Submucosal tunneling endoscopic resection: An effective and safe therapy for upper gastrointestinal submucosal tumors originating from the muscularis propria layer
2019-01-29ChenDuNingLiChaiEnQiangLingHuZhenJuanLiLongSongLiJiaLeZouLeiJiangZhongShengLuJiangYunMengPingTang
Chen Du, Ning-Li Chai, En-Qiang Ling-Hu, Zhen-Juan Li, Long-Song Li, Jia-Le Zou, Lei Jiang,Zhong-Sheng Lu, Jiang-Yun Meng, Ping Tang
Abstract AIM To evaluate the effectiveness and safety of submucosal tunneling endoscopic resection (STER) and compare its outcomes in esophageal and cardial submucosal tumors (SMTs) of the muscularis propria (MP) layer.METHODS From May 2012 to November 2017, 173 consecutive patients with upper gastrointestinal (GI) SMTs of the MP layer underwent STER. Overall, 165 patients were included, and 8 were excluded. The baseline characteristics of the patients and SMTs were recorded. The en bloc resection rate, complete resection rate,residual rate, and recurrence rate were calculated to evaluate the effectiveness of STER, and the complication rate was recorded to evaluate its safety. Effectiveness and safety outcomes were compared between esophageal and cardial SMTs.RESULTS One hundred and twelve men and 53 women with a mean age of 46.9 ± 10.8 years were included. The mean tumor size was 22.6 ± 13.6 mm. Eleven SMTs were located in the upper esophagus (6.7%), 49 in the middle esophagus (29.7%), 46 in the lower esophagus (27.9%), and 59 in the cardia (35.7%). Irregular lesions accounted for 48.5% of all lesions. STER achieved an en bloc resection rate of 78.7% (128/165) for GI SMTs with an overall complication rate of 21.2% (35/165).All complications resolved without intervention or were treated conservatively without the need for surgery. The en bloc resection rates of esophageal and cardial SMTs were 81.1% (86/106) and 72.1% (42/59), respectively (P = 0.142), and the complication rates were 19.8% (21/106) and 23.7% (14/59), respectively, (P =0.555). The most common complications for esophageal SMTs were gas-related complications and fever, while mucosal injury was the most common for cardial SMTs.CONCLUSION STER is an effective and safe therapy for GI SMTs of the MP layer. Its effectiveness and safety are comparable between SMTs of the esophagus and cardia.
Key words: Endoscopic resection; Submucosal tunnel; Submucosal tumor; Muscularis propria layer; Esophagus; Cardia
INTRODUCTION
A submucosal tumor (SMT) is defined as a protuberance in the gastrointestinal tract with a normal mucosa-covered surface. SMTs are often incidentally detected on imaging. SMTs have a broad differential diagnosis, and most SMTs with a diameter less than 3 cm are believed to be benign leiomyomas[1]. However, a proportion of SMTs, such as gastrointestinal stromal tumors (GISTs), have malignant potential[2].SMTs have a greater probability of malignancy when they originate from the muscularis propria (MP) layer, have a large diameter, or are mesenchymal neoplasms[3-7].
Thus, the accurate diagnosis of SMTs is of the greatest importance to guide further treatment. Without resection, it is difficult to obtain an accurate diagnosis of the subtypes of SMTs even by endoscopic ultrasound-guided fine needle aspiration (EUSFNA) and biopsy, which are regarded as the most reliable methods for obtaining a histological diagnosis[8-11]. Lifelong follow-up not only increases the financial burden and psychological stress to the patients but also delays the urgent diagnosis of malignancy and treatment[12-14].
Digestive endoscopic tunnel technique (DETT) was first reported by Ling-Hu et al[15,16]in 2009. In 2010, Inoue et al[17]reported peroral endoscopic myotomy (POEM)using DETT for the treatment of achalasia cardia (AC). Submucosal tunneling endoscopic resection (STER), which was inspired by DETT, was initially reported by Xu et al[18]in 2012 for the resection of SMTs originating from the MP layer. A tunnel between the mucosa and the MP layer is established, and the operation is performed within the tunnel. SMTs are resected while the mucosal covering was maintained.Although endoscopic submucosal excavation (ESE) and endoscopic full-thickness resection (EFR) have been reported to be effective and safe for the resection of SMTs located in the MP[19-23], they fail to maintain the integrity of the mucosa like the STER procedure. SMTs located in the cardia are considered more challenging and difficult to be resected by STER than those located in the esophagus. Several studies have demonstrated the effectiveness and safety of STER[12,14,24-26], however, few studies have enrolled large populations of more than 100 cases and compared the effectiveness and safety of STER for SMTs located in different locations[27,28]. In this retrospective study,we aimed to further evaluate the effectiveness and safety of STER for gastrointestinal(GI) SMTs originating from the MP layer in a large population and compare the feasibility of STER for resection of esophageal and cardial SMTs.
MATERIALS AND METHODS
Patients
From May 2012 to November 2017, at our center, STER was performed on 173 consecutive patients diagnosed with GI SMTs originating from the MP layer. In all,165 patients were included, and 8 were excluded (Figure 1). We excluded three patients with gastric antrum SMTs who underwent STER due to the small number of patients and because STER is less commonly performed in the antrum and requires further evaluation. The bent anatomical orientation of the stomach makes it challenging to perform STER because of the difficulty in establishing a submucosal tunnel. One patient diagnosed with cancer was excluded because the disease was not indicative of STER. Two patients with more than one SMT were excluded to eliminate the intervention for results. Two patients with AC and cardial SMTs underwent POEM and STER simultaneously and were excluded for the difficulty in the evaluation of the outcomes of STER.
In our study, patients with SMTs were considered eligible for STER if the following criteria were met: (1) SMTs were covered with the intact mucosa; (2) SMTs originated from the MP layer as confirmed by CT and/or endoscopic ultrasound (EUS); (3) SMTs had a transverse diameter of no more than 35.0 mm (≤ 35.0 mm); (4) patients were older than 18 years old; (5) patients had no signs of metastasis or invasion outside the digestive tract; (6) SMTs had no high-risk features of malignancy as assessed by EUS;and (7) patients signed an informed consent form. The exclusion criteria were as follows: (1) SMTs that were located less than 3-5 cm from the esophageal inlet; (2)SMTs that had signs of metastasis and/or invasion outside the digestive tract; (3)SMTs that were considered to be at high risk from surgery, such as those with an abundant blood supply; (4) patients who were pregnant; and (5) patients with coagulopathies (international normalized ratio > 1.5 and/or a platelet count < 50000).SMTs located in the upper esophagus at a distance less than 3-5 cm could not be resected by STER because of insufficient room to produce a tunnel.
STER procedures
Preoperative contrast-enhanced mediastinal CT and EUS (Prosound F75, Aloka,Tokyo, Japan and GF-UCT260, Olympus, Tokyo, Japan) were recommended for patients with suspected SMTs to evaluate the size, location, shape, and depth of the tumors and to rule out invasion outside the digestive tract and metastasis. All patients were fasted for 8 h before the procedures. STER was performed by experts with POEM experience in more than 100 cases.
STER was performed on patients under general anesthesia with a single-accessory channel endoscope (GIF Q260J/GIF Q290, Olympus) equipped with a transparent cap(D-201-11802, Olympus). A carbon dioxide (CO2) insufflator (UCR, Olympus) was used to achieve CO2insufflation. A high-frequency generator (VIO 200D, ERBE,Tübingen, Germany) and an argon plasma coagulation unit (APC300, ERBE) were used during the procedures. The STER procedures were primarily performed after endoscopic evaluation as follows (Figures 2 and 3): (1) Several milliliters of a mixture solution (100 mL saline + 2 mL indigo carmine + 1 mL epinephrine) were injected 3 cm to 5 cm proximal to the SMT with an injection needle (NM-4L-1, Olympus); (2) a longitudinal mucosal incision, transverse incision, or inverted T incision was made with a triangular knife (KD-640L, Olympus) as the tunnel entrance; (3) a tunnel was created between the mucosal and MP layers with the triangular knife and the tunnel ended at 1 cm to 2 cm distal to the SMT; (4) an insulation-tip knife (KD611L, IT2,Olympus), a triangular knife, or a snare (ASM-1-S or ASJ-1-S, Cook, Limerick, Ireland)was used to resect the SMT after it was completely exposed; and (5) the incision was closed with clips (HX-610-135, Olympus) after examination of the tunnel.
STER procedures for SMTs located in the cardia were more challenging due to the need to create a tunnel from the esophagus, through the lower esophageal sphincter(LES), to the cardia. It was difficult to identify the direction of tunnel. Methylene blue or indigo carmine can be used to locate the tumor and guide the direction of the tunnel after endoscopic evaluation[29].
Postoperative management and follow-up
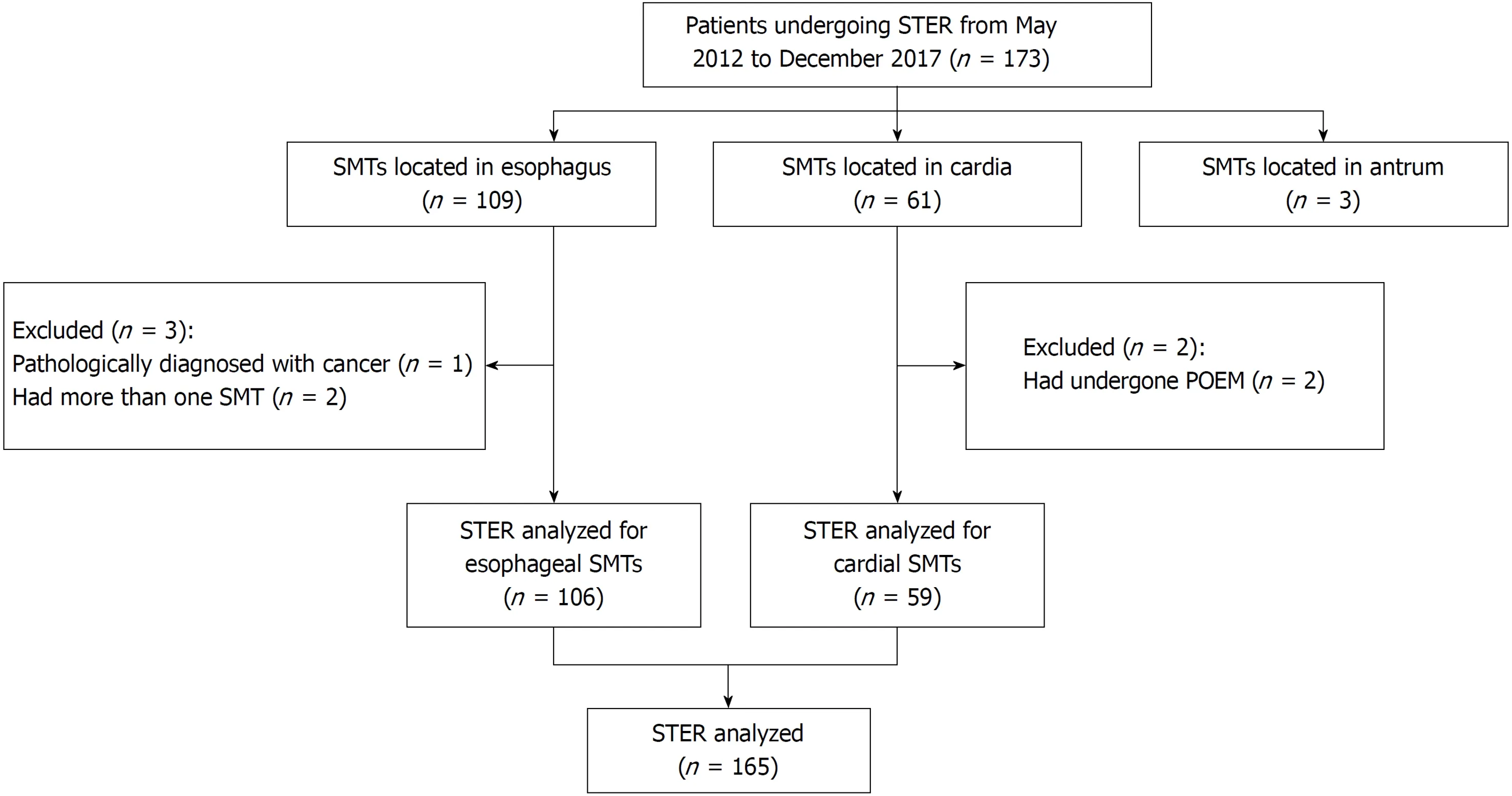
Figure 1 Study flowchart.
Patients were fasted for 2-3 d, followed by a liquid diet for 3 d, then they gradually returned to a normal diet within 2 wk after the STER procedures. Oral proton pump inhibitor (PPI) therapy was used for 4 wk, following 3 d of intravenous PPI treatment.Intravenous antibiotics were administered from the day STER was performed and were stopped after 2-3 d if no signs of infection were observed. Patients were closely monitored for any complications, such as subcutaneous emphysema, mediastinal emphysema, pneumothorax, pneumoperitoneum, fever, chest pain, abdominal pain,hematemesis, and hematochezia. If a patient suffered from severe chest and/or abdominal pain, a chest/abdominal X-ray or CT was performed.
Gastroscopy and/or EUS were recommended at 1, 3, 6, and 12 mo after the operation and then annually thereafter. For patients who were diagnosed with GISTs,an additional contrast-enhanced CT scan was recommended every 3-6 mo for approximately 5 years.
Outcome measures
The en bloc resection rate, complete resection rate, residual rate, and recurrence rate were calculated to evaluate the effectiveness of STER, while the complication rate was recorded to evaluate its safety.
Complete resection was defined as removal of the tumor en bloc with tumor freelateral and basal margins upon pathologic examination. Residual tumor was defined as redetection of an SMT within 1.0 cm around the primary resected SMT less than 6 mo after STER, while recurrence was defined as redetection of an SMT within 1.0 cm around the primary resected lesion more than 6 mo after STER. Fever was diagnosed if the axillary temperature was > 38 °C. Tumor size was determined according to the longest diameter measured on the resected specimen. If the tumor was removed by piecemeal resection, it was reconstructed to evaluate its size. Accurate specimen size was not available for residual SMTs, and therefore, the size of those tumors was determined by EUS evaluation. Operative time was regarded as the period between submucosal injection and endoscope withdrawal, while the hospital time began on the day of surgery. Subcutaneous emphysema, mediastinal emphysema,pneumothorax, and pneumoperitoneum were regarded as gas-related complications.
Statistical analysis
The analyses were performed with SPSS 22.0 software (IBM Corp, Armonk, NY,United States). Parametric data, including the tumor size, operative time, hospital time, tunnel length, number of clips, medical cost, and follow-up period, are expressed as the mean ± standard deviation (SD) or median with the range and were assessed by Student's t-test or a nonparametric test. Nonparametric variables, such as sex, location, shape, en bloc resection rate, and complete resection rate, are expressed as proportions and were assessed by the χ2test or Fisher's exact test. A P-value (twotailed) < 0.05 was considered statistically significant.
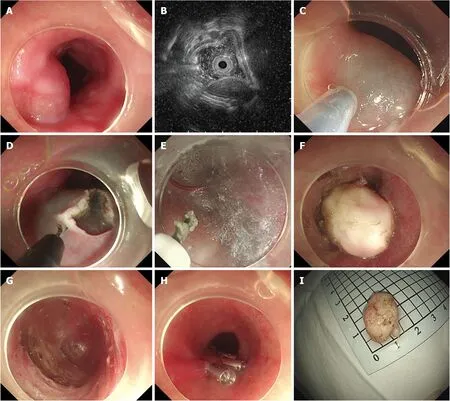
Figure 2 Submucosal tunneling endoscopic resection for a submucosal tumor originating from the muscularis propria layer in the esophagus. A:Endoscopic view of a submucosal tumor (SMT) in the esophagus; B: Endoscopic ultrasound view of the same SMT, showing that lesion originates from the muscularis propria (MP) layer; C: Submucosal injection at 5 cm proximal to the SMT; D: An inverted T mucosal incision; E: Establishment of a submucosal tunnel between the mucosal and MP layers; F: Exposure of the SMT; G: The tunnel after the resection of the tumor; H: Closure of the mucosal incision site with clips; I: The resected specimen.
RESULTS
From May 2012 to December 2017, 173 patients with GI SMTs originating from the MP layer underwent STER. After 8 patients were excluded, 165 patients were retrospectively enrolled, including 112 men and 53 women, with a mean age of 46.9 ±10.8 years. The median size of tumor sample was 20.0 (range, 5.0-80.0 mm). Of the 165 lesions, 11 (6.7%) were located in the upper esophagus, 49 (29.7%) in the middle esophagus, 46 (27.9%) in the lower esophagus, and 59 (35.7%) in the cardia. Irregular lesions accounted for 48.5% of all lesions. Pathological diagnosis revealed that there were 157 (95.2%) leiomyomas, 3 (1.8%) GISTs, 3 (1.8%) lipomas, 1 (0.6%) schwannoma,and 1 (0.6%) fibrous tumor. The sizes of each of these three GISTs were 8.0 mm × 8.0 mm, 24.0 mm × 11.0 mm, and 25.2 mm × 13.2 mm, while their mitotic rates were no more than 5/50 high-power fields. The detailed characteristics of the patients and SMTs are summarized in Table 1.
Effectiveness of STER
En bloc resection was achieved in 128 of the 165 lesions treated, for which the the en bloc resection rate was 78.7%. The complete resection rate was 78.7%. Four SMTs were not resected completely due to their large size, deep invasion, and/or proximity to the aortic arch, which resulted in a residual rate of 2.4% (4/165). No recurrence was noted during follow-up. The median operative time was 46 min (range 10-221 min). The median hospital time was 7 d (range 4-18 d). The median length of the tunnel was 7 cm (range 5-14 cm). The median number of clips was 5 (range 3-22). Patients spent a median of 4957.72 USD (range 3160.63-12882.63 USD). The effectiveness outcomes are shown in Table 2.
Safety of STER
All 35 patients experienced intraoperative and postoperative complications at a rate of 21.2% (35/165) (Table 3). The most common complications were fever (13/165),mucosal injury (12/165), and gas-related complications (10/165). No severe complications occurred, and all complications resolved without intervention or were treated conservatively without the need for surgery. One case of a large perforation of the MP layer occurred in a large lesion located in the cardia that deeply invaded the MP layer and adhered to the serosa. Clips were used to close the perforation after the resection of the mucosa near the perforation. The integrity of the mucosa was not maintained in that case.
Comparison of STER for GI SMTs in different locations
The patients were divided into two groups (esophagus group and cardia group)based on the location of the lesions. When the esophagus group was compared with the cardia group in terms of baseline characteristics (Table 4), SMTs located in the cardia appeared to be larger and were more likely to have an irregular shape than those located in the esophagus. No significant differences were observed in age or sex between patients in the two groups.
En bloc resection was achieved in 86 (81.1%) patients in the esophagus group and 42(72.1%) in the cardia group, and the difference was not statistically significant (P =0.142). Two residual tumors were noted in both groups, but no recurrence was noted during follow-up. The comparison of effectiveness outcomes between the two groupsis shown in Table 5. No significant differences were seen in operative time, hospital time, number of clips, or medical cost between the esophagus and cardia groups.
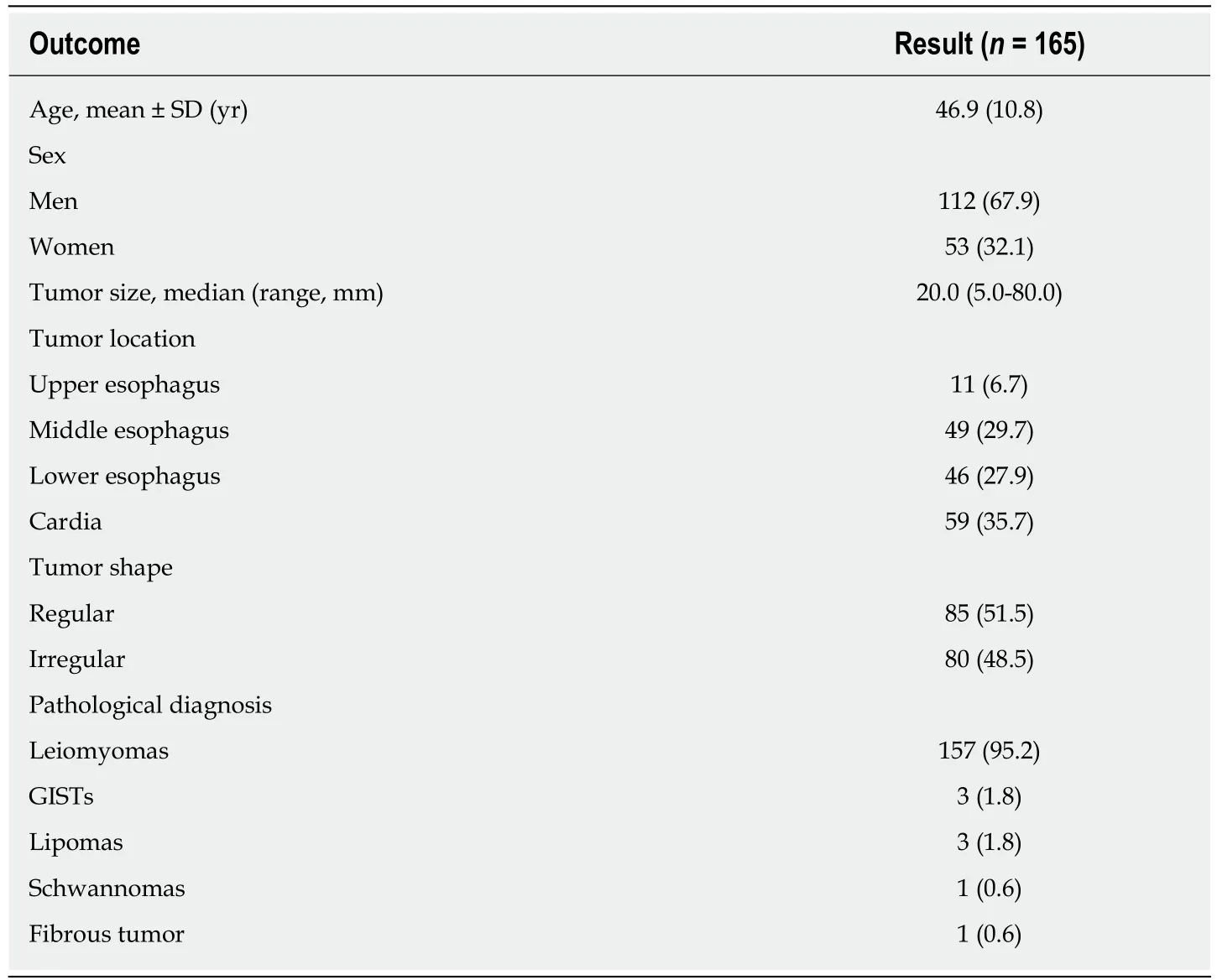
Table 1 Detailed characteristics of the 165 enrolled patients and submucosal tumors n (%)
Procedure-related complications occurred in 21 (19.8%) patients in the esophagus group and 14 (23.7%) patients in the cardia group (Table 6). Difference in the complication rates between the two groups was not statistically significant(esophagus, 19.8%; cardia, 23.7%; P = 0.555). The most common complications in the esophagus group were gas-related complications (8/106) and fever (9/106), while the mucosal injury (9/59) was the most common complication in the cardia group.
DISCUSSION
SMTs have a broad differential diagnosis and are mainly divided into leiomyomas,GISTs, fibrous tumors, and schwannomas. With the development of imaging techniques, the detection rate of SMTs has been increasing and the incidence of SMTs has been reported to be 3%[7,30]. SMTs are covered by intact mucosa, which increases the difficulty of EUS-FNA and biopsy, especially when the tumors originate in the MP layer. Considering the limited diagnostic value and the challenge of preoperative tissue collection especially when SMTs are easily resected and the accuracy of biopsy seems low[7,11,18,31-34], preoperative EUS-FNA was not performed in our study. Although benign leiomyomas are the most common SMTs in the esophagus, GISTs with malignant potential are the second most common SMTs. Treatment of SMTs in the esophagus is also important. Surgical resection and endoscopic resection are two methods used to resect SMTs. However, surgical resection, regardless of whether open surgery or video-assisted thoracoscopic surgery (VATS) is performed, seems to be more invasive than endoscopic resection[35-38]. STER is regarded as the optimum method for resecting SMTs originating from the MP layer based on its advantages of a high en bloc resection rate and the ability to maintain the integrity of the mucosa[29,39-41].The creation of a tunnel not only maintains the integrity of the mucosa, but also decreases the likelihood of perforation, postoperative infection, fistula, and stricture[12]. Although several studies have reported results of STER for GI SMTs[18,29,40,42-49], few studies have enrolled a large population. Thus, the results are less convincing and further studies are necessary[27,28]. This study was designed to further evaluate the effectiveness and safety of STER for GI SMTs and to compare the outcomes of STER between esophageal and cardial SMTs.
In our current study, STER achieved an en bloc resection rate of 78.7% (128/165) forGI SMTs with an overall complication rate of 21.2% (35/165). Only four SMTs were not completely resected, which resulted in a residual rate of 2.4% (4/165), however,no recurrence was noted during follow-up. Large size, deep invasion, and/or proximity to the aortic arch were risk factors for residual tumors. STER was not indicated for SMTs with a transverse diameter larger than 35.0 mm because the inner diameter of the tunnel was approximately 3.5 cm, however, the upper limit of the longest tumor diameter remains unknown. A 7-cm SMT was successfully resected by Chen et al[28]However, larger size is associated with a high risk of malignancy and may result in loss of endoscopic visualization. The en bloc resection rates of STER for esophageal SMTs and cardial SMTs were 81.1% (86/106) and 72.1% (42/59),respectively. The complication rates of STER for esophageal SMTs and cardial SMTs were19.8% (21/106) and 23.7% (14/59), respectively. No significant differences were observed in en bloc resection or complication rates between those two locations. The most common complications that occurred in the esophagus were gas-related complications and fever, while mucosal injury was the most common complication in the cardia. No severe complications that required surgical treatment or led to death occurred in our study.
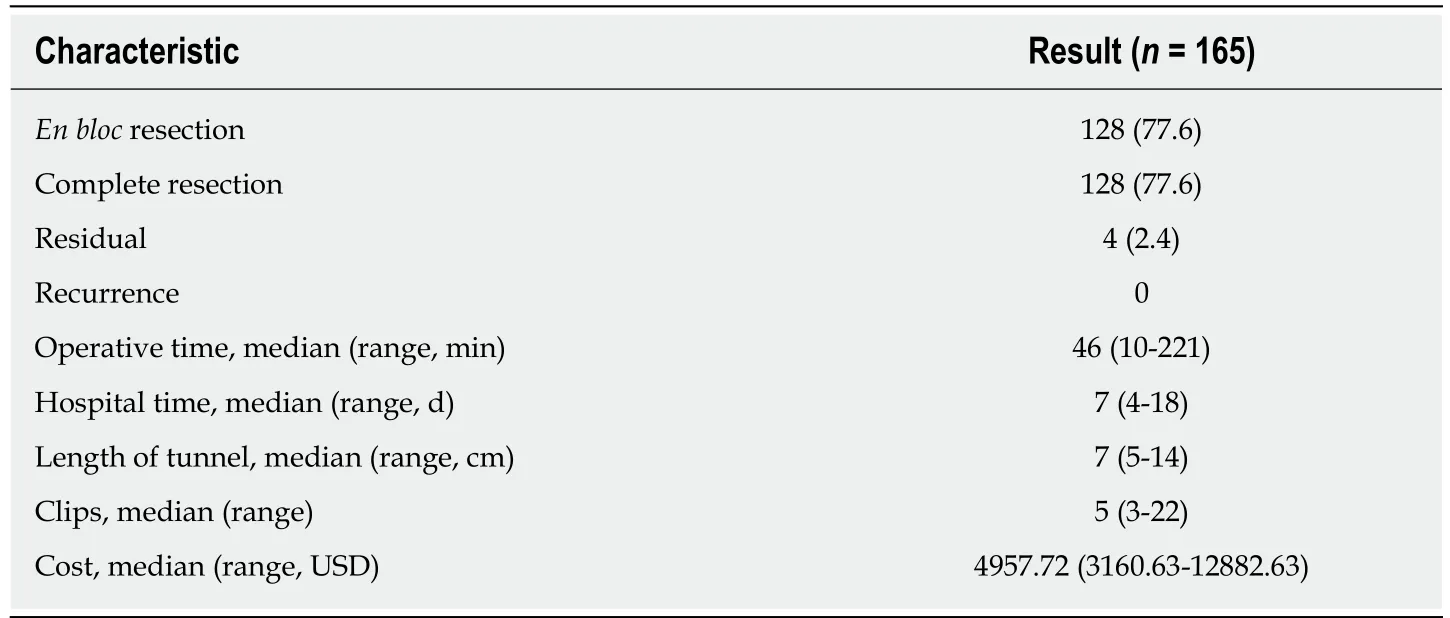
Table 2 Effectiveness outcomes of submucosal tunneling endoscopic resection for gastrointestinal submucosal tumors n (%)
STER was effective not only for esophageal SMTs but also for cardial SMTs, and had a high en bloc resection rate. En bloc resection rate demonstrated in this study was slightly lower than those in previous studies which ranged from 83.3% to 100%[24]. We speculated that a snare was used to quickly resect the lesion after the majority part of the SMT was exposed in some cases, which led to a high incidence of piecemeal resection[12,26]. Although STER for cardial SMTs was more challenging than that for esophageal SMTs, their en bloc resection rates were comparable even though cardial SMTs were larger and more irregular than esophageal SMTs. We speculate that there may be two reasons that explain these findings. First, the therapeutic outcomes of STER in different locations, including the esophagus, cardia, stomach, and rectum have been reported to be good, and therefore, the difference between these two locations might be too small to show any difference. In our study, the en bloc resection rate in the esophagus group was higher than that of the cardia group, however, the difference was not significant. Second, the cardia group only contained 59 patients,which is relatively small. The operative time was also comparable. The creation of a tunnel during STER for cardial SMTs was more difficult than for esophageal SMTs and thus required more time. However, SMT exposure as well as the resection and incision closure accounted for the majority of the operative time, thus, no significant difference was observed between the two groups with respect to operative time.
The STER-related complication rates mainly range from 5% to 25% with no reported deaths, and most of the complications reported are mild[14], which is in accordance with our results. A meta-analysis involving 12 studies including 397 patients and 430 lesions showed that the pooled complication rate of STER for GI SMTs was 21.5% (95%CI: 13.2-33.1%)[25]. Gas-related complications are regarded as the most common complication related to STER[28,35,45,46,48]. In our study, gas-related complications were the most common complications of STER for GI SMTs, with a complication rate of 9.7% (16/165). Gas-related complications were also the most common complications for esophageal SMTs, with a rate of 19.8% (19/106), which is consistent with previous studies. The pooled prevalence of gas-related symptoms was 14.8% (95%CI: 10.5%-20.5%) for subcutaneous emphysema and pneumomediastinum,6.1% (95%CI: 4.0%-9.0%) for pneumothorax, and 6.8% (95%CI: 4.7%-9.6%) for pneumoperitoneum, which were demonstrated in another meta-analysis[50].

Table 3 Safety outcomes of submucosal tunneling endoscopic resection for gastrointestinal submucosal tumors
The most common complications in patients with esophageal and cardial tumors were different in our study. The reasons for this were as follows: (1) The absence of a serous membrane in the esophagus makes it easier for gas to diffuse into the subcutis,mediastinum, thorax, and abdomen, thus, gas-related complications were more prevalent in the esophagus group; (2) the MP layer is thicker in the cardia than in the esophagus, which decreases the likelihood and amount of gas effusion; and (3) the anatomic structure of the cardia makes the direction of the tunnel difficult to identify and the tunnel difficult to establish, therefore, the mucosa was at higher risk of injury when the tunnel was created.
The present study has are several limitations. First, it was designed as a singlecenter, retrospective study. Second, the accuracy of the origin of the SMTs from the MP layer was not considered in this study due to the difficulty of retrospective evaluation based on EUS images. Third, the number of patients in the cardia group was small. Fourth, no control groups were included. Thus, randomized controlled studies involving a large population are warranted to evaluate the long-term outcome of STER compared with that of other treatments, such as ESE and EFR, for SMTs originating from the MP layer.
In conclusion, STER is an effective and safe method for the resection of upper GI SMTs with an overall en bloc resection rate of 77.6% and a complication rate of 21.2%.Gas-related symptoms and fever are the most common complications in patients with esophageal SMTs, while submucosal injury is the most common complication in patients with cardial SMTs. The effectiveness and safety of STER for tumors in the esophagus and cardia are comparable.
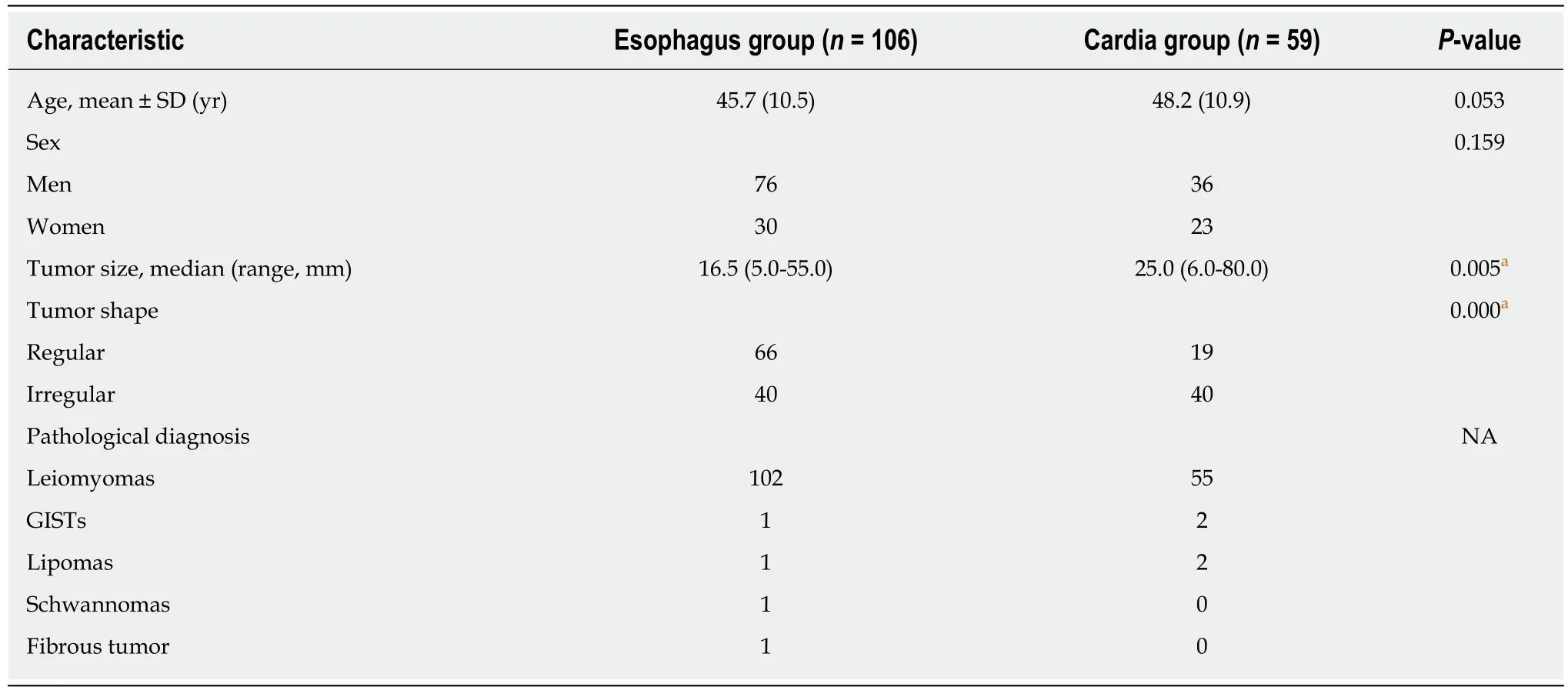
Table 4 Comparison of baseline characteristics of patients and submucosal tumors between esophagus group and cardia group n (%)
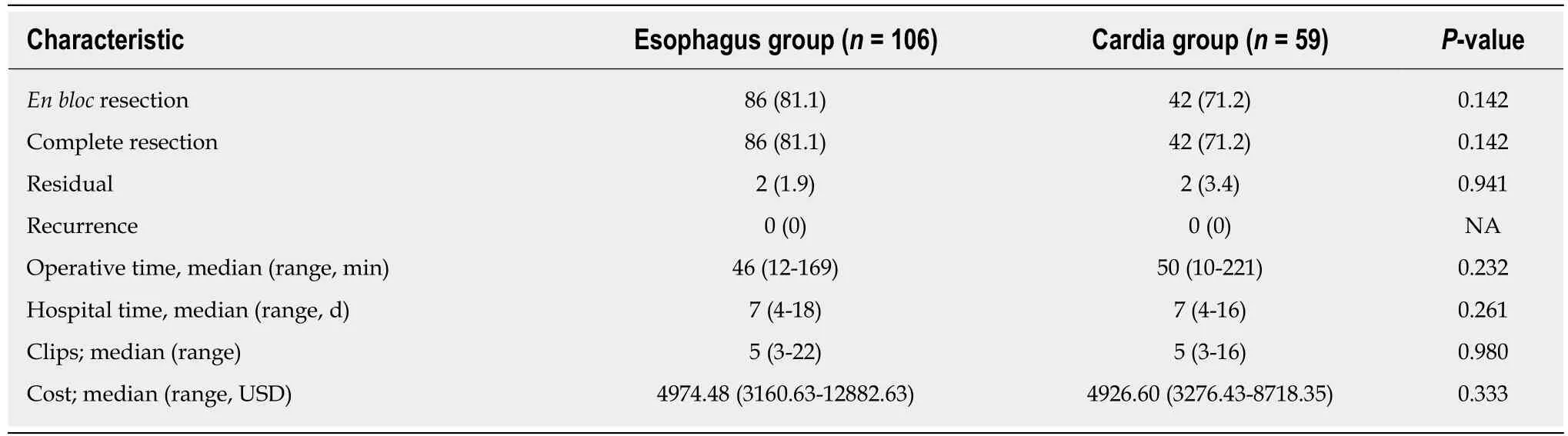
Table 5 Comparison of effectiveness outcomes between esophagus group and cardia group n (%)
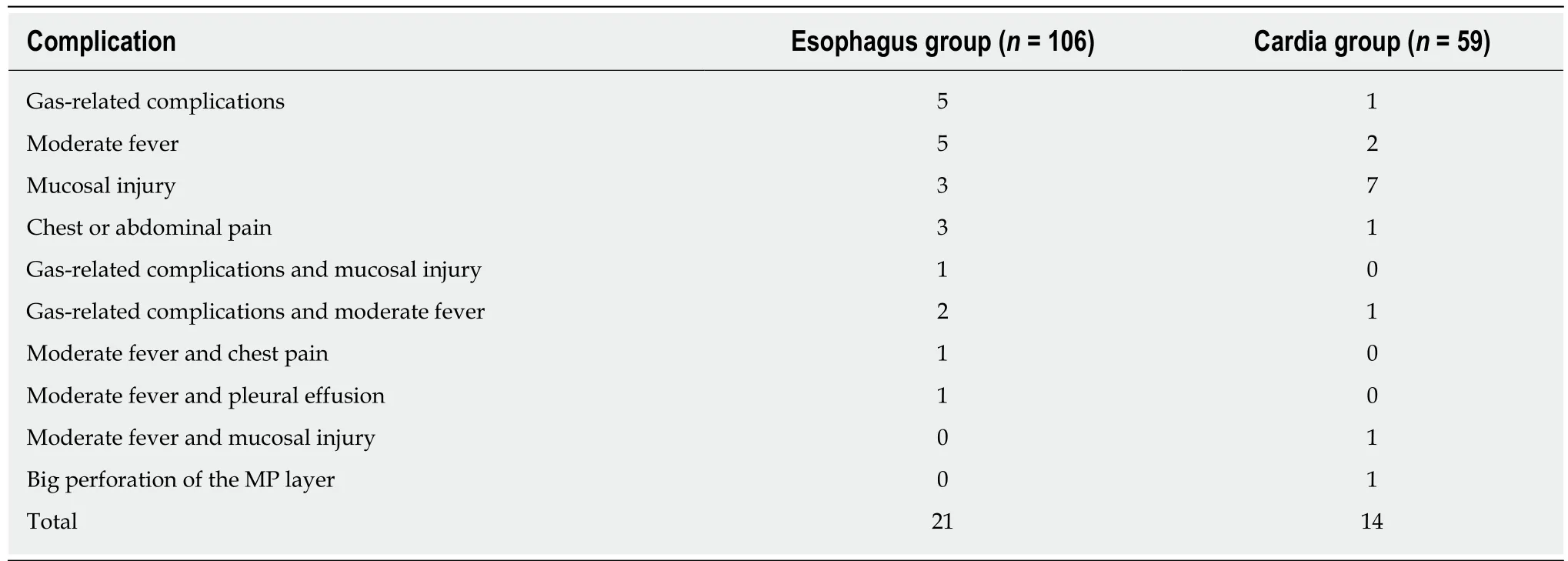
Table 6 Comparison of safety outcomes between esophagus group and cardia group
ARTICLE HIGHLIGHTS
Research background
Submucosal tumors (SMTs) have a greater possibility of malignancy when they originate from the muscularis propria (MP) layer, have a large diameter, or are mesenchymal neoplasms.Without resection, it is difficult to obtain an accurate diagnosis of the subtypes of SMTs even by endoscopic ultrasound-guided fine needle aspiration and biopsy, which are regarded as the most reliable methods. Submucosal tunneling endoscopic resection (STER), which was inspired by digestive endoscopic tunnel technique, was reported for the resection of SMTs originating from the MP layer with the advantage to maintain the integrity of the mucosa in 2012. As a minimally invasive produce, STER acts an important role in the treatment of SMTs.
Research motivation
Few studies describing STER for SMTs located in the MP layer have enrolled large populations of greater than 100 cases. Studies enrolled large samples are needed. Although STER procedures for SMTs located in the cardia were regarded to be more challenging due to the need to create a tunnel from the esophagus, through the lower esophageal sphincter, to the cardia, no studies comparing the effectiveness and safety of STER for SMTs located in different locations have been performed.
Research objectives
In this retrospective study, we further evaluated the effectiveness and safety of STER for gastrointestinal (GI) SMTs originating from the MP layer in a large population and compared the feasibility of STER for resection of esophageal and cardial SMTs.
Research methods
From May 2012 to November 2017, 173 consecutive patients with upper GI SMTs of the MP layer underwent STER. Overall, 165 patients were included, and 8 were excluded. The en bloc resection rate, complete resection rate, residual rate, and recurrence rate were calculated to evaluate the effectiveness of STER, and the complication rate was recorded to evaluate its safety.Effectiveness and safety outcomes of STER were compared between esophageal and cardial SMTs.
Research results
En bloc resection was achieved in 128 of the 165 lesions treated with an en bloc resection rate of 78.7%. Four SMTs were not resected completely owing to large size, deep invasion, and/or proximity to the aortic arch, leading to a residual rate of 2.4% (4/165). No recurrence was noted during follow-up. The complete resection rate was 78.7%. Thirty-five patients had intraoperative or postoperative complications, with a rate of 21.2% (35/165). The most common complications were fever (13/165), mucosal injury (12/165), and gas-related complications (10/165). No severe complications occurred. En bloc resection was achieved in 86 (81.1%) patients in the esophagus group and 42 (72.1%) in the cardia group, and there was no significant difference between them(P = 0.142). There was no significant difference in the complication rate between the two groups(esophagus, 19.8%; cardia, 23.7%; P = 0.555). The most common complications in the esophagus group were gas-related complications (8/106) and fever (9/106), while mucosal injury (9/59)was the most common complication in the cardia group. However, the accurate origin from the MP layer of the SMTs was not taken into consideration in this study and the number of patients in the cardia group was small.
Research conclusions
STER is an effective and safe therapy for GI SMTs of the MP layer with an en bloc resection rate of 78.7% and a complication rate of 21.2%. No recurrence was observed during follow-up, even after piecemeal resection. Although STER for cardial SMTs was more challenging than that of esophageal SMTs, their en bloc resection rates were comparable even though cardial SMTs were larger and more irregular than esophageal SMTs. The most common complications in the esophagus group were gas-related complications and fever, while mucosal injury was the most common complication in the cardia group.
Research perspectives
Although piecemeal resection may do not influence long-term outcomes, it affects pathological evaluation. Therefore, en bloc resection should be maintained. Randomized controlled studies involving a large population are warranted to evaluate the long-term outcome of STER compared with other treatments for SMTs originating from the MP layer, such as endoscopic submucosal excavation and endoscopic full-thickness resection.
杂志排行

World Journal of Gastroenterology的其它文章
- Role of diet and gut microbiota on colorectal cancer immunomodulation
- Current status, problems, and perspectives of non-alcoholic fatty liver disease research
- Prevention of overuse: A view on upper gastrointestinal endoscopy
- Adverse events related to colonoscopy: Global trends and future challenges
- Human antigen R mediated post-transcriptional regulation of inhibitors of apoptosis proteins in pancreatic cancer
- Six-long non-coding RNA signature predicts recurrence-free survival in hepatocellular carcinoma