Systematicevaluationand trialsequentialanalysisofwarming acupuncture combined with joint mobilization in the treatment of scapulohumeral periarthritis
2018-09-14RongTianDaLiYuHuiHanYiHuaFan
Rong Tian,Da Li,Yu-Hui Han,Yi-Hua Fan
1TianJin University of Sport,Tianjin,China.2Tianjin University of Traditional Chinese Medicine,Tianjin,China.3Department of Rehabilitation,Affiliated Hospital of Inner Mongolia University of Nationalities,Tong Liao,China.
Introduction
In recent years, the number of patients with scapulohumeral periarthritis has increased gradually,and problems of pain and joint dysfunction have attracted increasing attention [1].Scapulohumeral periarthritis refers to extensive aseptic inflammation caused by cold shoulder,trauma,shoulderstrain,and degenerative changes.The main clinical manifestations are shoulder pain and limitations in joint motion[2].The initial symptoms of the disease are relatively mild and patients are often easily overlooked.Therefore,it is easy to delay the opportunity for optimal treatment[3].If not treated promptly,scapulohumeral periarthritis can lead to a variety of complications and has a significant impact on patient quality of life[4].
Presently,Western medicine uses methods such as surgery,steroid hormones,and hydraulic expansion,to treat the scapulohumeral periarthritis.There is a certain risk for surgical treatment,and as time passes,the efficacy of drug therapy is maintained for only a short time.The shoulder joint hydraulic expansion method lacks the support of randomized controlled trial(RCT)results[5].Warming acupuncture was first recorded inShanghanzabinglun(215-282,A.D.Jin Dynasty)and prospered in the middle and end of Ming dynasty(1644,A.D.).It refers to the use of wormwood warming and dredge the channels,and also regulating Qi and blood.It is used to enhance the analgesic effect of simple acupuncture on local pain.It is a commonly used treatment for scapulohumeral periarthritis due to disharmony of Qi and blood.According to the record ofYixuerumen(1575,A.D.Ming Dynasty)said,“All the diseasethatcouldn’tbecured by medicinesand acupuncture must be treated with warm acupuncture”,and there is a relevant system evaluation that has confirmed a significant effect of warm acupuncture in the treatmentofscapulohumeralperiarthritis[4].Joint mobilization is a modern rehabilitation technique that uses articular surface sliding,rolling,rotation,and separation traction to relieve pain,promote synovial fluid flow,increase nutrition to the articular cartilage and articular cartilage avascular zone,and loosen tissue adhesion[6].Therefore,it is an effective treatment for scapulohumeral periarthritis,with the characteristics of quickness,low recurrence rate,and patienteasy acceptance [7].The treatmentof scapulohumeral periarthritis often involves comprehensive therapy to achieve a complementary and synergistic effect[8].
In recent years,there have been reports in the literature that warming acupuncture combined with joint mobilization has a good effect on the treatment of scapulohumeral periarthritis.However,individual studies have been based on a relatively small and insufficient amount of evidence.Therefore,to objectively evaluate the efficacy,it is necessary to perform a systematic evaluation.This study used trial sequential analysis(TSA)software to estimate the required information size(RIS)for each outcome to further evaluate the clinical efficacy of warming acupuncture combined with joint mobilization in the treatment of scapulohumeral periarthritis to provide a reference for clinical decision making.
Methods
Study types
This research used RCT and was not limited by language or the type of publication.
Search strategy
Foreign language databases were retrieved from the Cochrane Library,PubMed,Embase,and Web of Science;Chinese National Knowledge Infrastructure(CNKI),the Chinese Biomedical Literature Database(CBM),the Chinese Science and Technology Periodical Full-Text Database(VIP),and the Wanfang Database for the Chinese retrieval.The search time was limited to database building untilJanuary 30,2017.Forunpublished documents,search for related conference papers,academic reports,and full-text databases of Wanfang academic dissertation.At the same time,retrospective references of included literature.Chinese search terms:“关节松动术”,“Maitland 手法”,“温针灸”or“温针疗法”and “肩周炎”,“漏肩风”,“肩关节周围炎”,“肩凝”,“肩凝症”or“冻结肩”.English search terms included:“Joint”,“Mobilization”,“Maitland approach”,“Warming acupuncture”, “Moxa Needle Therapy” or “Chinese medicine therapy”and “Frozen shoulder”or “bursitis”.All databases are freely collocated with search terms,and included in the literature references to ensure recall ratio.
Study subjects
Subjects met the criteria for the diagnosis and efficacy of traditional Chinese medicine(TCM)diseases issued by the State Administration of Traditional Chinese Medicine in 1994[9].Diagnostic criteria for scapulohumeral periarthritis included:(1)No special findings found on X-ray examination;(2)Pressing pain at the anterior and apical shoulders;(3)Shoulder activity restricted,and obvious restrictions in rise,abduction,and internal rotation arm;(4)Gradual increase in pain on the shoulders,and difficulty with side lying,with no other serious cardiovascular or cerebrovascular diseases or complications.
Exclusion criteria
(1)Study that was non-RCT;(2)the outcome did not meet the requirements of the present study;(3)data that could not be extracted or the literature which has the confusing sign;(4)duplicate publication of the report or study;(5)case report;(6)review.
Interventions
The experimental group underwent warming acupuncture combined with joint mobilization.The control group used warming acupuncture or joint mobilization,or oral analgesics and other therapies.The basic treatments of the two groups were the same.We first conducted an overall analysis of differences between the experimental group and the control group,then according to different interventions in the control group to the subgroup analysis.
Document screening and data extraction
Two researchers independently screened the literature and performed data extraction according to the inclusion and exclusion criteria,and also included articles that were discussed or submitted to a third party for assistance.Data extraction items included the following:article title;first author’s name;publication year and literature source;baseline comparability;interventions;and outcomes for each group ofpatients.Ifdata were missing or information in the studies was unclear,the authors of those studies were contacted for clarification.
Outcomes
Primary outcomes:total efficiency was calculated as follows:
Total cases-invalid cases/total cases×100%
Efficacy judgment conformed to the Guidelines for the Clinical Research of Traditional Chinese Medicine New Drugs published in 1997,or the Criteria for Diagnosis and Efficacy of TCM Diseases,published by the State Administration of Traditional Chinese Medicine[9-10].
(1)Cure:cure was defined according to the following criteria:disappearance of shoulder pain symptoms and free movement of the shoulder;arm lift ≥ 150°,with extension ≥ 90°,and outreach ≥ 90°;shoulder joint function returned to normal,and the muscle atrophy essentially restored.
(2)Significant effect:significant effects were defined according to the following criteria:disappearance of shoulder joint pain or soreness;upper arm lift ≥ 130°,with reach ≥ 75°,abduction ≥ 75°;shoulder function returned to normal and muscle atrophy improved.
(3)Effective:effective treatment was defined as relief of shoulder joint pain;upper arm above≥ 110°,extruding≥60°,abduction ≥ 60°;and increase in shoulder range of motion.
(4)Invalid:no obvious improvement in pain in the shoulder joints.Arm lifted and the protraction and extension movements improved ≥ 30°.
Secondary outcomes
(1)Cure rate:cure rate was calcu lated as:
Number of cures/total number of cases×100%.
(2)The treatment times required for cure:this indicator referred to the number of treatments required for healing,the patient's shoulder joint can recover;
(3)Visual analog scale(VAS)method:the VAS score is represented by a 10 cm horizontal line in which one end is 0,indicating no pain,and the other end is 10,indicating severe pain;middle parts of the line represent different degrees of pain.Patients are asked to mark the line indicating the degree of pain.The average of mild pain scores was 2.57±1.04;the average of moderate pain was 5.18±1.41;the average of severe pain was 8.41±1.35.
Risk for bias assessment
According to the evaluation method for risk of bias recommended in theCochraneSystematicReview Handbook version 5.1.0,assessment of the risk for bias of the included studies was performed,including:(1)random allocation method;(2) allocation scheme concealment;(3)blinding adoption;(4)data integrity;(5)selective outcome reports;(6)other sources of bias.Each item was answered with “Yes”, “No”,or “Unclear”.“Yes”represented a low risk for bias,“No”represented a high risk for bias,and “Unclear”represented a lack of relevant information or bias is uncertain.
Statistical analysis
Meta-analysis was performed using RevMan 5.3 software provided by the Cochrane Collaboration.The weighted mean difference isa statistic used to assessthe measurement tool or unit consistent continuity data.If the measurement tool or unit is inconsistent,the standardized mean difference(SMD)is used as the statistic.The relative risk or odds ratio(OR)was used as the efficacy analysis statistic for the count data,and the merged results were estimated using the effect point and its 95%confidence interval(CI).The Chi-squared test was used to evaluate heterogeneity among the included studies.WhenP>0.1 and I2<50%,there is no statistical heterogeneity among the studies.The fixed effect model was used for analysis;ifP<0.1,I2>50%,indicating that there is heterogeneity among the studies,the source of heterogeneity is analyzed.If heterogeneity after dispose has not been eliminated,the data needs to be combined,and a random effect model is used for meta-analysis.Inclusion of no less than 10 outcomes was included in the study.Stata 12.0 was used for publication bias assessment.Egger linear regression and Begg rank correlation test were used to determine whether there was publication bias in the included studies.TSA was performed using TSA version 0.9 developed by the Copenhagen Clinical Trial Center in Denmark.The probability of type I error was set at α=0.05,and the power was determined to be 0.80.The probability and heterogeneity of the outcomes of each outcome in the control group and treatment group were automatically generated as the RIS and relative risk reduction,and TSA analysis was performed on each outcome.TSA analysis can reduce the statistical error probability of type I error by cumulative analysis and can determine whether the sample size is sufficient according to TSA critical value and RIS and accurately reflects the reliability of the conclusion.If the cumulative Z value does not cross the TSA critical value and does not exceed the RIS value,it indicates that the study’s sample size is insufficient and the conclusion is not stable.If the cumulative Z value crosses the TSA critical value,but does not reach the RIS value,it indicates that even if the sample size is insufficient,there is no need to increase the sample size;a reliable conclusion can be reached in advance.If the cumulative Z value crosses both the TSA critical value and the RIS value,it means that the sample size is sufficient and the conclusion is reliable.
Results
Literature search results
A total of 184 related documents were obtained from the database search,4 related documents were supplemented by other resources,33 articles were duplicated using Endnote,and 120 articles clearly did not fulfill the criteria by reading topics and abstracts,including 1 duplicate publication and 5 reviews.73 case series and 41 non-RCT were excluded.Through full-text reading,7 articles that did not meet the interventions,2 with missing data,8 articles exclusion by intensive reading,and 4 that did not meet the diagnosis criteria were excluded.Finally,14 articles were included[11-24]in the meta-analysis(Figure 1).
The basic feature of literature
This study included 14 RCT[11-24],there were 1090 patients,including 551 in the treatment group and 539 in the control group,with an average of 39 patients in each group.The course of treatment was 10-42 days and one study[20]conducted the number of treatments required for healing analysis.According to the characteristics of interventions,the included studies were divided into 8 articles addressing joint mobilization + warming acupuncture and joint mobilization for the control[11,12,14,18,20,21,22,24],1 article describing joint mobilization + warming acupuncture and electroacupuncture+medium-frequency therapy control[13],and 5 articles describing joint mobilization+warming acupuncture and warming acupuncture control[15,16,17,19,23].
Diagnostic criteria
Fourteen studies[11-24]used the“Criteria of diagnosis and efficacy of TCM diseases”,and 9 studies[11-16,19,22,24]used the“Guidelines for the Clinical Research of Traditional Chinese Medicine New Drugs”,1 study[18]used the “Modern Rehabilitation Therapeutics”,1 study[20]used the“Standard for the Diagnosis of Orthopaedic and Traumatological Diseases of TCM”,and 2 studies[17,21]did not clearly demonstrate efficacy.However,it consistent with the“Guidelines for the Clinical Research of New Drugs in Traditional Chinese Medicine”,the efficacy of judgment criteria on periarthritis(Table 1).
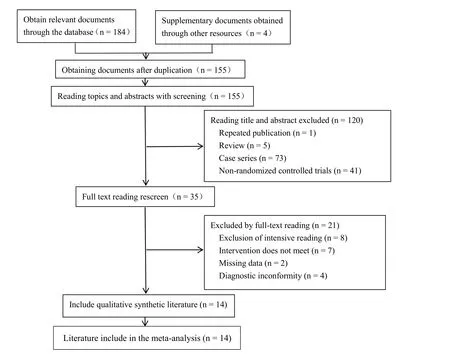
Figure 1 Flowchart of the systematic search process
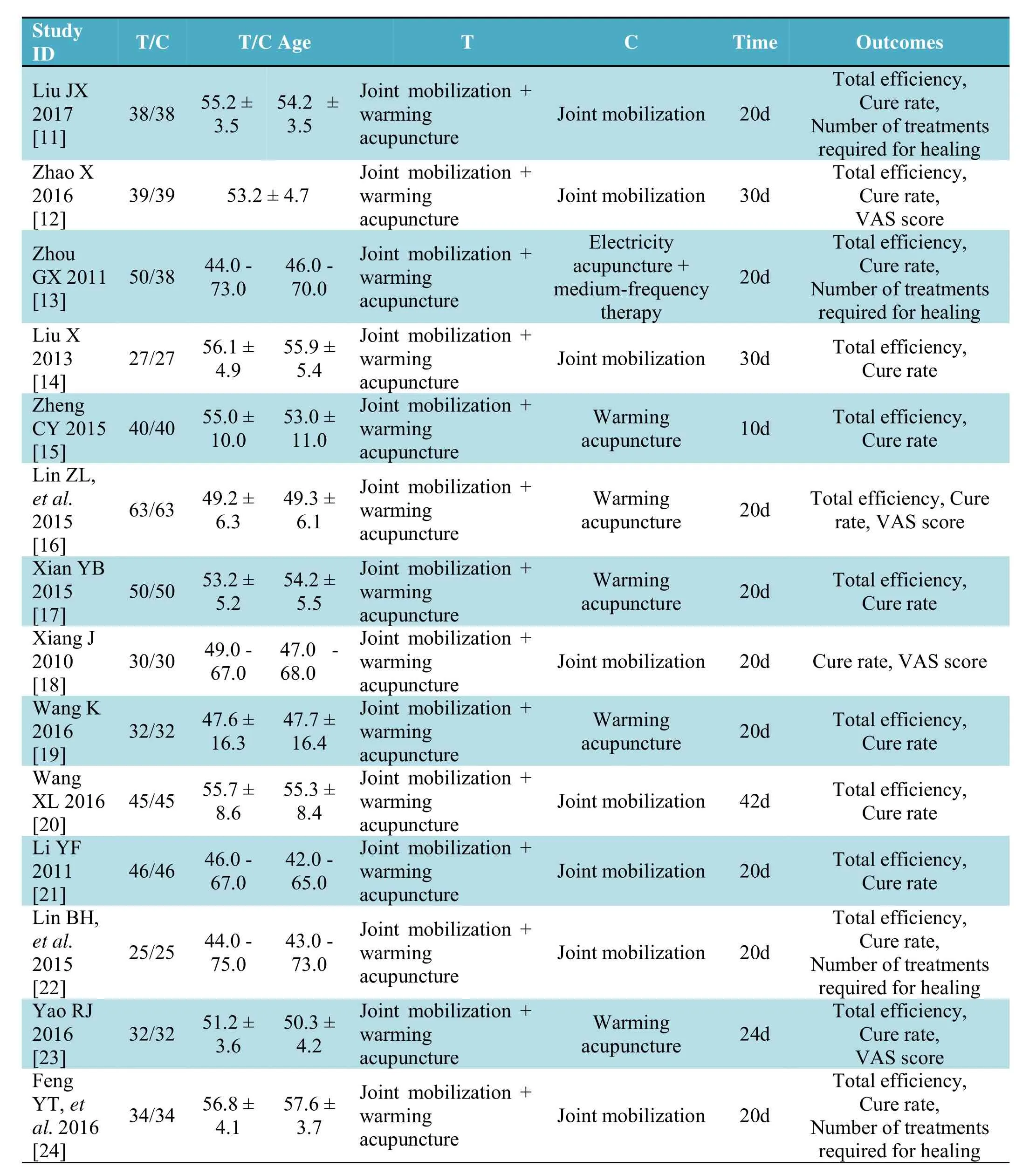
Table 1 Description of literature features
Risk for bias assessment
This study used the Cochrane systematic review manual 5.1.0 to assess the risk for bias of the included studies.Three studies[11,22,23]used a random number table method,1 study[16]used a computer stochastic method,and the remainder[12,13,14,15,17,18,19,20,21,24]only mentioned randomization withouta detailed explanation.None of the studies addressed allocation concealment schemes or blinding.As for incomplete data outcomesand selective reporting bias,the results demonstrated low risk for bias(Figure 2).
Meta-analysis and TSAresults
Total efficiencyIn 13 studies,the indicator was total efficiency,with 521 cases in the treatment group and 509 cases in the control group.The included studies were non-heterogeneous(P=0.97,I2=0%).Using the fixed-effect model,the combined effect OR was 6.16[95%CI(3.79,10.00)],Z=7.34.The difference was statistically significant(P< 0.001),suggesting that warming acupuncture and joint mobilization for scapulohumeral periarthritis has a significant effect.According to the different interventions in the control group,the subgroup analysis wasincluded in the literature;since the jointmobilization + warming acupuncture group vs.electroacupuncture+medium frequency therapy group only included 1[13]report;therefore it was excluded from the subgroup analysis.In 7 studies[11,12,14,20,21,22,24],groups were treated with warming acupuncture+joint mobilization.The control group used joint mobilization,of which 254 cases were in the treatment group and 254 cases were in the control group.There was no statistical heterogeneity(P=0.73,I2=0%);therefore,the fixed effect model was chosen.Meta-analysis revealed that warming acupuncture combined with jointmobilization can significantly improve overall efficacy[OR=6.95,95%CI(3.77,12.83),P<0.001].

Figure 2 Risk of bias graph
Five studies[15,16,17,19,23]used warming acupuncture + joint mobilization and warming acupuncture for comparison,with 217 cases in the treatment group and 217 in the control group.There was no statistical heterogeneity in the included studies(P=0.95,I2=0%);thus,the fixed-effect model was used for analysis.Meta-analysis revealed an[OR=5.13,95%CI(2.19,11.99),P< 0.001],a difference thatwas statistically significant(Figure 3).TSA revealed that an RIS of 3013 was needed to achieve a significant level of detection.The sample size(1030 cases)included in the analysis did not reach RIS;however,it crossed the traditionalcriticalvalue and TSA criticalvalues,suggesting that the results were likely stable(Figure 4).
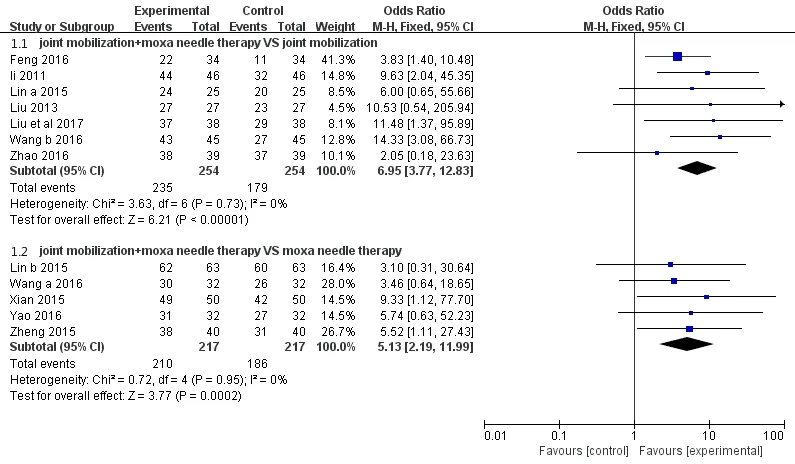
Figure 3 Forest map of total efficiency subgroup analysis

Figure 4 Total effective TSAresults
Clinical cure rate
Clinical cure rate was assessed in 14 studies[11-24],with 551 cases in the treatment group and 539 cases in the control group.There was no statistical heterogeneity among the studies(P=0.56,I2=0%);therefore,the fixed effect model was chosen.Meta-analysis revealed that warming acupuncture combined with joint mobilization significantly increased the cure rate[OR=2.84,95%CI(2.19,3.70),P<0.001].According to the different interventions in the control group,the included studies used subgroup analysis.Because the joint mobilization+warming acupuncture group vs.electroacupuncture+medium frequency therapy group only included 1 study[13],it was not included in the subgroup analysis.In 8 studies[11,12,14,18,20,21,22,24],warming acupuncture and joint mobilization were used in the treatment group(n=284),while in the control group used joint mobilization(n=284).There was no statistical heterogeneity among the studies(P=0.59,I2=0%);therefore, the fixed effect model was chosen.Meta-analysis revealed that warming acupuncture combined with mobilization of the joints significantly improved the cure rate[OR=3.73,95%CI(2.60,5.36),P<0.001].Five studies[15,16,17,19,23]used warming acupuncture+joint mobilization and warm needle acupuncture for comparison,with 217 cases in the treatment group and 217 cases in the control group.The test for heterogeneity revealed(P=0.99,I2=0%);therefore,a fixed effect model was used for analysis.Meta-analysis revealed statistically significant[OR=1.88,95%CI(1.22,2.88),P=0.004](Figure 5).TSA demonstrated that the RIS required to achieve significant test levels was 6014;however,the sample size(1090 cases)had not reached RIS.It passed through the traditionalcriticalvalue and TSA criticalvalues,indicating that warming acupuncture combine with joint mobilization was effective.The cure rate for mobilization of scapulohumeral periarthritis was verified and did not require further testing(Figure 6).
The number of treatments required for healing
The number of treatments required for healing was included as an outcome in 4 studies[11,13,22,24],which included 88 in the treatment group and 43 in the control group.There was no statistical heterogeneity among the studies(P=0.98,I2=0%);a fixed effect model was thus used.Meta-analysis revealed difference that was statistically significant[MD=-7.49,95%CI(-9.75,-5.23),P<0.001].Warm acupuncture and joint mobilization surgery reduced the number of treatments required for healing.According to the different interventions in the control group,included literature will do subgroup analysis;however,because the joint mobilization + warming acupuncture group vs.electroacupuncture+medium frequency therapy group included only 1 report[13],it was not included in the subgroup analysis.The three groups[11,22,24]used the warm acupuncture and joint mobilization surgery in the treatment group and joint mobilization surgery in the control group.There was no statistical heterogeneity among the studies(P=0.93,I2=0%).The fixed effect model was used;meta-analysis showed difference was statistically significant[MD=-7.63,95%CI(-10.18,-5.07),P<0.001](Figure 7).TSA revealed that the RIS required for the index to reach the significance level was 81 cases,and the sample size(131 cases)included in the study reached RIS,and it passed through the traditional boundary value and TSA critical values,indicating that warm acupuncture and moxibustion waseffective.Mobilization treatment for frozen shoulder can reduce the number of treatments required for healing for cure(Figure 8).
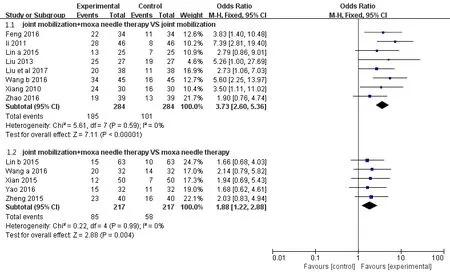
Figure 5 Forest map of subgroup of cure rate analysis
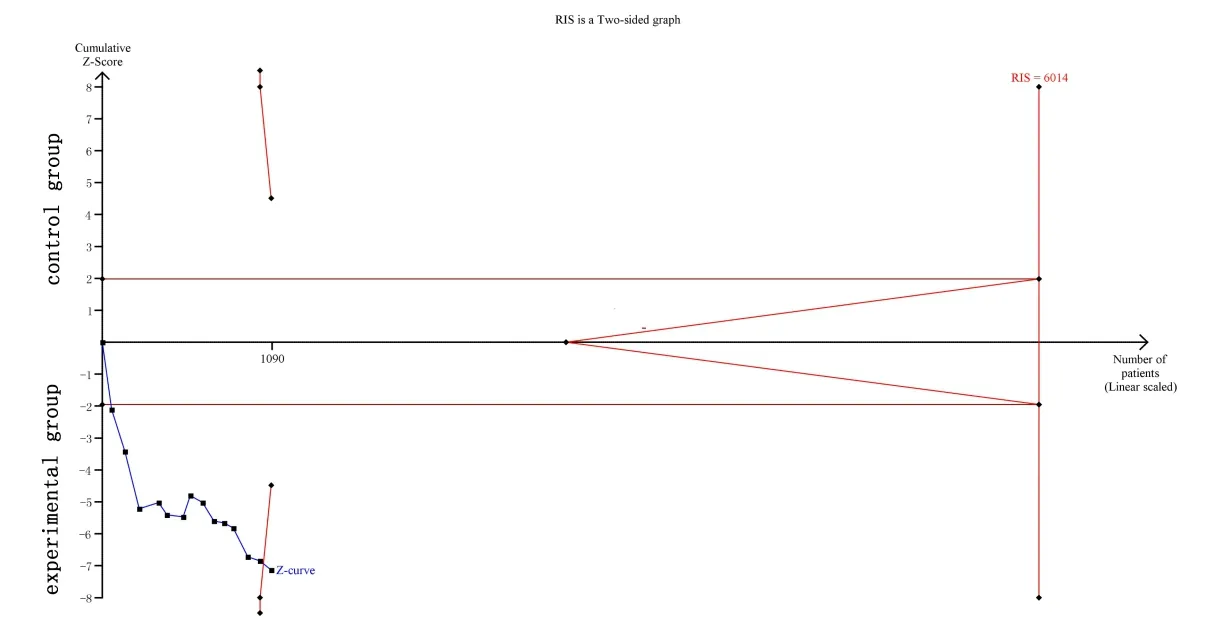
Figure 6 TSAresult of cure rate

Figure 7 Forest map of secondary subgroup analysis of the number of treatments required for healing
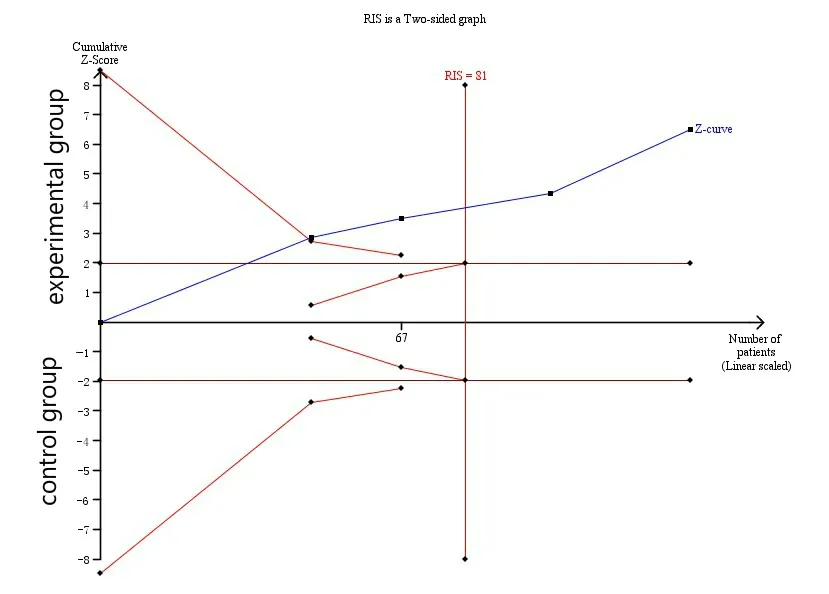
Figure 8 TSAresults for the number of treatments required for healing

Figure 9 Before and after treatment TSAresult of VAS score
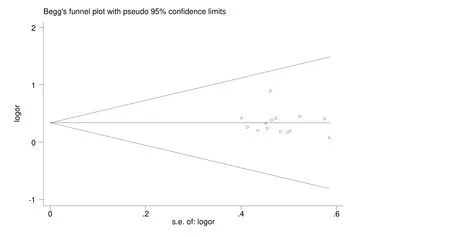
Figure 10 Funnel plot of Begg
VAS score
Outcomes based on VAS were included in 4 studies[12,16,18,23],of which 164 cases were in the treatment group and 164 cases in the control group.There were 2 studies[16,23]reporting VAS scores before and after treatment in the treatment and control groups.Meta-analysis results showed that[SMD=-2.01,95%CI(-2.37,-1.65),P<0.001],the difference was statistically significant.TSA revealed that the RIS required to reach the level of significance for this indicator was 137 cases,and the sample size(190 cases)included in the study reached RIS,and it passed through the traditional boundary value and TSA critical value,thus confirming the results of the meta-analysis(Figure 9).One study[12]reported VAS score after treatment in the treatment and control groups(P<0.001).One study[18]reported VAS scores in the treatment group before and after treatment(P<0.001),differences that were statistically significant.
Meta-analysis funnel diagram
Publication bias was evaluated for clinical cure rate.The result of Egger's linear regression wasP=0.352,and the result of the Begg rank correlation test wasP=0.26,suggesting that there was no publication bias.The Begg funnel diagram is shown in Figure 10.
Discussion
Scapulohumeral periarthritis belongs to the category of“leaky shoulder wind”and “shoulder pain”in TCM.Therefore,the method ofdredging the meridians,warming the circulation,dispersing cold,and activating blood circulation should be implemented in treatment[25].Warm acupuncture and moxibustion is a method that combines the efficacy of Qi and blood circulation that acupuncture and moxibustion has with the effect of warming meridians.The joint mobilization technique uses compression,distraction traction,long-axis traction,front-to-back swing,and internal and external swing to comprehensively perform activities with the patient's shoulder joint to promote the recovery of joint function.Though joint mobilization has a good effect only in relieving jointdysfunction,itseffecton dredging collaterals and relieving pain is poor[26].Warming acupuncture combined with joint mobilization to treat scapulohumeral periarthritis are mutually beneficial and can benefit patients,in whom shoulder function is better restored.
The present systematic review found that warming acupuncture combined with joint mobilization for the treatment of scapulohumeral periarthritis can not only effectively improve overall efficiency and cure rate,but also reduce the number of treatments required for healing and improve symptoms in patients with pain,which is worthy of clinical promotion.Meta-analysis is a process that quantitatively and comprehensively analyzes multiple studies with the same research subject.Its advantage lies in its ability to increase sample size and enhance the accuracy and robustness of results.However,traditional meta-analysis lacks attention to statistical performance.When the number of trials or the sample size was small,approximately 25%of the traditional meta-analysis result in false-positive conclusions due to random errors[27-28].If no statistically significant results are obtained,the intervention may be considered invalid,or it may lead to the conclusion that further relevant research needs to be conducted.However,it cannot be confirmed whether the result is due to the fact that the intervention is truly ineffective or due to a false-negative result because of an insufficient sample size.In addition,meta-analyses need to be updated as new studies are published,and repeated statistical tests increase the risk for type I errors(i.e.,false positives).In this study,TSA was used to avoid similar errors and make the results more credible.
Some limitations of this study should be addressed.The quality of the literature included in this study was low,none of the studies described the use of hidden and blinded allocations.Nine studies[12-15,17-21]only referred to randomization without detailed explanation of the randomization method,which increases the risk for selection bias,and measurement and evaluation of trial bias,which in turn affect the reliability of the conclusion.The included studies for acupuncture points were not uniform,only 5 studies[16,17,19,23,24]selected acupoints based on dialectical treatment,which has a certain impact on the evaluation of the results.Clinical evaluation indicators were mostly limited to the evaluation of efficacy.There was little attention devoted to the movement of the shoulder joint,quality of life and recurrence rate of the disease,and a lack of long-term follow-up studies.
Meta-analysis is a comprehensive analysis of RCT,and the quality of the literature determines the credibility of the conclusions.High-quality meta-analysis results are the highest level of evidence. Therefore, more standardized and scientific design should be incorporated in future studies,including multicenter,randomized,double-blind investigations.Periarthritis of the shoulder can be divided into wind-cold-damp impediment,syndrome of congealing cold with blood stasis,and dual vacuity ofQiand blood.Theuseofsyndrome differentiation can highlight the advantages of TCM.Follow-up was strengthens focus on patient quality of life and the recurrence rate of the disease to objectively evaluate efficacy.Estimates in advance of how many samples meet the research requirements can save our medical resources.
In summary,the modern rehabilitation therapy involving jointmobilization combined with TCM including warming acupuncture hasbeen evaluated through strict evaluation methods based on evidence-based medicine.We can be relatively confident that warming acupuncture combined with joint mobilization surgery is effective for the treatment of scapulohumeral periarthritis.In addition,we used TSA to avoid the occurrence of type I errors due to the lack of data and repeated testing.According to the stability of the results,we determined from the RIS that the test results achieved stability,and provide a good reference for future research and clinical guidance.
:
1. Guo Y,Guo JH.Progress of clinical rehabilitation treatment of frozen shoulder.Med Review 2014,20:2752-2754.
2. Shi MH. Therapeutic effect observation of penetrating acupuncture combined with warm needle in treating periarthritis of shoulder.Shanghai J Acupunc Moxibustion 2010,1:36-37.
3. Wang MM,Cai SC.Clinical research of acupuncture and moxibustion treatmentof periarthritis of shoulder.Chin J Med 2016,7:918-921.
4. Quan K,Jin PC,Quan HX,et al.Meta-analysis of randomized controlled clinical study literature of warm acupuncture and moxibustion for treatment of periarthritis of the shoulder.Henan J Tradit Chin Med 2014,34:2277-2279.
5. Qian H,Zhao JN,Bao NR.Treatment progress of frozen shoulder.J Cervical Low Back Pain 2017,38:69-72.
6. Tao R,Wang J,Li HQ,et al.Observation of the efficacy of buprenorphine combined with loosening of the joints in treating periarthritis of shoulder.Chinese J Physical Med Rehabilitation 2017,39:137-141.
7. Farrel CM,Sperling JW,Cofield RH.Manipulation for frozen shoulder:long-term results.J Shoulder Elbow Surg 2005,14:480-484.
8. Xu Y,Zhang W,Liu ZL,et al.Progress in Chinese treatment of frozen shoulder.World J IntegrTradit Western Med 2016,11:1619-1623.
9. State Administration of Traditional Chinese Medicine.Diagnostic Criteria forDiseasesin Traditional Chinese Medicine.Nanjing:Nanjing University Press,1994.
10.Zheng XY.Guiding principles for clinical research of new Chinese drugs.China Medical Science and Technology Press,2002.
11.Liu JX.Clinical efficacy of shoulder loosening combined with warm acupuncture moxibustion in the treatment of periarthritis of shoulder.Inner Mongolia J Tradit Chin Med 2017,36:118-119.
12.Zhao X.Comparativeanalysisoftheclinical efficacy of warm-needle acupuncture and joint loosening surgery for frozen shoulder. Med Education China 2016,1:172-174.
13.Zhou GX.Therapeutic effect of shoulder joint loosening and warm acupuncture moxibustion on frozen shoulder.Med Review 2011,17:2862-2864.
14.Liu X.Warming acupuncturecombined with loosening of joints for treatment of scapulohumeral periarthritis in 27 cases.Chin Med Modern Distance Education China 2013,7:45-46.
15.Zheng CY. Clinical observation of warm acupuncture moxibustion combined with loosening of joints for treatment of frozen shoulder.J Massage Rehabilit Med 2015,6:31-32.
16.Lin ZL,Zhou XJ,Lai JY.Clinical study of warm acupuncture combined with loosening of joints for treatment of frozen shoulder.Chin J Rehab Theory Practice 2011,17:997-998.
17.Xian YB.Clinicalefficacy analysisofwarm acupuncture and joint loosening surgery for periarthritis of shoulder.Clin J Integrated Tradit Chin Western Med 2015,11:68-69.
18.Xiang J.Observation ofclinicalefficacy of warm-needle acupuncture and joint loosening surgery for frozen shoulder.Community Physician of China:J Med 2010,17:119-120.
19.Wang K.Observation of the clinical curative effect of warm-needle acupuncture and joint loosening surgery for periarthritis of shoulder.J People Health 2016,14:38.
20.Wang XL.Clinical observation of warm-needle acupuncture and joint loosening surgery for frozen shoulderJ.Shanxi J Tradit Chin Med 2016,2:39-40.
21.Li YF.Treatment of 46 Cases of periarthritis of shoulder with warm acupuncture and joint loosing.Inner Mongolia J Tradit Chin Med 2011,30:24-25.
22.Lin BH,Yang L,Wan Z,et al.Therapeutic effect analysis of warm acupuncture moxibustion combined with loosening ofjoints in treating periarthritis of shoulder.J Practical Tradit Chin Med 2015,6:562-563.
23.Yao RJ.Observation of the clinical curative effect of warm acupuncturemoxibustion combinedwith loosening of joints for treatment of periarthritis of shoulder.Asia Pacific Tradit Med 2016,12:122-123.
24.Feng YT,Sheng YM.Clinical observation of warm acupuncture and moxibustion assisted shoulder joint loosening surgery for frozen shoulder.Chin J Ethno Folk Med 2016,23:93-94.
25.Zhao MM.Application of warm acupuncture and moxibustion combined with shoulder arthrodesis in periarthritis of shoulder.J Liaoning University Tradit Chin Med 2017,4:1.
26.Xu J,Li YX,Zheng Hong,et al.Observation of the clinical efficacy of warm acupuncture and moxibustion in the treatment of frozen shoulder.Med HealthAbstracts 2016,1:192.
27.Thorlund K,Devereaux PJ,Wetterslev J,et al.Can trial sequentialmonitoring boundaries reduce spurious inferences from metaanalyses.IntJ Epidemiol 2009,38:276-286.
28.Trikalinos TA,Churchill R,Ferri M,et al.Effect sizes in cumulative meta-analyses of mental health randomized trials evolved over time.Clin Epidemiol 2004,57:1124-1130.
猜你喜欢
杂志排行

TMR Non-Drug Therapy的其它文章
- Pricking cupping bloodletting combined with slide cupping for acne:a case report
- Effects ofmidwife-led psychologicalintervention on delivery outcomes:a meta-analysis
- Based on the theory of traditional Chinese and western medicine for the co-treatment of neck,chest,and waist
- Efficacy of Liuzijue respiratory exercise in patients with chronic obstructive pulmonary disease:a meta-analysis