Does knowledge of physical activity recommendations increase physical activity among Chinese college students?Empirical investigations based on the transtheoretical model
2018-04-26KhrAulPeterGrpelKiChenrgenBeckmnn
Khr Aul*,Peter GröpelKi Chen,Jürgen Beckmnn
aTechnical University of Munich,München 80992,Germany
bSouth West Jiao Tong University,Chengdu 611756,China
1.Introduction
Numerous studies show that regular physical activity(PA)benefits health and well-being.1-3Yet for the majority of the population worldwide,a significant drop in PA level in recent decades has been reported.4Health organizations such as the American College of Sports Medicine or the World Health Organization(WHO)published their recommendations on PA for health,suggesting at least 150 min of moderate-to vigorous-intensity PA throughout the week.5,6However,little effort has been taken to educate people about these guidelines.For example,Kay et al.7found that only 36%of the national survey responders were aware of the PA recommendations in the USA.Similarly,the recommendations were correctly recalled by only 15%of responders in the UK.8,9Thus,it is not clear whether the published guidelines actually affect people’s PA behavior.
To the best of our knowledge,until now no official PA guideline has been published in the Mainland of China.In an effort to provide guidance to public health authorities,the present study investigated whether people’s awareness of PA guidelines is associated with enhanced levels of PA.
Although awareness and knowledge of behavioral recommendations are important prerequisites for actual behavior and behavioral change,10,11prior research on the relationship between awareness of PA recommendations and actual PA shows mixed results.12-14Cameron et al.12and Plotnikoff et al.13found that awareness of PA recommendations predicted the level of PA,with those who were aware of the recommendations being significantly more physically active than those who were not aware of the recommendations.In contrast,Morrow et al.14found no association between awareness of the recommendations and the actual level of PA.Similarly,the results of intervention studies that increased participants’awareness level are also inconsistent.Loughlan and Mutrie15found a significant increase in the level of PA after the intervention,whereas Plotnikoff et al.13reported no significant change.
A possible explanation for the inconsistent results is that awareness of PA recommendations does not directly affect behavior;people must first develop intentions to exercise.Marcus et al.16argued that individuals need to move through different stages to finally alter their PA behavior.Marcus et al.16applied the transtheoretical model of health behavior change,which defines behavior change as a dynamic,stage-based process.17,18In this model,individuals first work through cognitive and affective processes leading to adoption of a new behavior,and then they move to using behavioral strategies to establish a new pattern of behavior.Based on this model,Marcus et al.16proposed 5 distinct stages involved in the process of PA behavior change:precontemplation,contemplation,preparation,action,and maintenance.Precontemplators are physically inactive and have no intention to become active.Contemplators are also inactive but are thinking about becoming active,though no actual action has yet taken place. Preparers are physically active but not at the recommended level.Individuals in the action stage are physically active at the recommended level but have been active for less than 6 months.Finally,individuals in the maintenance stage are physically active at the recommended level and have been active for 6 or more months.
Prior research supports the validity of the stages of PA behavior.18Marcus et al.16have also identified a number of cognitive and behavioral strategies used throughout the stages of change.Cognitive strategies,such as increasing knowledge,being aware of risks,or comprehending benefits,typically peak in the preparation stage,whereas behavioral strategies such as enlisting social support,rewarding oneself,or reminding oneself typically peak in the action stage.Accordingly,for a successful behavior change,increasing awareness of PA recommendations may apply only to precontemplation,contemplation,and preparation stages.19Therefore,awareness of PA recommendations is especially likely to increase intentions to take part in PA regularly.Regarding actual behavior,awareness of the recommendations may not automatically increase the level of PA because the behavioral strategies are of higher relevance in action and maintenance stages.16
To test this proposition,we measured the awareness of the international(WHO)PA recommendations,the stages of PA behavior change,and the level of PA among Chinese college students.Research evidence indicates that PA level throughout life declines most dramatically from late adolescence to early adulthood,that is,during college years.20-22Investigating college students may therefore have important implications for active lifestyle and health promotion among the population,and China has the largest college student population in the world,25.5 million in 2014.23
Two separate studies were conducted.In Study 1,we tested the associations between the awareness of PA recommendations,the stages of PA behavior change,and the current levels of PA.In Study 2,we tested whether increased awareness of PA recommendations resulted in a shift from earlier to later stages of PA behavior change and an increase in actual PA at the same time.As far as we know,the present study is the first attempt to assess the impact of PA recommendations on stages of PA behavior and PA level in China.
2.Study 1
Study 1 addressed the awareness of PA recommendations.Because there has been no prior research in this field in China,we were first interested in the proportion of students who were aware of the international(WHO)recommendations on PA for health.For descriptive reasons,awareness of the recommendations was also measured among physical education(PE)teachers,a sample of professionals that one would typically expect to have this knowledge.Furthermore,we tested whether students who were and who were not aware of the recommendations were at different stages of PA behavior.Finally,Study 1 also explored the association between awareness of the recommendations and the current level of self-reported PA.
2.1.Methods
2.1.1.Participants
A total of 9826 college students(5652 females and 4174 males)completed the survey.Participants were recruited across universities in Beijing,Chengdu,Wuhan,Ürümqi,and Kashgar.Their ages ranged from 16 to 30 years(21.00±2.13 years,mean±SD).In addition,251 PE teachers(109 females and 142 males)were surveyed on their awareness of PA recommendations.Teachers were on average 39.50±5.07 years old(range from 26 to 55 years).The study used a cross-sectional research design.The study was approved by the Ethics Board of Peking University,and all participants provided written informed consent before taking part in this study.
2.1.2.Instruments
Stages of PA behavior were measured with the Physical Activity Stage of Change Questionnaire.24In particular,we used the previously validated Chinese version.25The questionnaire consists of 4 items that group individuals into 1 of the 5 stages of PA behavior.An example item is“I intend to become more physically active in the next 6 months”.The participants’levels of PA were measured by the short version of the International Physical Activity Questionnaire.26We used the Chinese version,which was previously validated among college students and demonstrated good psychometric properties in the Mainland of China.27In this questionnaire,participants recall the frequency and the duration of walking and moderate and vigorous PA in the past 7 days across all life domains.An example item is“During the past 7 days,on how many days did you do vigorous physical activities like heavy lifting,digging,aerobics,or fast bicycling?”To assess the awareness of PA recommendations,participants were asked“Do you know what the international recommendations are for taking part in physical activity,in terms of minutes per week of moderate-to vigorous-intensity physical activity?”9Participants who responded “no”were labeled as“don’t know”.Participants who responded “yes”were then asked “What are the international physical activity recommendations?”Answers of 150 min per week,which are in line with current PA recommendations,6were considered correct.Participants with answers of greater than 150 min per week were labeled as overestimators,and those giving answers of less than 150 min per week were labeled as underestimators.
2.1.3.Statistical analyses
Descriptive analyses were conducted to examine the proportion of students and teachers who had accurate knowledge of PA guidelines.Pearson’s χ2test was used to test whether participants who were aware and not aware of PA guidelines were equally distributed across the stages of PA behavior,and Cramer’sVwas calculated to test the association between awareness of the recommendation and stages of PA behavior.Finally,independentttest was conducted to test the difference in PA levels among those who are aware and those who are not aware of the guideline.The total energy expenditure(metabolic equivalent of task;MET)was calculated as an index of actual PA as follows:MET minutes per week=8.0×vigorous-intensity minutes×vigorous-intensity days+4.0×moderate-intensity minutes×moderate days+3.3×walking minutes×walking days.28
2.2.Results
The PA recommendations were accurately reported by 4.4%of students,whereas 3.8%overestimated,10.9%underestimated,and 80.9%reported not being aware of the recommendations(Table 1).PE teachers had better knowledge,with 14.7%of them correctly reporting,13.2%overestimating,22.3%underestimating,and 49.8%who did not know.No gender differences were found except that there were moremale students(12%)than female students(10%)who underestimated the PA guidelines(χ2(1)=10.29,p=0.001).

Table 2Awareness of physical activity recommendations and the stages of physical activity behavior(n(%)).
Among the students,we compared the individuals who had correct knowledge of the PA recommendations with those who did not know the recommendations.(No further differentiation between under estimators and over estimators was considered.)Individuals aware and not aware of the PA recommendations were unequally distributed across the stages of PA behavior(χ2(4)=167.19,p< 0.001).In particular,those who were not aware of the recommendations were over-represented in the precontemplation and contemplation stages but underrepresented in preparation,action,and maintenance,as indicated respectively by the positive and negative values of the residuals(Table 2).Awareness of PA recommendations was significantly associated with later stages of PA behavior(Cramer’sV=0.14,p<0.001).Those who were aware of the recommendations were significantly more physically active than those who were not aware of the recommendations(MET minutes per week:1166.32±1255.82vs.1214.85±753.59,t(443.71)=9.00,p< 0.001,Cohen’sd=0.53).
2.3.Brief discussion
These results indicated a low awareness of the international(WHO)PA recommendations(4.4%)among college students in China.PE teachers,who are regarded as professionals in the domain of PA,had a level of knowledge(14.7%)similar to samples of non-professionals in such Western countries as the UK.8,9This might be explained by the fact that no national PA guidelines have been published in China so far,nor have the international guidelines on PA for health been disseminated to the general public.This highlights the need for an intervention study to test whether increasing awareness of the guidelines brings benefits for PA behavior.
The results of Study 1 are promising in this regard because participants with knowledge of PA recommendations are more physically active than those without such knowledge. Increasing awareness of PA guidelines may thus contribute to increased PA behavior.Study 2 was designed to test this hypothesis.
3.Study 2
Individuals who were not aware of the international PA recommendations were either educated on these recommendations or assigned to a control group.After a period of 4 months,we tested whether the educated participants would report a shift from earlier to later stages of PA behavior and a higher level of PA.
3.1.Methods
3.1.1.Participants
A new sample of 350 students was recruited at the Kashgar University in Western China.There were 302 persons who did not know the international PA recommendations.Of these,23 did not complete all assessments at 2 time points,thus resulting in the final sample of 279 participants(148 females and 131 males).The participants’ages ranged from 17 to 25 years(20.90±1.90 years,mean±SD).The study was approved by the Ethics Board of Peking University.All participants provided informed consent before taking part in this study.
3.1.2.Procedure
The study used a pre-post comparison group design to examine the differential change in pre-post stages of PA behavior and PA levels for the intervention group relative to the control group.In the pre-test,at the beginning of the semester in September,participants provided data on the awareness of PA recommendations,the stages of PA behavior,and the current levels of PA using the same instruments as in Study 1.Participants were then randomly(by drawing lots)allocated either to the intervention group or to the control group,but the study assessors were not blinded to group allocation.Control group participants were thanked for completing the questionnaires and dismissed.They received no further instructions.Intervention group participants were gathered in a classroom and provided with written materials that contained information on the international PA recommendations along with their health-related benefits and examples of moderate-to vigorous intensity PA.Very briefly,the intervention group participants were encouraged to adopt the international PA guidelines.In the post-test at the end of the semester in December,the participants’stages of PA behavior and self-reported PA level were measured for the second time in both groups.
3.1.3.Statistical analyses
The χ2test and McNemar’s test for correlated proportions were administered to examine the changes in stage distribution after the intervention.Repeated-measures analysis of variance was conducted to test the change inself-reported PA level,with the PA level being the dependent variable and the time and group being the independent variables.
3.2.Results
The proportion of individuals across the stages of PA behavior is presented in Table 3.The χ2analyses showed no significant group differences at pre-test(χ2(4)=7.28,p=0.12)but significant differences at post-test(χ2(4)=28.90,p< 0.001).McNemar’s test for correlated proportions indicated that there were significantly fewer persons in the precontemplation stage after the intervention(χ2(1)=112.06,p< 0.001).For those in the intervention group who were in the precontemplation stage at pre-test,85.2%advanced to the contemplation stage and 14.8%advanced to the preparation stage at post-test,whereas only 4.2%of control participants advanced to a later stage(preparation).Similarly,the test indicated significant changes in the contemplation stage(χ2(1)=118.76,p=0.03).For those inthe contemplation stage at pre-test,38.7%of intervention participants advanced to the preparation stage and 6.5%advanced to the action stage at post-test,whereas the proportion of control participants remained the same.No further significant differences were observed.
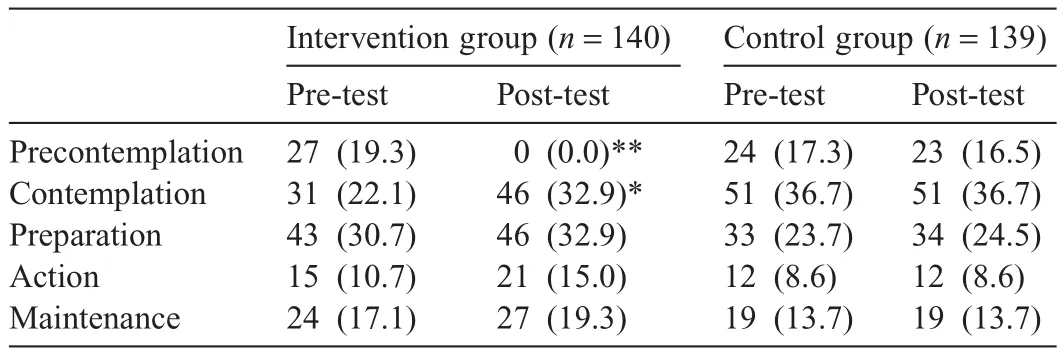
Table 3The number of intervention and control participants and the percentage of sample in each stage of physical activity behavior before and after the intervention.
We conducted a 2×2(Group×Time)repeated-measures analysis of variance to examine the current level of PA(MET)in both groups over the 2 test phases.The analysis revealed no effect of time(p=0.74),no effect of group(p=0.41),and no interaction(p=0.59).Pairedttests showed that the level of PA of the intervention group at post-test was not significantly higher than in the pre-test(1764.32±1490.57 min/weekvs.1740.77±1665.76 min/week,t(139)<1,p=0.89).Similarly,the level of PA of the control group was about the same at post-test as in the pre-test(1601.63±1190.28 min/weekvs.1701.34±1212.63 min/week,t(138)<1,p=0.48).
3.3.Brief discussion
In accordance with Marcus et al.,16the present results suggest that increasing awareness of PA recommendations may be an effective cognitive strategy to develop and strengthen intentions to PA behavior.A significant proportion of participants who were in the precontemplation and contemplation stages at pre-test advanced to a later stage after the educational intervention.However,the actual level of PA did not change,which supports the notion that behavioral rather than cognitive strategies are more relevant for regular PA.16An alternative explanation may be that after exposure to the recommendation,the intervention group participants may have refrained from exercising more because of upcoming exams and the beginning of winter,because the post-test was conducted at the end of the semester in December.
4.General discussion
The present article presents the first findings regarding the awareness of international PA guidelines,the impact of PA recommendations on the stages of PA behavior,and the actual level of PA among the Chinese student population.We found that students who were aware of the international PA recommendations were at later stages of PA behavior and more physically active than those who were not aware of the recommendations(Study 1).Furthermore,increasing awareness of the recommendations through an educational intervention resulted in stronger intentions to exercise but did not change the actual levels of PA during the test period(Study 2).
The results are in line with previously reported evidence that awareness of PA recommendations and the actual level of PA are significantly associated.12,29However,the present work also shows that simply providing knowledge of the guidelines is not sufficient to induce a more active lifestyle.In particular,intervention group participants in Study 2 who were educated about the PA recommendations did not report an enhanced level of PA 4 months later,but they had developed an intention for PA.However,individuals in the precontemplation or contemplation stages advanced to a later stage but not those in preparation,action,or maintenance stages.This is in line with the findings of Prochaska and DiClemente,17,30who proposed that cognitive processes such as increasing knowledge especially play a role in earlier stages of PA behavior.
The present work also found that only 4.4%of Chinese college students had correct knowledge of PA recommendations.The vast majority of Chinese students thus lack the proper knowledge about how much PA they need in everyday life.Results also indicated a low prevalence of that knowledge(14.7%)within the sample of Chinese PE teachers.A plausible explanation is that no national PA guidelines have been published in China so far,nor are there sufficient mass media health promotion campaigns,which would make people more aware of the international PA guidelines and its benefits for healthy life.In addition,the PE system in China should to some extent be held responsible for the low awareness of PA recommendations.Chinese PE is generally designed for learning a sports skill rather than focusing on PA promotion.31,32
It is necessary to be cautious when interpreting the results of Study 2,because PA behavior change is multifactorial and has aspects of information,motivation,behavior,social environment,and policy.Students’knowledge that how much PA is needed to accrue health benefits does not guarantee an actual behavior change,which may explain why the intervention was not successful in increasing PA.However,the present findings regarding the significant association between awareness and PA level in Study 1,along with the significant progress in PA stages among the intervention group students in Study 2,still suggest the urgency of official publication of China’s national guidelines for PA to increase people’s awareness of the recommendations,which may be effectively done by way of such mass media campaigns.33In addition,PA guidelines and their healthrelated benefits should be addressed more in college PE curricula because the level of PA declines most dramatically from high school to college.20-22Physical educators have the opportunity to proactively challenge the physical inactivity problem.The results of Study 2 seem promising in this regard,given that helping people to advance just 1 stage further can double the probability of improved health behavior in the future.34
Finally,the present findings suggest more integration of the stages of PA behavior model into the research on PA behavior.16We found that people aware of PA recommendations were more physically active than those not aware of the recommendations(Study 1),but increasing awareness of the recommendations did not result in higher levels of PA(Study 2).The stages of PA behavior model helps to resolve these seemingly inconsistent findings by showing that making people aware of PA recommendations primarily affects the intention for PA.16Consequently,increasing awareness of PA guidelines may be considered an effective cognitive strategy to promote PA behavior,even if effects on the actual level of PA are not yet visible.On the other hand,the finding that increasing awareness of PA recommendations primarily affects intentions to perform PA also implies limitations of such educational interventions.Developing intentions is a prerequisite for a new PA behavior; however, it alone is not sufficient for long-term maintenance of that behavior.19To foster PA adherence,therefore,physical educators and health promoters should employ behavioral strategies such as enlisting social support and rewarding or enriching sports or other PA environments.16,35,36Combining cognitive and behavioral strategies may contribute significantly to improving people’s health and quality of life.
Some limitations deserve mention.First,the present results are limited to student populations.Second,the educational intervention in Study 2 included information on benefits and examples of activities in addition to information on the guidelines.It is thus possible that the combination of this information and not solely the provision of guidelines resulted in stronger intentions to exercise.In addition,the educational intervention was rather brief and represented a simple public health message intervention.To achieve a successful PA behavior change,future studies should consider designs that involve both cognitive and behavioral change components.
5.Conclusion
We primarily investigated whether PA recommendations increase PA.Individuals who knew about the recommendations were more physically active than those without that knowledge base,but educating those who were unaware of the guidelines did not result in higher levels of PA.However,it did facilitate development of PA intentions and higher stages of PA behavior change.There was no follow-up after the posttest in Study 2,which would allow for testing a long-term effect on behavior change.The long-term effect on behavior and the generalizability of the present results are thus an avenue for future research.
Acknowledgment
We thank Nurali Abliz,Ablajan Abduwaqi,Fuquan Lu,Ning Li,Rui Zhang,Zhongkai He,Qinghua Zhang,Ziwide Kerim,and Maimaiti Aili for their help during the data collection.We would also like to thank Maia Smith of Helmholtz Center Munich for helping us with the copyediting of the manuscript.This work was partly supported by the China Scholarship Council(No.201406010330).The funding body was responsible for providing financial support,and it was not involved in the design,data collection,analysis,interpretation,or writing of the manuscript.
Authors’contributions
JB is the principal investigator of the research project;KA conceived of the idea for the article and designed the research;KC and KA collected the data;PG analyzed and interpreted the data.KA and PG wrote the first draft of the article;KC edited and formatted the manuscript;PG and JB critically revised and reviewed the manuscript.All authors read and approved the final manuscript,and agree with the order of presentation of the authors.
Competing interests
The authors declare that they have no competing interests.
1.Gerber M,Pühse U.Review article:do exercise and fitness protect against stress-induced health complaints?A review of the literature.Scand J Public Health2009;37:801-19.
2.Li J,Siegrist J.Physical activity and risk of cardiovascular disease-a meta-analysis of prospective cohort studies.Int J Environ Res Public Health2012;9:391-407.
3.Schulz KH,Meyer A,Langguth N.Physical activity and psychological well-being.Health Res2012;55:55-65.[in German].
4.Ng SW,Popkin BM.Time use and physical activity:a shift away from movement across the globe.Obes Rev2012;13:659-80.
5.Pate RR,Pratt M,Blair SN,Haskell WL,Macera CA,Bouchard C,et al.Physical activity and public health:a recommendation from the Centers for Disease Control and Prevention and the American College of Sports Medicine.JAMA1995;273:402-7.
6.World Health Organization.Global recommendations on physical activity for health.Geneva:World Health Organization Press;2010.
7.Kay MC,Carroll DD,Carlson SA,Fulton JE.Awareness and knowledge of the 2008 physical activity guidelines for Americans.J Phys Act Health2014;11:693-8.
8.Knox EC,Esliger DW,Biddle SJ,Sherar LB.Lack of knowledge of physical activity guidelines:can physical activity promotion campaigns do better?BMJ Open2012;3:e003633.doi:10.1136/bmjopen-2013-003633
9.Knox EC,Musson H,Adams EJ.Knowledge of physical activity recommendations in adults employed in England:associations with individual and workplace-related predictors.Int J Behav Nutr Phys Act2015;12:696.doi:10.1186/s12966-015-0231-3
10.Macdowall W,Bonnell C,Davies M.Health promotion practice.Maidenhead:McGraw-Hill Education;2006.
11.World Health Organization.Health education:theoretical concepts,effective strategies and core competencies.Cairo:WHO Regional Office for the Eastern Mediterranean;2012.
12.Cameron C,Craig CL,Bull FC,Bauman A.Canada’s physical activity guides:has their release had an impact?Can J Public Health2007;98(Suppl.2):S161-9.
13.Plotnikoff RC,Brunet S,Courneya KS,Spence JC,Birkett NJ,Marcus B,et al.The efficacy of stage-matched and standard public health materials for promoting physical activity in the workplace:the physical activity workplace study(PAWS).Am J Health Promot2007;21:501-9.
14.Morrow JR,Krzewinski-Malone JA,Jackson AW,Bungum TJ,Fitzgerald SJ.American adults’knowledge of exercise recommendations.Res Q Exerc Sport2004;75:231-7.
15.Loughlan C,Mutrie N.An evaluation of the effectiveness of three interventions in promoting physical activity in a sedentary population.Health Educ J1997;56:154-65.
16.Marcus BH,Rossi JS,Selby VC,Niaura RS,Abrams DB.The stages and processes of exercise adoption and maintenance in a worksite sample.Health Psychol1992;11:386-95.
17.Prochaska JO,DiClemente CC.Stages and processes of self-change of smoking:toward an integrative model of change.J Consult Clin Psychol1983;51:390-5.
18.Spencer L,Adams TB,Malone S,Roy L,Yost E.Applying the transtheoretical model to exercise:a systematic and comprehensive review of the literature.Health Promot Pract2006;7:428-43.
19.Marcus BH,Forsyth L.Motivating people to be physically active.Champaign,IL:Human Kinetics;2003.
20.Calfas KJ,Sallis JF,Lovato CY,Campbell J.Physical activity and its determinants before and after college graduation.Med Exerc Nutr Health1994;3:323-34.
21.Kwan MY,Cairney J,Faulkner GE,Pullenayegum EE.Physical activity and other health-risk behaviors during the transition into early adulthood:a longitudinal cohort study.Am J Prev Med2012;42:14-20.
22.Pinto BM,Marcus BH.A stages of change approach to understanding college students’physical activity.J Am Coll Health1995;44:27-31.
23.National Bureau of Statistics of China.The annual total number of college students.Available at:http://data.stats.gov.cn/easyquery.htm?cn=C01;[accessed 10.01.2016].
24.Marcus BH,Simkin LR.The stages of exercise behavior.J Sports Med Phys Fitness1993;33:83-8.
25.Abula K,Beckmann J,Chen K,Gröpel P.Validation of the Chinese version of the Physical Activity Stages of Change Questionnaire.Cogent Psychol2016;3:1228509.doi:10.1080/23311908.2016.1228509
26.Craig CL,Marshall AL,Sjorstrom M,Bauman AE,Booth ML,Ainsworth BE,et al.International Physical Activity Questionnaire:12-country reliability and validity.Med Sci Sports Exerc2003;35:1381-95.
27.Qu NN,Li KJ.Study on the reliability and validity of international physical activity questionnaire.Chin J Epidemiol2004;25:265-8.[in Chinese].
28.Guidelines for data processing and analysis of the International Physical Activity Questionnaire(IPAQ)—short and long forms.Available at:https://docs.google.com/viewer?a=v&pid=sites&srcid=ZGVmYXVsdGR vbWFpbnx0aGVpcGFxfGd4OjE0NDgxMDk3NDU1YWRlZTM;2005[accessed 01.06.2016].
29.Plotnikoff RC,Lippke S,Johnson ST,Hugo K,Rodgers W,Spence JC.Awareness of Canada’s physical activity guide to healthy active living in a large community sample.Am J Health Promot2011;25:294-7.
30.Prochaska JO,DiClemente CC.Towards a comprehensive model of change.In:Miller WR,Heather N,editors.Treating addictive behaviors:processes of change.New York,NY:Plenum Press;1986.p.3-27.
31.Chen Y.Analysis and strategies of college physical education reform.Asian Soc Sci2010;6:209-12.
32.Pan FC,Chen CH.Application of the transtheoretical model of exercise behavior change plan in high school students.WASET2010;4:1672-5.
33.Leavy JE,Bull FC,Rosenberg M,Bauman A.Physical activity mass media campaigns and their evaluation:a systematic review of the literature 2003-2010.Health Educ Res2011;26:1060-85.
34.DiClemente CC,Prochaska JQ,Fairhurst SK,Velicer WF,Velasquez MM,RossiJS.The process of smoking cessation:an analysis of precontemplation,contemplation,and preparation stages of change.J Consult Clin Psychol1991;59:295-304.
35.O’Connor MJ.Exercise promotion in physical education:application of the transtheoretical model.J Teach Phys Educ1994;14:2-12.
36.Gröpel P,Wegner M,Schüler J.Achievement motive and sport participation.Psychol Sport Exerc2016;27:93-100.
杂志排行

Journal of Sport and Health Science的其它文章
- Research highlights from the Status report for step it up!The surgeon general’s call to action to promote walking and walkable communities
- Environments favorable to healthy lifestyles:A systematic review of initiatives in Canada
- The built environment correlates of objectively measured physical activity in Norwegian adults:A cross-sectional study
- The association of various social capital indicators and physical activity participation among Turkish adolescents
- Feasibility of using pedometers in a state-based surveillance system:2014 Arizona Behavioral Risk Factor Surveillance System
- Matched or nonmatched interventions based on the transtheoretical model to promote physical activity.A meta-analysis of randomized controlled trials