviation of (33.1±7.5) years were enrolled in the study and screened forToxoplasmainfection. Out of all, 19.92% (55/276) and 2.17% (6/276) pregnant women were positive for anti-ToxoplasmaIgG and IgM Abs, respectively. Also, 5/276 (1.81%) pregnant women were positive for both IgM/IgG Abs. Detailed information is summarized in Table 1.
Moreover, molecular analysis was performed using Q-PCR on the seropositive pregnant women (either IgG or Ig M positive) (n=56)for confirmation of theirToxoplasmainfection status.T. gondiiDNA was found in 34/276 (12.3%) blood samples. All of the six women with positive IgM Ab had parasite′s DNA in their blood,detected by Q-PCR (P<0.001) (Table 1). Interestingly, 58.18%(32/55) of patients with positive anti-ToxoplasmaIgG Ab had also positive result forT. gondiiobtained by Q-PCR (P<0.001) (Table 2). The IgM positive (6/34) and IgG (32/34) positive individuals harbored an average (2 454.0±918.5) and (1 014.0±255.3)parasite/mL (Mean±SEM) , respectively. Although, IgM-positive individuals showed greater parasite loads; however, there was no statistically signi ficant difference in parasite load between IgM-positive and IgG-positive women (P>0.05).
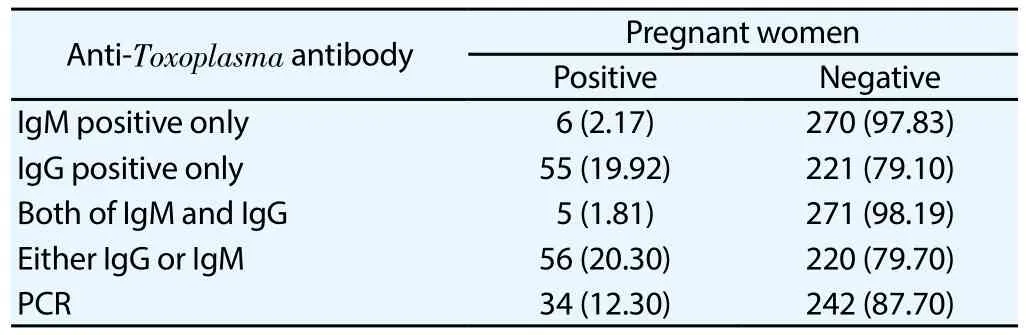
Table 1 Results of anti-Toxoplasma IgM and IgG antibodies in 276 studied pregnant women [n (%)].
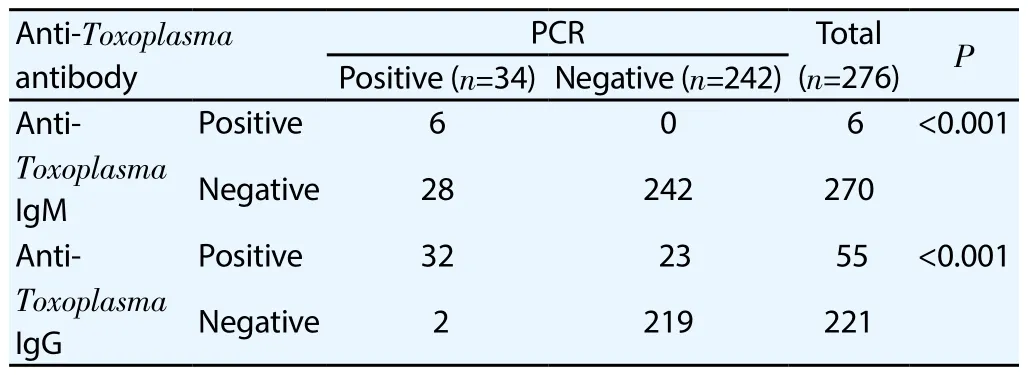
Table 2 Relationship between ELISA results and RT-PCR for Toxoplasma in 276 pregnant women.
Using the Kolmogorov-Smirnov test, none of the quantitative variables had abnormal distribution, thus for analysis of these variables, non-parametric Mann-Whitney test was used. The IgG and IgM Ab concentrations and age of the studied women were statistically signi ficantly higher in women with positive results ofT. gondiiby Q-PCR (Table 3).
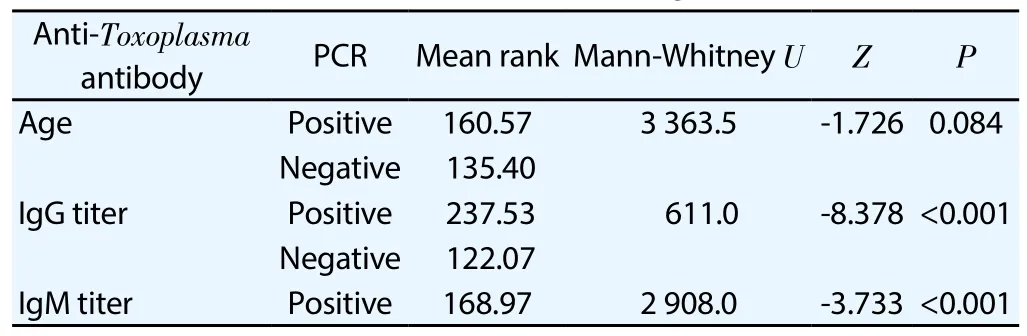
Table 3 Relationship ofmean age of studied pregnant women, anti-Toxoplasma IgM and IgG Abs titer and results of RT-PCR test for T. gondii.
Considering the demographic variables, the frequency of IgG Ab seropositivity was signi ficantly higher among the women being in contact or having a cat as a pet (P=0.022). Furthermore, all thesix IgM Ab positive individuals were housewives (P=0.031). No statistically signi ficant relationship was observed considering PCR result, IgG and IgM Ab seropositivity among the other studied demographic variables (Table 4).
4. Discussion
Toxoplasmosis is the ubiquitous parasitic infection. The importance of acquired toxoplasmosis is mainly in pregnancy,with the risk of severe congenital infection. Chronic maternal infection usually does not affect the fetus, however, the acute toxoplasmosis during pregnancy can lead to serious complications in fetus[5,6]. The current study investigated the prevalence ofT.gondiiinfection among pregnant women referred to the health care center in Salmas city, northwest of Iran using serological and molecular methods. The results showed that 19.92% and 2.17% of the studied pregnant women were seropositive for anti-ToxoplasmaIgG and IgM Abs, respectively. Remarkably,ToxoplasmaDNA was detected in 58.18% seropositive pregnant women.
There are many studies on theT. gondiiprevalence in the world[6,12]. The overall seroprevalence rate ofT. gondiiinfection among the Iranian general population is estimated 39.3%[1]. In meta-analysis by Mizaniet al., the seroprevalence ofT. gondiiAbs using the random-effect model in the pregnant women and girls were 43% (95%CI=38%-48%) and 33% (95%CI=23%-43%),respectively[5].
Salmas is located in the northwest Iran. In the literature, the seroprevalence ofT. gondiiinfection was reported as 47.00% and 45.12% in other parts of West Azerbaijan, Iran[13,14]. In the studies reported from neighboring province, East Azerbaijan, the IgG Ab seropositivity was from 35.1% to 38.66%[15,16]. In Turkey, a neighboring country of Iran, theT. gondiiAbsseroprevalence of in women of reproductive age was determined to be 58.3% for IgM Ab and 1% for IgG Ab[17]. The present study shows the low prevalence ofT. gondiiinfection in pregnant women in Salmas compared to the other nearby cities.
The diagnosis ofT. gondiiinfection is based on serological methods for demonstration of specific IgG, IgM, and IgA Abs[8,18]. There are several serology techniques that could be used. The enzyme-linked immunosorbent assay and indirect immunofluorescence assay are the most common methods in Iran, and recently the CLIA method has been used[15]. In the present study, screening of anti-ToxoplasmaIgG and IgM Abs in the pregnant women was done by CLIA. This method is more sensitive, automated, reliable, and convenient technique. However,the seropositivity for anti-ToxoplasmaAbs is one of the most challenging situations in pregnant women[18].
Determination of active and acute toxoplasmosis in pregnant women and commencement of a sufficient anti-Toxoplasmatreatment, if needed, can prevent the congenital toxoplasmosis and improve the prognosis. Molecular techniques, as alternative tools, have been used for detection ofT. gondiiDNA in clinical samples[4,19,20]. Currently, Q-PCR has been used for detection and quanti fication ofT. gondiiDNA in different clinical samples. The variation of the test performance is mostly associated with target genes and primer composition. Most investigators have used the B1 or RE gene for detection[21-23].
Hence, in the present study Q-PCR molecular technique was performed based on the RE gene ofT. gondiifor con firmation of active and acute toxoplasmosis. Using Q-PCR, the presence ofT.gondii DNA was detected in 12.30% of patients′ blood samples.All individuals with positive anti-ToxoplasmaIgM Ab had also parasite′s DNA in their peripheral blood. Interestingly, 58.18% of anti-ToxoplasmaIgG Ab positive women had also positive results by PCR. Based on these results, Q-PCR technique could be used as a relevant con firmatory test in diagnosis of acute toxoplasmosis.Although laboratory diagnosis of toxoplasmosis is performed using serology, molecular method such as real time PCR is also important in con firmation. As a limitation in this study, the PCR was not performed on seronegative samples due to lack of funding.Hence, in future studies it is better to survey all samples using molecular method. Salehiet al.showed that 33.3% of the pregnant women were seropositive forT. gondiiinfection in Arak, Iran.They also found parasite′s DNA in one cord blood sample after delivery, con firming congenital infection[24]. Our results showed that the parasite′s DNA could be found in more than 50% of theT. gondiiseropositive pregnant women. Furthermore, the high prevalence and parasite load are indicative as important markers for screening before and during pregnancy. Type Ⅱ strains are the most prevalent cause of human toxoplasmosis in North America and Europe. Conversely, the majority of strains isolated in Spain were typeⅠ[25,26]. Fuenteset al.determined the types ofT. gondiiand its association with human toxoplasmosis using genetic analysis of the SAG2 locus[26].They showed that typeⅠstrains were more commonly (75%) found in cases with congenital infection. TypeⅠstrains are considered as the most virulent, fast growing and usually causing high level of parasitemia. ThereforeT. gondiiinfection of pregnant women with genotypeⅠcan lead to severe fetal abnormalities or abortion.
Further the association betweenT. gondiiinfection and potential risk factors were analyzed. Among the pregnant women who participated in the study, there were no signi ficant differences considering age (P=0.084). On the other side, previous contact with cats has been shown as statistically significant risk factor for toxoplasmosis (P=0.022). These results are in agreement with previous meta-analysis data[1,5]. Surprisingly, all IgM Ab positive pregnant women were housewives (P=0.031). Our results indicate that housewives had higher risks for exposure to this parasite.Although the frequency of IgG Ab seropositivity was higher in housewives than employed women, there was no statistically signi ficant difference between occupational groups.
In conclusion, the results of the present study show that,pregnant women in Salmas city have a low anti-Toxoplasma Abs seroprevalence compared to most parts of Iran. The seronegative pregnant women are considered susceptible toT. gondiiinfection and women of childbearing age are at the higher risk. Therefore,pregnant women require regular checks for seroconversion. On the other hand, considerable rate of positive blood samples for the presence of parasite′s DNA should be considered. Based on the present findings, Q-PCR is an accurate method and it could be used for fast and precise diagnosis/con firmation of acute and active toxoplasmosis. Furthermore, de fining of the population structure at risk forT. gondiiinfections could lead to more effective prevention strategies. Finally, limitation of the contacts with the cats is also highly suggestive to pregnant women.
Conflict of interest statement
Authors declare there is no any con flict of interest. The sponsor or funding organization had no role in the design or conduct of this research.
Foundation project
This study was prepared from Elmira Zarghami′s MSc thesis and supported by Infectious and Tropical Disease Research Center,Tabriz University of Medical Sciences, Tabriz, Iran (Grant No.94/2-5/17).
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Resistance status of main malaria vector, Anopheles stephensi Liston(Diptera: Culicidae) to insecticides in a malaria Endemic Area, Southern Iran
- Frequency of typhoon occurrence accounts for the Poisson distribution of human leptospirosis cases across the different geographic regions in the Philippines
- Cytotoxic, antioxidant and antimicrobial activities of Nerium oleander collected in Morocco
- Surveillance of Chikungunya virus activity in some North-eastern states of India
- Potentiating activity of rhein in targeting of resistance genes in methicillin-resistant Staphylococcus aureus
- Antibiotic resistance of Neisseria species in Iran: A systematic review and meta-analysis