肠息肉介入治疗后复发危险因素的Logistic回归分析
2018-06-29
宜都市第一人民医院消化内科,湖北 宜都 443300
【Abstract】ObjectiveTo investigate the risk factors of the recurrence after interventional treatment of intestinal polys.MethodsOne hundred and thirty-six cases of adenomatous polyps were selected, all taken the endoscopic intestinal polyps electrocoagulation surgery. Patients were divided into relapse group (n=52) and non-recurrence group (n=84) according to the results of the follow-up. The general data (gender, age, the number of intestinal polyps, the size of intestinal polyps, the location of intestinal polyps, histological types) of the relapse group and non-recurrence group were compared, and multivariate Logistic regression analysis was performed. TheROCcurve was used to predict the value of the above factors in predicting the risk of the recurrence after interventional treatment of intestinal polys.ResultsThere was no significant difference in the location of intestinal polyps between two groups (P>0.05). In the relapse group, the proportion of male, age ≥60 years old, the number of intestinal polyps ≥3, the size of intestinal polyps ≥2 cm, villous adenoma or villous tubular adenoma (67.31%, 69.23%, 63.46%, 59.62%, 46.15%) were significantly higher than those in the non-recurrence group (48.81%, 45.24%, 44.05%, 35.71%, 21.43%) (P<0.05). Male, age ≥60 years old, the number of intestinal polyps ≥3, the size of intestinal polyps ≥2 cm, villous adenoma or villous tubular adenoma were the risk factors for relapse after interventional treatment of intestinal polyps (P<0.05). The sensitivity of sex, age, number of intestinal polyps, size of intestinal polyps, and histological types to predict postoperative recurrence were 0.467, 0.538, 0.515, 0.610 and 0.563, while the specificity were 0.643, 0.714, 0.750, 0.786 and 0.857.ConclusionMale, age ≥60 years old, the number of intestinal polyps ≥3, the size of intestinal polyps ≥2 cm, histological type of villous adenoma or villous tubular adenoma of the intestinal polyps have higher risk of recurrence after interventional treatment. It can adjust the follow-up program combined with the actual situation of patients to reduce the recurrence rate.
【Keywords】 Intestinal polyps; Interventional treatment; Recurrence; Risk factors; Logistic regression analysis
肠息肉为常见肠道病变,据报道,肠道病变具有腺瘤到肠癌的序贯表现,肠息肉已被认为是肠癌癌前病变。研究表明,我国肠癌发病率居各类型肿瘤发病率的第4位,死亡率则居第5位,及时发现肠息肉并予以有效治疗对于降低肠癌死亡率具有重要作用。肠息肉的临床治疗目前以介入治疗为主,有研究显示,肠息肉介入治疗后复发风险较大,4年内复发率为15%~60%。也有报道表明,随访时间越长,肠息肉介入治疗后的复发率越高,且部分患者发展为浸润性肠癌。明确肠息肉介入治疗后复发的危险因素并对患者进行术后定期随访对于预防术后复发、降低癌变几率具有重要作用。本研究以136例腺瘤性肠息肉患者为例,采用多因素Logistic回归分析明确肠息肉介入治疗后复发危险因素,现报道如下。
1 资料与方法
1.1一般资料选取宜都市第一人民医院2013年1月至2015年4月收治的136例腺瘤性肠息肉患者,男76例,女60例,年龄(62.89±7.88)岁(37~86岁)。纳入标准:(1)病理证实为腺瘤性肠息肉;(2)行内镜下肠息肉电凝电切术;(3)年龄>18岁。排除标准:(1)有家族性息肉病史者;(2)合并克罗恩病、炎症性肠病、结直肠癌者;(3)合并血液系统疾病者。研究获医院伦理委员会批准,患者均签署知情同意书。
1.2 方法
1.2.1 治疗方法:所有患者均行内镜下肠息肉电凝电切术:手术前1 d的夜间进流食,手术当天禁食,肠镜操作前6 h左右让患者服用复方聚乙二醇电解质散(加2 000 ml温水,分4次服用,每次间隔30 min)。用药前可应用开塞露,必要时行清洁灌肠,至排出清水样便为止。进镜至回盲部,退镜过程中观察全结肠及直肠,明确息肉数量、大小、位置、表面、基底等。于基底部注射肾上腺素5 mg至息肉基底部隆起,将圈套器置于息肉基底部,慢慢将圈套器钢丝收紧,混合凝切22~30 U。对于基底部创面较大者,用钛夹对创面进行封堵。息肉组织送检。术后对患者进行随访,2年内返院进行结肠镜检查。
1.2.2 研究方法:根据随访的复发结果将患者分为复发组(n=52)与未复发组(n=84)。比较复发组与未复发组患者的一般资料,包括:(1)性别;(2)年龄:分为<60岁与≥60岁;(3)肠息肉数目:分为<3枚与≥3枚;(4)肠息肉大小:分为<2 cm与≥2 cm(多发肠息肉者以最大息肉的直径为准);(5)肠息肉位置:分为近端结肠(包括盲肠、升结肠、横结肠、结肠肝区、结肠脾区)与远端结肠(包括直肠、乙状结肠、降结肠),多发肠息肉者的位置以所有肠息肉中最接近回盲部者为准;(6)组织学类型:分为管状腺瘤与绒毛腺瘤或绒毛管状腺瘤(多发性肠息肉者以分化程度最差的息肉为准)。比较两组患者的一般情况并进行术后复发的多因素Logistic回归分析,通过ROC曲线对以上因素预测肠息肉介入治疗后复发风险的价值进行预测。
1.3统计学方法采用SPSS 19.0统计软件处理数据,计数资料用例数/%表示,采用χ2检验;危险因素分析采用多因素Logistic回归分析,用ROC曲线评估有关因素对肠息肉介入治疗后复发风险的预测价值。P<0.05为差异有统计学意义。
2 结果
2.1复发组与未复发组一般情况的比较两组患者肠息肉位置占比相比,差异无统计学意义(P>0.05);复发组患者中男性、≥60岁、肠息肉数目≥3枚、肠息肉大小≥2 cm、绒毛腺瘤或绒毛管状腺瘤的占比明显高于未复发组(P<0.05)(见表1)。

表1 复发组与未复发组一般情况的比较Tab 1 Comparison of general conditions between relapse group and non-recurrence group 比例/%
2.2肠息肉介入治疗后复发的多因素Logistic回归分析将有统计学意义的变量纳入多因素Logistic回归分析,结果显示,男性、年龄≥60岁、肠息肉数目≥3枚、肠息肉大小≥2 cm、绒毛腺瘤或绒毛管状腺瘤为肠息肉介入治疗后复发危险因素(P<0.05)(见表2)。
2.3肠息肉介入治疗后复发的ROC预测模型性别、年龄、肠息肉数目、大小、组织学类型对肠息肉介入治疗后复发的ROC曲线下面积分别为0.733、0.745、0.769、0.805、0.782,敏感度分别为0.467、0.538、0.515、0.610、0.563,特异度分别为0.643、0.714、0.750、0.786、0.857,对肠息肉介入治疗后的复发有一定的预测价值(见图1)。

表2 肠息肉介入治疗后复发的多因素Logistic回归分析Tab 2 Multivariate Logistic regression analysis of recurrence after interventional treatment of intestinal polyps
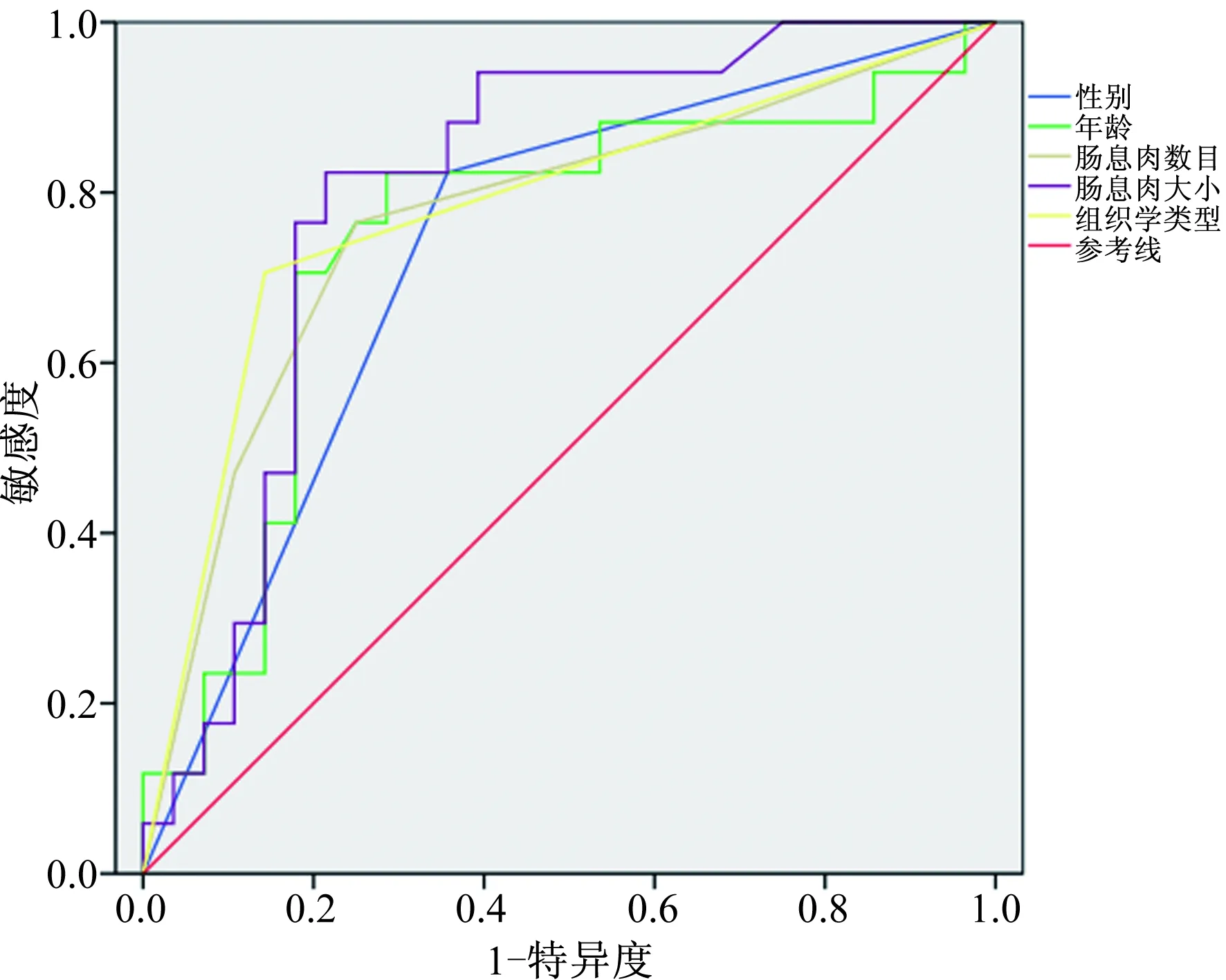
图1 肠息肉介入治疗后复发的ROC曲线Fig 1 The ROC curve of recurrence after interventional treatment of intestinal polyps
3 讨论
3.1性别与年龄对肠息肉复发的影响目前,已有研究表明,男性肠息肉患者的术后复发率更高。本研究复发组中男性占比(67.31%)明显高于未复发组(48.81%),与有关研究结论一致。多因素Logistic回归分析证实,性别为男性是术后复发的危险因素之一。有研究[6]指出,男性与女性的生理差异决定了二者体内雌/孕激素含量的不同,女性体内雌/孕激素含量显著高于男性。据报道[7],雌/孕激素可通过受体拮抗发挥抗癌作用,该作用可能是降低肠息肉术后复发率出现性别差异的主要原因。男性与女性在吸烟、蛋白质、脂肪及纤维素摄入等方面也有明显不同,可能与性别因素的差异有关,有待进一步证实。国外有研究[8]显示,60岁以上肠息肉患者的术后复发风险更高。也有研究[9]显示,右半结肠腺瘤性息肉的复发率随年龄增长而升高。本研究中复发组年龄≥60岁患者的占比达69.23%,明显高于未复发组的45.24%,多因素Logistic回归分析证实,年龄≥60岁为术后复发的危险因素。有证据[10]显示,肠息肉的发生与肠道受到机械性及炎性刺激有关。随着年龄的增长,胃肠功能紊乱、便秘、腹泻症状较年轻人更为常见,增加了肠道刺激,这可能是≥60岁肠息肉患者术后复发率更高的主要原因。也有研究[11]指出,非甾体类抗炎药物的应用对肠息肉的复发有一定影响,而老年人的非甾体类抗炎药物应用频率高于年轻人,故术后复发率更高。
3.2肠息肉数目、大小及组织学类型对肠息肉复发的影响多发性息肉术后复发风险更大的观念已被较多学者认可。肠息肉数量的增加为息肉的进一步生长提供了条件。有研究[12]显示,肠息肉癌变风险随息肉数量增加而增大。也有研究[13]证实,息肉数目与复发有关而与癌变无关。研究[14]则多支持息肉数目与术后复发有关,与癌变的关系还有待进一步研究。本研究复发组中肠息肉数目≥3枚患者的占比为63.46%,明显高于未复发组的44.05%,多因素Logistic回归分析证实,肠息肉数目≥3枚为术后复发危险因素之一。与肠息肉数目类似,直径大小也与肠息肉癌变有一定关联。本研究复发组中息肉大小≥2 cm患者的占比为59.62%,高于未复发组的35.71%。多因素Logistic回归分析证实,息肉大小≥2 cm为术后复发的危险因素。也有研究[15]表明,肠息肉大小与术后复发之间无明显相关性,与本研究结论存在较大差异,推测可能与肠息肉的漏诊有关。复查时部分患者息肉视为复发息肉,导致息肉大小对术后复发影响的结果被误判。另外,国外研究[16]显示,肠息肉大小影响术后复发的临界值为10 mm,小于本研究中的划分界限2 cm,推测其中息肉大小的测量操作不可忽视,测量结果的精确度对临界值的影响较大,还可能与样本量、种族有关,有待进一步确认。本研究中,复发组患者中绒毛腺瘤或绒毛管状腺瘤的占比为46.15%,显著高于未复发组的21.43%。多因素Logistic回归分析证实,绒毛腺瘤或绒毛管状腺瘤为术后复发的危险因素之一。组织学类型对术后复发的影响主要与异型增生有关,有研究[17]发现,异型增生可被视为腺瘤性肠息肉到肠癌的发展过度阶段。管状腺瘤较少发展至重度异型增生,而绒毛管状腺瘤或绒毛腺瘤多伴上皮或腺体异型增生,增加了复发风险。也有研究[18]认为,组织学类型对术后复发风险的影响与绒毛组织有关。绒毛组织恶性程度高,组织细胞分裂与生长速度更快,故绒毛管状腺瘤或绒毛腺瘤患者的复发率更高。
3.3性别、年龄、肠息肉数目、大小、组织学类型对术后复发的预测价值目前,临床主要以结肠镜作为检测复发的主要手段,随访时间也因患者自身情况而有所不同。近年美国多社会任务小组等机构颁布了肠息肉术后的随访指南[17],但考虑到国情、种族体质等方面的差异,仍无法完全统一。本研究采用ROC曲线将性别、年龄、肠息肉数目、大小、组织学类型等因素对术后复发的预测价值进行分析,结果显示,敏感度分别为0.467、0.538、0.515、0.610、0.563,特异度分别为0.643、0.714、0.750、0.786、0.857,显示出一定的预测价值,可为术后随访提供一定的参考价值。已有研究[19]提出,可将肠息肉大小作为指导术后随访时间间隔的参考指标。对于术前合并相关危险因素尤其同时合并多项危险因素的患者,术后复发风险较大,可缩短随访间隔时间;而未合并危险因素的患者,随访间隔时间可适当延长至3年,但随访总时间需延长,最好达10年,以避免远期复发。
综上所述,男性、年龄≥60岁、肠息肉数量≥3枚、息肉大小≥2 cm、病理类型为绒毛腺瘤或绒毛管状腺瘤的患者肠息肉介入治疗后的复发率更高。肠息肉患者介入治疗后的随访可结合实际情况进行适当调整以降低复发率。
[1] 陈平, 袁晓琴, 谢玲, 等. 上海市嘉定地区1265例结肠直肠息肉内镜下诊治临床资料回顾性分析[J]. 胃肠病学和肝病学杂志, 2016, 25(5): 524-528. DOI: 10.3969/j.issn.1006-5709.2016.05.011.
CHEN P, YUAN X Q, XIE L, et al. A clinical retrospective study of colonoscopy in diagnosis and treatment of colorectal polyps in Jiading district of Shanghai [J]. Chin J Gastroenterol Hepatol, 2016, 25(5): 524-528. DOI: 10.3969/j.issn.1006-5709.2016.05.011.
[2] 陈冬妹, 肖文, 张满芬, 等. 叶酸对结直肠腺瘤复发干预作用的随访研究[J]. 中国全科医学, 2012, 15(5): 496-497. DOI: 10.3969/j.issn.1007-9572.2012.05.007.
CHEN D M, XIAO W, ZHANG M F, et al. Interventional effects of folic acid on recurrence of colorectal adenoma: follow-up study [J]. Chinese General Practice, 2012, 15(5): 496-497. DOI: 10.3969/j.issn.1007-9572.2012.05.007.
[3] 钟清连, 郑昌京, 黄健, 等. 结直肠息肉切除术后的再发特点及肠镜监测研究[J]. 中国医师杂志, 2016, 18(7): 1005-1007, 1012. DOI: 10.3760/cma.j.issn.1008-1372.2016.07.013.
ZHONG Q L, ZHENG C J, HUANG J, et al. Investigation on colorectal polyp recurrence and colonoscopic surveillance after polypectomy [J]. Journal of Chinese Physician, 2016, 18(7): 1005-1007, 1012. DOI: 10.3760/cma.j.issn.1008-1372.2016.07.013.
[4] 舒晴, 赵素芳, 焦璐, 等. 结肠息肉癌变的相关危险因素及内镜治疗随访结果分析[J]. 现代消化及介入诊疗, 2016, 21(1): 24-27. DOI: 10.3969/j.issn.1672-2159.2016.01.008.
SHU Q, ZHAO S F, JIAO L, et al. Analysis of the risk factors and the effect of endoscopy for the colorectal polyp cancerization [J]. Modern Digestion & Intervention, 2016, 21(1): 24-27. DOI: 10.3969/j.issn.1672-2159.2016.01.008.
[5] 姚兰杰, 唐建荣. 肠息肉患者215例复发危险因素的Logistic回归分析[J]. 中国临床研究, 2014, 27(9): 1078-1079. DOI: 10.13429/j.cnki.cjcr.2014.09.016.
YAO L J, TANG J R. Logistic regression analysis of risk factors for recurrence in 215 patients with intestinal polyps [J]. Chinese Journal of Clinical Research, 2014, 27(9): 1078-1079. DOI: 10.13429/j.cnki.cjcr.2014.09.016.
[6] 李婷珊, 黄颖娴, 彭林, 等. 辨证施膳降低肠息肉术后复发率的回顾性分析研究[J]. 护士进修杂志, 2016, 31(19): 1742-1744. DOI: 10.16821/j.cnki.hsjx.2016.19.006.
LI T S, HUANG Y X, PENG L, et al. Retrospective analysis for reducing the recurrence rate of postoperative intestinal polyps by dialectical meal [J]. Journal of Nurses Training, 2016, 31(19): 1742-1744. DOI: 10.16821/j.cnki.hsjx.2016.19.006.
[7] 邓德昌, 方晓明, 居海红, 等. 内镜黏膜切除术治疗结直肠息肉2609例[J]. 中华胃肠外科杂志, 2012, 15(12): 1301-1303. DOI: 10.3760/cma.j.issn.1671-0274.2012.12.028.
DENG D C, FANG X M, JU H H, et al. Endoscopic mucosal resection in the treatment of 2609 cases with colorectal polyps [J]. Chinese Journal of Gastrointestinal Surgery, 2012, 15(12): 1301-1303. DOI: 10.3760/cma.j.issn.1671-0274.2012.12.028.
[8] NAVANEETHAN U, LOURDUSAMY D, MEHTA D, et al. Endoscopic resection of large sporadic non-ampullary duodenal polyps: efficacy and long-term recurrence [J]. Surg Endosc, 2014, 28(9): 2616-2622. DOI: 10.1007/s00464-014-3512-z.
[9] 步春升, 陈宪秋, 于勇, 等. 大肠镜介入切除直肠息肉样肿物86例分析[J]. 中国老年学杂志, 2011, 31(11): 2083-2084. DOI: 10.3969/j.issn.1005-9202.2011.11.065.
BU C S, CHEN X Q, YU Y, et al. Interventional resection of rectal polypoid masses by colonoscopy: analysis of 86 cases [J]. Chinese Journal of Gerontology, 2011, 31(11): 2083-2084. DOI: 10.3969/j.issn.1005-9202.2011.11.065.
[10] 张黎明, 刘玉兰, 朱元民, 等. 结肠腺瘤高频电凝切除术术后复发情况分析[J]. 中华消化内镜杂志, 2012, 29(8): 429-432. DOI: 10.3760/cma.j.issn.1007-5232.2012.08.003.
ZHANG L M, LIU Y L, ZHU Y M, et al. Colon adenoma recurrence after endoscopic high-frequency electric polypectomy [J]. Chinese Journal of Digestive Endoscopy, 2012, 29(8): 429-432. DOI: 10.3760/cma.j.issn.1007-5232.2012.08.003.
[11] 陈莹璐, 徐月. 济生乌梅片防治大肠息肉内镜治疗后再复发的临床研究[J]. 中国中医急症, 2014, 23(4): 691-692. DOI: 10.3969/j.issn.1004-745X.2014.04.056.
CHEN Y L, XU Y. The study on the clinical effect of Jishengwumei Tablet on prevention and treatment in colorectal polyps relapse again after endoscopic treatment [J]. Journal of Emergency in Traditional Chinese Medicine, 2014, 23(4): 691-692. DOI: 10.3969/j.issn.1004-745X.2014.04.056.
[12] KAY M, ENG K, WYLLIE R. Colonic polyps and polyposis syndromes in pediatric patients [J]. Curr Opin Pediatr, 2015, 27(5): 634-641. DOI: 10.1097/MOP.0000000000000265.
[13] OYSU K, SEKI M, OGAWA S, et al. Multiple myeloma recurring as small intestinal polyposis after autologous hematopoietic stem cell transplantation [J]. Rinsho Ketsueki, 2015, 56(4): 400-405. DOI: 10.11406/rinketsu.56.400.
[14] KIM H G, THOSANI N, BANERJEE S, et al. Underwater endoscopic mucosal resection for recurrences after previous piecemeal resection of colorectal polyps (with video) [J]. Gastrointest Endosc, 2014, 80(6): 1094-1102. DOI: 10.1016/j.gie.2014.05.318.
[15] 袁广众, 韩树堂, 肖君, 等. 中西医防治结肠息肉术后复发的研究进展[J]. 中国临床研究, 2017, 30(5): 695-697. DOI: 10.13429/j.cnki.cjcr.2017.05.037.
YUAN G Z, HAN S T, XIAO J, et al. Progress in research of prevention of recurrence of colonic polyp by Chinese and western medicine [J]. Chinese Journal of Clinical Research, 2017, 30(5): 695-697.
[16] ORTIZ A M, BHARGAVI P, ZUCKERMAN M J, et al. Endoscopic mucosal resection recurrence rate for colorectal lesions [J]. South Med J, 2014, 107(10): 615-621. DOI: 10.14423/SMJ.0000000000000180.
[17] BRADY P G. Commentary on "endoscopic mucosal resection recurrence rate for colorectal lesion [J]. South Med J, 2014, 107(10): 622-623. DOI: 10.14423/SMJ.0000000000000178.
[18] CHOI Y S, LEE J B, LEE E J, et al. Can endoscopic submucosal dissection technique be an alternative treatment option for a difficult giant (≥30 mm) pedunculated colorectal polyp? [J]. Diseases of the Colon and Rectum, 2013, 56(5): 660-666. DOI: 10.1097/DCR.0b013e318276d2b9.
[19] 宋洁菲, 盛剑秋. 结肠镜检查和息肉切除术后随访策略进展[J]. 胃肠病学, 2015, 20(7): 424-427. DOI: 10.3969/j.issn.1008-7125.2015.07.010.
SONG J F, SHENG J Q. Advances in follow-up colonoscopy strategy after endoscopic resection of colorectal polyps [J]. Chin J Gastroenterol, 2015, 20(7): 424-427. DOI: 10.3969/j.issn.1008-7125.2015.07.010.
