Efficacy of Liuzijue respiratory exercise in patients with chronic obstructive pulmonary disease:a meta-analysis
2018-09-14TingTingLiuMengJieLeiHuiPingWangYanQiuHuangChangDeJin
Ting-Ting Liu,Meng-Jie Lei,Hui-Ping Wang,Yan-Qiu Huang,Chang-De Jin
1Tianjin University of Traditional Chinese Medicine,School of Postgraduate,Tianjin,China.
2Tianjin University of Traditional Chinese Medicine,School of Nursing,Tianjin,China.
Introduction
Chronic obstructive pulmonary disease(COPD),a destructive lung disease,is characterized by airflow limitation that is not fully reversible.The airflow limitation is associated with an abnormal inflammatory responseofthelungsto noxious particles or gases and is typically progressive[1].The high prevalence,morbidity,and mortality of COPD pose a sudstantial economic burden on the people and society[2].Although guidelines for COPD diagnosis and treatmentathomeand abroad havebeen continuously updated and its methods of prevention and rehabilitation have made some progress,the current therapy using chemical drugs is limited;therefore,most drugs are only used for the treatment of symptoms and have side effects[3].
Liuzijue is a health-preserving method that originated in ancient China.Liuzijue,characterized by diaphragmatic breathing and pursed lip breathing,is performed via expiration by producing six sounds,namely Xu(嘘),He(呵),Hu(呼),Si(呬),Chui(吹),and Xi(嘻),corresponding to limb movements,thereby guiding the operation of different Zangfu organs,meridians,and collaterals as well as the Qi and blood[4].As early as the Qin and Han dynasties,the treatment of pulmonary diseases with guided breathing has already been recorded in the ancient book ofLüshichunqiu(B.C.239, Warring States).Gongjuzhong also stated inHongludianxue(A.D.1380,Ming Dynasty)that Liuzijue could adjust and control the breath as well as improve lung functions.
As a low-intensity aerobic exercise of the non-drug traditional Chinese medicine therapy,the effectiveness and safety of Liuzijue exercise performed in patients with COPD have also been confirmed in some studies[5-6].However,the effects observed in other researches differed from each other,and Liuzijue respiratory exercise has not yet been widely used in clinical practice[7-8].Thus,the present meta-analysis was conducted to authenticate the efficacy of Liuzijue respiratory exercise in patients with COPD and provide evidence for clinical practice.
Materials and methods
Search strategy
A search of the Cochrane Library databases,Pubmed,Embase,Web of Science,CNKI,Wangfang,VIP and CBM,was performed using the following terms:“chronic obstructive pulmonary disease”, “COPD”,“pulmonary disease,chronic obstructive”, “chronic obstructive lung disease”, “bronchitis,chronic”,“emphysema”, “chronic airflow obstruction”,“Liuzijue”, “six character formula*”, “six letters formula*”, “six strategies”,and “TCM pulmonary rehabilitation exercise”.Subject terms and free words were combined,and the searching date was until May 2018.Potentially eligible citations from the retrieved articles were reviewed to identify additional relevant studies.No language orotherrestrictionswere imposed.
Inclusion criteria
Studies would be included in the following criteria were met:(1)Subjects were patients diagnosed with COPD according to the“Guidelines for the diagnosis and treatment of COPD (established by Chinese Medical Association)”which confirmed the air-flow limitation of less than 70%in the predicted value of forced expiratory volume in 1 second(FEV1)after inhaling a bronchodilator[9-10];(2)Intervention was Liuzijue respiratory exercise;(3)Intervention duration was at least 3 months;(4)Control was managed with conventional health education or whole-body respiratory exercise; (5)The study design was randomized controlled trials(RCTs).
Exclusion criteria
Studies wereexcluded ifany ofthefollowing exclusion criteria were met:(1)Intervention was the combination of Liuzijue and other special measures,such as message,resistance training,and acupoint sticking,among others;(2)Repeated published articles;(3)Research quality was rated as“C”;(4)Incomplete outcome data and not available even after contacting its author;(5)Subjects who were in acute phase,under open surgery,or teenagers.
Study interventions
Intervention groups took the measure of Liuzijue respiratory exercise, which was done through expiration by producing six different sounds(Xu,He,Hu,Si,Chui,and Xi)and combined with simple limb activity [4].Controlgroups took measures of conventional care or whole-body respiratory exercise.Conventional care included health education,drug therapy,and oxygen therapy,among others[11-12].The whole-body respiratory exercise was performed with upper limb,lateral bending,and swivel activities based on abdominal and pursed lip breathing[13].To ensure the clinical homogeneity,we divided the included studies into two subgroups:“Liuzijue respiratory exercise vs.conventionalcare”and“Liuzijue respiratory exercise vs. whole-body respiratory exercise”.
Study selection and data extraction
The title and abstract of each search result were screened to identify potential studies first,and then full texts were screened to determine studies that met the inclusion criteria.Two independent reviewers performed screening and evaluation.Disagreements were resolved by discussion between the two reviewers.If the disagreement could not be resolved,another experienced reviewer made the final decision.
The following data were extracted from the eligible studies:author information,year of publication,study design, population, gender, age, sample size,intervention,control,duration of the intervention,the frequency of the intervention,and outcome data.
Outcome measures
The primary outcomes were lung function or functional capacity,and secondary outcomes involved quality of life and effectiveness rate.All outcomes were measured at the point of intervention finished(3 or 6 months).Test methods and evaluation standards for each outcome were shown in Table 1.
Statistical analysis
The weighted mean difference (WMD) (or standardized mean difference)and 95%confidence interval(CI)were used for continuous variables,and relative risk and 95%CI were used for dichotomous variables.The I2was calculated as an index of heterogeneity between studies.If the I2was less than 50%,a fixed-effect model was used.If the I2was more than 50%,a random-effect model was used.Analyses were performed using Review Manager 5.3.
Quality assessment and risk of bias
Study quality and risk of bias were assessed via the Cochrane Randomized Controlled Trial Bias Risk Tool,which contained seven assessment domains related to random sequence generation,allocation concealment,blinding of participants and personnel,blinding of outcome assessment,incomplete outcome data,selective reporting,and other biases.Each domain was assessed as low,high,or unclear risk of bias[16].Two reviewers independently evaluated these items.
Results
Search results and description of studies
Our search process yielded 232 potentially relevant studies,excluding 94 duplicate studies.After screening the titles and abstracts,56 articles were selected for full-text review.Among these,11 studies including 915 patients with COPD were eligible for meta-analysis, consisting of 459 patients in intervention groups and 456 in control groups.The search process is shown in Figure 1.Among the final 11 studies,7 were comparing Liuzijue respiratory exercise and conventional care[5,7,11,12,17-19],and the other 4 studies were comparing Liuzijue respiratory exercise and whole-body respiratory exercise[13-15,20].
Characteristics and quality assessment of included studies
The main characteristics of the included studies are shown in Table 2.The quality of studies included in this meta-analysis was all grades B according to the Cochrane Randomized Controlled Trial Bias Risk Tool.Eight of the 11 studies correctly reported random sequence generation methods and processes[7,12-14,17-20],and only Shen’study reported allocation concealment[7].Due to the particularity of the intervention,implementing blinding methods on the patients and researchers is difficult.Two studies reported the blinding of outcome measures[5,20].Although some of these studies did not implement the blinding method[7,11,14,19],their outcomes[FEV1,FEV1%pred,FEV1/FVC%(Forced vital capacity),and 6-min walk distance]were measured by objective instruments and subjectively slightly influenced by individuals;therefore,we rated them as low risk.Three of the studies that had withdrawal cases did not do intention-to-treat analysis,and the cases that withdrawn were uncoordinated[11,12,18];therefore,they were assessed as high risk of incomplete outcome data.No obvious alternative reporting and other biases were found in all studies.Detailed information on the quality assessment is shown in Figures 2 and 3.
Outcomes
FEV1
Among the 11 included studies,6 reported the effect on FEV1,which included 396 patients with 200 in the intervention groups and 196 in the control groups[7,11-14,18].Among these,4 studies compared the“Liuzijue respiratory exercise and conventional care”and 2 studies compared“Liuzijue respiratory exercise and whole-body respiratory exercise”(Figure 4).The random-effect model was used to merge the WMD values,and the pooled effect size in favor of Liuzijue was 0.18[95%CI(0.06,0.3)]and-0.02[95%CI(-0.14,-0.11)]in two subgroups,respectively,which means that Liuzijue improved the FEV1 in patients with COPD compared with conventional care,but had no difference compared with the whole-body respiratory exercise.I2in each subgroup was much lower than that in the total group(49%,0%,vs.60%),which suggested thatthe difference ofcontrol measures may be the main reason for heterogeneity.
FEV1%pred
Among the 11 included studies,5 reported the effect on FEV1%pred,which included 305 patients with 155 in the intervention groups and 150 in the control groups[11,13,14,18,19].Among these,3 studies compared “Liuzijue respiratory exercise and conventional care,”and 2 studies compared “Liuzijue respiratory exercise and whole-body respiratory exercise”(Figure 5).The random-effect model was used to merge the WMD values,and the pooled effect size in favor of Liuzijue was 10.21[95%CI(7.25,13.18)]and-1.27[95%CI(-5.06,-2.52)]in two subgroups,respectively,which means that Liuzijue improved the FEV1%pred in patients with COPD compared with conventionalcare,buthad no difference compared with the whole-body respiratory exercise.I2in each subgroup was much lower than that in the total group(25%,0%,vs.89%),which suggested that the difference of control measures may be the main reason for heterogeneity.
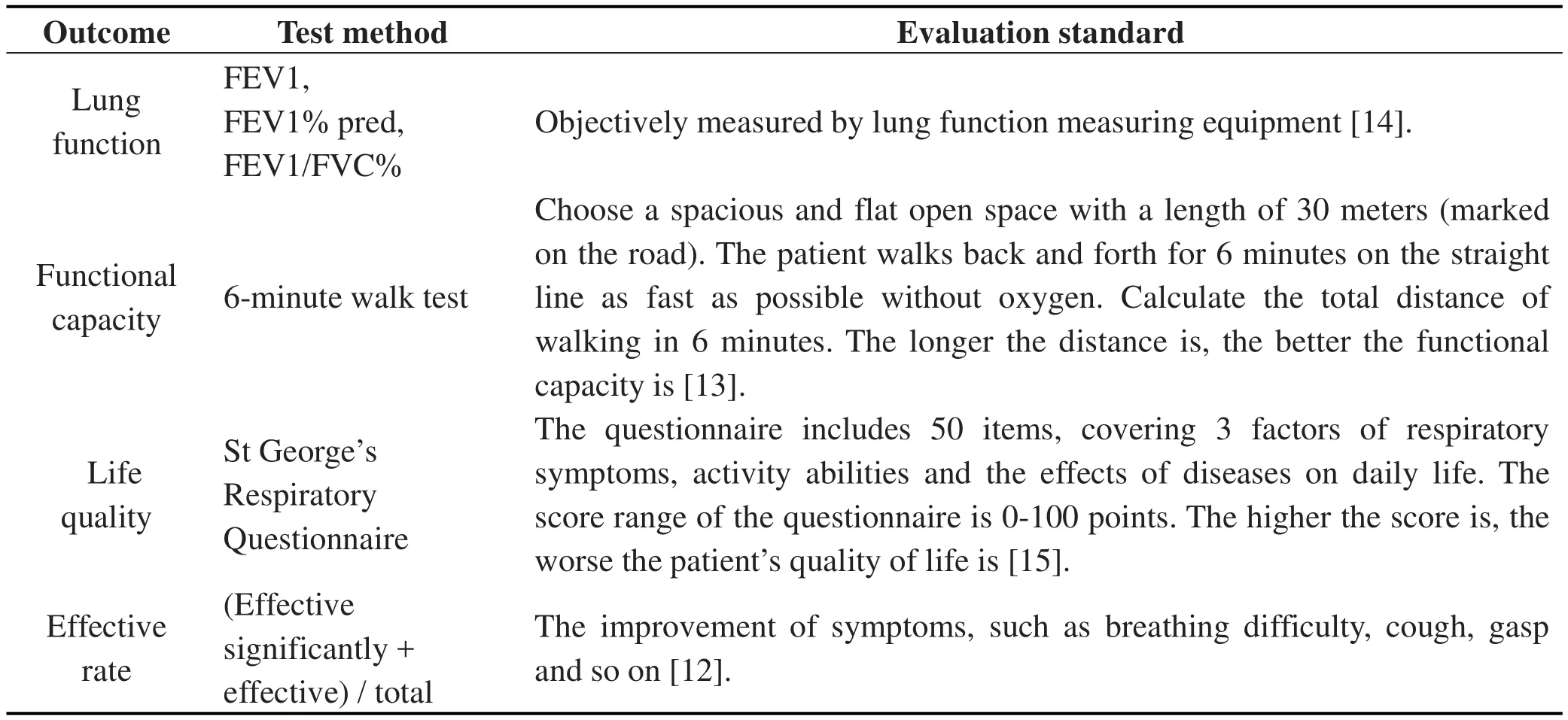
Table1 Test method and evaluation standard for each outcome
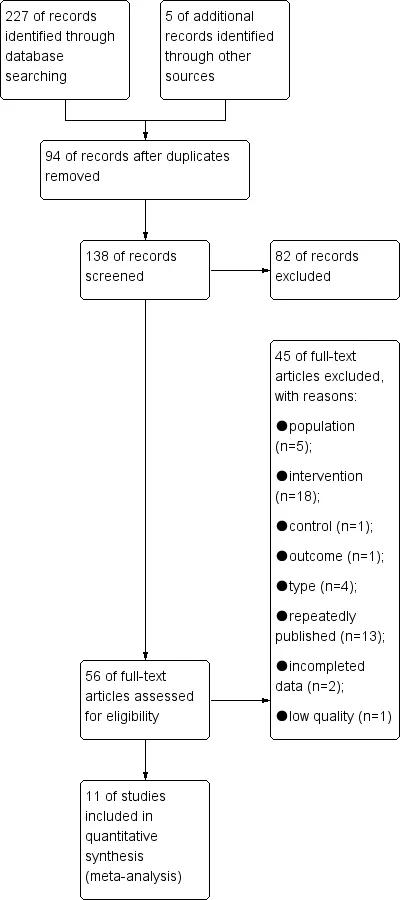
Figure 1 Flowchart of the systematic search process
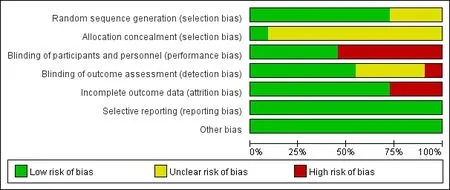
Figure 2 Risk of bias graph

Figure 3 Risk of bias summary
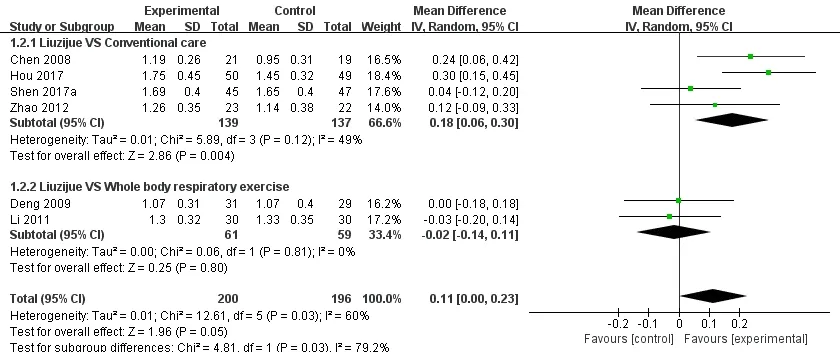
Figure 4 Effect of Liuzijue on FEV1
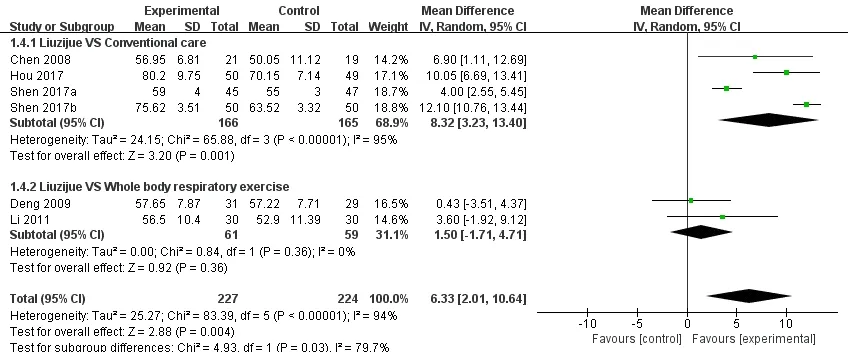
Figure 5 Effect of Liuzijue on FEV1%pred
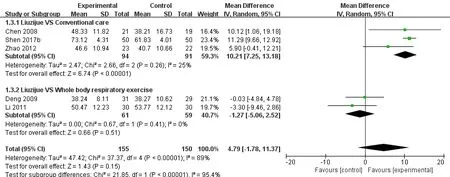
Figure 6 Effect of Liuzijue on FEV1/FVC%

Table 2 Characteristics of included studies
FEV1/FVC%
Among the 11 included studies,6 reported the effect on FEV1/FVC%,which included 451 patients with 227 in the intervention groups and 224 in the control groups[7,12-14,18,19].Among these,4 studies compared “Liuzijue respiratory exercise and conventional care,”and 2 studies compared“Liuzijue respiratory exercise and whole-body respiratory exercise”(Figure 6).A random-effect model was used.The pooled effect size in“Liuzijue respiratory exercise vs.conventional care”subgroup was 8.32[95%CI(3.23,13.4)],whereas in“Liuzijue respiratory exercise vs.whole-body respiratory exercise”subgroup,it was 1.50[95%CI(-1.71,-4.71)].The result revealed that Liuzijue improved the FEV1/FVC%in patients with COPD compared with conventionalcare,buthad no difference compared with the whole-body respiratory exercise.The reasons for heterogeneity were unclear.
6-minute walk test
Among the 11 included studies,4 reported the effect on 6-min walk test,which included 352 patients with 178 in the intervention groups and 174 in the control groups[5,11,13,20].Among these,2 studies compared “Liuzijue respiratory exercise and conventional care,”and 2 studies compared“Liuzijue respiratory exercise and whole-body respiratory exercise”(Figure 7).The random-effect model was used to merge the WMD values,and the pooled effect size in favor of Liuzijue was 10.97[95%CI(5.81,16.12)]and 37.82[95%CI(6.51,69.13)]in two subgroups respectively,which means that Liuzijue improved the functional capacity in patients with COPD compared with either conventional care or whole-body respiratory exercise.I2in each subgroup was much lower than that in the total group(0%,42%,vs.56%),which suggested that the difference of control measures may be the main reason for heterogeneity.
St George's respiratory questionnaire
Among the 11 included studies,4 reported the effect on quality of life,which included 322 patients with 162 in the intervention groups and 160 in the control groups[12,13,15,17].Among these,2 studies compared “Liuzijue respiratory exercise and conventional care,”and 2 studies compared“Liuzijue respiratory exercise vs. whole-body respiratory exercise”(Figure 8).The random-effect model was used to merge the WMD values,and the pooled effect size in favor of Liuzijue was-10.07[95%CI(-12.84,-7.30)]and-2.67[95%CI(-6.71,1.36)]in the two subgroups,respectively,which means that Liuzijue improved the quality of life in patients with COPD compared with those who received conventional care,but had no difference compared with the whole-body respiratory exercise.I2in each subgroup was much lower than that in the total group(0%,0%,vs.66%),which suggested that the difference of control measures may be the main reason for heterogeneity.
Effectiveness rate
Among the 11 included studies,2 reported the effects on effectiveness rate,which included 142 patients with 75 in the intervention groups and 67 in the control groups(Figure 9)[12,17].All 2 studies compared “Liuzijue respiratory exercise and conventional care.”The result showed that effectiveness rate of Liuzijue was higher than that of conventionalcare,butthe difference wasnot significant,indicating a need for more studies to examine the effectiveness rate of Liuzijue.
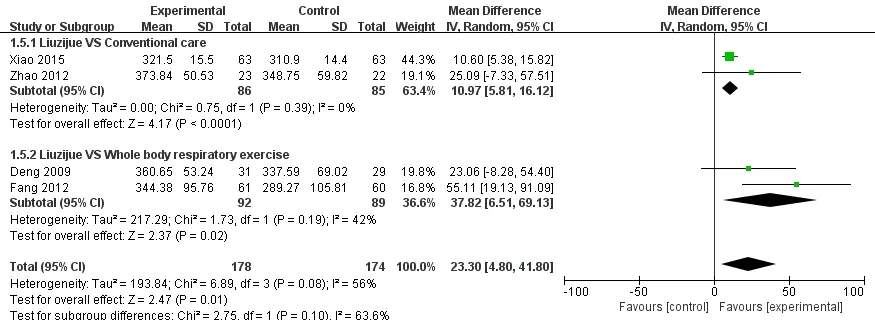
Figure 7 Effect of Liuzijue on 6-minute walk test
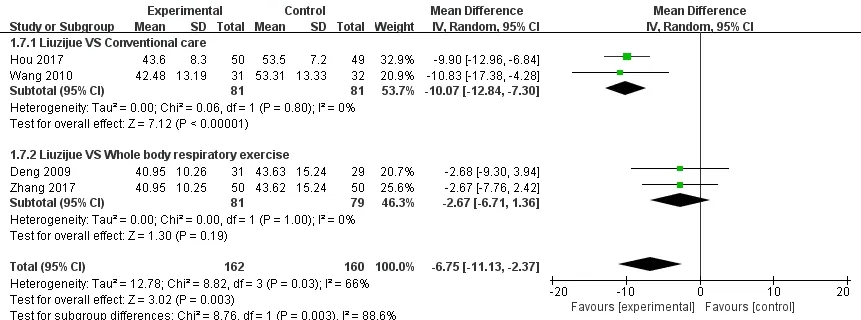
Figure 8 Effect of Liuzijue on St George's respiratory questionnaire
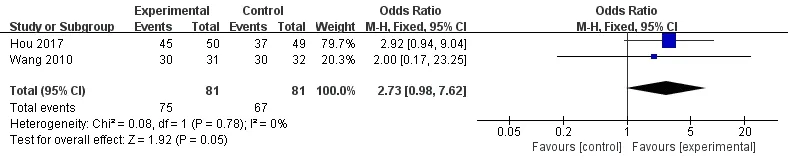
Figure 9 Effect of Liuzijue on the effective rate
Discussion
Rapid shallow breathing is the characteristic breathing pattern in patients with COPD.Controlled breathing techniques,such as abdominal breathing and pursed lip breathing,have long been incorporated as treatment components in pulmonary rehabilitation programs[21].Liuzijue,as a traditional Chinese respiratory exercise,is a method to control the breath.It can not only produce increased asynchronousand paradoxical breathing movements but also prolong expiration and slow breathing rate.As shown in our results,Liuzijue has a more satisfactory effect on lung function than conventionalcare,which isconsistentwith the previous study [22].The whole-body respiratory exercise also includes controlled breathing exercise,which may be why no significant differences in lung function were observed between Liuzijue and whole-body respiratory exercise.However,Liuzijue is a more simple and easy to grasp breathing pattern and is more commonly recommended in clinical practice.
Liuzijue originates from traditional Chinese Qigong,which are low-intensity physical activities with a mean induced maximum heart rate ranging from 43%to 49% of the predicted maximum heart rate and estimated metabolic equivalents ranging from 1.5 to 2.6[23-25].Therefore,this should be a physiological mechanism to explain how Liuzijue improved the functional capacity of the participants.Low-intensity regular physical activities,in addition to having less chance of inducing muscle damage,may have a modulation effect on low-level inflammation,which was demonstrated in patientswith diabetes and cardiovasculardiseases [26-27].Improvementin overall health status upon the modulation of the chronicsystematicinflammationin COPD may explain why Liuzijue as a low-intensity physical activity improved the functional capacity in patients with COPD.
In addition,the character “Hu”in the Liuzijue respiratory exercise corresponds to the person’s spleen in Chinese medicine.The training of the “Hu”character helps enhance the function of the spleen,helps food digestion,allows the blood to be transported to various organs,and nourished the skeletal muscles,thereby strengthening the bones and enhancing functional capacity[13,18].Moreover,during the training process,Liuzijue respiratory exercise also cooperates with limb flexion,extension,rotation,and other actions to make the limb flexible and balanced,which helps increase the stability of limb activity and increase the activity time in patients with COPD[28].Therefore,these may be the main reasons why Liuzijue respiratory exercise has a better effect than whole-body respiratory exercise to improve the functional capacity of patients with COPD.
The quality of life index in patients with COPD is closely related to their lung function.With the improvement of lung function and the reduction of airflow limitation symptoms in patients with COPD,the quality of life index will also be improved[29].Mood problems(e.g.,depression and anxiety)are strongly associated with chronic respiratory diseases[30,31].The severity of psychosocial stress in individuals with a respiratory disease has a direct effect on quality of life[32].In traditional Chinese medicine,Qigong has long been considered a pattern of mind-body intervention that simultaneously exercises the mind and body for the treatment of various chronic diseases and promotion of healthy life[33].This phenomenon was also found in Guan’study,which showed that Liuzijue exercise,can be used for body,breath,and mood adjustments.In addition,long-term practice helps stabilize the patient’s mood,calms the mind,and relieves anxiety,thereby improves their quality of life[34].Therefore,Liuzijue can more effectively improve the quality of life in patients with COPD compared with the conventional care.Because the whole-body breathing can also improve the lung function in patients with COPD,the quality of life in patients who underwent whole-body breath exercises may also improve,which may be the reason why the difference in the quality of life between the two groups was not significant.As a traditional Chinese Qigong,Liuzijue has more advantages in mood adjustment;thus,it is more recommended than the whole-body respiratory exercise[33].
The effectiveness rate of Liuzijue was higher than that of conventional care,but the difference was not significant.One possible reason for it is that the number of included studies was small with only 2 studies and 81 patients.Therefore,more studies should be conducted to examine the effectiveness rate of Liuzijue.Moreover,patients’effectiveness rate was subjectively evaluated through symptom improvement;hence,different investigators may rate it as different results,which may also influence our results[12].
Conclusion
Compared with the conventionalcare,Liuzijue respiratory exercise could improve the lung function,functional capacity,and quality of life in patients with COPD.When compared with the whole-body breathing exercise,Liuzijue could improve the functional capacity in patients with COPD,but has no differences in lung function and quality of life.As the conclusion of this meta-analysis was drawn based on middle-quality RCTs,more large-sample,high-quality,multicenter RCTs are still needed for its verification in the future.
:
1. Celli BR,MacNee W,Agusti A,et al.Standards for the diagnosis and treatment of patients with COPD:a summary of the ATS/ERS position paper.Eur Respir J 2004,23:932-946.
2. Lopez A,Shibuya K,Rao C,et al.Chronic obstructive pulmonary disease:current burden and future projections.Eur Respir J 2006,27:397-412.
3. Qi YJ,He ZY.New progress in drug therapy for chronic obstructive pulmonary disease.Chin J Clin Med 2017,45:12-14.
4. Association CHQ.Chinese Health Qigong-Liu Zi Jue.Beijing:Chinese Health Qigong Association,2007.
5. Xiao CM,Zhuang YC.Efficacy of Liuzijue Qigong in individuals with chronic obstructive pulmonary disease in remission.J Am Geriatr Soc 2015,63:1420-1425.
6. Wu W,Liu X,Liu J,et al.Effectiveness of water-based Liuzijue exercise on respiratory muscle strength and peripheral skeletal muscle function in patients with COPD.Int J Chron Obstruct Pulmon Dis 2018,13:1713-1726.
7. Shen Q.Study on the influence of"Liuzijue"exercise on patients with stable COPD(grade I).J External Ther TCM 2017,26:3-6.
8. Zhao DX.Rehabilitation of modified exercise prescription forelderly patientswith stable COPD.Guangzhou Medical University 2011.
9. Chinese Medical Association Respiratory Disease Society Chronic Obstructive Pulmonary Disease Group.Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease(revised edition 2013).Chinese J Tuberc Respir D 2013,36:255-264.
10.Chinese Medical Association Respiratory Disease Society Chronic Obstructive Pulmonary Disease Group.Guidelines for the diagnosis and treatment of chronic obstructive pulmonary disease(revised edition 2007).Chinese J Tuberc Respir D 2007,30:8-17.
11.Zhao DX,Zhou YM,Li FL,et al.Rehabilitation of modified exercise prescription for patients with stable chronic obstructive pulmonary disease.Int J Respir 2012,32:678-682.
12.Hou MY,Cui XP.The observation on the simplify Six-character formula on the survival quality in Qi deficiency of lung and kidney syndrome patients with COPD.Guangming J Chin Med 2017,32:3518-3521.
13.Deng LJ.The effects of Six-character formula respiratory gymnastics in stable patients with COPD.Fujian Univ TCM 2009,1:8-22.
14.Li DX.The effect of Six-character formula respiratory gymnastics in relation to respiratory mechanics in patients with chronic obstructive pulmonary disease.Fujian Univ TCM 2011,23:9-23.
15.Zhang J,Lu XQ.Effect of health education combined with respiratory exercise on pulmonary function of COPD patients.J Clin Lab 2017,6:522-523.
16.Higgins JPT,Green S.Cochrane handbook for systematic reviews of interventions.Cochrane Collaboration 2011,102:182-234.
17.Wang ZW,Yang PL,Tang J,et al.Effects of“Six Letters Formula”on quality of life and syndrome of traditional Chinese medicine in patientswith chronic obstructive pulmonary disease.Sh J TCM 2010,44:54-59.
18.ChenJX,ZhangWX,ZhengGH,etal.Application of Liuzijue exercise in pulmonary rehabilitation of chronic obstructive pulmonary disease patients.J FJ Univ TCM 2008,18:3-4.
19.Shen Q.A community intervention study on treating COPD stabilization(level I)in elderly patients by “six strategics”health exercises.Clin J Chin Med 2017,9:23-25.
20.Fang DP,Liu Y,Zhu XL,et al.Application and effects of six-character formula respiratory gymnastics in continuous nursing for stable patients with COPD.J Nurs Admin 2012,12:813-815.
21.Borge CR,Hagen KB,Mengshoel AM,et al.Effects of controlled breathing exercises and respiratory muscle training in people with chronic obstructive pulmonary disease:resultsfrom evaluating the quality of evidence in systematic.BMC Pulm Med 2014,14:1-15.
22.Jing JH,Qiu XH,Qin YX,et al.Comparative study of the influences of Liuzijue and Ba Duan Jin on college students.Hubei Sport Sci 2013,32:1056-1059.
23.Xiao ZC.A brief talk on the true essence of Tao Hongjing's"Six Characters".Dong Fang Qigong 2000,2:10-11.
24.Lan C,Chou SW,Chen SY,et al.The aerobic capacity and ventilatory efficiency during exercise in Qigong and Tai Chi Quan practitioners.Am J Chin Med 2004,32:141-150.
25.ChaoYF,ChenSY,LanC,etal.The cardiorespiratory response and energy expenditure of Tai-Chi-Qui-Gong.Am J Chin Med 2002,30:451-461.
26.Nimmo MA,Leggate M,Viana JL,et al.The effectofphysicalactivity on mediatorsof inflammation.Diabetes Obes Metab 2013,15:51-60.
27.Lavie CJ,Church TS,Milani RV,et al.Impact of physical activity,cardiorespiratory fitness,and exercise training on markers of inflammation.J Cardiopulm Rehabil Prev 2011,31:137-145.
28.Jing JH,Qiu XH,Qin YX,et al.Comparative study of the influences of Liuzijue and Ba Duan Jin on college students.Hubei Sport Sci 2013,32:1056-1059.
29.Wijkstra P,TenVergert E,Mark T,et al.Relation of lung function,maximal inspiratory pressure,dyspnoea,and quality of life with exercise capacity in patients with chronic obstructive pulmonary disease.Thorax 1994,49:468-472.
30.Panagioti M,Scott C,Blakemore A,et al.Overview of the prevalence,impact,and management of depression and anxiety in chronic obstructive pulmonary disease.IntJChron Obstruct Pulmon Dis 2014,2014:1289-1306.
31.Yohannes AM,Alexopoulos GS.Depression and anxiety in patients with COPD.Eur Respir Rev 2014,23:345-349.
32.Kullowatz A,Rosenfield D,Dahme B,et al.Stress effects on lung function in asthma are mediated by changes in airway inflammation.Psychosom Med 2008,70:468-475.
33.Tsang HW,Tsang WW,Jones AY,et al.Psycho-physical and neurophysiological effects of qigong on depressed elders with chronic illness.Aging Ment Health 2013,17:336-348.
34.Guan FG,Wang T,Liu XZ.Effects of“Si”tactic of breathing exercises on the quality of life in patients with COPD in stable phase.Guangming J Chin Med 2014,29:1190-1192.
杂志排行

TMR Non-Drug Therapy的其它文章
- Pricking cupping bloodletting combined with slide cupping for acne:a case report
- Effects ofmidwife-led psychologicalintervention on delivery outcomes:a meta-analysis
- Systematicevaluationand trialsequentialanalysisofwarming acupuncture combined with joint mobilization in the treatment of scapulohumeral periarthritis
- Based on the theory of traditional Chinese and western medicine for the co-treatment of neck,chest,and waist