Surveillance of Chikungunya virus activity in some North-eastern states of India
2019-01-30PrafullaDuttaSirajKhanAnilPhukanSaratHazarikaNabaHazarikaSumiChetryAbdulKhanHarpreetKaur
Prafulla Dutta, Siraj A. Khan, Anil C. Phukan, Sarat Hazarika, Naba K. Hazarika, Sumi Chetry, Abdul M. Khan, Harpreet Kaur
1ICMR-Regional Medical Research Center, NE Region, Dibrugarh, Assam, India
2North Eastern Indira Gandhi Regional Institute of Health & Medical Sciences, Shillong, Meghalaya, India
3Jorhat Medical College & Hospital, Jorhat, Assam, India
4Gauhati Medical College & Hospital, Guwahati, Assam, India
5Indian Council of Medical Research, New Delhi, India
Keywords:Chikungunya Northeast India Aedes aegypti Aedes albopictus
ABSTRACT Objective: To detect the prevalence pattern of Chikungunya virus in three states of Northeast India. Methods: A total of 1 510 samples were collected from different private and government hospitals of Assam, Arunachal Pradesh and Meghalaya. Serum was tested for the presence of IgM antibodies against Chikungunya virus followed by RT-PCR for ampli fication of Chikungunya E1 gene region using speci fic primers. Results: Overall, 11.83% (172/1 454)clinical samples were positive by MAC-ELISA and/or RT-PCR assay. Asymptomatic infection was seen in 17.86%. Males were more affected than females and age group 16-30 years was mostly affected. Fever (100.00%) was the primary symptom followed by headache (72.03%)and arthralgia (41.53%). Only 118 Chikungunya positive cases could be traced, of which 25.42% complained about sequelae of infection. In entomological investigation, Aedes aegypti was more predominant (92.10%) than Aedes albopictus (7.90%). No mosquito pools could be incriminated for Chikungunya virus. Conclusions: In this study, Chikungunya was observed to be prevalent in Assam, Arunachal Pradesh and Meghalaya. Though Chikungunya is a selflimiting infection, increasing morbidity by CHIKV infection is affecting social and economic status of individual. Thus, a community empowerment to effectively control mosquito population by employing different mosquito control measures along with personal protection is mandatory to tackle future outbreak of the disease.
1. Introduction
Chikungunya virus (CHIKV) is an alphavirus belonging to the family Togaviridae. Alphaviruses are small spherical enveloped viruses of 60-70 nm in diameter. The genome is a single-stranded RNA molecule of positive polarity[1], having two large open reading frames (ORF). The first ORF encodes four non structural proteins(nsP1, nsP2, nsP3 and nsP4) and ORF2 encodes structural proteins that include one capsid protein (C), two major envelope surface glycoproteins (E1, E2) and two small proteins (E3, 6K)[2,3]. The surface glycoprotein mediates attachment, fusion, and penetration[4].
This arbovirus is transmitted byAedesspecies mosquito vectors mainlyAedes aegypti(Ae. aegypti) andAedes albopictus(Ae.albopictus)[5].
CHIKV was first isolated in 1952 in Tanganyika (present day Tanzania); however, the first description of the disease might have been given by David Bylon in 1779 during an epidemic in Jakarta[6].In India, this virus was isolated for the first time in Calcutta in 1963[7].
Chikungunya infection produces a self-limiting illness in humans that is often characterized by sudden onset of fever, headache,fatigue, nausea, vomiting, rash, myalgia, and severe and very painful polyarthralgia, which lasts for one to ten days. However, arthralgia may persist for months to years[8,9]. During early phase of the infection, the symptoms are often clinically indistinguishable from those observed in dengue fever[10]. Also, simultaneous isolation of both dengue and Chikungunya from the sera of the same patients indicating the presence of dual infections has been reported earlier[11]. CHIKV transmission from mother to child also has been observed[12].
Chikungunya was first reported in 2008 from Assam, a state in Northeast region of India[13]. Subsequently, another state Meghalaya has been affected by this disease in 2010[14] and is still a major health problem in the particular area. Dengue outbreak is also a major problem in this part of the country. Abundant presence of the vector mosquito in this part of the country[15] carries risk of CHIKV circulation and spread to newer areas. This present study was conducted to detect the prevalence pattern of the virus in different states of Northeast India.
2. Material and methods
2.1. Ethics
The study was approved by Institutional Ethics Committee, Indian Council of Medical Research (ICMR)-Regional Medical Research Centre, NE Region, Dibrugarh, India [No. RMRC/Dib./IEC(Human)/2013-14/61 dated 11.04.2014]. This committee follows the ethical guidelines developed by ICMR, New Delhi for biomedical research on human participants, 2006. The guidelines were developed according to the Guidelines of Council for International Organisations of Medical Sciences developed in 1964 at Helsinki and follow the Helsinki Declaration published in 2004. Informed consent was taken from the study participants at the time of sample collection.
2.2. Study area
This study was conducted from December, 2014 to November, 2017 in three states of Northeast Indiaviz., Assam (26.14°N 91.77°E),Arunachal Pradesh (27.06°N 93.37°E) and Meghalaya (25.57°N 91.88°E). Samples were collected from different districts of Assam;in Meghalaya, the Chikungunya cases were mainly concentrated in Tura area of West Garo Hills from where outbreaks were reported in earlier years; and in Arunachal Pradesh, samples collected during a Dengue outbreak in Pasighat in 2014-2015 were included in the study. Vector collection was followed in the vicinity of the positive cases.
2.3. Study population
Study population included patients with suspected dengue and/or Chikungunya cases, acute encephalitis syndrome (AES) cases and pyrexia of unknown origin (PUO) cases negative for the most common etiologies. According to WHO, characteristic symptoms of Chikungunya infection are abrupt onset of fever often accompanied by joint pain, muscle pain, headache, nausea, fatigue and rash,and the joint pain may be long-lasting. Sometimes, the infection may be asymptomatic or very mild and hence go unrecognized,and sometimes it could be misdiagnosed with dengue in dengue endemic areas. Due to these reasons, dengue suspected but negative cases, PUO and healthy cases were included in the study. AES is characterized with acute onset of fever and a change in mental status and/or new onset of seizures. It has a varied range of causative agentsviz. viruses, bacteria, fungi, spirochetes, parasites, chemicals and toxins[16]. Japanese encephalitis virus is the primary cause of AES in Assam and other etiologies like Scrub typhus[17] and leptospirosis[18]were also reported from here. To observe whether Chikungunya also contributing in AES cases of this region, the AES samples negative for the most common etiologies in this region were also included.
2.4. Sample collection
2.4.1. Human blood samples
A total of 1 510 samples were collected during the study period.Out of these samples, 337 samples were obtained from AES patients,994 from dengue/Chikungunya suspected patients, 123 from PUO patients. The remaining 56 samples were collected from apparently healthy individuals living in and around the positive cases and did not suffer from fever in last 6 months and volunteered to provide their blood samples during the follow up visits to the case reporting areas (Table 1).
2.4.2. Mosquito vector collection
Mosquito larvae were collected from the localities from where Chikungunya positive cases were reported in these states. Larvae were collected from different containers like tyre, water tanketc.The container index (CI) of potential vectors was recorded. The emerged mosquitoes were pooled according to the species, gender and location and stored at -80 ℃ for further processing.
2.5. Serological study
Serum from the blood sample was separated and one microlitre of serum was used for the detection of Chikungunya speci fic IgM antibodies using MAC-ELISA kits (National Institute of Virology,Pune, India) following manufacturer′s instructions. The provided test wells were pre-coated with anti-human IgM antibodies. After addition of the serum sample, Chikungunya antigen and secondary anti-Chikungunya monoclonal antibodies were added to the wells followed by Avidin-HRP. Finally chromogenic substrate was added which changes in colour in case of a positive reaction. The reaction is stopped by 1N H2SO4and the intensity of the colour was measured at 450 nm. One positive and one negative control were included for validating the result. For result interpretation, the threshold for positivity was set as per instructions given in the kit. If optical density (OD) value of sample tested is less than OD of Negative control by a factor of 2.0 (Sample OD≤Negative control OD×2.0),the sample is considered as “Negative”. If Samples OD≥Negative control OD×3.0, the sample is considered as “Positive”. Samples with OD value comprised between 2 and 3 times that of the Negative control OD are considered as “Equivocal”.
This study aimed to identify the prevalence of Chikungunya,therefore, detection of IgG antibodies was not included, as past infection would likely alter the true scenario of the infection during the study period.
2.6. Molecular study
A conserved region of the virusi.e.Envelope-1 glycoprotein gene region was targeted for amplification using specific primers[19].Sequencing of the ampli fied product was followed by phylogenetic tree construction (Maximum Likelihood tree based on Kimura-2 parameter model with 1 000 bootstraps) with other Indian and Global CHIKV sequences belonging to the three genotypes, namely Asian,West African and East Central South African (ECSA) genotype using MEGA6. Also another phylogenetic tree using the same parameters was constructed for comparing the study sequences with Indian Ocean Lineage (IOL) strains that caused severe Chikungunya endemics in Indian Ocean islands[20].
2.7. Calculation of container index
The container index (CI) was calculated by using the following formulae:

2.8. Statistical analysis
Information on demography, behavioural practicesetc. were recorded from the study participant to determine the frequency of exposure. Statistical signi ficance of the disease with respect to gender and age was calculated by logistic regression using SPSS version 20.0.P<0.05 was considered as statistically signi ficant.
2.9. Follow up survey
Follow-up of Chikungunya positive patients was done during the period and a detailed questionnaire regarding their social status and behavioural practices were filled up. A second blood sample was collected from a few positive patients after obtaining written consent.All the samples were processed for the detection of Chikungunya IgM antibody. Frequencies of different variables were calculated to observe different behavioural practices of the patients.
3. Results
3.1. Serological and molecular detection of Chikungunya cases
Out of the total 1 454 clinical samples processed for MAC-ELISA,11.21% (163/1 454) was found to be positive for anti-Chikungunya IgM antibodies by MAC-ELISA. Viral RNA was detected in nine samples. One IgM positive sample was also found to be positive for Chikungunya RNA by RT-PCR. Out of the nine RT-PCR positive samples, two were from Pasighat, Arunachal Pradesh and seven were from Guwahati, Assam (only four samples out of these seven samples were quali fied for sequencing). The study locations (district level) in these three states from where we found positive cases are depicted in Figure 1. The year wise and monthly distribution of the positive cases is also shown in Table 2 and Figure 2 respectively.
Apart from the total 1 454 clinical cases, another 56 samples were collected from the apparently healthy volunteers, of which 10(17.86%) were found to be positive by MAC-ELISA suggesting asymptomatic infection. The state wise detail of the collected samples was shown in Table 1.

Table 1 Details of the total chikungunya suspected samples collected during the study.

Table 2 Year wise case distribution of clinical chikungunya cases.

Figure 1. Map depicting Chikungunya cases reporting districts in Assam, Arunachal Pradesh and Meghalaya in Northeast India.
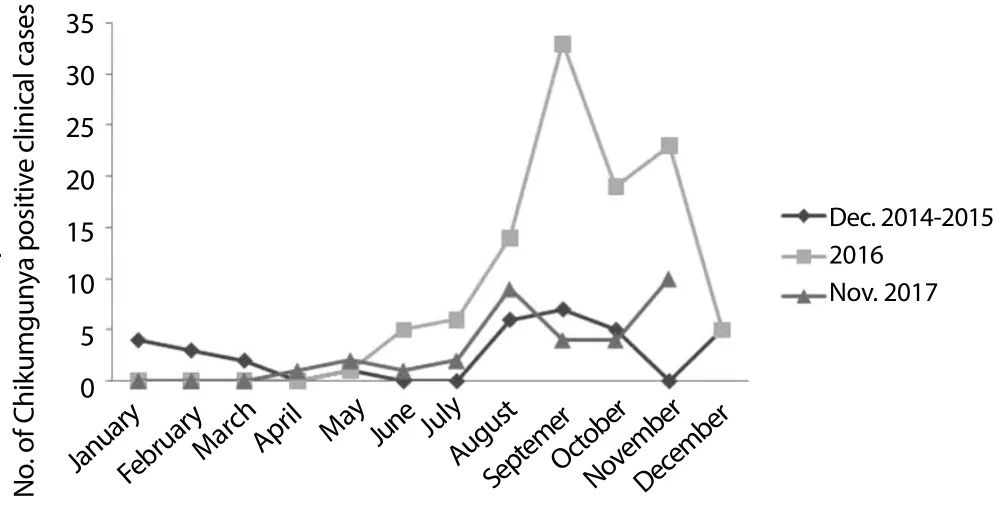
Figure 2. Month wise case distribution of Chikungunya positive clinical cases.
3.2. Phylogenetic analysis
Phylogenetic tree revealed that the samples from Guwahati, Assam and Pasighat, Arunachal Pradesh belonged to the ECSA genotype of the virus (Figure 3A). The second tree (Figure 3B) constructed to compare the same study sequences with IOL strains (IOL is a descendant of ECSA genotype) showed that Chikungunya virus strains of this region did not belong to IOL.
3.3. Demographic characterization of positive cases
Demographic characteristics of the positive patients revealed that 54.07% (93/172) of the cases were male and 45.93% (79/172) were female. Maximum number of cases belongs to the age group of 16-30 years followed by 31-45 years. However, statistical analysis revealed no statistically significant association between these variables and the disease (Table 3).

Table 3 Association of different variables with chikungunya infection.
3.4. Clinical spectrum of the positive cases

Figure 3. Molecular phylogenetic analyses by maximum likelihood method based on the Kimura 2-parameter model.
Out of total 172 Chikungunya positive clinical cases, details of their clinical symptoms were available for 118 cases. Fever (100.00%)was recorded as the primary symptom followed by headache(72.03%) and arthralgia (41.53%). Other symptoms recorded were fatigue (35.6%), myalgia (28.81%), chills (28.81%), vomiting(17%), abdominal pain (16.1%), nausea (5.93%), backache (3.39%),diarrhoea (1.69%), insomnia (0.85%), photophobia (0.85%) and skin rash (0.85%).
3.5. Sequelae status, social status and behavioral characteristics of positive cases
Out of the 172 positive clinical cases, only 118 could be followed up. Out of these 118 cases, 30 (25.42%) complained about sequelae of the disease, like joint pain, fatigueetc. even after one to seven months (Median: 3.5 months) of infection. Only 16 patients agreed to provide a second blood sample during the follow up. When these convalescent sera were processed for detection of IgM antibodies,50.00% (8/16) of them showed IgM antibody positivity even after two to ten months (Median: 6 months) of initial infection.
During follow up, the patients were inquired regarding their social status and daily behavioral practices. Out of the 118 positive cases followed up, 28.80% used mosquito repellent, 44.10% used bednet on a daily basis, 56.00% lived in an urban area, 37.30% lived in cemented homes and 18.60% lived in a mud-plastered home, 39.02%did not have in-house tap facility and 48.80% had stored water in containers due to infrequent water supply.
3.6. Entomological investigation
A total of 1 240Aedesmosquitoes were emerged from the larvae collected from different areas of Assam, Meghalaya and Arunachal Pradesh from where Chikungunya positive cases were reported during the study. Out of these mosquitoes, 1 142 (92.1%) wereAedes aegypti(Male: 503; Female: 639) and 98 (7.9%) wereAe. albopictus(Male: 70; Female: 28). The details of breeding habitat along with CI value is mentioned in Table 4. Overall, a total of 191 pools were prepared; however, none showed any positivity for Chikungunya viral RNA.
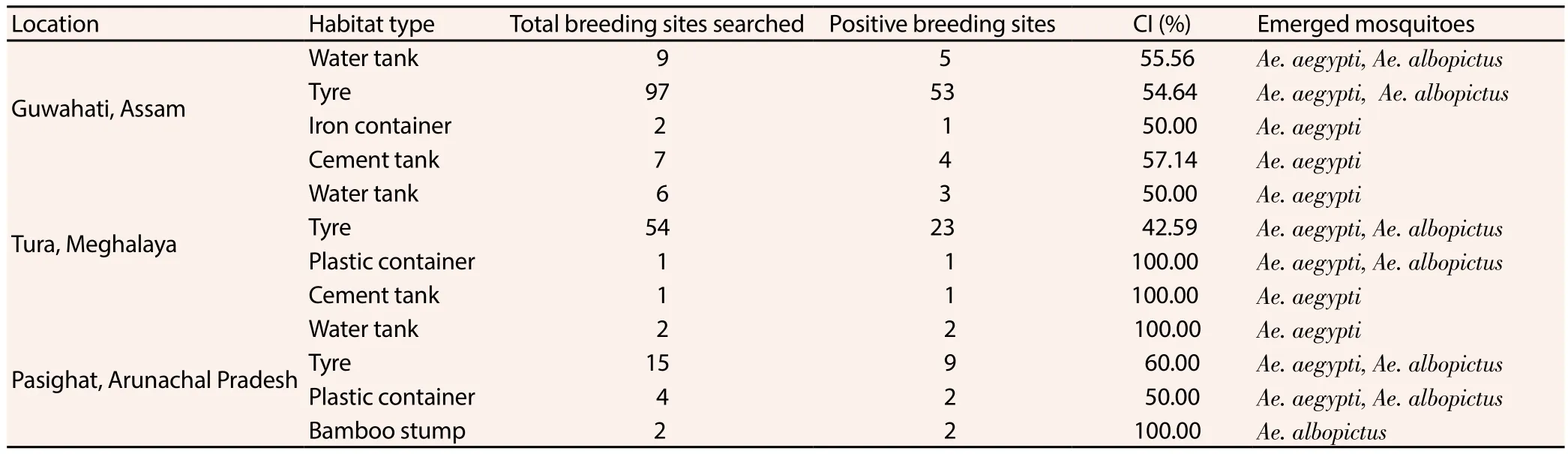
Table 4 Details of Aedes collection with container index values.
4. Discussion
Northeast region of India is affected by different vector borne diseases like Malaria, Japanese encephalitis, dengueetc. Since a decade, Chikungunya has been emerging in this region alongside dengue. Both the diseases have somewhat similar clinical spectrum and same vector mosquitoes. Due to this, Chikungunya is often misdiagnosed. As this region is abundant ofAedesmosquitoes, there is a chance of circulation of Chikungunya since a long time. But due to lack of advance diagnostic tools, diagnosis of Chikungunya was almost lacking. Chikungunya was reported for the first time from Assam and Meghalaya in 2008 and 2010 respectively[13,14].
During this study, prevalence of Chikungunya was found in Assam, Arunachal Pradesh and Meghalaya. Male of age group 16-30 followed by 31-45 were observed to be affected mostly. Others previous studies from different parts of India also reported higher involvement of males than females[21]. Also, persons belonging to above two age groups mostly involve in the outdoor activities and hence are mostly in the risk of mosquito bites. However, no statistical signi ficance was found between the association of gender and age group with the disease.
Phylogenetic study of the CHIKV from Guwahati, Assam and Pasighat, Arunachal Pradesh revealed the presence of East Central South African genotype of the virus in the region. These findings were already reported[22,23]. Though the previous Indian isolates of CHIKV belonged to Asian genotype, the East Central South African genotype is circulating in India after re-emergence of Chikungunya after a gap of 32 years[24]. Also, when we compared the sequences from this study with Indian Ocean Lineage which was responsible for severe outbreaks in Indian Ocean Island[20], we found that the study sequences did not belong to the lineage. Due to lack of previous genetic level data of CHIKV from NE region, we are unable to depict any conclusion regarding similarities or differences with the present one.
In our study, we observed that fever was common in all the cases.Arthralgia, which is a typical Chikungunya symptom, was not present in all the cases. Sequelae of arthralgia persisted in 25.42%,which showed that the disease is not that much severe in this region compared to other studies where large number of patients experienced long term sequlae[25]. Our study is comparable to already published reports which also showed that long term persistence of arthralgia is common phenomenon in case of Chikungunya[26]. The reason of low severity observed in Chikungunya patients of this region could perhaps be attributed to the circulating virus strain.However, detailed analysis of pathogenesis of CHIKV from this region is necessary for confirmation. Also IgM antibodies were observed persisting for long time, which is also comparable to other studies[27].
Only 56 individuals who had not suffered from fever in last 6 months voluntarily provided blood samples for Chikungunya diagnosis. The healthy individuals were concentrated in and around the locality of positive patients and positivity were observed in 17.86% cases. Our study is comparable to a previous seroepidemiological report from India where the researcher found 17.5%asymptomatic infection[28]. Asymptomatic infection in this region suggests that a detailed systematic study for mass Chikungunya surveillance could draw a true picture of the infection burden caused by Chikungunya virus in this part of the country.
These three study states of Northeast India are rich inAedesspecies[15]. During our present study, we collectedAedesspecies from localities of positive patients in whichAe. aegyptiwas predominating in terms of numbers. During this study we were unable to incriminateAedesspecies for CHIKV. Although no mosquito pool was positive for Chikungunya virus, our study reported the prevalence of both the potential vectors in this region.This part of India is considered as biodiversity hotspot and high prevalence of bothAe. aegyptiandAe. albopictusin this region has been reported. Presence of these potential vectors along with actively circulating Chikungunya virus can pose a serious threat of occurring Chikungunya in newer areas in near future.
In absence of a suitable treatment or vaccine, mosquito control and personal protection from mosquitoes are the most feasible options to combat Chikungunya. Mosquito population is increasing, especially in urban areas due to improved transportation to these areas and unplanned and unorganized urbanization. Health officials should be trained about different types of mosquito control measures. The localities of affected areas must be educated about different mosquito control measures like source reduction and personal protection from mosquito bitesetc.
Conflict of interest statement
The authors declare that they have no con flict of interest.
Acknowledgements
Excellent technical assistance received from Mr. C.K. Sarma during the study is highly acknowledged. Authors also acknowledge Mr.Himanshu Medhi for his help in preparing the map and the assistance of Mr. Dipanjal Bhuyan, Mr. Amberly Shylla and Mr. Khageswar Das in both field survey and laboratory work. Last but not the least,all the staffs of health authority of the three states and all staffs of Entomology and Filariasis Division are highly acknowledged for their help and cooperation during the study.
Foundation project
This study was supported by Indian Council of Medical Research,New Delhi(No. NER/23/2013-ECD-I).
杂志排行
Asian Pacific Journal of Tropical Medicine的其它文章
- Resistance status of main malaria vector, Anopheles stephensi Liston(Diptera: Culicidae) to insecticides in a malaria Endemic Area, Southern Iran
- Frequency of typhoon occurrence accounts for the Poisson distribution of human leptospirosis cases across the different geographic regions in the Philippines
- Cytotoxic, antioxidant and antimicrobial activities of Nerium oleander collected in Morocco
- Diagnosis of Toxoplasma gondii infection in pregnant women using automated chemiluminescence and quantitative real time PCR
- Potentiating activity of rhein in targeting of resistance genes in methicillin-resistant Staphylococcus aureus
- Antibiotic resistance of Neisseria species in Iran: A systematic review and meta-analysis